Real-World Treatment Patterns and Clinical Outcomes among Patients Receiving CDK4/6 Inhibitors for Metastatic Breast Cancer in a Canadian Setting Using AI-Extracted Data

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
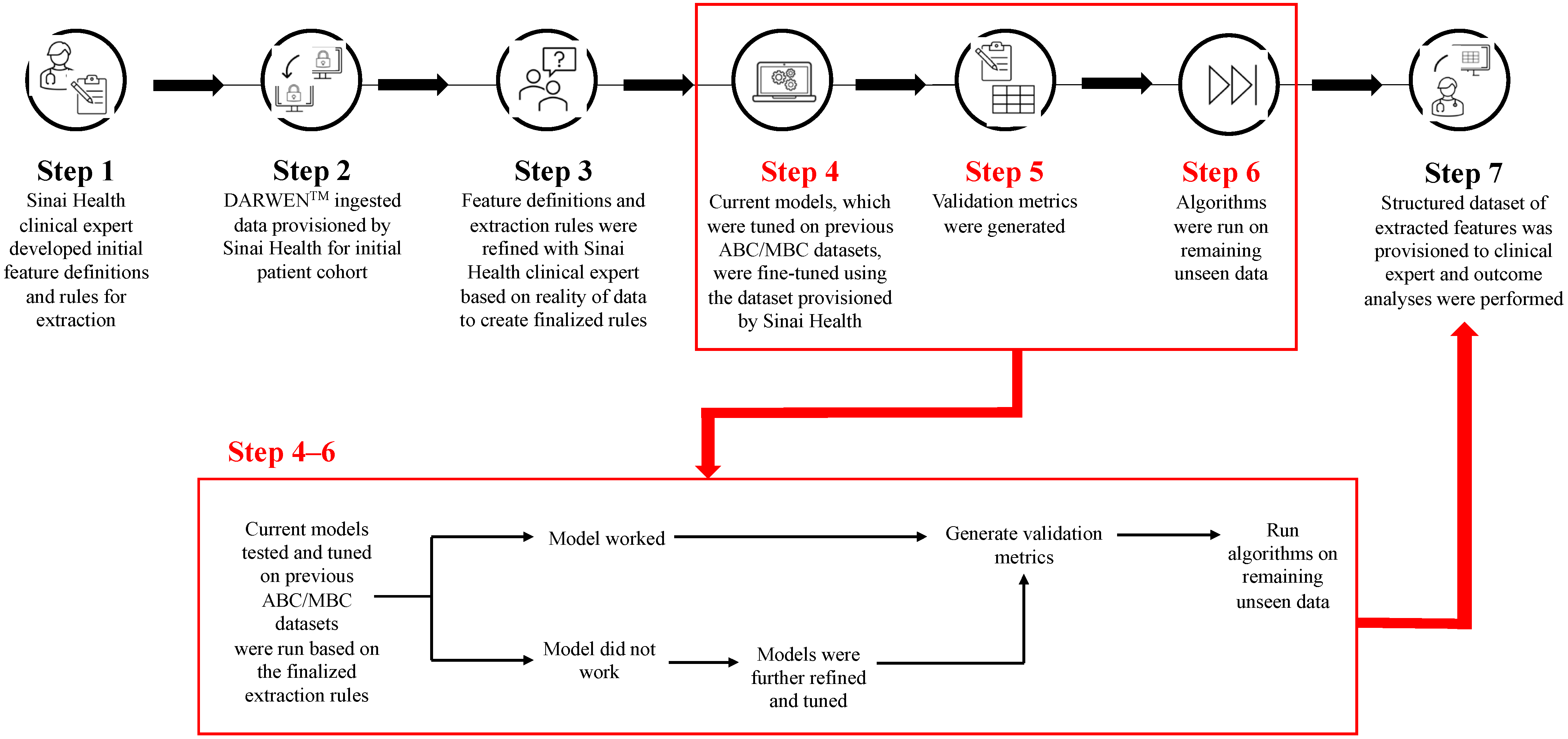
2.2. Clinical Feature Extraction
2.3. Outcomes
2.4. Statistical Analyses
3. Results
3.1. Patients
3.2. Treatment Patterns
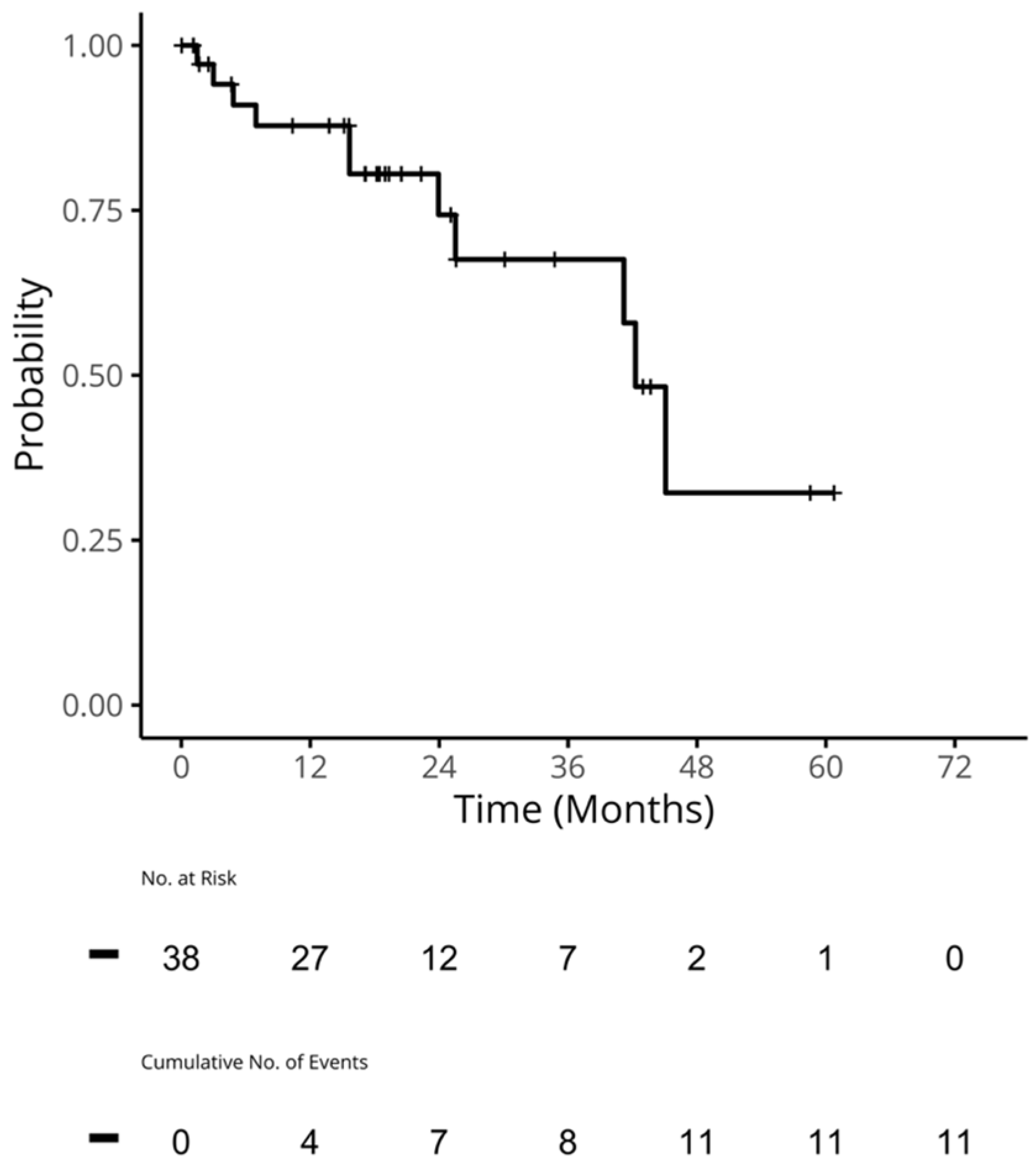
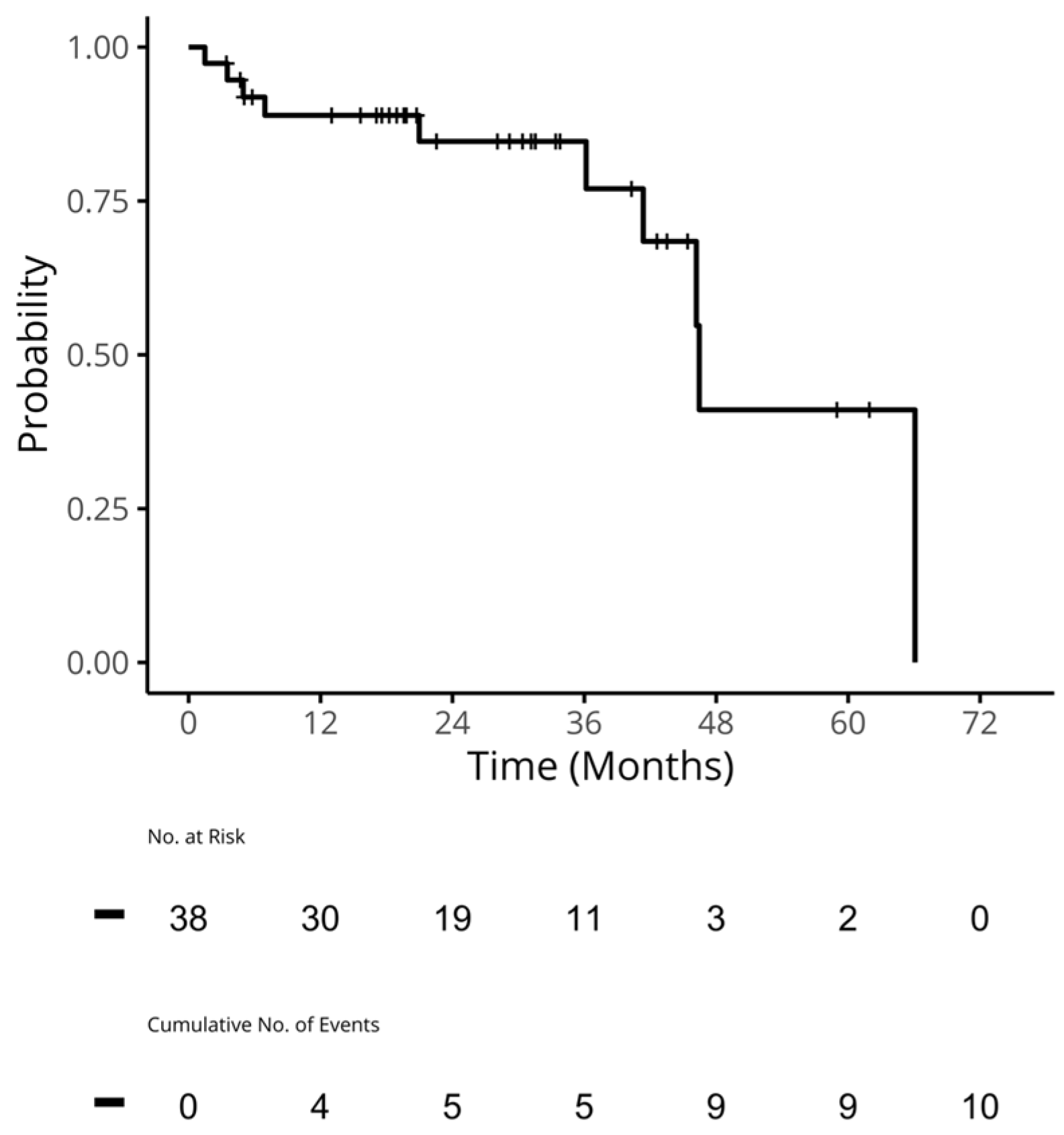
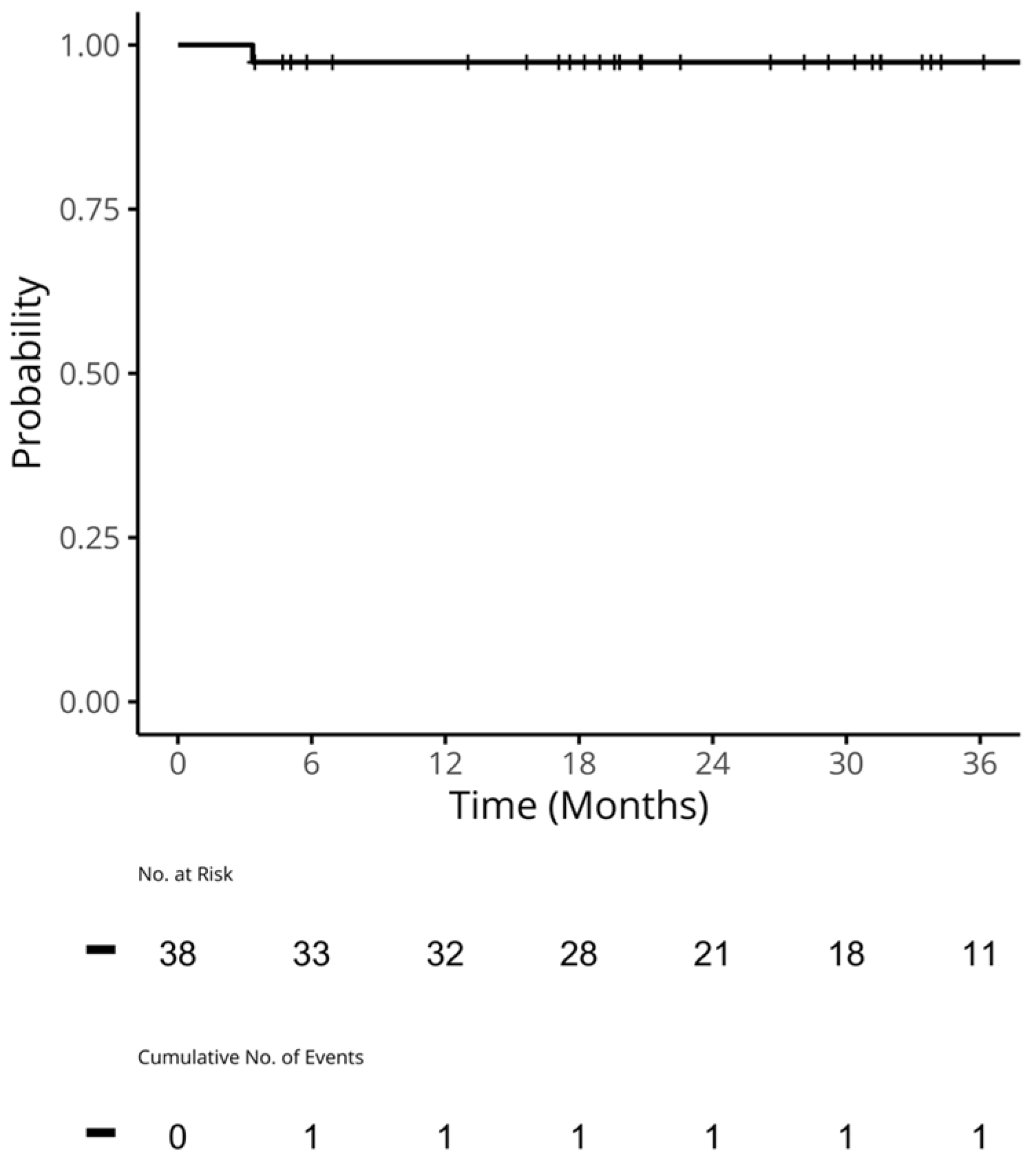
3.3. Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Release Notice—Canadian Cancer Statistics 2021. Health Promot. Chronic Dis. Prev. Can. 2021, 41, 399. [CrossRef]
- Survival Statistics for Breast Cancer | Canadian Cancer Society. Available online: https://cancer.ca/en/cancer-information/cancer-types/breast/prognosis-and-survival/survival-statistics (accessed on 7 June 2023).
- Migliaccio, I.; Bonechi, M.; McCartney, A.; Guarducci, C.; Benelli, M.; Biganzoli, L.; Di Leo, A.; Malorni, L. CDK4/6 inhibitors: A focus on biomarkers of response and post-treatment therapeutic strategies in hormone receptor-positive HER2− negative breast cancer. Cancer Treat. Rev. 2021, 93, 102136. [Google Scholar] [CrossRef] [PubMed]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; Dang, C.; et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 691–722. [Google Scholar] [CrossRef]
- Jerzak, K.J.; Bouganim, N.; Brezden-Masley, C.; Edwards, S.; Gelmon, K.; Henning, J.-W.; Hilton, J.F.; Sehdev, S. HR+/HER2– Advanced Breast Cancer Treatment in the First-Line Setting: Expert Review. Curr. Oncol. 2023, 30, 5425–5447. [Google Scholar] [CrossRef]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.-A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef]
- Rugo, H.S.; Finn, R.S.; Diéras, V.; Ettl, J.; Lipatov, O.; Joy, A.A.; Harbeck, N.; Castrellon, A.; Iyer, S.; Lu, D.R.; et al. Palbociclib plus letrozole as first-line therapy in estrogen receptor-positive/human epidermal growth factor receptor 2-negative advanced breast cancer with extended follow-up. Breast Cancer Res. Treat. 2019, 174, 719–729. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.-S.; Sonke, G.S.; Paluch-Shimon, S.; Campone, M.; Blackwell, K.L.; André, F.; Winer, E.P.; et al. Ribociclib as First-Line Therapy for HR-Positive, Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1738–1748. [Google Scholar] [CrossRef]
- Goetz, M.P.; Toi, M.; Campone, M.; Sohn, J.; Paluch-Shimon, S.; Huober, J.; Park, I.H.; Trédan, O.; Chen, S.-C.; Manso, L.; et al. MONARCH 3: Abemaciclib As Initial Therapy for Advanced Breast Cancer. J. Clin. Oncol. 2017, 35, 3638–3646. [Google Scholar] [CrossRef]
- DeMichele, A.; Cristofanilli, M.; Brufsky, A.; Liu, X.; Mardekian, J.; McRoy, L.; Layman, R.M.; Emir, B.; Torres, M.A.; Rugo, H.S.; et al. Comparative effectiveness of first-line palbociclib plus letrozole versus letrozole alone for HR+/HER2− metastatic breast cancer in US real-world clinical practice. Breast Cancer Res. 2021, 23, 37. [Google Scholar] [CrossRef]
- Rugo, H.S.; Brufsky, A.; Liu, X.; Li, B.; McRoy, L.; Chen, C.; Layman, R.M.; Cristofanilli, M.; Torres, M.A.; Curigliano, G.; et al. Real-world study of overall survival with palbociclib plus aromatase inhibitor in HR+/HER2− metastatic breast cancer. npj Breast Cancer 2022, 8, 114. [Google Scholar] [CrossRef] [PubMed]
- Goyal, R.K.; Chen, H.; Abughosh, S.M.; Holmes, H.M.; Candrilli, S.D.; Johnson, M.L. Overall survival associated with CDK4/6 inhibitors in patients with HR+/HER2– metastatic breast cancer in the United States: A SEER-Medicare population-based study. Cancer 2023, 129, 1051–1063. [Google Scholar] [CrossRef] [PubMed]
- Canadian Cancer Society. Treatments for Stage 4 Breast Cancer. Available online: https://cancer.ca/en/cancer-information/cancer-types/breast/treatment/stage-4 (accessed on 7 June 2023).
- Maio, M.D.; Perrone, F.; Conte, P. Real-World Evidence in Oncology: Opportunities and Limitations. Oncologist 2020, 25, e746. [Google Scholar] [CrossRef] [PubMed]
- Corrigan-Curay, J.; Sacks, L.; Woodcock, J. Real-World Evidence and Real-World Data for Evaluating Drug Safety and Effectiveness. JAMA 2018, 320, 867–868. [Google Scholar] [CrossRef] [PubMed]
- Cejuela, M.; Gil-Torralvo, A.; Castilla, M.Á.; Domínguez-Cejudo, M.Á.; Falcón, A.; Benavent, M.; Molina-Pinelo, S.; Ruiz-Borrego, M.; Salvador Bofill, J. Abemaciclib, Palbociclib, and Ribociclib in Real-World Data: A Direct Comparison of First-Line Treatment for Endocrine-Receptor-Positive Metastatic Breast Cancer. Int. J. Mol. Sci. 2023, 24, 8488. [Google Scholar] [CrossRef]
- Gauthier, M.P.; Law, J.H.; Le, L.W.; Li, J.J.N.; Zahir, S.; Nirmalakumar, S.; Sung, M.; Pettengell, C.; Aviv, S.; Chu, R.; et al. Automating Access to Real-World Evidence. JTO Clin. Res. Rep. 2022, 3, 100340. [Google Scholar] [CrossRef] [PubMed]
- Yanamadala, S.; Morrison, D.; Curtin, C.; McDonald, K.; Hernandez-Boussard, T. Electronic Health Records and Quality of Care: An Observational Study Modeling Impact on Mortality, Readmissions, and Complications. Medicine 2016, 95, e3332. [Google Scholar] [CrossRef]
- Evans, R.S. Electronic Health Records: Then, Now, and in the Future. Yearb. Med. Inform. 2016, 25, S48–S61. [Google Scholar] [CrossRef]
- Zhou, L.; Soran, C.S.; Jenter, C.A.; Volk, L.A.; Orav, E.J.; Bates, D.W.; Simon, S.R. The relationship between electronic health record use and quality of care over time. J. Am. Med. Inform. Assoc. 2009, 16, 457–464. [Google Scholar] [CrossRef]
- Pons, E.; Braun, L.M.M.; Hunink, M.G.M.; Kors, J.A. Natural Language Processing in Radiology: A Systematic Review. Radiology 2016, 279, 329–343. [Google Scholar] [CrossRef]
- Petch, J.; Batt, J.; Murray, J.; Mamdani, M. Extracting Clinical Features From Dictated Ambulatory Consult Notes Using a Commercially Available Natural Language Processing Tool: Pilot, Retrospective, Cross-Sectional Validation Study. JMIR Med. Inform. 2019, 7, e12575. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Thompson, W.K.; Herr, T.M.; Zeng, Z.; Berendsen, M.A.; Jonnalagadda, S.R.; Carson, M.B.; Starren, J. Natural Language Processing for EHR-Based Pharmacovigilance: A Structured Review. Drug Saf. 2017, 40, 1075–1089. [Google Scholar] [CrossRef] [PubMed]
- Petch, J.; Kempainnen, J.; Pettengell, C.; Aviv, S.; Butler, B.; Pond, G.; Saha, A.; Bogach, J.; Allard-Coutu, A.; Sztur, P.; et al. Developing a Data and Analytics Platform to Enable a Breast Cancer Learning Health System at a Regional Cancer Center. JCO Clin. Cancer Inform. 2023, 7, e2200182. [Google Scholar] [CrossRef] [PubMed]
- Carrell, D.S.; Cronkite, D.; Palmer, R.E.; Saunders, K.; Gross, D.E.; Masters, E.T.; Hylan, T.R.; Von Korff, M. Using natural language processing to identify problem usage of prescription opioids. Int. J. Med. Inform. 2015, 84, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Melton, G.B.; Hripcsak, G. Automated detection of adverse events using natural language processing of discharge summaries. J. Am. Med. Inform. Assoc. 2005, 12, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Vender, R.; Lynde, C. AI-Powered Patient Identification to Optimize Care; Canadian Dermatology Association: Ottawa, ON, Canada, 2023. [Google Scholar]
- Birtwhistle, R.; Williamson, T. Primary care electronic medical records: A new data source for research in Canada. CMAJ: Can. Med. Assoc. J. 2015, 187, 239. [Google Scholar] [CrossRef] [PubMed]
- Law, J.H.; Pettengell, C.; Le, L.W.; Aviv, S.; DeMarco, P.; Merritt, D.C.; Lau, S.C.M.; Sacher, A.G.; Leighl, N.B. Generating real-world evidence: Using automated data extraction to replace manual chart review. J. Clin. Oncol. 2019, 37, e18096. [Google Scholar] [CrossRef]
- Law, J.; Pettengell, C.; Chen, L.; Le, L.; Sung, M.; Aviv, S.; Lau, S.; Sacher, A.; Merritt, D.; Demarco, P.; et al. EP1.16-05 Real World Outcomes of Advanced NSCLC Patients with Liver Metastases. J. Thorac. Oncol. 2019, 14, S1066. [Google Scholar] [CrossRef]
- Pettengell, C.; Law, J.; Le, L.; Sung, M.; Lau, S.; Sacher, A.; Merritt, D.; Demarco, P.; Leighl, N. P1.16-07 Real World Evidence of the Impact of Immunotherapy in Patients with Advanced Lung Cancer. J. Thorac. Oncol. 2019, 14, S588. [Google Scholar] [CrossRef]
- Cheung, W.Y.; Farrer, C.; Darwish, L.; Pettengell, C.; Stewart, E.L. 82P Exploring treatment patterns and outcomes of patients with advanced lung cancer (aLC) using artificial intelligence (AI)-extracted data. Ann. Oncol. 2021, 32, S1407. [Google Scholar] [CrossRef]
- Grant, B.M.; Zarrin, A.; Zhan, L.; Ajaj, R.; Darwish, L.; Khan, K.; Patel, D.; Chiasson, K.; Balaratnam, K.; Chowdhury, M.T.; et al. Abstract 4087: Developing a standardized framework for curating oncology datasets generated by manual abstraction and artificial intelligence. Cancer Res. 2022, 82, 4087. [Google Scholar] [CrossRef]
- Mycock, K.; Zhan, L.; Taylor-Stokes, G.; Milligan, G.; Mitra, D. Real-World Palbociclib Use in HR+/HER2− Advanced Breast Cancer in Canada: The IRIS Study. Curr. Oncol. 2021, 28, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Tripathy, D.; Rocque, G.; Blum, J.L.; Karuturi, M.S.; McCune, S.; Kurian, S.; Moezi, M.M.; Anderson, D.; Gauthier, E.; Zhang, Z.; et al. 251P Real-world clinical outcomes of palbociclib plus endocrine therapy (ET) in hormone receptor–positive advanced breast cancer: Results from the POLARIS trial. Ann. Oncol. 2022, 33, S651–S652. [Google Scholar] [CrossRef]
- Siddique, S.; Chow, J. Artificial intelligence in radiotherapy. Rep. Pract. Oncol. Radiother. 2020, 25, 656–666. [Google Scholar] [CrossRef]
- Schork, N.J. Artificial Intelligence and Personalized Medicine. In Precision Medicine in Cancer Therapy; Von Hoff, D.D., Han, H., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 265–283. [Google Scholar]
- Davenport, T.; Kalakota, R. The potential for artificial intelligence in healthcare. Future Healthc. J. 2019, 6, 94. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.E.W.; Pollard, T.J.; Shen, L.; Lehman, L.H.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Anthony Celi, L.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef]
- Turchin, A.; Masharsky, S.; Zitnik, M. Comparison of BERT implementations for natural language processing of narrative medical documents. Inform. Med. Unlocked 2023, 36, 101139. [Google Scholar] [CrossRef]
- Chase, H.S.; Mitrani, L.R.; Lu, G.G.; Fulgieri, D.J. Early recognition of multiple sclerosis using natural language processing of the electronic health record. BMC Med. Inform. Decis. Mak. 2017, 17, 24. [Google Scholar] [CrossRef] [PubMed]
- Afzal, N.; Sohn, S.; Abram, S.; Liu, H.; Kullo, I.J.; Arruda-Olson, A.M. Identifying Peripheral Arterial Disease Cases Using Natural Language Processing of Clinical Notes. In Proceedings of the 2016 IEEE-EMBS International Conference on Biomedical and Health Informatics (BHI), Las Vegas, NV, USA, 24–27 February 2016. [Google Scholar]
- Banerjee, I.; Bozkurt, S.; Caswell-Jin, J.L.; Kurian, A.W.; Rubin, D.L. Natural Language Processing Approaches to Detect the Timeline of Metastatic Recurrence of Breast Cancer. JCO Clin. Cancer Inform. 2019, 3, 1–12. [Google Scholar] [CrossRef]
- Benedum, C.M.; Sondhi, A.; Fidyk, E.; Cohen, A.B.; Nemeth, S.; Adamson, B.; Estévez, M.; Bozkurt, S. Replication of Real-World Evidence in Oncology Using Electronic Health Record Data Extracted by Machine Learning. Cancers 2023, 15, 1853. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (N = 48) | Patients Receiving CDK4/6i in 1L (N = 38) | |
|---|---|---|
| Age at ABC/MBC diagnosis | ||
| Mean (SD) | 57.9 (14.0) | 58.4 (13.0) |
| Median | 60.5 | 61.0 |
| Q1, Q3 | 48.8, 67.0 | 50.0, 65.5 |
| Range | 23.0–89.0 | 23.0–84.0 |
| Year of ABC/MBC diagnosis a | ||
| 2016–2018 | 20 (41.7%) | 16 (42.1%) |
| 2019–2021 | 28 (58.3%) | 22 (57.9%) |
| Sex | ||
| Female | 48 (100.0%) | 38 (100.0%) |
| Tumor histology | ||
| Ductal | 32 (66.7%) | 25 (65.8%) |
| Lobular | 7 (14.6%) | (NR) |
| Mixed | (NR) | (NR) |
| Other | 8 (16.7%) | 8 (21.1%) |
| De novo/recurrent at initial BC diagnosis | ||
| De novo | 14 (29.2%) | 10 (26.3%) |
| Recurrent | 34 (70.8%) | 28 (73.7%) |
| HER2 status at ABC/MBC diagnosis | ||
| Negative | 48 (100.0%) | 38 (100.0%) |
| ER status at ABC/MBC diagnosis | ||
| Positive | 48 (100.0%) | 38 (100.0%) |
| PR status at ABC/MBC diagnosis | ||
| Negative | 13 (27.1%) | 11 (28.9%) |
| Positive | 30 (62.5%) | 23 (60.5%) |
| Unknown | (NR) | (NR) |
| ECOG at ABC/MBC diagnosis | ||
| 0 | 6 (12.5%) | (NR) |
| 1 | 12 (25.0%) | 10 (26.3%) |
| 2 | (NR) | (NR) |
| 3 | (NR) | (NR) |
| Unknown | 26 (54.2%) | 21 (55.3%) |
| Tumor grade at ABC/MBC diagnosis | ||
| 1 | (NR) | (NR) |
| 2 | 11 (22.9%) | 8 (21.1%) |
| 3 | (NR) | (NR) |
| Unknown | 29 (60.4%) | 24 (63.2%) |
| Organ-level metastatic sites b | ||
| Bone | 35 (72.9%) | 26 (68.4%) |
| Bone-only metastases | 15 (31.2%) | 12 (31.6%) |
| Brain | (NR) | (NR) |
| Lung | 19 (39.6%) | 16 (42.1%) |
| Liver | 18 (37.5%) | 12 (31.6%) |
| Number of metastatic sites during study period | ||
| 0 | (NR) | (NR) |
| 1 | 22 (45.8%) | 19 (50.0%) |
| 2 | 14 (29.2%) | 9 (23.7%) |
| 3 | (NR) | (NR) |
| 4 | (NR) | (NR) |
| Comorbidities at ABC/MBC diagnosis b | ||
| Atrial Fibrillation | (NR) | (NR) |
| Hypertension | 18 (37.5%) | 12 (31.6%) |
| Diabetes | 7 (14.6%) | (NR) |
| Coronary Artery Disease | (NR) | (NR) |
| Radiotherapy for ABC/MBC b | ||
| Any radiotherapy | 18 (37.5%) | 13 (34.2%) |
| Follow-up since diagnosis (months) | ||
| Mean (SD) | 28.8 (16.7) | 28.7 (16.9) |
| Median | 29.3 | 28.7 |
| Q1, Q3 | 17.5, 37.2 | 17.8, 39.3 |
| Range | 3.4–67.6 | 3.4–67.6 |
| 1L Treatment Regimen | All Patients (N = 48) |
|---|---|
| Palbociclib + ET | 30 (62.5%) |
| Palbociclib + ET + goserelin | (NR) |
| Other CDK4/6i + ET | (NR) |
| Other CDK4/6i + ET + goserelin | (NR) |
| ET | (NR) |
| Chemotherapy | 7 (14.6%) |
| 2L treatment regimen | All patients (N = 21) |
| Palbociclib + ET | (NR) |
| Palbociclib + ET + goserelin | (NR) |
| Other CDK4/6i + ET | 7 (33.3%) |
| Other CDK4/6i + ET + goserelin | (NR) |
| Alpelisib + ET | (NR) |
| ET | (NR) |
| Chemotherapy | 6 (28.6%) |
| 3L treatment regimen | All patients (N = 12) |
| Palbociclib + ET + goserelin | (NR) |
| Other CDK4/6i | (NR) |
| Chemotherapy | 10 (83.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moulson, R.; Feugère, G.; Moreira-Lucas, T.S.; Dequen, F.; Weiss, J.; Smith, J.; Brezden-Masley, C. Real-World Treatment Patterns and Clinical Outcomes among Patients Receiving CDK4/6 Inhibitors for Metastatic Breast Cancer in a Canadian Setting Using AI-Extracted Data. Curr. Oncol. 2024, 31, 2172-2184. https://doi.org/10.3390/curroncol31040161
Moulson R, Feugère G, Moreira-Lucas TS, Dequen F, Weiss J, Smith J, Brezden-Masley C. Real-World Treatment Patterns and Clinical Outcomes among Patients Receiving CDK4/6 Inhibitors for Metastatic Breast Cancer in a Canadian Setting Using AI-Extracted Data. Current Oncology. 2024; 31(4):2172-2184. https://doi.org/10.3390/curroncol31040161
Chicago/Turabian StyleMoulson, Ruth, Guillaume Feugère, Tracy S. Moreira-Lucas, Florence Dequen, Jessica Weiss, Janet Smith, and Christine Brezden-Masley. 2024. "Real-World Treatment Patterns and Clinical Outcomes among Patients Receiving CDK4/6 Inhibitors for Metastatic Breast Cancer in a Canadian Setting Using AI-Extracted Data" Current Oncology 31, no. 4: 2172-2184. https://doi.org/10.3390/curroncol31040161
APA StyleMoulson, R., Feugère, G., Moreira-Lucas, T. S., Dequen, F., Weiss, J., Smith, J., & Brezden-Masley, C. (2024). Real-World Treatment Patterns and Clinical Outcomes among Patients Receiving CDK4/6 Inhibitors for Metastatic Breast Cancer in a Canadian Setting Using AI-Extracted Data. Current Oncology, 31(4), 2172-2184. https://doi.org/10.3390/curroncol31040161