Hamartochondroma Pleural Lesion Mimicking Liposarcoma: A Case Report

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
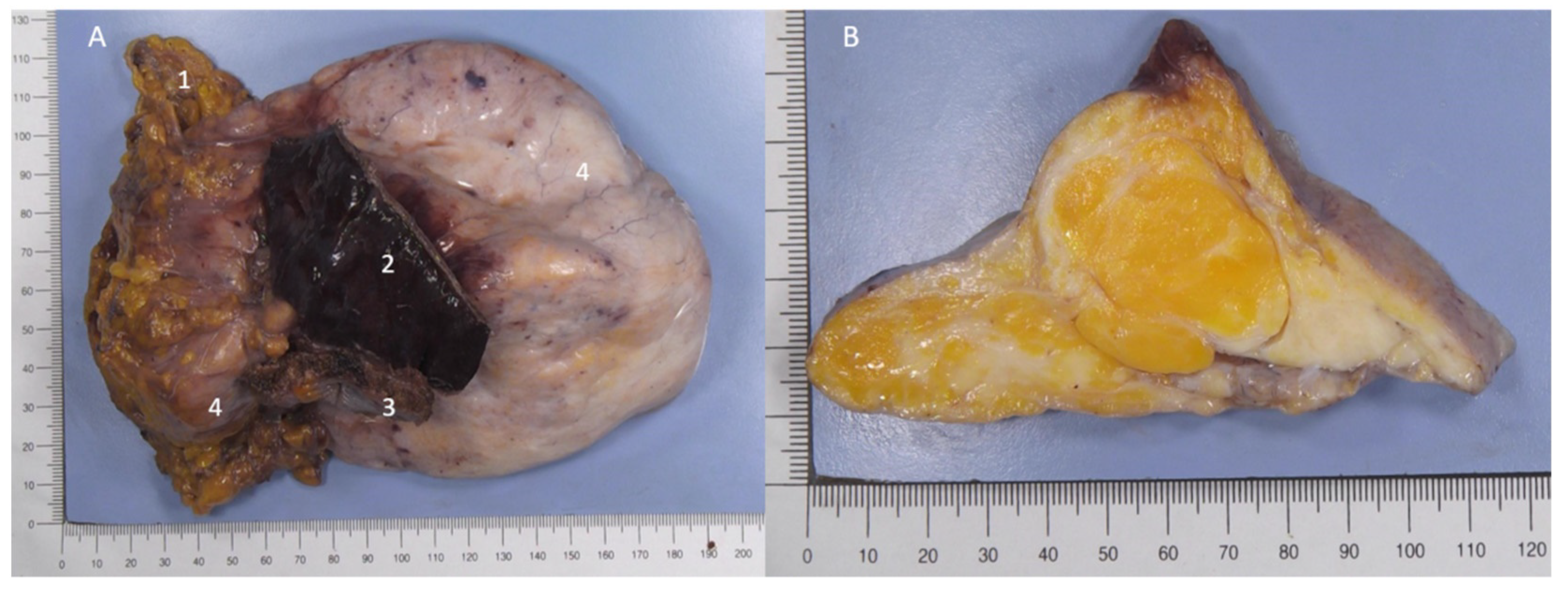
2. Case Presentation
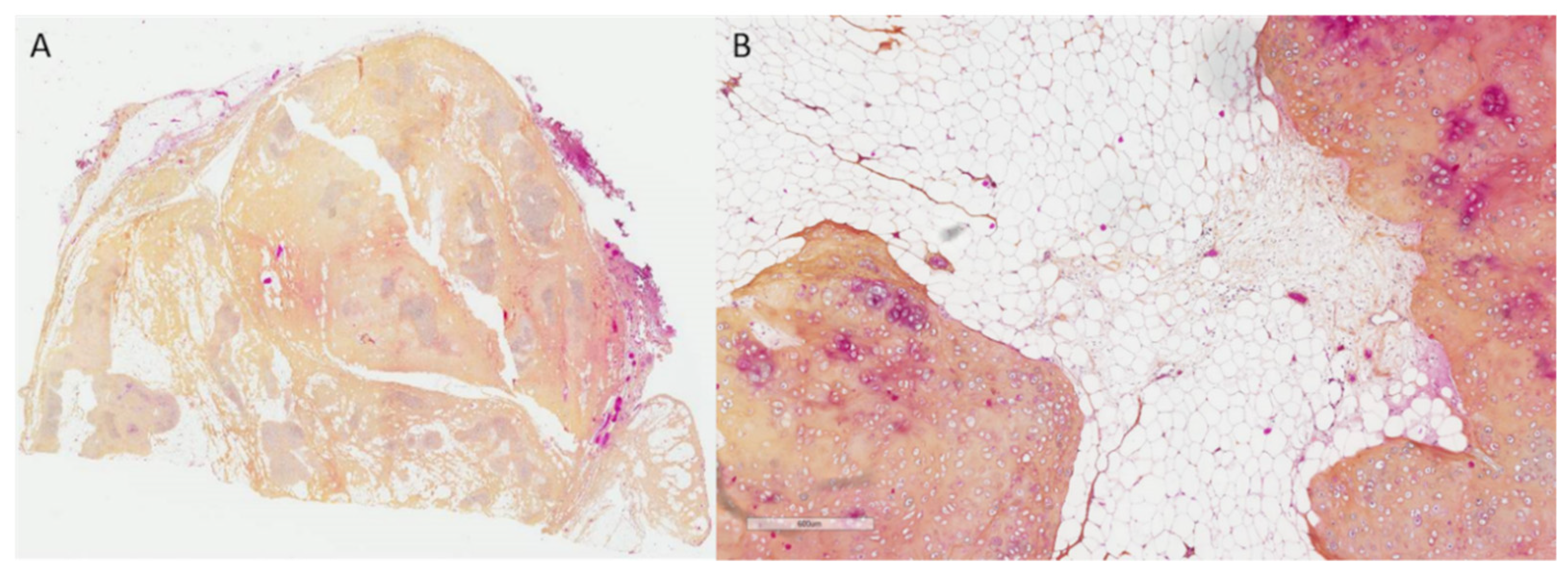
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, C.P.; Liu, D.N.; Zhou, N.N.; Tian, X.Y.; Wang, Z.; Liu, B.N.; Hao, C.Y. Prediction of Histologic Subtype and FNCLCC Grade by SUVmax Measured on 18F-FDG PET/CT in Patients with Retroperitoneal Liposarcoma. Contrast Media Mol. Imaging 2021, 6, 7191363. [Google Scholar] [CrossRef] [PubMed]
- Aluja Jaramillo, F.; Gutierrez, F.; Bhalla, S. Pleural tumours and tumour-like lesions. Clin. Radiol. 2018, 73, 1014–1024. [Google Scholar] [CrossRef] [PubMed]
- Van den Bosch, J.M.; Wagenaar, S.S.; Corrin, B.; Elbers, J.R.; Knaepen, P.J.; Westermann, C.J. Mesenchymoma of the lung (so called hamartoma): A review of 154 parenchymal and endobronchial cases. Thorax 1987, 42, 790–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaerte, S.C.; Meyer, C.A.; Winer-Muram, H.T.; Tarver, R.D.; Conces, D.J., Jr. Fat-containing lesions of the chest. Radiographics 2002, 22, S61–S78. [Google Scholar] [CrossRef] [PubMed]
- Geramizadeh, B.; Mottavvas, M.; Zeyaian, B.; Amirian, A. Giant hamartoma of lung presented with massive hemoptysis: A rare case report and review of the literature. Rare Tumors 2019, 11, 2036361318823926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, T.J.; Collins, J. MR imaging evaluation of disorders of the chest wall. Magn. Reson. Imaging Clin. N. Am. 2008, 16, 355–379. [Google Scholar] [CrossRef] [PubMed]
- Berry, M.F.; Sporn, T.A.; Moore, J.O.; D’Amico, T.A. Giant thoracic liposarcoma treated with induction chemotherapy followed by surgical resection. J. Thorac. Oncol. 2009, 4, 768–769. [Google Scholar] [CrossRef] [Green Version]
- Cosío, B.G.; Villena, V.; Echave-Sustaeta, J.; de Miguel, E.; Alfaro, J.; Hernandez, L.; Sotelo, T. Endobronchial hamartoma. Chest 2002, 122, 202–205. [Google Scholar] [CrossRef]
- Endo, T.; Endo, S.; Hasegawa, T.; Tetsuka, K.; Yamamoto, S.; Otani, S.; Kanai, Y.; Tezuka, Y. Extrapulmonary hamartoma. Gen. Thorac. Cardiovasc. Surg. 2011, 59, 209–211. [Google Scholar] [CrossRef]
- Hermant, P.; Bellamy, J.; Georges, O. Hamartome pulmonaire à forme lipomateuse [Pulmonary hamartoma with lipomatous form]. Rev. Mal. Respir. 2011, 28, 677–680. [Google Scholar] [CrossRef] [PubMed]
- Gholoum, S.; Fraser, R.; Ferri, L.E. Posterior mediastinal chondromatous hamartoma. Ann. Thorac. Surg. 2007, 83, 1528–1530. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zheng, D.; Zuo, M.; Li, Y.; Zhang, H. Chondromesenchymal hamartomas in a 24-year-old male mimicking a posterior mediastinal tumor and a 5-month-old boy with postoperative disseminated intravascular coagulation: Two case reports. Diagn. Pathol. 2020, 15, 53. [Google Scholar] [CrossRef] [PubMed]
- Altaner, S.; Yoruk, Y.; Bilgi, S.; Puyan, F.O.; Doganay, L.; Kutlu, K. Multifocal mesenchymal hamartoma of the chest wall. Respirology 2006, 11, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Brichon, P.Y.; Pilichowski, P.; Brambilla, E.; Coulomb, M.; Latreille, R. Mediastinal chondrohamartoma. Eur. J. Cardiothorac. Surg. 1987, 1, 176–179. [Google Scholar] [CrossRef]
- Guo, W.; Zhao, Y.P.; Jiang, Y.G.; Wang, R.W.; Ma, Z. Surgical treatment and outcome of pulmonary hamartoma: A retrospective study of 20-year experience. J. Exp. Clin. Cancer Res. 2008, 27, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elsayed, H.; Abdel Hady, S.M.; Elbastawisy, S.E. Is resection necessary in biopsy-proven asymptomatic pulmonary hamartomas? Interact. Cardiovasc. Thorac. Surg. 2015, 21, 773–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribet, M.; Jaillard-Thery, S.; Nuttens, M.C. Pulmonary hamartoma and malignancy. J. Thorac. Cardiovasc. Surg. 1994, 107, 611–614. [Google Scholar] [CrossRef]
- Karasik, A.; Modan, M.; Jacob, C.O.; Lieberman, Y. Increased risk of lung cancer in patients with chondromatous hamartoma. J. Thorac. Cardiovasc. Surg. 1980, 80, 217–220. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drevet, G.; Kovacs, E.; Chalabreysse, L.; Gamondes, D.; Tronc, F. Hamartochondroma Pleural Lesion Mimicking Liposarcoma: A Case Report. Curr. Oncol. 2022, 29, 3489-3493. https://doi.org/10.3390/curroncol29050281
Drevet G, Kovacs E, Chalabreysse L, Gamondes D, Tronc F. Hamartochondroma Pleural Lesion Mimicking Liposarcoma: A Case Report. Current Oncology. 2022; 29(5):3489-3493. https://doi.org/10.3390/curroncol29050281
Chicago/Turabian StyleDrevet, Gabrielle, Erik Kovacs, Lara Chalabreysse, Delphine Gamondes, and François Tronc. 2022. "Hamartochondroma Pleural Lesion Mimicking Liposarcoma: A Case Report" Current Oncology 29, no. 5: 3489-3493. https://doi.org/10.3390/curroncol29050281
APA StyleDrevet, G., Kovacs, E., Chalabreysse, L., Gamondes, D., & Tronc, F. (2022). Hamartochondroma Pleural Lesion Mimicking Liposarcoma: A Case Report. Current Oncology, 29(5), 3489-3493. https://doi.org/10.3390/curroncol29050281