Cancer-Specific Outcomes in the Elderly with Triple-Negative Breast Cancer: A Systematic Review


Abstract
:1. Introduction
2. Methods
2.1. Literature Search Method
2.2. Selection Criteria
2.3. Quality Assessment
2.4. Data Extraction
3. Results
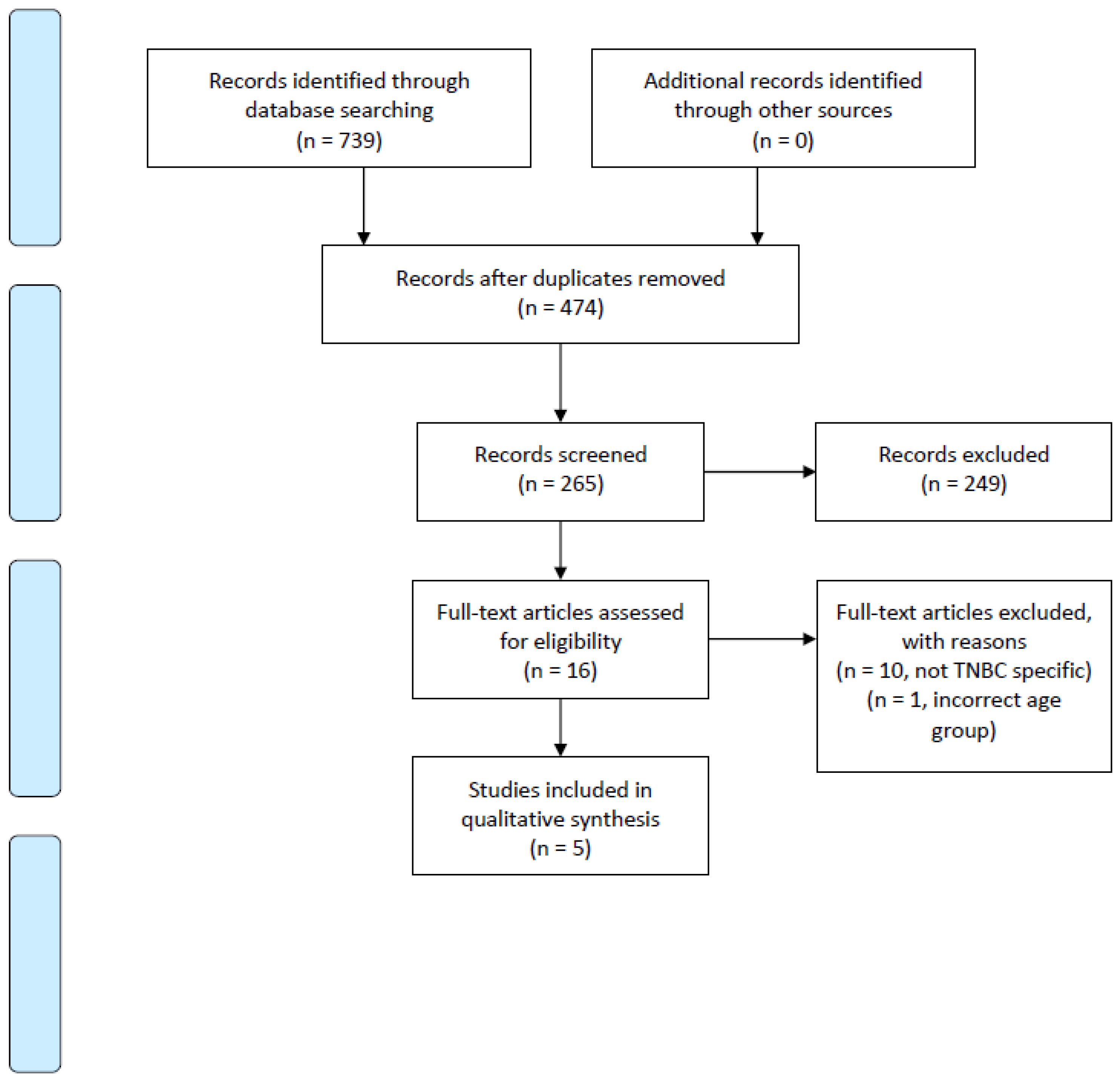
3.1. Included Studies
3.2. Clinicopathologic Features of TNBC Tumor in the Elderly
3.3. Zhu et al.
3.4. Bhoo-Pathy et al.
3.5. Kaplan et al.
3.6. Kozak et al.
3.7. Syed et al.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Breast Cancer Facts & Figures 2019–2020; American Cancer Society: Atlanta, GA, USA, 2019. [Google Scholar]
- Chang-Qing, Y.; Jie, L.; Shi-Qi, Z.; Kun, Z.; Zi-Qian, G.; Ran, X.; Hui-Meng, L.; Ren-Bin, Z.; Gang, Z.; Da-Chuan, Y.; et al. Recent treatment progress of triple negative breast cancer. Prog. Biophys. Mol. Biol. 2020, 151, 40–53. [Google Scholar] [CrossRef]
- Kumar, P.; Aggarwal, R. An overview of triple-negative breast cancer. Arch. Gynecol. Obstet. 2016, 293, 247–269. [Google Scholar] [CrossRef]
- Bauer, K.R.; Brown, M.; Cress, R.D.; Parise, C.A.; Caggiano, V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: A population-based study from the California cancer Registry. Cancer 2007, 109, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.W.; Ogunwole, S.U.; Blakeslee, L.; Rabe, M.A. The Population 65 Years and Older in the United States: 2016; US Census Bureau: Washington, DC, USA, 2018. [Google Scholar]
- Blackmore, T.; Lawrenson, R.; Lao, C.; Edwards, M.; Kuper-Hommel, M.; Elwood, M.; Campbell, I. The characteristics, management and outcomes of older women with breast cancer in New Zealand. Maturitas 2018, 112, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Biganzoli, L.; Wildiers, H.; Oakman, C.; Marotti, L.; Loibl, S.; Kunkler, I.; Reed, M.; Ciatto, S.; Voogd, A.C.; Brain, E.; et al. Management of elderly patients with breast cancer: Updated recommendations of the International Society of Geriatric Oncology (SIOG) and European Society of Breast Cancer Specialists (EUSOMA). Lancet Oncol. 2012, 13, e148–e160. [Google Scholar] [CrossRef]
- Bhoo-Pathy, N.; Verkooijen, H.M.; Wong, F.-Y.; Pignol, J.-P.; Kwong, A.; Tan, E.-Y.; Taib, N.A.; Nei, W.-L.; Ho, G.-F.; Tan, B.; et al. Prognostic role of adjuvant radiotherapy in triple-negative breast cancer: A historical cohort study. Int. J. Cancer 2015, 137, 2504–2512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, H.G.; Malmgren, J.A.; Atwood, M.K. Triple-negative breast cancer in the elderly: Prognosis and treatment. Breast J. 2017, 23, 630–637. [Google Scholar] [CrossRef]
- Kozak, M.M.; Xiang, M.; Pollom, E.L.; Horst, K.C. Adjuvant treatment and survival in older women with triple negative breast cancer: A surveillance, epidemiology, and end results analysis. Breast J. 2019, 25, 469–473. [Google Scholar] [CrossRef]
- Syed, B.M.; Green, A.R.; Nolan, C.C.; Morgan, D.A.L.; Ellis, I.O.; Cheung, K.-L. Biological characteristics and clinical outcome of triple negative primary breast cancer in older women—Comparison with their younger counterparts. PLoS ONE 2014, 9, e100573. [Google Scholar] [CrossRef]
- Zhu, W.; Perez, E.A.; Hong, R.; Li, Q.; Xu, B. Age-related disparity in immediate prognosis of patients with triple-negative breast cancer: A population-based study from SEER cancer registries. PLoS ONE 2015, 10, e0128345. [Google Scholar] [CrossRef] [Green Version]
- Haque, W.; Verma, V.; Hsiao, K.; Hatch, S.; Arentz, C.; Szeja, S.; Schwartz, M.; Niravath, P.; Bonefas, E.; Miltenburg, D.; et al. Omission of radiation therapy following breast conservation in older (≥70 years) women with T1-2N0 triple-negative breast cancer. Breast J. 2019, 25, 1126–1133. [Google Scholar] [CrossRef]
- Algan, O.; Zhao, Y.D.; Herman, T. Radiotherapy in patients 70 years and older with triple-negative breast cancer. Clin. Breast Cancer 2016, 16, e99–e106. [Google Scholar] [CrossRef] [PubMed]
- Freedman, R.A.; Keating, N.L.; Lin, N.U.; Winer, E.P.; Vaz-Luís, I.; Lii, J.; Exman, P.; Barry, W.T. Breast cancer-specific survival by age: Worse outcomes for the oldest patients. Cancer 2018, 124, 2184–2191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, M.J.; Campbell, I.D.; Lawrenson, R.A.; Kuper-Hommel, M.J. Influence of comorbidity on chemotherapy use for early breast cancer: Systematic review and meta-analysis. Breast Cancer Res. Treat. 2017, 165, 17–39. [Google Scholar] [CrossRef] [PubMed]
- Wan, S.; Jubelirer, S. Geographic access and age-related variation in chemotherapy use in elderly with metastatic breast cancer. Breast Cancer Res. Treat. 2015, 149, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Yu, X.; Chen, J.; Yang, Z.; Shao, Z.; Zhang, Z.; Guo, X.; Feng, Y. Radiotherapy can improve the disease-free survival rate in triple-negative breast cancer patients with T1–T2 disease and one to three positive lymph nodes after mastectomy. Oncologist 2013, 18, 141–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Wang, X.-X.; Lian, J.-Y.; Song, C.-G. Effect of postmastectomy radiotherapy on triple-negative breast cancer with T1-2 and 1-3 positive axillary lymph nodes: A population-based study using the SEER 18 database. Oncotarget 2019, 10, 5245–5252. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.T.; Park, C.H.; Kim, S.Y.; Nam, S.J.; Kang, E.Y.; Moon, B.-I.; Lee, H.J.; Jeon, Y.W.; Gwak, H.; Suh, Y.J. The effect of adjuvant chemotherapy on survival in Korean patients with node negative T1c, triple negative breast cancer. PLoS ONE 2018, 13, e0197523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yancik, R.; Wesley, M.N.; Ries, L.A.; Havlik, R.J.; Edwards, B.K.; Yates, J.W. Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. JAMA 2001, 285, 885–892. [Google Scholar] [CrossRef]
- Muss, H.B.; Woolf, S.; Berry, D.; Cirrincione, C.; Weiss, R.B.; Budman, D.; Wood, W.C.; Henderson, I.C.; Hudis, C.; Winer, E.; et al. Adjuvant chemotherapy in older and younger women with lymph node-positive breast cancer. JAMA 2005, 293, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762, Erratum in: Lancet 2013, 382, 1328. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Author, Year | Bias Due to Confounding | Bias in Selection of Participants | Bias in Classification of Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of Reported Result |
|---|---|---|---|---|---|---|
| Bhoo-Pathy, 2015 [8] | Low | Moderate | Low | Low | Low | Low |
| Kaplan, 2017 [9] | Low | Moderate | Low | Low | Low | Moderate |
| Kozak, 2019 [10] | Low | Moderate | Low | Low | Low | Moderate |
| Syed, 2014 [11] | Low | Moderate | Low | Low | Low | Moderate |
| Zhu, 2015 [12] | Serious | Moderate | Low | Low | Low | Moderate |
| Study Characteristics | ||||||
|---|---|---|---|---|---|---|
| Author, Year, Country | Data Source | Study Period | Patients (n), Age Range | Patient and Tumor Characteristics | Treatment Findings | Breast-Cancer-Specific Survival (BCSSS) Outcomes |
| Bhoo-Pathy, 2015, Asia [8] | 5 hospital-based cancer registries | 2016–2011 | 205, 65–96 | Ethnicity, T stage, N stage, tumor grade, lymphovascular invasion | Less radiation use ≥65 vs. >65 (34.9% vs.67.8%) | No survival advantage with radiation in ≥65 (HR 1.34, CI 0.67–2.68, p > 0.05) |
| Kaplan, 2017, USA [9] | Institution-specific breast cancer registry data base | 1990–2014 | 59, 75–93 | Race, stage, histologic grade, nuclear grade, mean tumor size, N stage | No difference in radiation use ≥75 vs. <75 (79% vs. 75%, p = 0.821) Less use of chemotherapy ≥75 vs. <75 (40% vs. 76%, p < 0.001) Less use of surgery, radiation and chemotherapy in ≥75 vs. <75 75 (29% vs. 62%, p < 0.001) | Less use of surgery, radiation and chemotherapy was not associated with a difference in 5-year BCSS (90% <75 vs. 83% ≥75, p = 0.322) |
| Kozak, 2019, USA [10] | SEER | 2010–2014 | 422, 70–100 | Race, region, grade, stage | Less use of radiation in ≥70 vs. <70 (46.3% vs. 53.6% <0.0001) Less use of chemotherapy ≥70 vs. <70 (42.2% vs. 83.1% p < 0.0001) | Decreased use of radiation and chemotherapy in ≥70 vs. <70 was associated with a relative increase in cancer-specific mortality by 25% and increased breast cancer mortality rate (12.8% vs. 10.2%, p < 0.0001). |
| Syed, 2014, UK [11] | Prospective single institution | 1973–2010 | 127, 70–91 | Histological type, size, axillary lymph node status, grade | Less use of chemotherapy ≥70 vs. >70 (0% vs. 47%) | No difference in BCSS ≥70 vs. <70 (73% vs. 79%, p = 0.39) |
| Zhu, 2015, USA [12] | SEER | 2010–2011 | 1224, 70–100 | TN, stage, grade | Less use of surgery in ≥70 vs. <70 (92.8% vs. 94.6%, p = 0.002) Less use of RT in ≥70 vs. <70 (69.9% vs. 61.2%, p < 0.001) | Surgery BCSS 1 HR 0.250, 95% CI, 0.186 to 0.337, p < 0.001 Radiation BCSS HR 0.504, 95% CI, 0,390 to 0.651, p < 0.001 Decreased surgery and radiation in ≥70 associated with 5.9% cancer-specific mortality vs. 2.7% in <70 (p < 0.0001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, J.; Knapp, G.; Quan, M.L.; Bouchard-Fortier, A. Cancer-Specific Outcomes in the Elderly with Triple-Negative Breast Cancer: A Systematic Review. Curr. Oncol. 2021, 28, 2337-2345. https://doi.org/10.3390/curroncol28040215
Yoon J, Knapp G, Quan ML, Bouchard-Fortier A. Cancer-Specific Outcomes in the Elderly with Triple-Negative Breast Cancer: A Systematic Review. Current Oncology. 2021; 28(4):2337-2345. https://doi.org/10.3390/curroncol28040215
Chicago/Turabian StyleYoon, Jenny, Gregory Knapp, May Lynn Quan, and Antoine Bouchard-Fortier. 2021. "Cancer-Specific Outcomes in the Elderly with Triple-Negative Breast Cancer: A Systematic Review" Current Oncology 28, no. 4: 2337-2345. https://doi.org/10.3390/curroncol28040215
APA StyleYoon, J., Knapp, G., Quan, M. L., & Bouchard-Fortier, A. (2021). Cancer-Specific Outcomes in the Elderly with Triple-Negative Breast Cancer: A Systematic Review. Current Oncology, 28(4), 2337-2345. https://doi.org/10.3390/curroncol28040215