
Efficacy and Security of Tetrodotoxin in the Treatment of Cancer-Related Pain: Systematic Review and Meta-Analysis

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Study Selection
2.2. Study Characteristics
2.3. Meta-Analysis
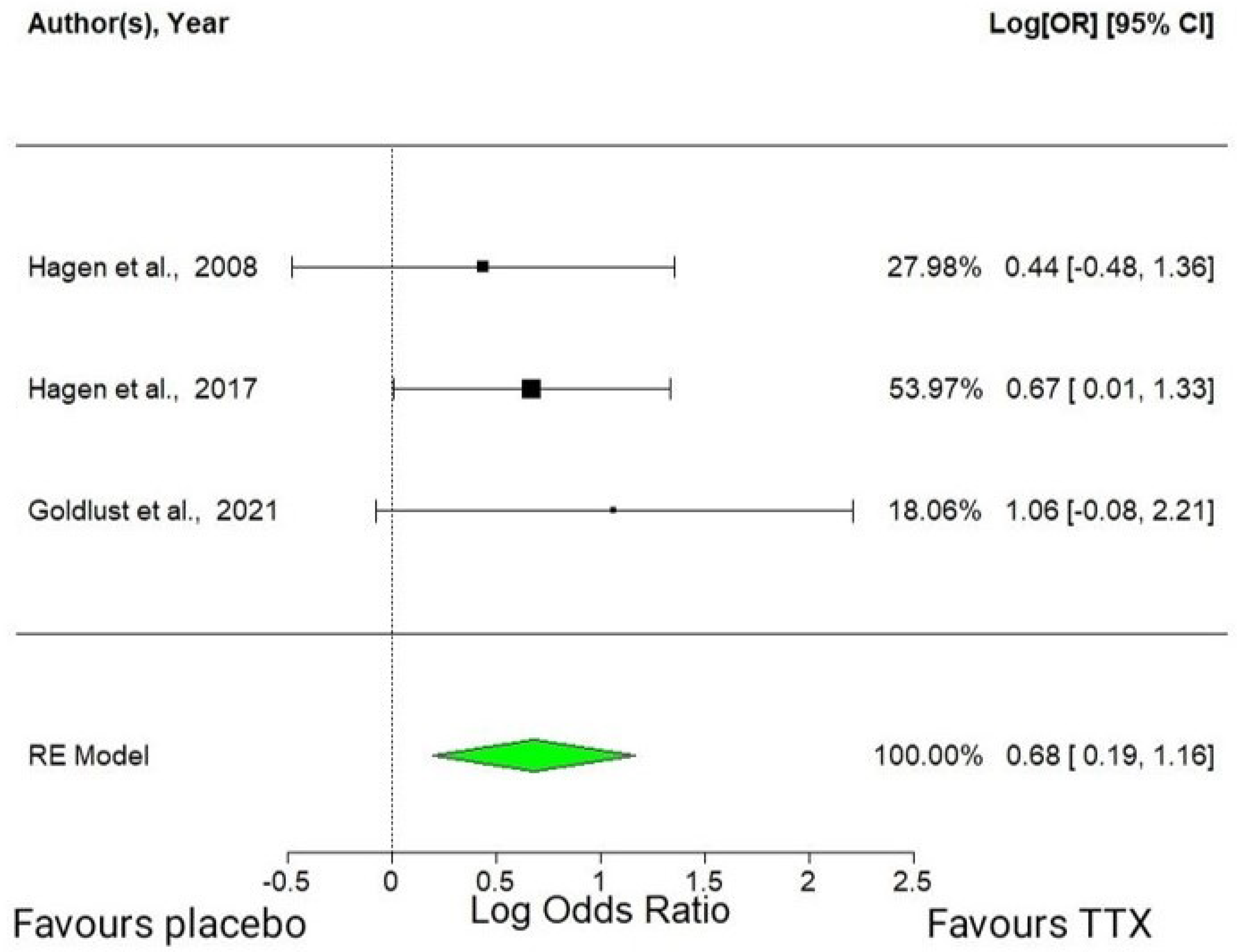
2.3.1. Efficacy of Tetrodotoxin in RCTs
2.3.2. Security of Tetrodotoxin in RCTs
2.4. Risk of Bias
2.5. Publication Bias
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Protocol and Registration
5.2. PICO Research Question
5.3. Information Sources and Search Strategy
5.4. Inclusion and Exclusion Criteria
5.5. Article Selection
5.6. Data Extraction
5.7. Meta-Analysis and Statistics
5.8. Risk of Bias Assessment
5.9. Publication Bias
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Everdingen, M.H.J.v.d.B.; Hochstenbach, L.M.J.; Joosten, E.A.J.; Tjan-Heijnen, V.C.G.; Janssen, D.J.A. Update on Prevalence of Pain in Patients with Cancer: Systematic Review and Meta-Analysis. J. Pain. Symptom. Manag. 2016, 51, 1070–1090.e9. [Google Scholar] [CrossRef] [PubMed]
- Boström, B.; Sandh, M.; Lundberg, D.; Fridlund, B. Cancer-Related Pain in Palliative Care: Patients’ Perceptions of Pain Management. J. Adv. Nurs. 2004, 45, 410–419. [Google Scholar] [CrossRef]
- Breivik, H.; Cherny, N.; Collett, B.; de Conno, F.; Filbet, M.; Foubert, A.J.; Cohen, R.; Dow, L. Cancer-Related Pain: A Pan-European Survey of Prevalence, Treatment, and Patient Attitudes. Ann. Oncol. 2009, 20, 1420–1433. [Google Scholar] [CrossRef] [PubMed]
- Ahles, T.A.; Blanchard, E.B.; Ruckdeschel, J.C. The Multidimensional Nature of Cancer-Related Pain. Pain 1983, 17, 277. [Google Scholar] [CrossRef] [PubMed]
- Lema, M.J.; Foley, K.M.; Hausheer, F.H. Types and Epidemiology of Cancer-Related Neuropathic Pain: The Intersection of Cancer Pain and Neuropathic Pain. Oncologist 2010, 15, 3–8. [Google Scholar] [CrossRef]
- Falk, S.; Bannister, K.; Dickenson, A.H. Cancer Pain Physiology. Br. J. Pain 2014, 8, 154–162. [Google Scholar] [CrossRef]
- Brown, T.J.; Sedhom, R.; Gupta, A. Chemotherapy-Induced Peripheral Neuropathy. JAMA Oncol. 2019, 5, 750. [Google Scholar] [CrossRef]
- Zajączkowska, R.; Kocot-Kępska, M.; Leppert, W.; Wrzosek, A.; Mika, J.; Wordliczek, J. Mechanisms of Chemotherapy-Induced Peripheral Neuropathy. Int. J. Mol. Sci. 2019, 20, 1451. [Google Scholar] [CrossRef]
- Loprinzi, C.L.; Lacchetti, C.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Hertz, D.L.; Kelley, M.R.; Lavino, A.; Lustberg, M.B.; Paice, J.A.; et al. Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy in Survivors of Adult Cancers: ASCO Guideline Update. J. Clin. Oncol. 2020, 38, 3325–3348. [Google Scholar] [CrossRef]
- Seretny, M.; Currie, G.L.; Sena, E.S.; Ramnarine, S.; Grant, R.; MacLeod, M.R.; Colvin, L.A.; Fallon, M. Incidence, Prevalence, and Predictors of Chemotherapy-Induced Peripheral Neuropathy: A Systematic Review and Meta-Analysis. Pain 2014, 155, 2461. [Google Scholar] [CrossRef]
- Caraceni, A.; Shkodra, M. Cancer Pain Assessment and Classification. Cancers 2019, 11, 510. [Google Scholar] [CrossRef]
- Leppert, W.; Zajaczkowska, R.; Wordliczek, J.; Dobrogowski, J.; Woron, J.; Krzakowski, M. Pathophysiology and Clinical Characteristics of Pain in Most Common Locations in Cancer Patients. J. Physiol. Pharmacol. 2016, 67, 787–799. [Google Scholar]
- Staff, N.P.; Grisold, A.; Grisold, W.; Windebank, A.J. Chemotherapy-Induced Peripheral Neuropathy: A Current Review. Ann. Neurol. 2017, 81, 772–781. [Google Scholar] [CrossRef]
- Fallon, M.; Giusti, R.; Aielli, F.; Hoskin, P.; Rolke, R.; Sharma, M.; Ripamonti, C.I. Management of Cancer Pain in Adult Patients: ESMO Clinical Practice Guidelines†. Ann. Oncol. 2018, 29, iv166–iv191. [Google Scholar] [CrossRef] [PubMed]
- Mawatari, H.; Shinjo, T.; Morita, T.; Kohara, H.; Yomiya, K. Revision of Pharmacological Treatment Recommendations for Cancer Pain: Clinical Guidelines from the Japanese Society of Palliative Medicine. J. Palliat. Med. 2022, 25, 1095–1114. [Google Scholar] [CrossRef]
- Swarm, R.A.; Paice, J.A.; Anghelescu, D.L.; Are, M.; Bruce, J.Y.; Buga, S.; Chwistek, M.; Cleeland, C.; Craig, D.; Gafford, E.; et al. Adult Cancer Pain, Version 3.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 977–1007. [Google Scholar] [CrossRef]
- Virgen, C.G.; Kelkar, N.; Tran, A.; Rosa, C.M.; Cruz-Topete, D.; Amatya, S.; Cornett, E.M.; Urits, I.; Viswanath, O.; Kaye, A.D. Pharmacological Management of Cancer Pain: Novel Therapeutics. Biomed. Pharmacother. 2022, 156, 113871. [Google Scholar] [CrossRef] [PubMed]
- Laird, B.; Colvin, L.; Fallon, M. Management of Cancer Pain: Basic Principles and Neuropathic Cancer Pain. Eur. J. Cancer 2008, 44, 1078–1082. [Google Scholar] [CrossRef] [PubMed]
- Vadalouca, A.; Raptis, E.; Moka, E.; Zis, P.; Sykioti, P.; Siafaka, I. Pharmacological Treatment of Neuropathic Cancer Pain: A Comprehensive Review of the Current Literature. Pain. Pract. 2012, 12, 219–251. [Google Scholar] [CrossRef]
- Shkodra, M.; Caraceni, A. Treatment of Neuropathic Pain Directly due to Cancer: An Update. Cancers 2022, 14, 1992. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpaa, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for Neuropathic Pain in Adults: Systematic Review, Meta-Analysis and Updated NeuPSIG Recommendations. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Sałat, K. Chemotherapy-Induced Peripheral Neuropathy: Part 1—Current State of Knowledge and Perspectives for Pharmacotherapy. Pharmacol. Rep. 2020, 72, 486–507. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Lacchetti, C.; Dworkin, R.H.; Lavoie Smith, E.M.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Gavin, P.; Lavino, A.; Lustberg, M.B.; et al. Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2014, 32, 1941–1967. [Google Scholar] [CrossRef]
- Wang, C.; Chen, S.; Jiang, W. Treatment for Chemotherapy-Induced Peripheral Neuropathy: A Systematic Review of Randomized Control Trials. Front. Pharmacol. 2022, 13, 1080888. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.C.; Lewis, R.J. Sodium Channels and Pain: From Toxins to Therapies. Br. J. Pharmacol. 2018, 175, 2138–2157. [Google Scholar] [CrossRef]
- Lago, J.; Rodríguez, L.P.; Blanco, L.; Vieites, J.M.; Cabado, A.G. Tetrodotoxin, an Extremely Potent Marine Neurotoxin: Distribution, Toxicity, Origin and Therapeutical Uses. Mar. Drugs 2015, 13, 6384–6406. [Google Scholar] [CrossRef] [PubMed]
- Nieto, F.R.; Cobos, E.J.; Tejada, M.Á.; Sánchez-Fernández, C.; González-Cano, R.; Cendán, C.M. Tetrodotoxin (TTX) as a Therapeutic Agent for Pain. Mar. Drugs 2012, 10, 281–305. [Google Scholar] [CrossRef]
- de Lera Ruiz, M.; Kraus, R.L. Voltage-Gated Sodium Channels: Structure, Function, Pharmacology, and Clinical Indications. J. Med. Chem. 2015, 58, 7093–7118. [Google Scholar] [CrossRef]
- Marcil, J.; Walczak, J.-S.; Guindon, J.; Ngoc, A.H.; Lu, S.; Beaulieu, P. Antinociceptive Effects of Tetrodotoxin (TTX) in Rodents. Br. J. Anaesth. 2006, 96, 761–768. [Google Scholar] [CrossRef]
- Alguacil, L.F.; Pérez-García, C.; Salas, E.; González-Martín, C.; Castillo, C.; Polanco, M.J.; Herradón, G.; Morales, L. Subcutaneous Tetrodotoxin and Inflammatory Pain. Br. J. Anaesth. 2008, 100, 729–730. [Google Scholar] [CrossRef]
- González-Cano, R.; Tejada, M.Á.; Artacho-Cordón, A.; Nieto, F.R.; Entrena, J.M.; Wood, J.N.; Cendán, C.M. Effects of Tetrodotoxin in Mouse Models of Visceral Pain. Mar. Drugs 2017, 15, 188. [Google Scholar] [CrossRef]
- Kayser, V.; Viguier, F.; Ioannidi, M.; Bernard, J.-F.; Latrémolière, A.; Michot, B.; Vela, J.-M.; Buschmann, H.; Hamon, M.; Bourgoin, S. Differential Anti-Neuropathic Pain Effects of Tetrodotoxin in Sciatic Nerve- versus Infraorbital Nerve-Ligated Rats--Behavioral, Pharmacological and Immunohistochemical Investigations. Neuropharmacology 2010, 58, 474–487. [Google Scholar] [CrossRef]
- Hong, B.; Sun, J.; Zheng, H.; Le, Q.; Wang, C.; Bai, K.; He, J.; He, H.; Dong, Y. Effect of Tetrodotoxin Pellets in a Rat Model of Postherpetic Neuralgia. Mar. Drugs 2018, 16, 195. [Google Scholar] [CrossRef]
- Nieto, F.R.; Entrena, J.M.; Cendán, C.M.; Del Pozo, E.; Vela, J.M.; Baeyens, J.M. Tetrodotoxin Inhibits the Development and Expression of Neuropathic Pain Induced by Paclitaxel in Mice. Pain 2008, 137, 520–531. [Google Scholar] [CrossRef]
- Alvarez, P.; Levine, J.D. Antihyperalgesic Effect of Tetrodotoxin in Rat Models of Persistent Muscle Pain. Neuroscience 2015, 311, 499–507. [Google Scholar] [CrossRef]
- Zheng, Q.; Fang, D.; Cai, J.; Wan, Y.; Han, J.-S.; Xing, G.-G. Enhanced Excitability of Small Dorsal Root Ganglion Neurons in Rats with Bone Cancer Pain. Mol. Pain 2012, 8, 24. [Google Scholar] [CrossRef] [PubMed]
- González-Cano, R.; Ruiz-Cantero, M.C.; Santos-Caballero, M.; Gómez-Navas, C.; Tejada, M.Á.; Nieto, F.R. Tetrodotoxin, a Potential Drug for Neuropathic and Cancer Pain Relief? Toxins 2021, 13, 483. [Google Scholar] [CrossRef]
- Hagen, N.A.; Fisher, K.M.; Lapointe, B.; du Souich, P.; Chary, S.; Moulin, D.; Sellers, E.; Ngoc, A.H.; Canadian Tetrodotoxin Study Group. An Open-Label, Multi-Dose Efficacy and Safety Study of Intramuscular Tetrodotoxin in Patients with Severe Cancer-Related Pain. J. Pain Symptom. Manag. 2007, 34, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Hagen, N.A.; du Souich, P.; Lapointe, B.; Ong-Lam, M.; Dubuc, B.; Walde, D.; Love, R.; Ngoc, A.H. Tetrodotoxin for Moderate to Severe Cancer Pain: A Randomized, Double Blind, Parallel Design Multicenter Study. J. Pain Symptom. Manag. 2008, 35, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Hagen, N.A.; Lapointe, B.; Ong–Lam, M.; Dubuc, B.; Walde, D.; Gagnon, B.; Love, R.; Goel, R.; Hawley, P.; Ngoc, A.H.; et al. A Multicentre Open-Label Safety and Efficacy Study of Tetrodotoxin for Cancer Pain. Curr. Oncol. 2011, 18, e109–e116. [Google Scholar] [CrossRef]
- Hagen, N.A.; Cantin, L.; Constant, J.; Haller, T.; Blaise, G.; Ong-Lam, M.; du Souich, P.; Korz, W.; Lapointe, B. Tetrodotoxin for Moderate to Severe Cancer-Related Pain: A Multicentre, Randomized, Double-Blind, Placebo-Controlled, Parallel-Design Trial. Pain Res. Manag. 2017, 2017, 7212713. [Google Scholar] [CrossRef]
- Goldlust, S.A.; Kavoosi, M.; Nezzer, J.; Kavoosi, M.; Korz, W.; Deck, K. Tetrodotoxin for Chemotherapy-Induced Neuropathic Pain: A Randomized, Double-Blind, Placebo-Controlled, Parallel-Dose Finding Trial. Toxins 2021, 13, 235. [Google Scholar] [CrossRef]
- Li, Y.; North, R.Y.; Rhines, L.D.; Tatsui, C.E.; Rao, G.; Edwards, D.D.; Cassidy, R.M.; Harrison, D.S.; Johansson, C.A.; Zhang, H.; et al. DRG Voltage-Gated Sodium Channel 1.7 Is Upregulated in Paclitaxel-Induced Neuropathy in Rats and in Humans with Neuropathic Pain. J. Neurosci. 2018, 38, 1124–1136. [Google Scholar] [CrossRef]
- Li, L.; Shao, J.; Wang, J.; Liu, Y.; Zhang, Y.; Zhang, M.; Zhang, J.; Ren, X.; Su, S.; Li, Y.; et al. MiR-30b-5p Attenuates Oxaliplatin-Induced Peripheral Neuropathic Pain through the Voltage-Gated Sodium Channel Nav1.6 in Rats. Neuropharmacology 2019, 153, 111–120. [Google Scholar] [CrossRef]
- Tseng, T.-J.; Hsieh, Y.-L.; Ko, M.-H.; Hsieh, S.-T. Redistribution of Voltage-Gated Sodium Channels after Nerve Decompression Contributes to Relieve Neuropathic Pain in Chronic Constriction Injury. Brain Res. 2014, 1589, 15–25. [Google Scholar] [CrossRef]
- Zhang, Q.; Martin-Caraballo, M.; Hsia, S.V. Modulation of Voltage-Gated Sodium Channel Activity in Human Dorsal Root Ganglion Neurons by Herpesvirus Quiescent Infection. J. Virol. 2020, 94, e01823-19. [Google Scholar] [CrossRef] [PubMed]
- Black, J.A.; Cummins, T.R.; Plumpton, C.; Chen, Y.H.; Hormuzdiar, W.; Clare, J.J.; Waxman, S.G. Upregulation of a Silent Sodium Channel after Peripheral, but Not Central, Nerve Injury in DRG Neurons. J. Neurophysiol. 1999, 82, 2776–2785. [Google Scholar] [CrossRef] [PubMed]
- Black, J.A.; Nikolajsen, L.; Kroner, K.; Jensen, T.S.; Waxman, S.G. Multiple Sodium Channel Isoforms and Mitogen-Activated Protein Kinases Are Present in Painful Human Neuromas. Ann. Neurol. 2008, 64, 644–653. [Google Scholar] [CrossRef] [PubMed]
- Coward, K.; Aitken, A.; Powell, A.; Plumpton, C.; Birch, R.; Tate, S.; Bountra, C.; Anand, P. Plasticity of TTX-Sensitive Sodium Channels PN1 and Brain III in Injured Human Nerves. Neuroreport 2001, 12, 495–500. [Google Scholar] [CrossRef]
- Lindia, J.A.; Köhler, M.G.; Martin, W.J.; Abbadie, C. Relationship between Sodium Channel NaV1.3 Expression and Neuropathic Pain Behavior in Rats. Pain 2005, 117, 145–153. [Google Scholar] [CrossRef]
- Zimmer, T.; Haufe, V.; Blechschmidt, S. Voltage-Gated Sodium Channels in the Mammalian Heart. Glob. Cardiol. Sci. Pract. 2014, 2014, 449–463. [Google Scholar] [CrossRef]
- Kavoosi, M.; O’Reilly, T.E.; Kavoosi, M.; Chai, P.; Engel, C.; Korz, W.; Gallen, C.C.; Lester, R.M. Safety, Tolerability, Pharmacokinetics, and Concentration-QTc Analysis of Tetrodotoxin: A Randomized, Dose Escalation Study in Healthy Adults. Toxins 2020, 12, 511. [Google Scholar] [CrossRef]
- Seide, S.E.; Röver, C.; Friede, T. Likelihood-Based Random-Effects Meta-Analysis with Few Studies: Empirical and Simulation Studies. BMC Med. Res. Methodol. 2019, 19, 16. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-Bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-Bias Assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study/Clinical Phase/Condition | Number/Country | Administration/ Doses | Efficacy in Primary Outcome | Secondary Outcomes |
|---|---|---|---|---|
| Hagen et al., 2007 [38] Phase IIa SCP | 24 Canada | i.m. injections/ 4 days of 7.5, 15, 22.5, and 30 μg BID or 30 μg TID | In total, 17 of 31 (54.85%) patients had a ≥33% reduction in the intensity of the worst, average, or current pain for at least two consecutive days. | For BPI#9A (general activity), 13 responders and 4 non-responders improved. For BPI#9G (enjoyment of life), 12 responders and 0 non-responders improved. |
| Hagen et al., 2008 [39] MSCP | 82 Canada | s.c. injections/ 4 days of 30 μg BID or placebo | In total, 16 of 38 (42%) patients in the TTX arm and 12 of 39 (31%) patients in the placebo arm were responders. | Improvements in pain or significant reductions in opioid use, along with improvements in QoL, were observed in 17 of 38 (45%) responders to TTX and 8 of 39 (21%) responders to placebo. The duration of analgesia was 19.5 days in the intervention group versus 14.3 in the placebo group (NNT: 4.2). |
| Hagen et al., 2011 [40] MSCP | 45 Canada | s.c. injections/ 4 days of 30 μg BID | There were 16 (39%) responders, 5 (12%) clinical responders, and 20 (49%) non-responders to TTX in treatment cycle 1. In subsequent cycles, the effect on pain did not change. | After the first cycle of TTX at 30 μg BID for 4 days, pain relief lasted, on average, 21 days. The average duration of pain relief remained at about 20 days for all subsequent cycles. |
| Hagen et al., 2017 [41] Phase III MSCP | 165 Australia, Canada, and NZ | s.c. injections/ 4 days of 30 μg BID or placebo | In total, 33 (50.8%) patients who received TTX and 29 (34.5%) patients who received a placebo were responders. | When adding QoL to the analysis, the proportions of responders to treatment with TTX during EPIP or LPIP were not statistically significant. The duration of the analgesic response was 56.7 days in the intervention group versus 9.9 days in the placebo group (NNT: 6.2). |
| Goldlust et al., 2021 [42] Phase II CINP | 125 USA | s.c. injections/ 4 days of 7.5, 15, and 30 μg BID, 30 μg QD, or placebo | Numbers of responders: 7.5 µg BID: 9 (36.0%), 15 µg BID: 11 (45.8%), 30 µg QD: 10 (40.0%), 30 µg BID: 15 (57.7%), and placebo: 8 (32.0%). | On day 28, there were benefits of TTX at 15 μg BID and 30 μg BID on all outcome subscales of the SF-36 and the sensory and motor nerve function subscales of the EORTC CIPN20. |
| Study | Mild Adverse Events | Severe Adverse Events |
|---|---|---|
| Hagen et al., 2007 [38] Phase IIa SCP | All 24 subjects in the 31 treatments experienced AEs (531 reported). Approximately 98% of the total were rated as mild, with paresthesia and hypesthesia the most repeated, followed by nausea. These AEs appeared to increase in frequency in a dose-dependent manner. | AEs in the 30 µg TID dose group led to three patients discontinuing treatment partway through the four-day treatment period and a subsequent decision to discontinue further dose escalation. One of these AEs was an episode of severe ataxia after the seventh injection of TTX, which resolved within 24 h. |
| Hagen et al., 2008 [39] MSCP | In total, 648 of 690 AEs were considered mild or moderate, and 38 of 41 patients in the TTX group presented one or more AEs (92.7%). Overall, treatment-emergent AEs were greater in the TTX arm than in the placebo arm, but almost all were mild and related to tingling, numbness, or other transient sensory symptoms. | Three patients discontinued TTX (1) due to moderately severe but transient ataxia; (2) due to the development of malignant epidural spinal cord compression; or (3) due to the development of transient moderate dysphagia with a 3½ h duration that was probably related to the studied drug. |
| Hagen et al., 2011 [40] MSCP | Most AEs were described as mild (82%) or moderate (13%) in severity; all were well tolerated and had short durations (from 20 min to 1 h). Close to half of the patients described mild peri-oral tingling or numbness. Transient nausea was also reported by approximately one third of patients. | Four serious AEs were reported. Only one was related to the studied drug. The patient started taking the studied drug at a dose of 30 μg BID, and an hour after the second dose on day 1, she experienced hypertension and dizziness. Both events resolved the same day, and the patient was discharged. |
| Hagen et al., 2017 [41] Phase III MSCP | AEs were generally mild to moderate and transient. In the TTX group, all 77 patients experienced at least one AE that was considered drug-related. The most common were nausea, dizziness, oral numbness/tingling, and injection site irritation. | There were 12 serious AEs. Five AEs that occurred in three patients were probably related to TTX: ataxia (2), nystagmus (1), other neurotoxicity (1), and aspiration pneumonia (1). The aspiration pneumonia occurred in a patient who was at risk of aspiration. |
| Goldlust et al., 2021 [42] Phase II CINP | Across the TTX cohorts, 80.0 to 92.3% of the patients experienced at least one AE. The most frequent were oral paresthesia (34/100 TTX patients) and oral hypesthesia (28/100 TTX patients). Other common AEs were headache (19/100 TTX patients) and nausea (13/100 TTX patients). | Four patients had serious AEs, three of which were possibly related to treatment (hypertension, paresthesia, extremity pain, and a burning sensation). Two patients withdrew due to AEs: one patient with moderate vertigo and another with vertigo and an influenza-like illness, which were possibly related. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huerta, M.Á.; de la Nava, J.; Artacho-Cordón, A.; Nieto, F.R. Efficacy and Security of Tetrodotoxin in the Treatment of Cancer-Related Pain: Systematic Review and Meta-Analysis. Mar. Drugs 2023, 21, 316. https://doi.org/10.3390/md21050316
Huerta MÁ, de la Nava J, Artacho-Cordón A, Nieto FR. Efficacy and Security of Tetrodotoxin in the Treatment of Cancer-Related Pain: Systematic Review and Meta-Analysis. Marine Drugs. 2023; 21(5):316. https://doi.org/10.3390/md21050316
Chicago/Turabian StyleHuerta, Miguel Á., Javier de la Nava, Antonia Artacho-Cordón, and Francisco R. Nieto. 2023. "Efficacy and Security of Tetrodotoxin in the Treatment of Cancer-Related Pain: Systematic Review and Meta-Analysis" Marine Drugs 21, no. 5: 316. https://doi.org/10.3390/md21050316
APA StyleHuerta, M. Á., de la Nava, J., Artacho-Cordón, A., & Nieto, F. R. (2023). Efficacy and Security of Tetrodotoxin in the Treatment of Cancer-Related Pain: Systematic Review and Meta-Analysis. Marine Drugs, 21(5), 316. https://doi.org/10.3390/md21050316