Strengthening Preparedness for Arbovirus Infections in Mediterranean and Black Sea Countries: A Conceptual Framework to Assess Integrated Surveillance in the Context of the One Health Strategy

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria for Articles and Gray Literature
- were published in scientific peer-reviewed journals and gray literature for the period 2000–2014;
- were in English, French, or Italian;
- focused on descriptive/analytical epidemiology and surveillance evaluation;
- analyzed the functioning of public health surveillance systems for West Nile virus (WNV), chikungunya virus (CHKV), dengue virus (DENV), and Rift Valley fever virus (RVFV);
- reported integration between sectors.
2.2. Search Strategy and Data Extraction for Articles
2.3. Search Strategy and Data Extraction for the Gray Literature
2.4. Analysis
3. Results
3.1. Scientific Literature
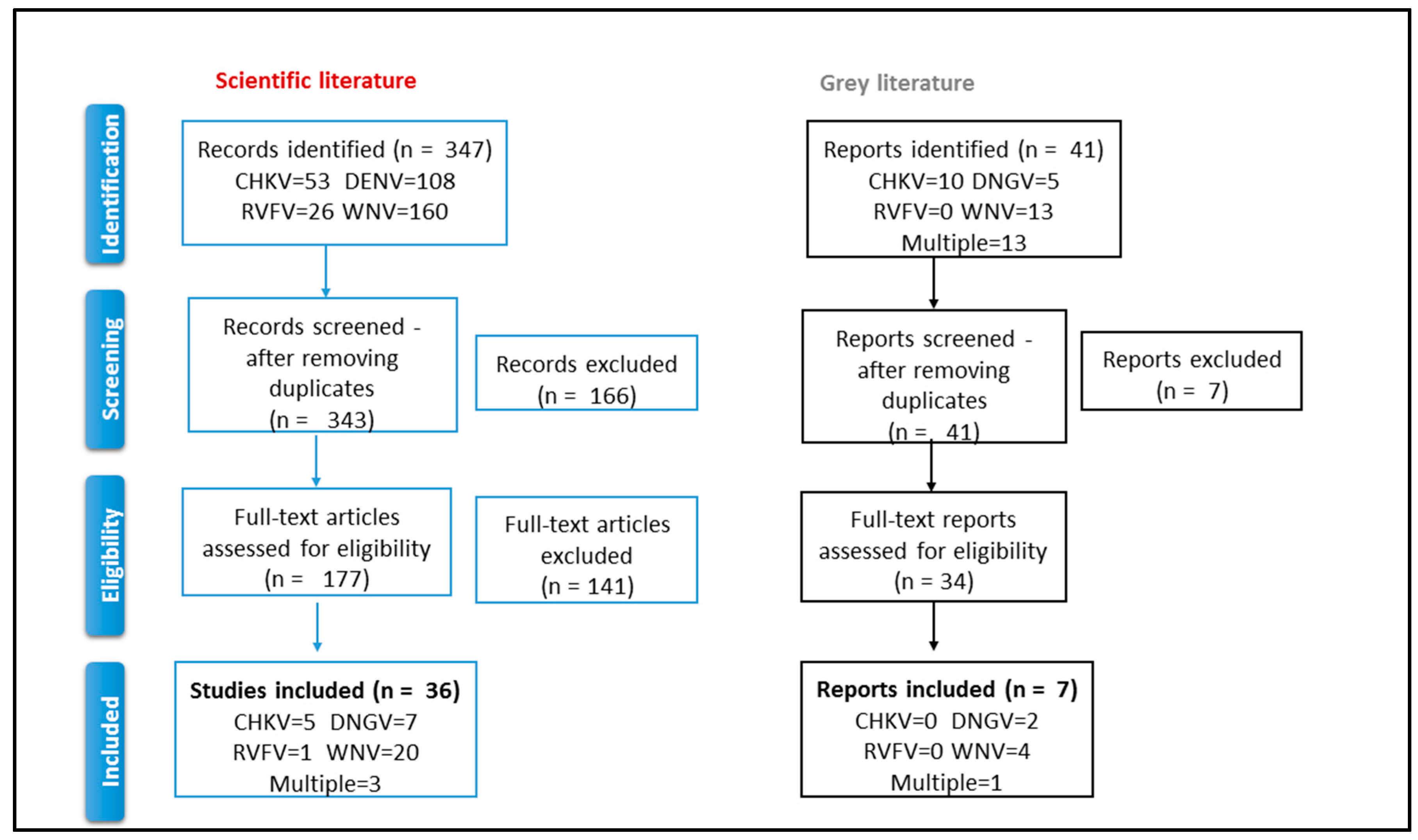
3.1.1. The Selection Process
3.1.2. The Integration between Sectors
3.1.3. The Level of Integration
3.2. The Gray Literature Reports
3.2.1. The Selection Process
3.2.2. The Integration between Sectors
3.2.3. The Level of Integration
3.3. Lessons Learned from the Articles and Documents
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Rushton, J.; Häsler, B.; De Haan, N.; Rushton, R. Economic benefits or drivers of a “One Health” approach: Why should anyone invest? Onderstepoort J. Vet. Res. 2012, 79, 5. [Google Scholar] [CrossRef] [PubMed]
- IOM (Institute of Medicine). Emerging Viral Diseases: The One Health Connection; The National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Torres-Vélez, F.; Brown, C. Emerging infections in animals—Potential new zoonoses? Clin. Lab. Med. 2004, 24, 825–828. [Google Scholar] [CrossRef] [PubMed]
- One Health Initiative. Available online: http://www.onehealthinitiative.com/index.php (accessed on 15 December 2017).
- Kahn, L.H. Confronting zoonoses, linking human and veterinary medicine. Emerg. Infect. Dis. 2006, 12, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Häsler, B.; Gilbert, W.; Jones, B.A.; Pfeiffer, D.U.; Rushton, J.; Otte, M.J. The Economic Value of One Health in Relation to the Mitigation of Zoonotic Disease Risks. Curr. Top. Microbiol. Immunol. 2012, 365, 127–151. [Google Scholar] [CrossRef]
- Faburay, B. The case for a ‘One Health’ approach to combating vector-borne diseases. Infect. Ecol. Epidemiol. 2015, 5, 28132. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, M.; Dobler, G. Emergence of zoonotic arboviruses by animal trade and migration. Parasites Vectors 2010, 3, 35. [Google Scholar] [CrossRef] [PubMed]
- Morens, D.M.; Fauci, A.S. Emerging infectious diseases: Threats to human health and global stability. PLoS Pathog. 2013, 9, e1003467. [Google Scholar] [CrossRef] [PubMed]
- Bueno-Marí, R.; Almeida, A.P.G.; Navarro, J.C. Editorial: Emerging zoonoses: Eco-epidemiology, involved mechanisms, and public health implications. Front. Public Health 2015, 3, 157. [Google Scholar] [CrossRef] [PubMed]
- Conrad, P.A.; Meek, L.A.; Dumit, J. Operationalizing a One Health approach to global health challenges. Comp. Immunol. Microbiol. Infect. Dis. 2013, 36, 211–216. [Google Scholar] [CrossRef] [PubMed]
- One Health Commission. Available online: https://www.onehealthcommission.org (accessed on 15 December 2017).
- ProMED Mail. Available online: http://www.promedmail.org (accessed on 21 December 2017).
- GlobalHealth.gov-Global Programs & Initiatives. Available online: http://www.globalhealth.gov/global-programs-and-initiatives/one-health/index.html (accessed on 21 December 2017).
- Decision No 1082/2013/EU of the European Parliament and of the Council of 22 October 2013 on Serious Cross-Border Threats to Health and Repealing Decision No 2119/98/EC; Official Journal of the European: Luxembourg, 2013.
- Grace, D. The business case for One Health. Onderstepoort J. Vet. Res. 2014, 81, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcotty, T.; Thys, E.; Conrad, P.; Godfroid, J.; Craig, P.; Zinsstag, J.; Meheus, F.; Boukary, A.R.; Badé, M.A.; Sahibi, H.; et al. Intersectoral collaboration between the medical and veterinary professions in low-resource societies: The role of research and training institutions. Comp. Immunol. Microbiol. Infect. Dis. 2013, 36, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Kock, R. Structural One Health—Are We There Yet? Vet. Rec. 2015, 176, 140–142. [Google Scholar] [CrossRef] [PubMed]
- Queenan, K.; Häsler, B.; Rushton, J. A One Health approach to antimicrobial resistance surveillance: Is there a business case for it? Int. J. Antimicrob. Agents 2016. [Google Scholar] [CrossRef] [PubMed]
- Zinsstag, J.; Schelling, E.; Waltner-Toews, D.; Tanner, M. From “one medicine” to “one health” and systemic approaches to health and well-being. Prev. Vet. Med. 2011, 101, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Stärk, K.D.C.; Arroyo Kuribreña, M.; Dauphin, G.; Vokaty, S.; Ward, M.P.; Wieland, B.; Lindberg, A. One Health surveillance—More than a buzz word? Prev. Vet. Med. 2015, 120, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Napoli, C.; Bella, A.; Declich, S.; Grazzini, G.; Lombardini, L.; Nanni Costa, A.; Nicoletti, L.; Pompa, M.G.; Pupella, S.; Russo, F.; et al. Integrated human surveillance systems of West Nile virus infections in Italy: The 2012 experience. Int. J. Environ. Res. Public Health 2013, 10, 7180–7192. [Google Scholar] [CrossRef] [PubMed]
- Goutard, F.L.; Binot, A.; Duboz, R.; Rasamoelina-Andriamanivo, H.; Pedrono, M.; Holl, D.; Peyre, M.I.; Cappelle, J.; Chevalier, V.; Figuié, M.; et al. Surveillance: How to reach the poor? Surveillance in low-income countries, lessons from experiences in Cambodia and Madagascar. Prev. Vet. Med. 2015, 120, 12–26. [Google Scholar] [CrossRef] [PubMed]
- FAO; OIE; WHO. Four-Way Linking Project for Assessing Health Risks at the Human-Animal Interface. Project Description. August 2013. Available online: http://www.oie.int/fileadmin/Home/eng/Media_Center/docs/pdf/13_08_web_summary_4-way_linking_v7_fin_for_clearance__3_.pdf (accessed on 21 December 2017).
- GLEWS. The Joint FAO–OIE–WHO Global Early Warning System for Health Threats and Emerging Risks at the Human–Animal–Ecosystems Interface. Available online: http://www.glews.net/ (accessed on 21 December 2017).
- Network for Evaluation of One Health (NEOH). Available online: http://neoh.onehealthglobal.net/ (accessed on 5 March 2018).
- Baum, S.E.; Machalaba, C.; Daszak, P.; Salerno, R.H.; Karesh, W.B. Evaluating one health: Are we demonstrating effectiveness? One Health 2017, 3, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Rabinowitz, P.M.; Kock, R.; Kachani, M.; Kunkel, R.; Thomas, J.; Gilbert, J.; Wallace, R.; Blackmore, C.; Wong, D.; Karesh, W.; et al. Toward proof of concept of a One Health approach to disease prediction and control. Emerg. Infect. Dis. 2013. [Google Scholar] [CrossRef] [PubMed]
- Babo Martins, J.; Rushton, J.; Stärk, K.D.C. Rushton Economic Assessment of Zoonoses Surveillance in a ‘One Health’ Context: A Conceptual Framework. Zoonoses Public Health 2016, 63, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Benelli, G.; Duggan, M.F. Management of arthropod vector data—Social and ecological dynamics facing the One Health perspective. Acta Trop. 2018. [Google Scholar] [CrossRef] [PubMed]
- Dente, M.G.; Fabiani, M.; Gnesotto, R.; Putoto, G.; Montagna, C.; Simon-Soria, F.; Martin de Pando, C.; Barboza, P.; Ait-Belghiti, F.; Kojouharova, M.; et al. EpiSouth: A network for communicable disease control in the Mediterranean region and the Balkans. Euro Surveill. 2009, 14, 19113. [Google Scholar] [CrossRef] [PubMed]
- Episouth WP8 Directory of Human Public Health and Veterinary Public Health Officials for Zoonose. Available online: http://www.episouth.org/search_zoonosis.php (accessed on 21 December 2017).
- Declich, S.; Simon Soria, F.; Martin de Pando, C. EpiSouth Strategic Documents (2010). EpiSouth Report 10/2010. Available online: http://www.episouth.org/outputs/wp4/1_EpiSouth%20Strategic%20Documents_Rev%20Luglio%202010.pdf (accessed on 21 December 2017).
- Medilabsecure Project. Available online: http://medilabsecure.com (accessed on 21 December 2017).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2017, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Khan, K.S.; Kunz, R.; Kleijnen, J.; Antes, G. Five steps to conducting a systematic review. J. R. Soc. Med. Mar. 2003, 96, 118–121. [Google Scholar] [CrossRef]
- Relevo, R. Effective Search Strategies for Systematic Reviews of Medical Tests in Methods Guide for Medical Test Reviews; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2012. [Google Scholar]
- DeLuca, J.B.; Mullins, M.M.; Lyles, C.M.; Crepaz, N.; Kay, L.; Thadipharthi, S. Developing a comprehensive strategy for evidence based systematic reviews. Evid. Based Lib. Inf. Pract. 2008, 3, 3–32. [Google Scholar] [CrossRef]
- World Health Organization. Monitoring & Evaluation Indicators for Integrated Vector Management. WHO/HTM/NTD/VEM/2012.4. Available online: http://apps.who.int/iris/bitstream/10665/76504/1/9789241504027_eng.pdf (accessed on 21 December 2017).
- Dente, M.G.; Riccardo, F.; Nacca, G.; Ranghiasci, A.; Manuguerra, J.; Escadafal, C.; Jimenez-Clavero, M.A.; Ramirez, E.P.; Robert, V.; Picard, M.; et al. Strengthening Integrated Surveillance for Arboviruses in the Mediterranean and Black Sea Regions in the Framework of the One Health Approach. QUADERNI DELLA SOCIETÀ ITALIANA DI MEDICINA TROPICALE E SALUTE GLOBALE N. 1, 2016. Available online: http://www.simetweb.eu/Page/WebObjects/PageSimet.woa/wa/displayPage?name=Pubblicazioni (accessed on 5 March 2018).
- PubMED Website. Available online: http://www.ncbi.nlm.nih.gov/pubmed (accessed on 5 March 2018).
- Gobbi, F.; Capelli, G.; Angheben, A.; Giobbia, M.; Conforto, M.; Franzetti, M.; Cattelan, A.M.; Raise, E.; Rovere, P.; Mulatti, P.; et al. Human and entomological surveillance of West Nile fever, dengue and chikungunya in Veneto Region, Italy, 2010–2012. BMC Infect. Dis. 2014, 14, 60. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, C.; Salcuni, P.; Nicoletti, L.; Ciufolini, M.G.; Russo, F.; Masala, R.; Frongia, O.; Finarelli, A.C.; Gramegna, M.; Gallo, L.; et al. Epidemiological surveillance of West Nile neuroinvasive diseases in Italy, 2008 to 2011. Euro Surveill. 2012, 17, 20172. [Google Scholar] [PubMed]
- Angelini, P.; Tamba, M.; Finarelli, A.C.; Bellini, R.; Albieri, A.; Bonilauri, P.; Cavrini, F.; Dottori, M.; Gaibani, P.; Martini, E.; et al. West Nile virus circulation in Emilia-Romagna, Italy: The integrated surveillance system 2009. Euro Surveill. 2010, 15, 19547. [Google Scholar] [PubMed]
- Chaintoutis, S.C.; Dovas, C.I.; Papanastassopoulou, M.; Gewehr, S.; Danis, K.; Beck, C.; Lecollinet, S.; Antalis, V.; Kalaitzopoulou, S.; Panagiotopoulos, T.; et al. Evaluation of a West Nile virus surveillance and early warning system in Greece, based on domestic pigeons. Comp. Immunol. Microbiol. Infect. Dis. 2014, 37, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Ben Hassine, T.; Hammami, S.; Elghoul, H.; Ghram, A. Detection of circulation of West Nile virus in equine in the north-west of Tunisia. Bull. Soc. Pathol. Exot. 2011, 104, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, N.P.; Staples, J.E.; Lehman, J.A. Surveillance for human West Nile virus disease—United States, 1999–2008. MMWR Surveill. Summ. 2010, 59, 1–17. [Google Scholar] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Hadler, J.L.; Patel, D.; Bradley, K.; Hughes, J.M.; Blackmore, C.; Etkind, P.; Kan, L.; Getchell, J.; Blumenstock, J.; Engel, J. National capacity for surveillance, prevention, and control of West Nile virus and other arbovirus infections—United States, 2004 and 2012. Morb. Mortal. Wkly. Rep. 2014, 63, 281–284. [Google Scholar]
- Cito, F.; Narcisi, V.; Danzetta, M.L.; Iannetti, S.; Sabatino, D.D.; Bruno, R.; Carvelli, A.; Atzeni, M.; Sauro, F.; Calistri, P. Analysis of surveillance systems in place in European Mediterranean countries for West Nile virus (WNV) and Rift Valley fever (RVF). Transbound. Emerg. Dis. 2013, 60 (Suppl. 2), 40–44. [Google Scholar] [CrossRef] [PubMed]
- Krisztalovics, K.; Ferenczi, E.; Molnar, Z.; Csohan, A.; Ban, E.; Zoldi, V.; Kaszas, K. West Nile virus infections in Hungary, August–September 2008. Euro Surveill. 2008, 13, 19030. [Google Scholar]
- Hernández-Ávila, J.E.; Rodríguez, M.H.; Santos-Luna, R.; Sánchez-Castañeda, V.; Román-Pérez, S.; Ríos-Salgado, V.H.; Salas-Sarmiento, J.A. Nation-wide, web-based, geographic information system for the integrated surveillance and control of dengue fever in Mexico. PLoS ONE 2013, 8, e70231. [Google Scholar] [CrossRef] [PubMed]
- Vrbova, L.; Stephen, C.; Kasman, N.; Boehnke, R.; Doyle-Waters, M.; Chablitt-Clark, A.; Gibson, B.; FitzGerald, M.; Patrick, D.M. Systematic Review of Surveillance Systems for Emerging Zoonoses. Transbound. Emerg. Dis. 2010, 57, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Halliday, J.; Cleaveland, S.; Auty, H.; Hampson, K.; Mtema, Z.; Bronsvoort, M.; Breiman, R. Surveillance and Monitoring of Zoonoses: Report for the Department for International Development; Project Report; Department for International Development, University of Glasgow: Glasgow, UK, 2011. [Google Scholar]
- Wendt, A.; Kreienbrock, L.; Campe, A. Zoonotic Disease Surveillance—Inventory of Systems Integrating Human and Animal Disease. Inf. Zoonoses Public Health 2015, 62, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Häsler, B.; Cornelsen, L.; Bennani, H.; Rushton, J. A review of the metrics for One Health benefits. Rev. Sci. Tech. 2014, 33, 453–464. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Level of Integration | Sublevels of Integration | Criteria |
|---|---|---|
| Policy and institutional | Policy | 1. Existence of a national policy addressing integrated surveillance for a specific pathogen |
| 2. Existence of a policy addressing integrated surveillance for a specific pathogen at subnational level | ||
| Institutional | 3. Existence of agreements among the institutions involved in human/animal/entomological surveillance for the specific pathogen | |
| 4. Existence of coordination mechanisms among the institutions involved | ||
| 5. Existence of identified focal points for each human/animal/entomological surveillance for the specific pathogen | ||
| Data collection and analysis | Interoperability mechanisms at data collection | 6. Existence of integrated data collection tools |
| 7. Existence of activation mechanisms of human surveillance based on signals from animal/entomological surveillance | ||
| 8. Other interoperability mechanisms at data collection level | ||
| Interoperability mechanisms at data analysis | 9. Presence of database exchange/merging/other mechanisms to facilitate joint analysis among sectors. | |
| 10. Performance of joint/integrated data analysis among the different surveillance sectors | ||
| 11. Other interoperability mechanisms at data analysis level | ||
| Dissemination | - | 12. Existence of joint results dissemination mechanisms (e.g., bulletins, reports, papers, media reports, websites, etc.) |
| Search Axes | Description |
|---|---|
| Intervention | Surveillance of a viral Vector Born Diseases (VBDs) that integrates human virology, animal virology and/or medical entomology components |
| Outcome | Models of integrated surveillance for this viral VBDs |
| Exposure | West Nile virus (WNV) |
| chikungunya virus (CHKV) | |
| dengue virus (DENV) | |
| Rift Valley fever virus (RVFV) |
| Common Root | Exposure Disease | Strings |
|---|---|---|
| Intervention and Outcome | West Nile virus (WNV) | Common root and WNV |
| chikungunya virus (CHKV) | Common root and CHKV | |
| dengue virus (DENV) | Common root and DENV | |
| Rift Valley fever virus (RVFV) | Common root and RVFV |
| Sectors | Pathogen | |||||
|---|---|---|---|---|---|---|
| CHKV | DENV | Multi | RVFV | WNV | Total | |
| human and entomological | 5 | 4 | 2 | 0 | 1 | 12 |
| human and animal | 0 | 0 | 1 | 1 | 4 | 6 |
| human and animal and entomological | 0 | 0 | 0 | 0 | 12 | 12 |
| human and entomological and environmental | 0 | 2 | 0 | 0 | 0 | 2 |
| human and animal and entomological and environmental | 0 | 0 | 0 | 0 | 3 | 3 |
| Total | 5 | 6 | 3 | 1 | 20 | 35 |
| Sectors | Pathogen | |||||
|---|---|---|---|---|---|---|
| CHKV | DENV | Multi | RVFV | WNV | Total | |
| policy and institutional level | 0 | 0 | 1 | 0 | 1 | 2 |
| data collection and analysis level | 0 | 3 | 0 | 0 | 0 | 3 |
| data collection and analysis and dissemination levels | 2 | 1 | 0 | 0 | 3 | 6 |
| policy and institutional and data collection and analysis levels | 1 | 0 | 0 | 0 | 0 | 1 |
| policy and institutional and data collection and analysis and dissemination levels | 2 | 1 | 1 | 0 | 11 | 15 |
| Total | 5 | 7 | 3 | 1 | 20 | 27 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dente, M.G.; Riccardo, F.; Nacca, G.; Ranghiasci, A.; Escadafal, C.; Gaayeb, L.; Jiménez-Clavero, M.A.; Manuguerra, J.-C.; Picard, M.; Fernández-Pinero, J.; et al. Strengthening Preparedness for Arbovirus Infections in Mediterranean and Black Sea Countries: A Conceptual Framework to Assess Integrated Surveillance in the Context of the One Health Strategy. Int. J. Environ. Res. Public Health 2018, 15, 489. https://doi.org/10.3390/ijerph15030489
Dente MG, Riccardo F, Nacca G, Ranghiasci A, Escadafal C, Gaayeb L, Jiménez-Clavero MA, Manuguerra J-C, Picard M, Fernández-Pinero J, et al. Strengthening Preparedness for Arbovirus Infections in Mediterranean and Black Sea Countries: A Conceptual Framework to Assess Integrated Surveillance in the Context of the One Health Strategy. International Journal of Environmental Research and Public Health. 2018; 15(3):489. https://doi.org/10.3390/ijerph15030489
Chicago/Turabian StyleDente, Maria Grazia, Flavia Riccardo, Gloria Nacca, Alessia Ranghiasci, Camille Escadafal, Lobna Gaayeb, Miguel Angel Jiménez-Clavero, Jean-Claude Manuguerra, Marie Picard, Jovita Fernández-Pinero, and et al. 2018. "Strengthening Preparedness for Arbovirus Infections in Mediterranean and Black Sea Countries: A Conceptual Framework to Assess Integrated Surveillance in the Context of the One Health Strategy" International Journal of Environmental Research and Public Health 15, no. 3: 489. https://doi.org/10.3390/ijerph15030489
APA StyleDente, M. G., Riccardo, F., Nacca, G., Ranghiasci, A., Escadafal, C., Gaayeb, L., Jiménez-Clavero, M. A., Manuguerra, J. -C., Picard, M., Fernández-Pinero, J., Pérez-Ramírez, E., Robert, V., Victoir, K., & Declich, S. (2018). Strengthening Preparedness for Arbovirus Infections in Mediterranean and Black Sea Countries: A Conceptual Framework to Assess Integrated Surveillance in the Context of the One Health Strategy. International Journal of Environmental Research and Public Health, 15(3), 489. https://doi.org/10.3390/ijerph15030489