
Potential Diagnostic Value of Salivary Tumor Markers in Breast, Lung and Ovarian Cancer: A Preliminary Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Description of Study Groups
2.1.1. Breast Cancer
2.1.2. Lung Cancer
2.1.3. Ovarian Cancer
2.2. Collection of Saliva and Determination of Tumor Markers
2.3. Determination of Tumor Markers in Blood Serum
2.4. Statistical Analysis
3. Results
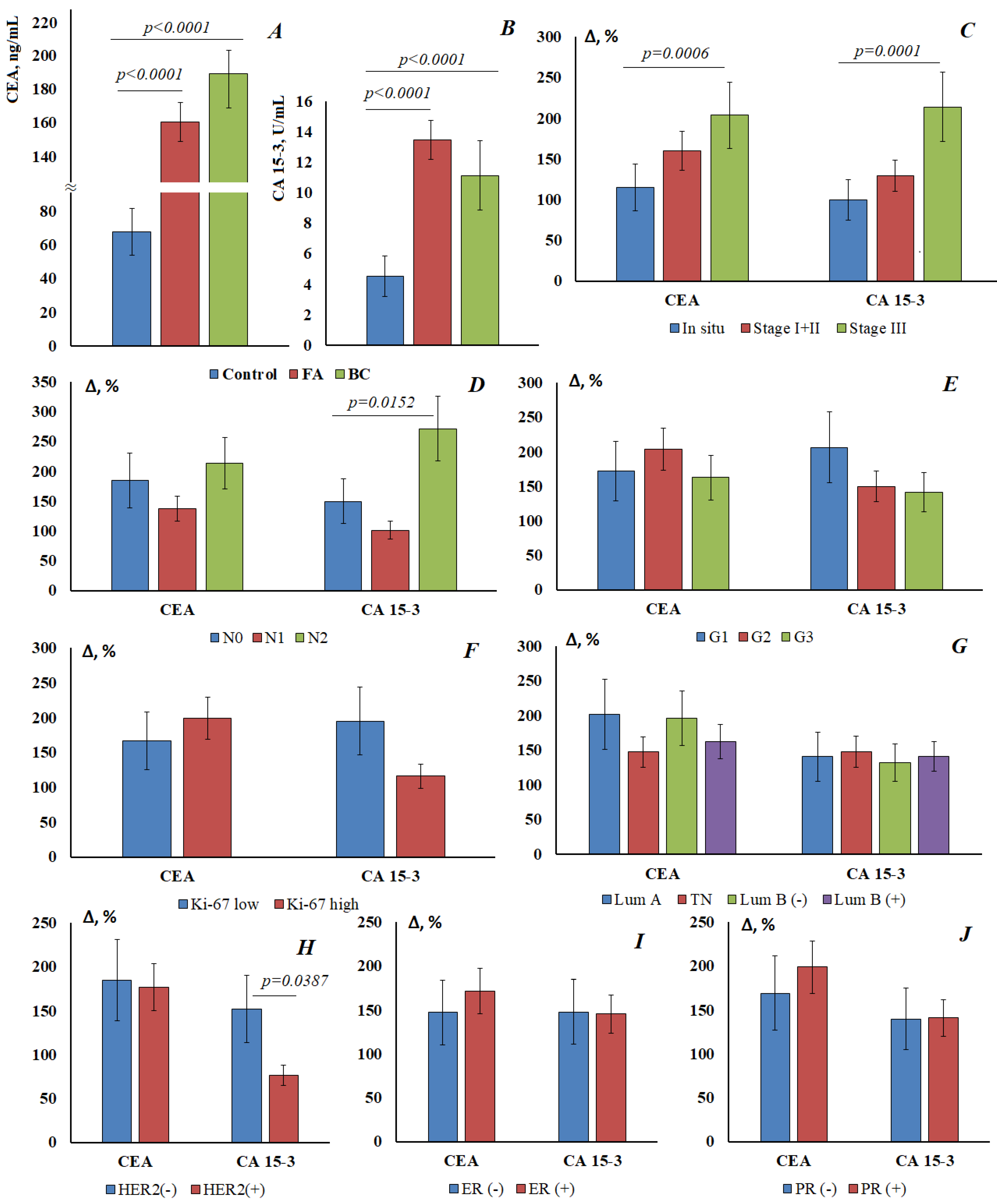
3.1. Determination of Tumor Markers in Saliva for Breast Cancer
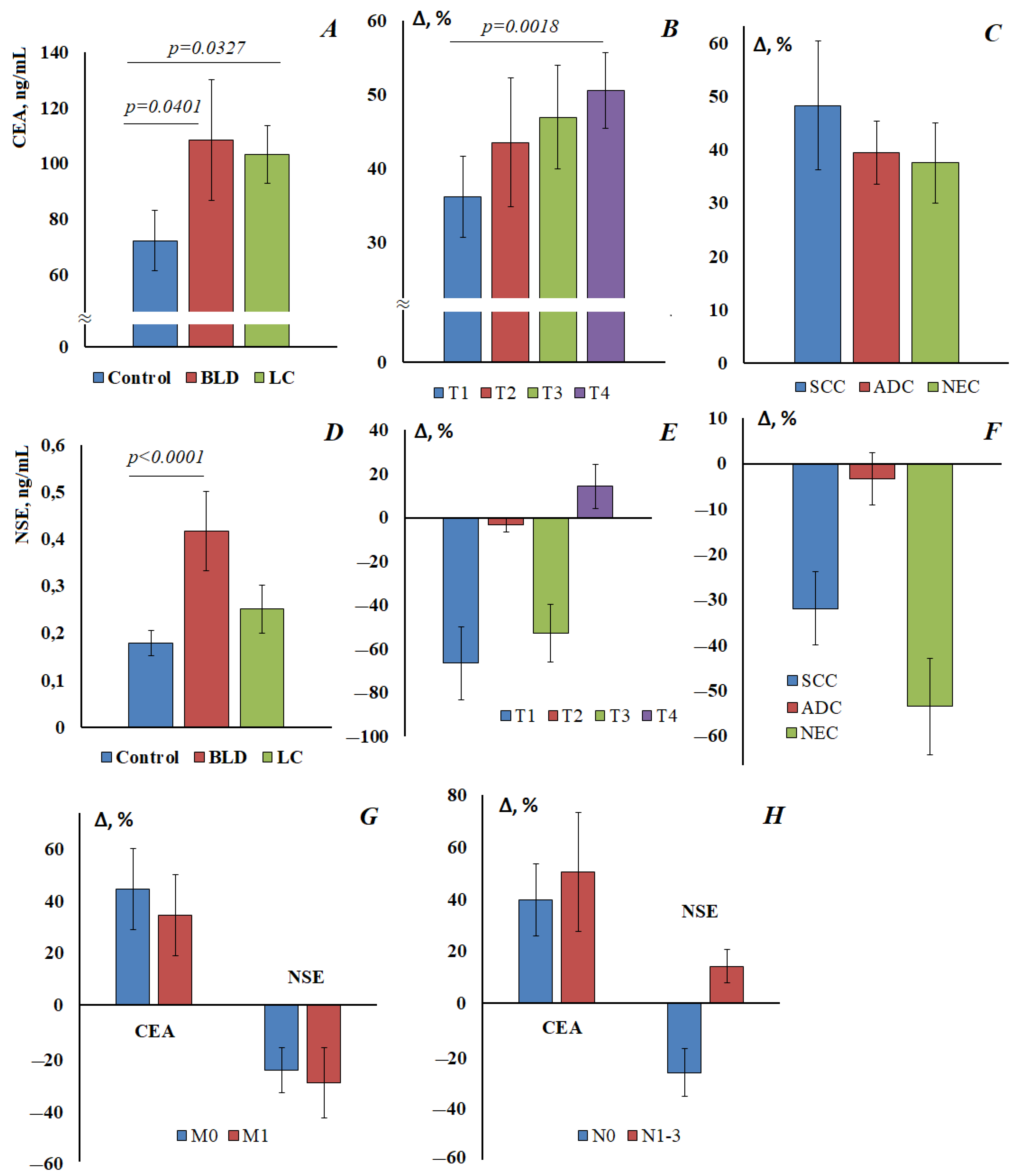
3.2. Determination of Tumor Markers in Saliva for Lung Cancer
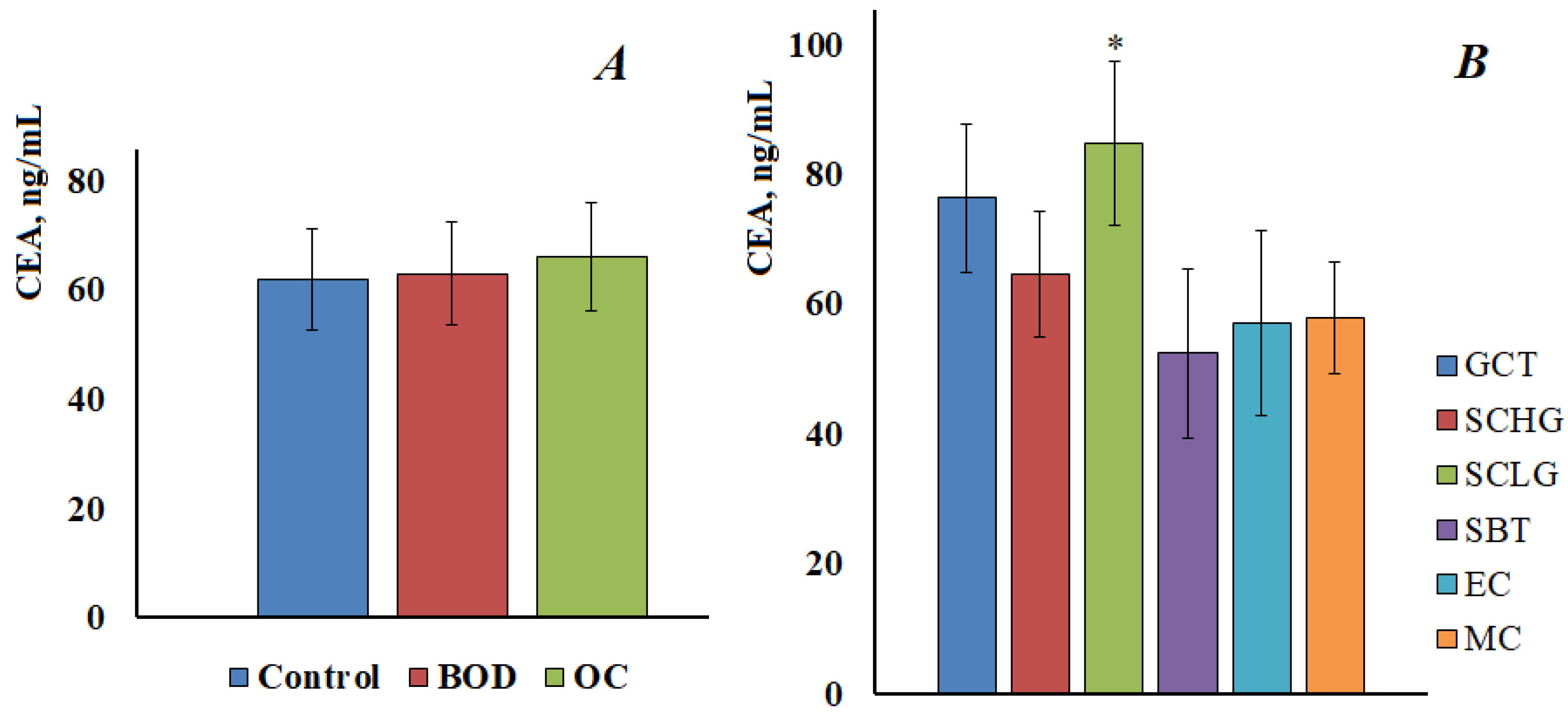
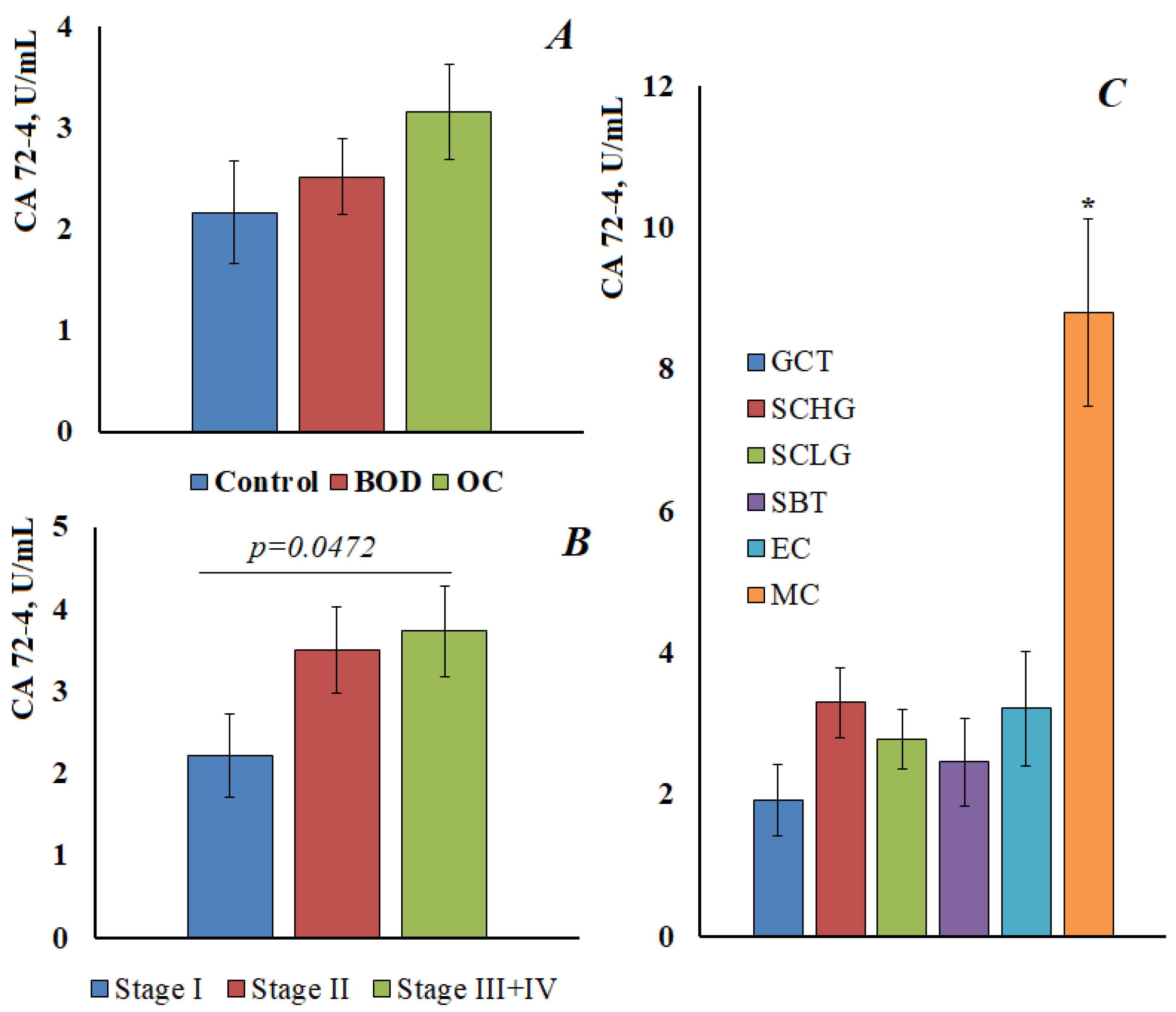
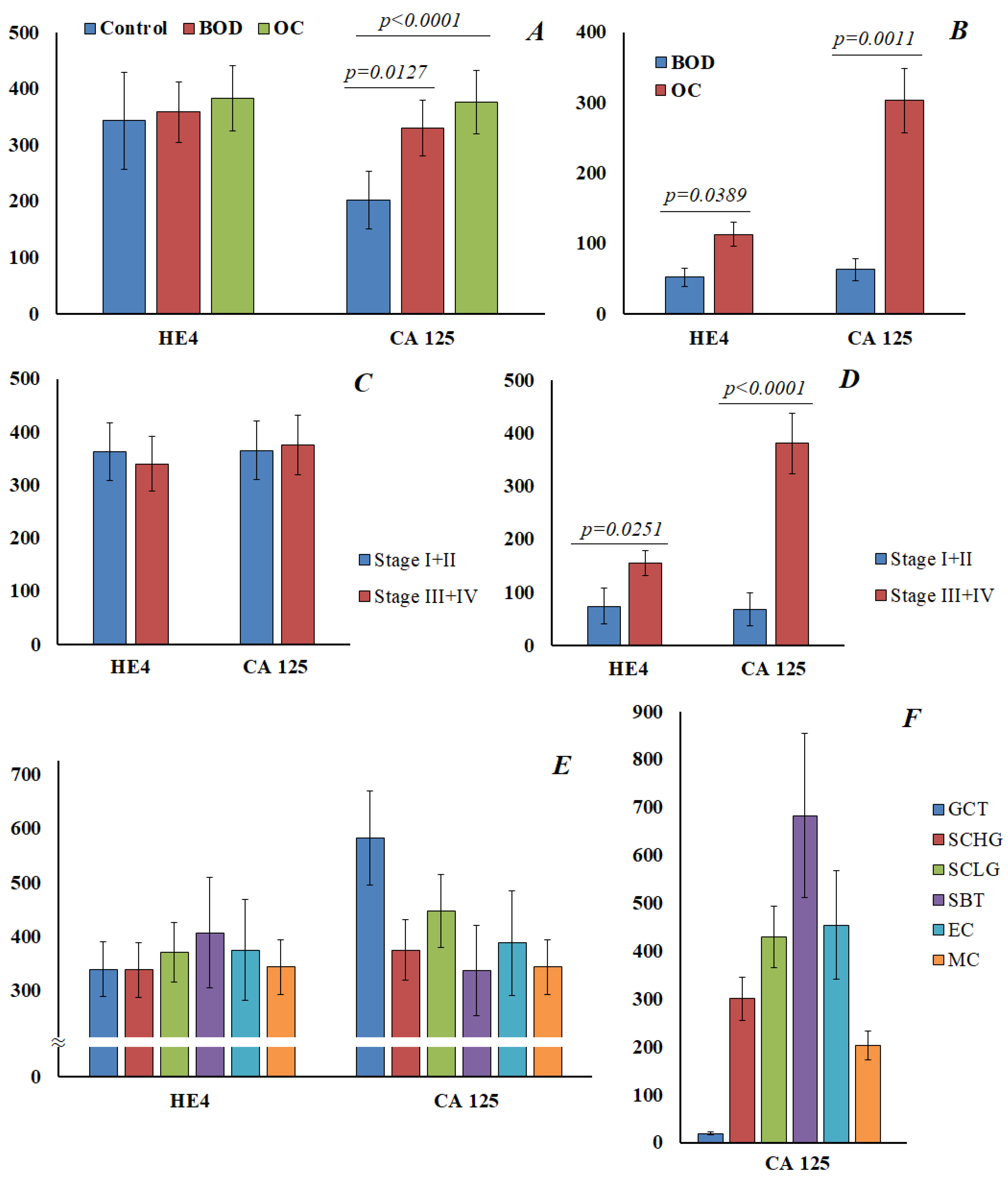
3.3. Determination of Tumor Markers in Saliva and Blood for Ovarian Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, Z.; Yang, X.; Huang, Y.; Tang, Z.; Chen, Y.; Liu, H.; Huang, M.; Qing, L.; Li, L.; Wang, Q.; et al. Saliva—A new opportunity for fluid biopsy. Clin. Chem. Lab. Med. 2023, 61, 4–32. [Google Scholar] [CrossRef] [PubMed]
- Roblegg, E.; Coughran, A.; Sirjanim, D. Saliva: An all-rounder of our body. Eur. J. Pharm. Biopharm. 2019, 142, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Bai, H.; Zhang, P.; Zhou, X.; Ying, B. Promising applications of human-derived saliva biomarker testing in clinical diagnostics. Int. J. Oral Sci. 2023, 15, 2. [Google Scholar] [CrossRef] [PubMed]
- Roi, A.; Rusu, L.C.; Roi, C.I.; Luca, R.E.; Boia, S.; Munteanu, R.I. A New Approach for the Diagnosis of Systemic and Oral Diseases Based on Salivary Biomolecules. Hindawi Dis. Markers 2019, 2019, 8761860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khurshid, Z.; Warsi, I.; Moin, S.F.; Slowey, P.D.; Latif, M.; Zohaib, S.; Zafar, M.S. Biochemical analysis of oral fluids for disease detection. Adv. Clin. Chem. 2021, 100, 205–253. [Google Scholar] [PubMed]
- Nunes, L.A.; Mussavira, S.; Bindhu, O.S. Clinical and diagnostic utility of saliva as a non-invasive diagnostic fluid: A systematic review. Biochem. Med. 2015, 25, 177–192. [Google Scholar] [CrossRef]
- Meghnani, V.; Mohammed, N.; Giauque, C.; Nahire, R.; David, T. Performance characterization and validation of saliva as an alternative specimen source for detecting hereditary breast cancer mutations by next generation sequencing. Int. J. Genom. 2016, 2016, 2059041. [Google Scholar] [CrossRef] [Green Version]
- Cascella, R.; Stocchi, L.; Strafella, C.; Mezzaroma, I.; Mannazzu, M.; Vullo, V.; Montella, F.; Parruti, G.; Borgiani, P.; Sangiuolo, F.; et al. Comparative analysis between saliva and buccal swabs as source of DNA: Lesson from HLA-B*57:01 testing. Pharmacogenomics 2015, 16, 1039–1046. [Google Scholar] [CrossRef] [Green Version]
- Assad, D.X.; Mascarenhas, E.C.P.; de Lima, C.L.; de Toledo, I.P.; Chardin, H.; Combes, A.; Acevedo, A.C.; Guerra, E.N.S. Salivary metabolites to detect patients with cancer: A systematic review. Int. J. Clin. Oncol. 2020, 25, 1016–1036. [Google Scholar] [CrossRef]
- Hasanzadeh, M.; Sharifi, S.; Dizaj, S.M.; Khalilov, R.; Ahmadian, E. Bioassay of saliva proteins: The best alternative for conventional methods in non-invasive diagnosis of cancer. Int. J. Biol. Macromol. 2019, 124, 1246–1255. [Google Scholar]
- Kaczor-Urbanowicz, K.E.; Wei, F.; Rao, S.L.; Kim, J.; Shin, H.; Cheng, J.; Tu, M.; Wong, D.T.W.; Kim, Y. Clinical validity of saliva and novel technology for cancer detection. BBA-Rev. Cancer 2019, 1872, 49–59. [Google Scholar] [CrossRef] [PubMed]
- de Lima, L.T.F.; Bark, J.M.; Rasheduzzaman, M.; Weeramange, C.E.; Punyadeera, C. Saliva as a matrix for measurement of cancer biomarkers. In Clinical Aspects and Laboratory Determination. Cancer Biomarkers; Elsevier: Amsterdam, The Netherlands, 2022; pp. 297–351. [Google Scholar]
- Nijakowski, K.; Zdrojewski, J.; Nowak, M.; Gruszczyński, D.; Knoll, F.; Surdacka, A. Salivary Metabolomics for Systemic Cancer Diagnosis: A Systematic Review. Metabolites 2023, 13, 28. [Google Scholar] [CrossRef] [PubMed]
- Eftekhari, A.; Dizaj, S.M.; Sharifi, S.; Salatin, S.; Khalilov, R.; Samiei, M.; Vahed, S.Z.; Ahmadian, E. Salivary biomarkers in cancer. Adv. Clin. Chem. 2022, 110, 171–192. [Google Scholar]
- Streckfus, C.; Bigler, L.; Dellinger, T.; Dai, X.; Kingman, A.; Thigpen, J.T. The presence of soluble c-erbB-2 in saliva and serum among women with breast carcinoma: A preliminary study. Clin. Cancer Res. 2000, 6, 2363–2370. [Google Scholar] [PubMed]
- Chen, D.X.; Schwartz, P.E.; Li, F.Q. Saliva and serum CA125 assays for detecting malignant ovarian tumors. Obstet. Gynecol. 1990, 75, 701–704. [Google Scholar] [PubMed]
- Balan, J.J.; Rao, R.S.; Premalatha, B.R.; Patil, S. Analysis of tumor marker CA 125 in saliva of normal and oral squamous cell carcinoma patients: A comparative study. J. Contemp. Dent. Pract. 2012, 13, 671–675. [Google Scholar] [CrossRef]
- Rajkumar, K.; Ramya, R.; Nandhini, G.; Rajashree, P.; Ramesh Kumar, A.; Nirmala Anandan, S. Salivary and serum level of CYFRA 21-1 in oral precancer and oral squamous cell carcinoma. Oral Dis. 2015, 21, 90–96. [Google Scholar] [CrossRef]
- Jafari, M.; Hasanzadeh, M. Non-invasive bioassay of Cytokeratin Fragment 21.1 (Cyfra 21.1) protein in human saliva samples using immunoreaction method: An efficient platform for early-stage diagnosis of oral cancer based on biomedicine. Biomed. Pharmacother. 2020, 131, 110671. [Google Scholar] [CrossRef]
- Joshi, S.; Kallappa, S.; Kumar, P.; Shukla, S.; Ghosh, R. Simple diagnosis of cancer by detecting CEA and CYFRA 21-1 in saliva using electronic sensors. Sci. Rep. 2022, 12, 15315. [Google Scholar] [CrossRef]
- Liang, Y.-H.; Chang, C.-C.; Chen, C.-C.; Chu-Su, Y.; Lin, C.-W. Development of an Au/ZnO thin film surface plasmon resonance-based biosensor immunoassay for the detection of carbohydrate antigen 15-3 in human saliva. Clin. Biochem. 2012, 45, 1689–1693. [Google Scholar] [CrossRef]
- Farahani, H.; Amri, J.; Alaee, M.; Mohaghegh, F.; Rafiee, M. Serum and Saliva Levels of Cancer Antigen 15-3, Carcinoembryonic Antigen, Estradiol, Vaspin, and Obestatin as Biomarkers for the Diagnosis of Breast Cancer in Postmenopausal Women. Lab. Med. 2020, 51, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Yio, X.Y.; Jiang, J.; Yin, F.Z.; Ruan, K.-H. Highly Sensitive Sandwich Enzyme Immunoassay for Alpha-Fetoprotein in Human Saliva. Ann. Clin. Biochem. 1992, 29, 519–522. [Google Scholar] [CrossRef] [PubMed]
- López-Jornet, P.; Aznar, C.; Ceron, J.; Asta, T. Salivary biomarkers in breast cancer: A cross-sectional study. Support. Care Cancer 2021, 29, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Agha-Hosseini, F.; Mirzaii-Dizgah, I.; Rahimi, A. Correlation of serum and salivary CA15-3 levels in patients with breast cancer. Med. Oral Patol. Oral Cir. Bucal 2009, 14, e521-4. [Google Scholar] [CrossRef] [Green Version]
- Jokerst, J.V.; Raamanathan, A.; Christodoulides, N.; Floriano, P.N.; Pollard, A.A.; Simmons, G.W.; Wong, J.; Gage, C.; Furmaga, W.B.; Redding, S.W.; et al. Nano-bio-chips for high performance multiplexed protein detection: Determinations of cancer biomarkers in serum and saliva using quantum dot bioconjugate labels. Biosens. Bioelectron. 2009, 24, 3622–3629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geng, X.F.; Du, M.; Han, J.X.; Zhang, M.; Tang, X.F.; Xing, R.D. Saliva CA125 and TPS levels in patients with oral squamous cell carcinoma. Int. J. Biol. Markers 2013, 28, 216–220. [Google Scholar] [CrossRef]
- Zhang, K.-Y.; Liu, C.-Y.; Hua, L.; Wang, S.-L.; Li, J. Clinical evaluation of salivary carbohydrate antigen 125 and leptin in controls and parotid tumours. Oral Dis. 2016, 22, 630–638. [Google Scholar] [CrossRef]
- He, H.; Chen, G.; Zhou, L.; Liu, Y. A joint detection of CEA and CA-50 levels in saliva and serum of patients with tumors in oral region and salivary gland. J. Cancer Res. Clin. Oncol. 2009, 135, 1315–1321. [Google Scholar] [CrossRef]
- Zheng, J.; Sun, L.; Yuan, W.; Xu, J.; Yu, X.; Wang, F.; Sun, L.; Zeng, Y. Clinical value of Naa10p and CEA levels in saliva and serum for diagnosis of oral squamous cell carcinoma. J. Oral Pathol. Med. 2018, 47, 830–835. [Google Scholar] [CrossRef]
- Khosravi, N.; Bahrami, N.; Khosravi, A.; Abedini, A.; Kiani, A.; Sharifynia, S.; Gharaeeyan, P.; Seifi, S.; Mohamadnia, A. Expression of mammaglobin and carcinoembryonic antigen in peripheral blood of patients with breast cancer using real time polymerase chain reaction. Open J. Clin. Diagn. 2017, 7, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Rubins, J.B.; Dunitz, J.; Rubins, H.B.; Maddaus, M.A.; Niewoehner, D.E. Serum carcinoembryonic antigen as an adjunct to preoperative staging of lung cancer. J. Torac. Cardiovasc. Surg. 1998, 116, 412–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, M.N.; Wang, J.; Li, Y.; Zhang, R.; Elashoff, D.; Wong, D.T. Salivary protein factors are elevated in breast cancer patients. Mol. Med. Rep. 2008, 1, 375–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Streckfus, C.; Bigler, L. The use of soluble, salivary c-erbB-2 for the detection and post-operative follow-up of breast cancer in women: The results of a five-year translational research study. Adv. Dent. Res. 2005, 18, 17–24. [Google Scholar] [CrossRef]
- Laidi, F.; Bouziane, A.; Lakhdar, A.; Khabouze, S.; Amrani, M.; Rhrab, B.; Zaoui, F. Significant correlation between salivary and serum CA15-3 in healthy women and breast cancer patients. Asian Pac. J. Cancer Prev. 2014, 15, 4659–4662. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.J.; Hu, Y.; Qian, H.L.; Jiao, S.C.; Liu, Z.F.; Tao, H.T.; Han, L. Expression and significance of ER, PR, VEGF, CA15-3, CA125 and CEA in judging the prognosis of breast cancer. Asian Pac. J. Cancer Prev. 2013, 14, 3937–3940. [Google Scholar] [CrossRef]
- Assad, D.X.; Mascarenhas, E.C.; Normando, A.C.; Chardin, H.; Barra, G.B.; Pratesi, R.; Nóbrega, Y.D.; Acevedo, A.; Guerra, E.N. Correlation between salivary and serum CA15-3 concentrations in patients with breast cancer. Mol. Clin. Oncol. 2020, 13, 155–161. [Google Scholar] [CrossRef]
- Choi, S.B.; Park, J.M.; Ahn, J.H.; Go, J.; Kim, J.; Park, H.S.; Kim, S.I.; Park, B.-W.; Park, S. Ki-67 and breast cancer prognosis: Does it matter if Ki-67 level is examined using preoperative biopsy or postoperative specimen? Breast Cancer Res. Treat. 2022, 192, 343–352. [Google Scholar] [CrossRef]
- Friedrich, R.E.; Davidoff, M.S.; Bartel-Friedrich, S. Expression of Neuron-specific Enolase in Irradiated Salivary Glands of the Rat: A Pilot Study. Anticancer Res. 2010, 30, 1569–1571. [Google Scholar]
- Hergenroeder, G.W.; Redell, J.B.; Moore, A.N.; Dash, P.K. Biomarkers in the clinical diagnosis and management of traumatic brain injury. Mol. Diagn. Ther. 2008, 12, 345–358. [Google Scholar] [CrossRef]
- Bayerl, C.; Lauk, J.; Moll, I.; Jung, E.G. Immunohistochemical characterization of HSP, alpha-MSH, Merkel cells and neuronal markers in acute UV dermatitis and acute contact dermatitis in vivo. Inflamm. Res. 1997, 46, 409–411. [Google Scholar] [CrossRef]
- Al-Rawi, N.H.; Atiyah, K.M. Salivary neuron specific enolase: An indicator for neuronal damage in patients with ischemic stroke and stroke-prone patients. Clin. Chem. Lab. Med. 2009, 47, 1519–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Wang, J.; Cao, D.; Yang, J.; Shen, K.; Huang, H.; Shi, X. Alpha-fetoprotein (AFP)-producing epithelial ovarian carcinoma (EOC): A retrospective study of 27 cases. Arch. Gynecol. Obstet. 2021, 304, 1043–1053. [Google Scholar] [CrossRef] [PubMed]
- Meguro, S.; Yasuda, M. Alpha-fetoprotein-producing ovarian tumor in a postmenopausal woman with germ cell differentiation. Ann. Diagn. Pathol. 2013, 17, 140–144. [Google Scholar] [CrossRef]
- Jha, S.; Sinha, J.; Bharti, S. Alpha Fetoprotein Secreting Mucinous Epithelial Ovarian Carcinoma in a Young Woman—A Rare Case Report and Review of Literature. EJMO 2021, 5, 80–84. [Google Scholar] [CrossRef]
- You, X.Y.; Jiang, J.; Yin, F.Z. Preliminary observation on human saliva alpha-fetoprotein in patients with hepatocellular carcinoma. Chin. Med. J. 1993, 106, 179–182. [Google Scholar] [PubMed]
- Buderath, P.; Kasimir-Bauer, S.; Aktas, B.; Rasch, J.; Kimmig, R.; Zeller, T.; Heubner, M. Evaluation of a novel ELISA for the tumorassociated antigen CA 72-4 in patients with ovarian cancer. Future Sci. OA 2016, 2, FSO145. [Google Scholar] [CrossRef] [Green Version]
- Granato, T.; Midulla, C.; Longo, F.; Colaprisca, B.; Frati, L.; Anastasi, E. Role of HE4, CA72.4, and CA125 in monitoring ovarian cancer. Tumor Biol. 2012, 33, 1335–1339. [Google Scholar] [CrossRef]
- Sergeeva, N.S.; Marshutina, N.V.; Solokhina, M.P.; Alentov, I.I.; Kaprin, A.D. Clinical significance of CA 72-4 as a serological tumor-associated marker. Onkologiya. Zhurnal Im. P.A. Gertsena 2019, 8, 120–125. (In Russian) [Google Scholar] [CrossRef]
- Agha-Hosseini, F.; Mirzaii-Dizgah, I.; Rahimi, A.; Seilanian-Toosi, M. Correlation of serum and salivary CA125 levels in patients with breast cancer. J. Contemp. Dent. Pract. 2009, 10, E001-8. [Google Scholar]
- Tay, S.K.; Chua, E.K. Correlation of serum, urinary and salivary CA 125 levels in patients with adnexal masses. Ann. Acad. Med. Singap. 1994, 23, 311–314. [Google Scholar]
- Vuković, A.; Kuna, K.; Brzak, B.L.; Boras, V.V.; Šeparović, R.; Šekerija, M.; Šumilin, L.; Vidranski, V. The role of salivary and serum CA125 and routine blood tests in patients with ovarian malignancies. Acta Clin. Croat. 2021, 60, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Plante, M.; Wong, G.Y.; Nisselbaum, J.S.; Almadrones, L.; Hoskins, W.J.; Rubin, S.C. Relationship between saliva and serum CA125 in women with and without epithelial ovarian cancer. Obstet. Gynecol. 1993, 81, 989–992. [Google Scholar] [PubMed]
- Dochez, V.; Caillon, H.; Vaucel, E.; Dimet, J.; Winer, N.; Ducarme, G. Biomarkers and algorithms for diagnosis of ovarian cancer: CA125, HE4, RMI and ROMA, a review. J. Ovarian Res. 2019, 12, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bingle, L.; Cross, S.S.; High, A.S.; Wallace, W.A.; Rassl, D.; Yuan, G.; Hellstrom, I.; Campos, M.A.; Bingle, C.D. WFDC2 (HE4): A potential role in the innate immunity of the oral cavity and respiratory tract and the development of adenocarcinomas of the lung. Respir. Res. 2006, 7, 61. [Google Scholar] [CrossRef] [Green Version]
- Karlsen, N.S.; Karlsen, M.A.; Høgdall, C.K.; Høgdall, E.V.S. HE4 Tissue Expression and Serum HE4 Levels in Healthy Individuals and Patients with Benign or Malignant Tumors: A Systematic Review. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2285–2295. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Breast Cancer, n = 48 | Lung Cancer, n = 34 | Ovarian Cancer, n = 51 |
|---|---|---|---|
| Age, years | 56.7 [49.0; 64.0] | 60.1 [55.3; 64.4] | 54.6 [37.9; 61.6] |
| Clinical stage | |||
| In situ | 4 (8.3%) | - | - |
| Stage I | 13 (27.1%) | 4 (11.8%) | 17 (33.4%) |
| Stage II | 19 (39.6%) | 15 (44.1%) | 5 (9.8%) |
| Stage III | 12 (25.0%) | 7 (20.6%) | 26 (50.9%) |
| Stage IV | - | 8 (23.5%) | 3 (5.9%) |
| Lymph node status | |||
| pN0 | 30 (62.5%) | 18 (52.9%) | - |
| pN1 | 10 (28.1%) | 4 (11.8%) | - |
| pN2 + pN3 | 8 (16.6%) | 12 (35.3%) | - |
| Metastasis status | |||
| pM0 | 48 (100%) | 26 (76.5%) | 48 (94.1%) |
| pM1 | - | 8 (23.5%) | 3 (5.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bel’skaya, L.V.; Sarf, E.A.; Loginova, A.I.; Vyushkov, D.M.; Choi, E.D. Potential Diagnostic Value of Salivary Tumor Markers in Breast, Lung and Ovarian Cancer: A Preliminary Study. Curr. Issues Mol. Biol. 2023, 45, 5084-5098. https://doi.org/10.3390/cimb45060323
Bel’skaya LV, Sarf EA, Loginova AI, Vyushkov DM, Choi ED. Potential Diagnostic Value of Salivary Tumor Markers in Breast, Lung and Ovarian Cancer: A Preliminary Study. Current Issues in Molecular Biology. 2023; 45(6):5084-5098. https://doi.org/10.3390/cimb45060323
Chicago/Turabian StyleBel’skaya, Lyudmila V., Elena A. Sarf, Alexandra I. Loginova, Dmitry M. Vyushkov, and En Djun Choi. 2023. "Potential Diagnostic Value of Salivary Tumor Markers in Breast, Lung and Ovarian Cancer: A Preliminary Study" Current Issues in Molecular Biology 45, no. 6: 5084-5098. https://doi.org/10.3390/cimb45060323
APA StyleBel’skaya, L. V., Sarf, E. A., Loginova, A. I., Vyushkov, D. M., & Choi, E. D. (2023). Potential Diagnostic Value of Salivary Tumor Markers in Breast, Lung and Ovarian Cancer: A Preliminary Study. Current Issues in Molecular Biology, 45(6), 5084-5098. https://doi.org/10.3390/cimb45060323