Sociodemographic Factors Influencing the Use of eHealth in People with Chronic Diseases


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
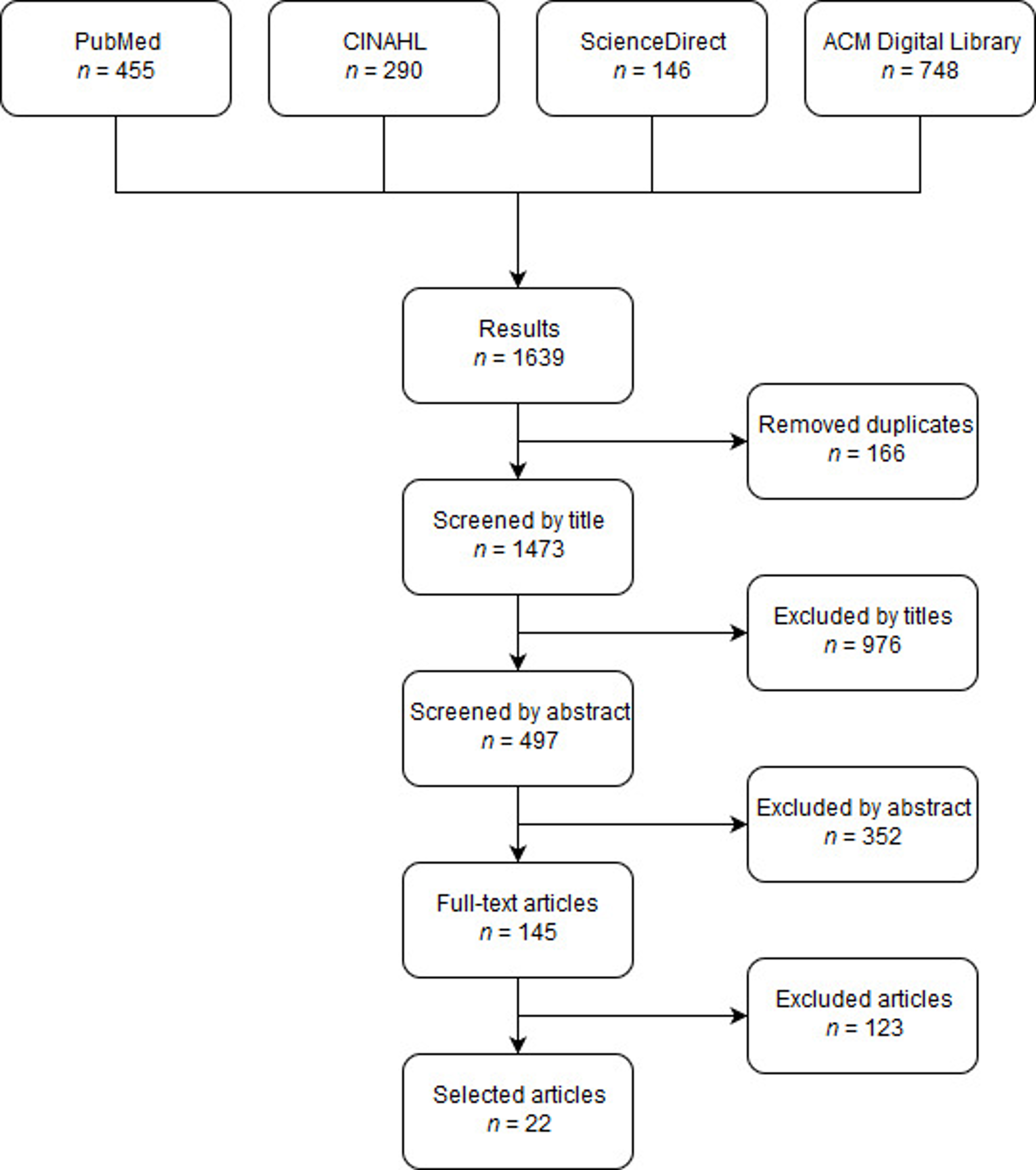
2.2. Article Selection
2.3. Data Extraction
2.4. Assessment of Methodological Quality
2.5. Data Analysis
3. Results
3.1. Quality of Included Articles
3.2. General Findings in the Selected Articles
3.3. Sociodemographic Factors
3.3.1. Age
3.3.2. Gender
3.3.3. Income
3.3.4. Education
3.3.5. Vocational Status
3.3.6. Ethnicity
3.3.7. Place of Residence
3.4. Suggested Directions for Interventions
3.4.1. Personalization of eHealth; Different Ways of Information Delivery
3.4.2. Facilitate Access to Internet; Use of Different Devices and Modes of Delivery
3.4.3. Inclusion of Family Members
3.4.4. Complementary Remarks Considering Improvement of Uptake of eHealth
4. Discussion
4.1. Summary of the Main Results
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases (NCDs) and Mental Health Challenges and Solutions. 2018. Available online: https://www.who.int/beat-ncds/en/ (accessed on 5 December 2018).
- United Nations, Department of Economic and Social Affairs. World Population Prospects: The 2015 Revision, Key Findings and Advance Tables; United Nations, Department of Economic and Social Affairs: New York, NY, USA, 2015. [Google Scholar]
- Tremmel, M.; Gerdtham, U.-G.; Nilsson, P.; Saha, S. Economic burden of obesity: A systematic literature review. Int. J. Environ. Res. Public Health 2017, 14, 435. [Google Scholar] [CrossRef] [PubMed]
- Gheorghe, A.; Griffiths, U.; Murphy, A.; Legido-Quigley, H.; Lamptey, P.; Perel, P. The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: A systematic review. BMC Public Health 2018, 18, 975. [Google Scholar] [CrossRef] [PubMed]
- Settumba, S.N.; Sweeney, S.; Seeley, J.; Biraro, S.; Mutungi, G.; Munderi, P.; Grosskurth, H.; Vassall, A. The health system burden of chronic disease care: An estimation of provider costs of selected chronic diseases in Uganda. Trop. Med. Int. Health 2015, 20, 781–790. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable diseases. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 5 December 2018).
- Shrivastava, S.; Shrivastava, P.; Ramasamy, J. Role of self-care in management of diabetes mellitus. J. Diabetes Metab. Disord. 2013, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Talboom-Kamp, E.P.W.A.; Verdijk, N.A.; Kasteleyn, M.J.; Numans, M.E.; Chavannes, N.H. From chronic disease management to person-centered eHealth; A review on the necessity for blended care. Clin. eHealth 2018, 1, 3–7. [Google Scholar] [CrossRef]
- Forkner-Dunn, J. Internet-based patient self-care: The next generation of health care delivery. J. Med. Internet Res. 2003, 5, e8. [Google Scholar] [CrossRef] [PubMed]
- Samoocha, D.; Bruinvels, D.J.; Elbers, N.A.; Anema, J.R.; van der Beek, A.J. Effectiveness of web-based interventions on patient empowerment: A systematic review and meta-analysis. J. Med. Internet Res. 2010, 12, e23. [Google Scholar] [CrossRef] [PubMed]
- Murray, E.; Burns, J.; See Tai, S.; Lai, R.; Nazareth, I. Interactive health communication applications for people with chronic disease. Cochrane Database Syst. Rev. 2005, 4. [Google Scholar] [CrossRef] [PubMed]
- Tistad, M.; Lundell, S.; Wiklund, M.; Nyberg, A.; Holmner, Å.; Wadell, K. Usefulness and relevance of an eHealth tool in supporting the self-management of chronic obstructive pulmonary disease: Explorative qualitative study of a cocreative process. JMIR Hum. Factors 2018, 5, e10801. [Google Scholar] [CrossRef] [PubMed]
- Stellefson, M.; Chaney, B.; Barry, A.E.; Chavarria, E.; Tennant, B.; Walsh-Childers, K.; Sriram, P.; Zagora, J. Web 2.0 chronic disease self-management for older adults: A systematic review. J. Med. Internet Res. 2013, 15, e35. [Google Scholar] [CrossRef] [PubMed]
- Graetz, I.; Gordon, N.; Fung, V.; Hamity, C.; Reed, M.E. The Digital divide and patient portals: Internet access explained differences in patient portal use for secure messaging by age, race, and income. Med. Care 2016, 54, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Showell, C. Barriers to the use of personal health records by patients: A structured review. PeerJ 2017, 5, e3268. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Hong, Q.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018; McGill: Montréal, QC, Canada, 2018. [Google Scholar]
- Hofstede, J.; de Bie, J.; van Wijngaarden, B.; Heijmans, M. Knowledge, use and attitude toward eHealth among patients with chronic lung diseases. Int. J. Med. Inform. 2014, 83, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Morita, P.P.; Picton, P.; Seto, E.; Zbib, A.; Cafazzo, J.A. Uptake of a consumer-focused mHealth application for the assessment and prevention of heart disease: The <30 days study. JMIR mHealth uHealth 2016, 4, e32. [Google Scholar] [CrossRef] [PubMed]
- Kamis, K.; Janevic, M.R.; Marinec, N.; Jantz, R.; Valverde, H.; Piette, J.D. A study of mobile phone use among patients with noncommunicable diseases in La Paz, Bolivia: Implications for mHealth research and development. Glob. Health 2015, 11. [Google Scholar] [CrossRef] [PubMed]
- Anglada-Martínez, H.; Rovira-Illamola, M.; Martin-Conde, M.; Sotoca-Momblona, J.M.; Codina-Jané, C. mHealth intervention to improve medication management in chronically ill patients: Analysis of the recruitment process. Postgrad. Med. 2016, 128, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Duplaga, M. A cross-sectional study assessing determinants of the attitude to the introduction of eHealth services among patients suffering from chronic conditions. BMC Med. Inform. Decis. Mak. 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- Edwards, L.; Thomas, C.; Gregory, A.; Yardley, L.; O’Cathain, A.; Montgomery, A.A.; Salisbury, C. Are people with chronic diseases interested in using telehealth? A cross-sectional postal survey. J. Med. Internet Res. 2014, 16, e123. [Google Scholar] [CrossRef] [PubMed]
- Nelson, L.A.; Mulvaney, S.A.; Gebretsadik, T.; Ho, Y.-X.; Johnson, K.B.; Osborn, C.Y. Disparities in the use of a mHealth medication adherence promotion intervention for low-income adults with type 2 diabetes. JAMIA 2016, 23, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Pollom, E.L.; Wang, E.; Bui, T.T.; Ognibene, G.; von Eyben, R.; Divi, V.; Sunwoo, J.; Kaplan, M.; Dimitri Colevas, A.; Le, Q.-T.; et al. A prospective study of electronic quality of life assessment using tablet devices during and after treatment of head and neck cancers. Oral Oncol. 2015, 51, 1132–1137. [Google Scholar] [CrossRef] [PubMed]
- Samiei, V.; Wan Puteh, S.E.; Abdul Manaf, M.R. Are Malaysian diabetic patients ready to use the new generation of health care service delivery? A telehealth interest assessment. Malays. J. Med. Sci. 2016, 23, 44–52. [Google Scholar] [PubMed]
- Smith, R.; Menon, J.; Rajeev, J.G.; Feinberg, L.; Kumar, R.K.; Banerjee, A. Potential for the use of mHealth in the management of cardiovascular disease in Kerala: A qualitative study. BMJ Open 2015, 5, e009367–e009367. [Google Scholar] [CrossRef] [PubMed]
- Drewes, C.; Kirkovits, T.; Schiltz, D.; Schinkoethe, T.; Haidinger, R.; Goldmann-Posch, U.; Harbeck, N.; Wuerstlein, R. EHealth acceptance and new media preferences for therapy assistance among breast cancer patients. JMIR Cancer 2016, 2, e13. [Google Scholar] [CrossRef] [PubMed]
- Saied, A.; Sherry, S.J.; Castricone, D.J.; Perry, K.M.; Katz, S.C.; Somasundar, P. Age-related trends in utilization of the internet and electronic communication devices for coordination of cancer care in elderly patients. J. Geriatr. Oncol. 2014, 5, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Terschüren, C.; Mensing, M.; Mekel, O.C. Is telemonitoring an option against shortage of physicians in rural regions? Attitude towards telemedical devices in the North Rhine-Westphalian health survey, Germany. BMC Health Serv. Res. 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Jaser, S.S.; Faulkner, M.S.; Murphy, K.; Delamater, A.; Grey, M. Type 1 diabetes ehealth psychoeducation: Youth recruitment, participation, and satisfaction. J. Med. Internet Res. 2013, 15, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Rho, M.J.; Kim, H.-S.; Yoon, K.-H.; Choi, I.Y. Compliance patterns and utilization of e-health for glucose monitoring: Standalone internet gateway and tablet device. Telemed. J. E. Health 2017, 23, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Rixon, L.; Hirani, P.H.; Cartwright, M.; Beynon, M.; Selva, A.; Sanders, C.; Newman, P.S. What influences withdrawal because of rejection of telehealth – the whole systems demonstrator evaluation. J. Assist. Technol. 2013, 7, 219–227. [Google Scholar] [CrossRef]
- Sarkar, U.; Piette, J.D.; Gonzales, R.; Lessler, D.; Chew, L.D.; Reilly, B.; Johnson, J.; Brunt, M.; Huang, J.; Regenstein, M.; et al. Preferences for self-management support: Findings from a survey of diabetes patients in safety-net health systems. Patient Educ. Couns. 2008, 70, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Tatum, K.; Greene, G.; Chen, R.C. eHealth literacy and partner involvement in treatment decision making for men with newly diagnosed localized prostate cancer. Oncol. Nurs. Forum 2017, 44, 225–233. [Google Scholar] [PubMed]
- Hanberger, L.; Ludvigsson, J.; Nordfeldt, S. Use of a Web 2.0 Portal to improve education and communication in young patients with families: Randomized controlled trial. J. Med. Internet Res. 2013, 15, e175. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Sunderland, N.; Kendall, E.; Gudes, O.; Henniker, G. Professional practice and innovation: Chronic disease, geographic location and socioeconomic disadvantage as obstacles to equitable access to e-Health. Health Inf. Manag. J. 2010, 39, 30–36. [Google Scholar] [CrossRef]
- LaMonica, H.M.; English, A.; Hickie, I.B.; Ip, J.; Ireland, C.; West, S.; Shaw, T.; Mowszowski, L.; Glozier, N.; Duffy, S.; et al. Examining internet and eHealth practices and preferences: Survey study of australian older adults with subjective memory complaints, mild cognitive impairment, or dementia. J. Med. Internet Res. 2017, 19, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.; Johnson, J.; Mynatt, E.D. MyPath: Investigating breast cancer patients’ use of personalized health information. Proc. ACM Hum. Comput. Interact. 2018, 2, 1–21. [Google Scholar] [CrossRef]
- Van Deursen, A.J.A.M.; Helsper, E.J. The third-level digital divide: Who benefits most from being online? Com. Inform. Technol. Annual 2015, 29–52. [Google Scholar]


{kind=link}
| Group | Search Terms |
|---|---|
| (1) Chronic disease | “chronic diseases” OR dementia OR “Alzheimer’s disease” OR obesity OR “non-communicable disease” OR NCD OR “non-communicable condition” OR “cardiovascular disease” OR diabetes OR cancer OR “chronic respiratory disease” OR “chronic condition” OR “lung disease” OR “heart disease” OR “long-term disease” OR hypertension OR “chronic illness” |
| (2) eHealth | e-Health OR eHealth OR “electronic health” OR “electronic devices” OR “Web 2.0” OR “net health” OR “digital health technology” OR “health care information” OR “interactive health communication” OR telemonitoring OR tele-health OR mHealth OR telehealth OR telecare OR “health technology” |
| (3) Factors | factors OR barriers OR characteristics OR facilitators OR “sociodemographic factors” OR predictors OR “digital divide” OR “health inequalities” OR disparities OR inequalities |
| (4) Suggested interventions | programme OR recommendations OR recommendation OR program OR strategy OR suggestion OR implementation OR adoption OR trial OR solution OR coaching OR intervention |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reiners, F.; Sturm, J.; Bouw, L.J.W.; Wouters, E.J.M. Sociodemographic Factors Influencing the Use of eHealth in People with Chronic Diseases. Int. J. Environ. Res. Public Health 2019, 16, 645. https://doi.org/10.3390/ijerph16040645
Reiners F, Sturm J, Bouw LJW, Wouters EJM. Sociodemographic Factors Influencing the Use of eHealth in People with Chronic Diseases. International Journal of Environmental Research and Public Health. 2019; 16(4):645. https://doi.org/10.3390/ijerph16040645
Chicago/Turabian StyleReiners, Fabienne, Janienke Sturm, Lisette J.W. Bouw, and Eveline J.M. Wouters. 2019. "Sociodemographic Factors Influencing the Use of eHealth in People with Chronic Diseases" International Journal of Environmental Research and Public Health 16, no. 4: 645. https://doi.org/10.3390/ijerph16040645
APA StyleReiners, F., Sturm, J., Bouw, L. J. W., & Wouters, E. J. M. (2019). Sociodemographic Factors Influencing the Use of eHealth in People with Chronic Diseases. International Journal of Environmental Research and Public Health, 16(4), 645. https://doi.org/10.3390/ijerph16040645