Successful Treatment with Selpercatinib for Ectopic Cushing’s Syndrome Due to Medullary Thyroid Cancer


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
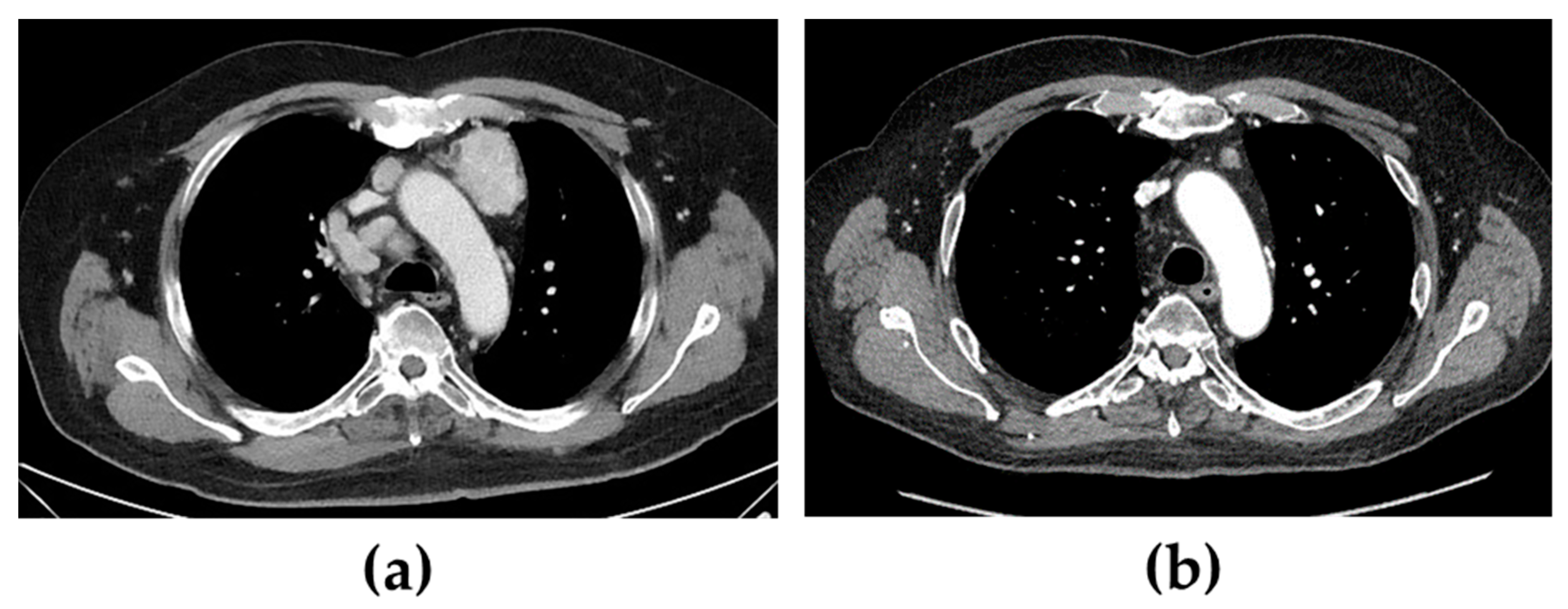
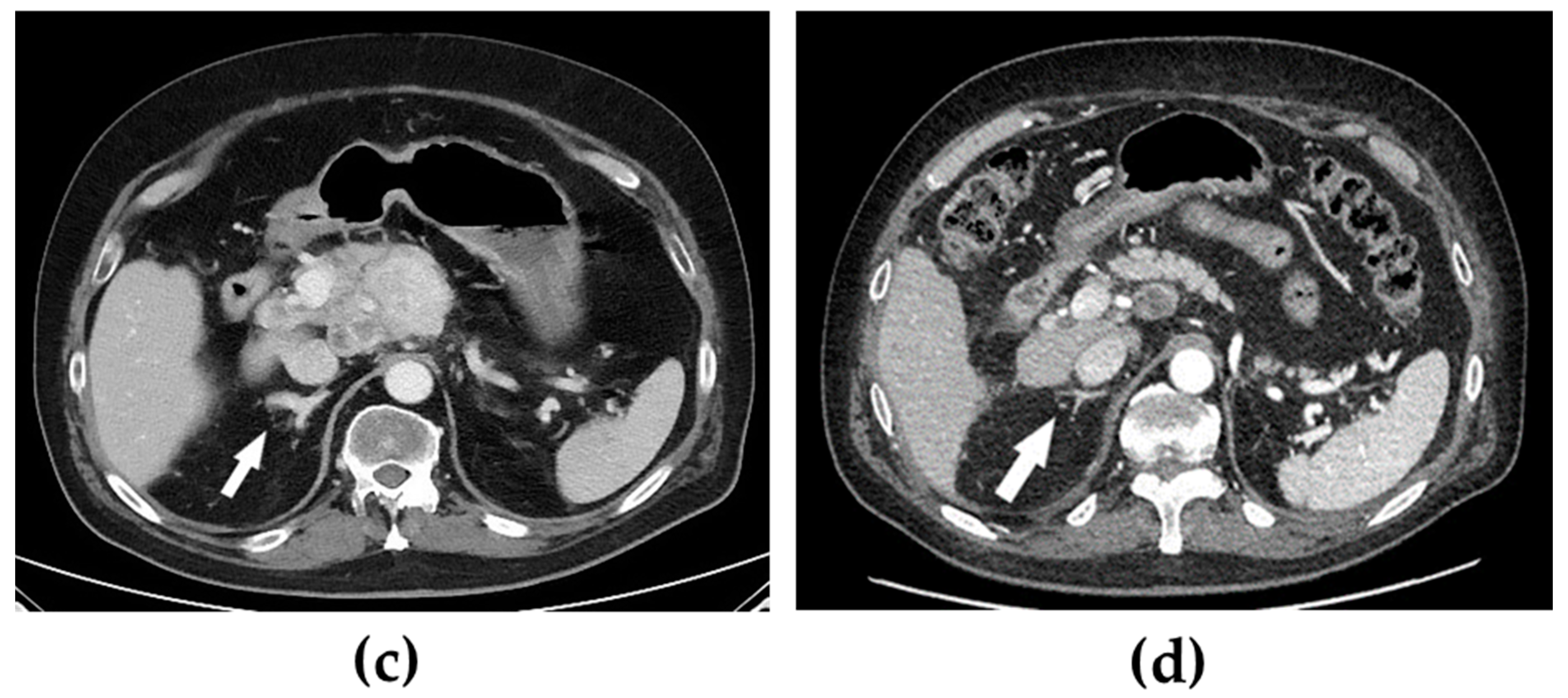
2. Case Presentation
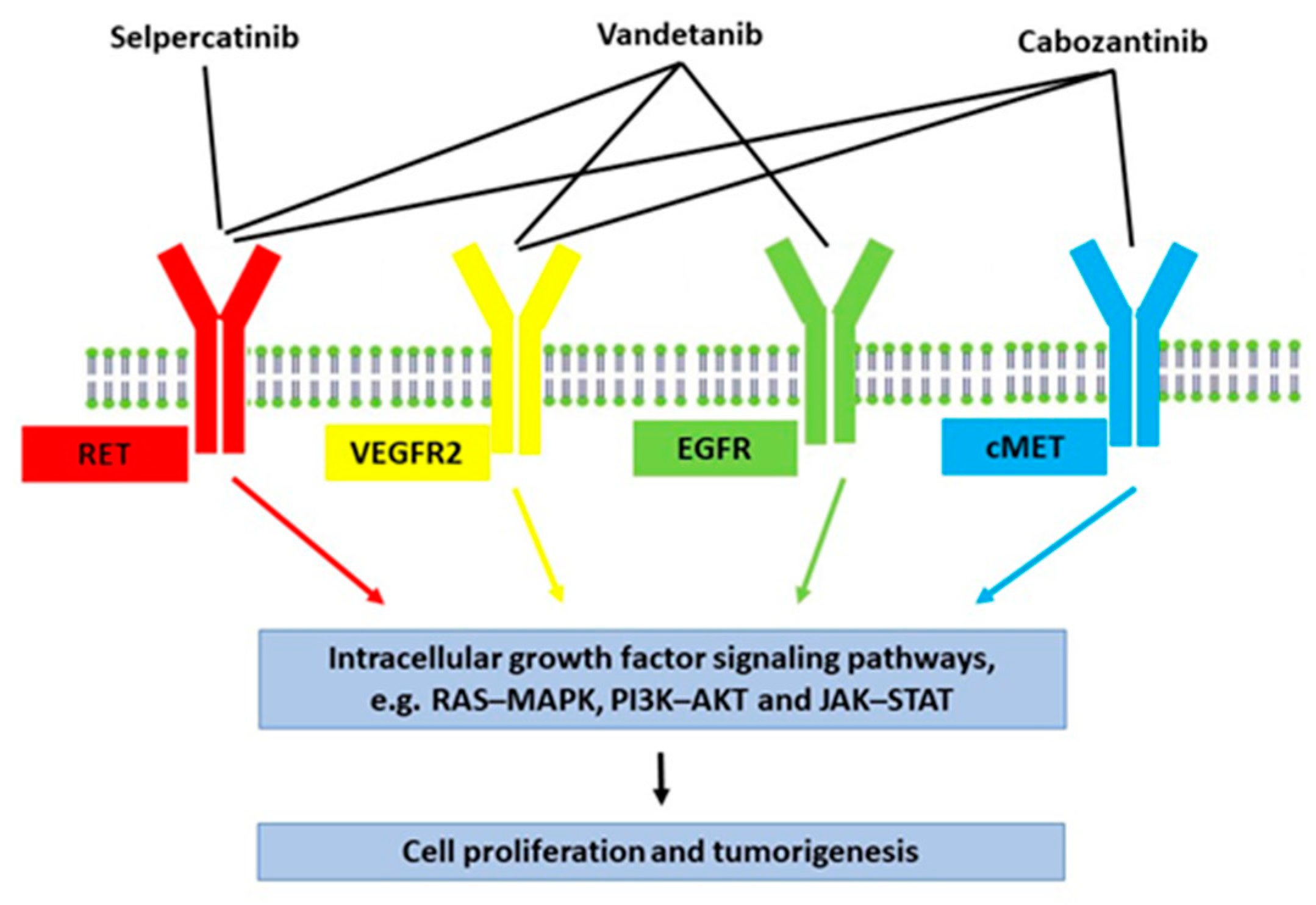
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Puerto, M.; Borson-Chazot, F.; Tabarin, A. Updates on therapy for medullary thyroid cancer in 2021. Ann. Endocrinol. 2021, 83, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Pelizzo, M.; Boschin, I.M.; Bernante, P.; Toniato, A.; Piotto, A.; Pagetta, C.; Nibale, O.; Rampin, L.; Muzzio, P.; Rubello, D. Natural history, diagnosis, treatment and outcome of medullary thyroid cancer: 37 years experience on 157 patients. Eur. J. Surg. Oncol. 2007, 33, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Kebebew, E.; Ituarte, P.H.; Siperstein, A.E.; Duh, Q.Y.; Clark, O.H. Medullary thyroid carcinoma: Clinical characteristics, treatment, prognostic factors, and a comparison of staging systems. Cancer 2000, 88, 1139–1148. [Google Scholar] [CrossRef]
- Davi, M.V.; Cosaro, E.; Piacentini, S.; Reimondo, G.M.; Albiger, N.; Arnaldi, G.; Faggiano, A.; Mantovani, G.; Fazio, N.; Piovesan, A.; et al. Prognostic factors in ectopic Cushing’s syndrome due to neuroendocrine tumors: A multicenter study. Eur. J. Endocrinol. 2017, 176, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moura, M.M.; Cavaco, B.; Pinto, A.; Domingues, R.; Santos, J.R.; Cid, M.O.; Bugalho, M.J.; Leite, V. Correlation of RET somatic mutations with clinicopathological features in sporadic medullary thyroid carcinomas. Br. J. Cancer 2009, 100, 1777–1783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbosa, S.L.-S.; Rodien, P.; Leboulleux, S.; Niccoli-Sire, P.; Kraimps, J.-L.; Caron, P.; Archambeaud-Mouveroux, F.; Conte-Devolx, B.; Rohmer, V.; Endocrines, G.D.D.T. Ectopic Adrenocorticotropic Hormone-Syndrome in Medullary Carcinoma of the Thyroid: A Retrospective Analysis and Review of the Literature. Thyroid 2005, 15, 618–623. [Google Scholar] [CrossRef] [PubMed]
- Koehler, V.F.; Fuss, C.T.; Berr, C.M.; Frank-Raue, K.; Raue, F.; Hoster, E.; Hepprich, M.; Christ, E.; Pusl, T.; Reincke, M.; et al. Medullary thyroid cancer with ectopic Cushing’s syndrome: A multicentre case series. Clin. Endocrinol. 2021, 96, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Valassi, E.; Santos, A.; Yaneva, M.; Toth, M.; Strasburger, C.J.; Chanson, P.; Wass, J.A.H.; Chabre, O.; Pfeifer, M.; Feelders, R.A.; et al. The European Registry on Cushing’s syndrome: 2-year experience. Baseline demographic and clinical characteristics. Eur. J. Endocrinol. 2011, 165, 383–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheikh-Ali, M.; Krishna, M.; Lloyd, R.; Smallridge, R.C. Predicting the development of Cushing’s syndrome in medullary thyroid cancer: Utility of proopiomelanocortin messenger ribonucleic acid in situ hybridization. Thyroid 2007, 17, 631–634. [Google Scholar] [CrossRef] [PubMed]
- von Mach, M.A.; Kann, P.; Piepkorn, B.; Bruder, S.; Beyer, J. Cushing’s syndrome caused by paraneoplastic ACTH secretion 11 years after occurence of a medullary thyroid carcinoma. Dtsch. Med. Wochenschr. 2002, 127, 850–852. [Google Scholar] [CrossRef] [PubMed]
- Nagy-Mignotte, H.; Shestaeva, O.; Vignoud, L.; Guillem, P.; Ruckly, S.; Chabre, O.; Sakhri, L.; Duruisseaux, M.; Mousseau, M.; Timsit, J.-F.; et al. Prognostic Impact of Paraneoplastic Cushing’s Syndrome in Small-Cell Lung Cancer. J. Thorac. Oncol. 2014, 9, 497–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valassi, E.; Tabarin, A.; Brue, T.; Feelders, R.A.; Reincke, M.; Netea-Maier, R.; Toth, M.; Zacharieva, S.; Webb, S.M.; Tsagarakis, S.; et al. High mortality within 90 days of diagnosis in patients with Cushing’s syndrome: Results from the ERCUSYN registry. Eur. J. Endocrinol. 2019, 181, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Ragnarsson, O.; Olsson, D.S.; Papakokkinou, E.; Chantzichristos, D.; Dahlqvist, P.; Segerstedt, E.; Olsson, T.; Petersson, M.; Berinder, K.; Bensing, S.; et al. Overall and Disease-Specific Mortality in Patients With Cushing Disease: A Swedish Nationwide Study. J. Clin. Endocrinol. Metab. 2019, 104, 2375–2384. [Google Scholar] [CrossRef] [PubMed]
- Ntali, G.; Asimakopoulou, A.; Siamatras, T.; Komninos, J.; Vassiliadi, D.; Tzanela, M.; Tsagarakis, S.; Grossman, A.B.; Wass, J.A.H.; Karavitaki, N. Mortality in Cushing’s syndrome: Systematic analysis of a large series with prolonged follow-up. Eur. J. Endocrinol. 2013, 169, 715–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maxwell, J.E.; Sherman, S.K.; O’Dorisio, T.M.; Howe, J.R. Medical management of metastatic medullary thyroid cancer. Cancer 2014, 120, 3287–3301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijewardene, A.A.; Glastras, S.J.; Learoyd, D.L.; Robinson, B.G.; Tsang, V.H.M. ACTH-secreting medullary thyroid cancer: A case series. Endocrinol. Diabetes Metab. Case Rep. 2017, 2017, 16–0110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciampi, R.; Romei, C.; Ramone, T.; Prete, A.; Tacito, A.; Cappagli, V.; Bottici, V.; Viola, D.; Torregrossa, L.; Ugolini, C.; et al. Genetic Landscape of Somatic Mutations in a Large Cohort of Sporadic Medullary Thyroid Carcinomas Studied by Next-Generation Targeted Sequencing. iScience 2019, 20, 324–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wirth, L.J.; Sherman, E.; Robinson, B.; Solomon, B.; Kang, H.; Lorch, J.; Worden, F.; Brose, M.; Patel, J.; Leboulleux, S.; et al. Efficacy of Selpercatinib in RET-Altered Thyroid Cancers. N. Engl. J. Med. 2020, 383, 825–835. [Google Scholar] [CrossRef] [PubMed]
- Berr, C.M.; Di Dalmazi, G.; Osswald, A.; Ritzel, K.; Bidlingmaier, M.; Geyer, L.L.; Treitl, M.; Hallfeldt, K.; Rachinger, W.; Reisch, N.; et al. Time to recovery of adrenal function after curative surgery for Cushing’s syndrome depends on etiology. J. Clin. Endocrinol. Metab. 2015, 100, 1300–1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forde, H.E.; Mehigan-Farrelly, N.; Ryan, K.; Moran, T.; Greally, M.; Duffy, A.G.; Byrne, M.M. Metastatic medullary thyroid carcinoma presenting as ectopic Cushing’s syndrome. Endocrinol. Diabetes Metab. Case Rep. 2021, 2021, 20–0207. [Google Scholar] [CrossRef]
- Agosto, S.S.V.; Zhu, E.; Nguyen, M.; Kherani, J.; Olek, E.; Rothenberg, S.M.; Kane, M.; Sherman, S.I. Successful resolution of Cushing syndrome due to ectopic ACTH syndrome in metastatic medullary thyroid carcinoma during treatment with selpercatinib (LOXO-292), a novel highly selective RET inhibitor. In Proceedings of the 89th Annual Meeting American Thyroid Association, Chicago, IL, USA, 30 October–3 November 2019. [Google Scholar]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ragnarsson, O.; Piasecka, M.; Hallqvist, A. Successful Treatment with Selpercatinib for Ectopic Cushing’s Syndrome Due to Medullary Thyroid Cancer. Curr. Oncol. 2022, 29, 3494-3498. https://doi.org/10.3390/curroncol29050282
Ragnarsson O, Piasecka M, Hallqvist A. Successful Treatment with Selpercatinib for Ectopic Cushing’s Syndrome Due to Medullary Thyroid Cancer. Current Oncology. 2022; 29(5):3494-3498. https://doi.org/10.3390/curroncol29050282
Chicago/Turabian StyleRagnarsson, Oskar, Marta Piasecka, and Andreas Hallqvist. 2022. "Successful Treatment with Selpercatinib for Ectopic Cushing’s Syndrome Due to Medullary Thyroid Cancer" Current Oncology 29, no. 5: 3494-3498. https://doi.org/10.3390/curroncol29050282
APA StyleRagnarsson, O., Piasecka, M., & Hallqvist, A. (2022). Successful Treatment with Selpercatinib for Ectopic Cushing’s Syndrome Due to Medullary Thyroid Cancer. Current Oncology, 29(5), 3494-3498. https://doi.org/10.3390/curroncol29050282