Remineralization of Artificial Dentin Caries Using Dentin and Enamel Matrix Proteins


 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Isolation of DMPs According to Schlagenhauf
2.2. Sample Preparation
2.3. Sample Treatment
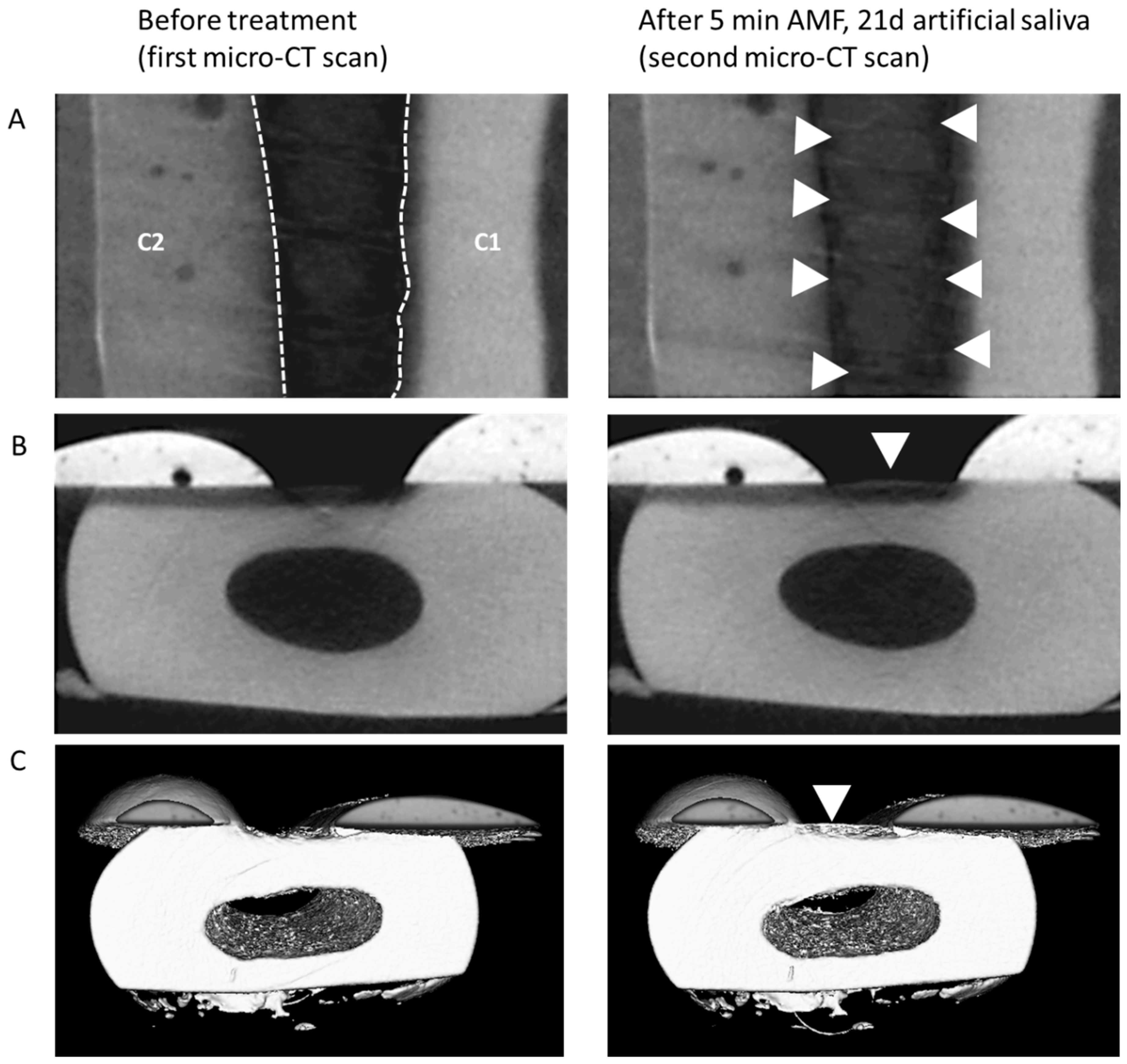
2.4. Micro-CT Scanning
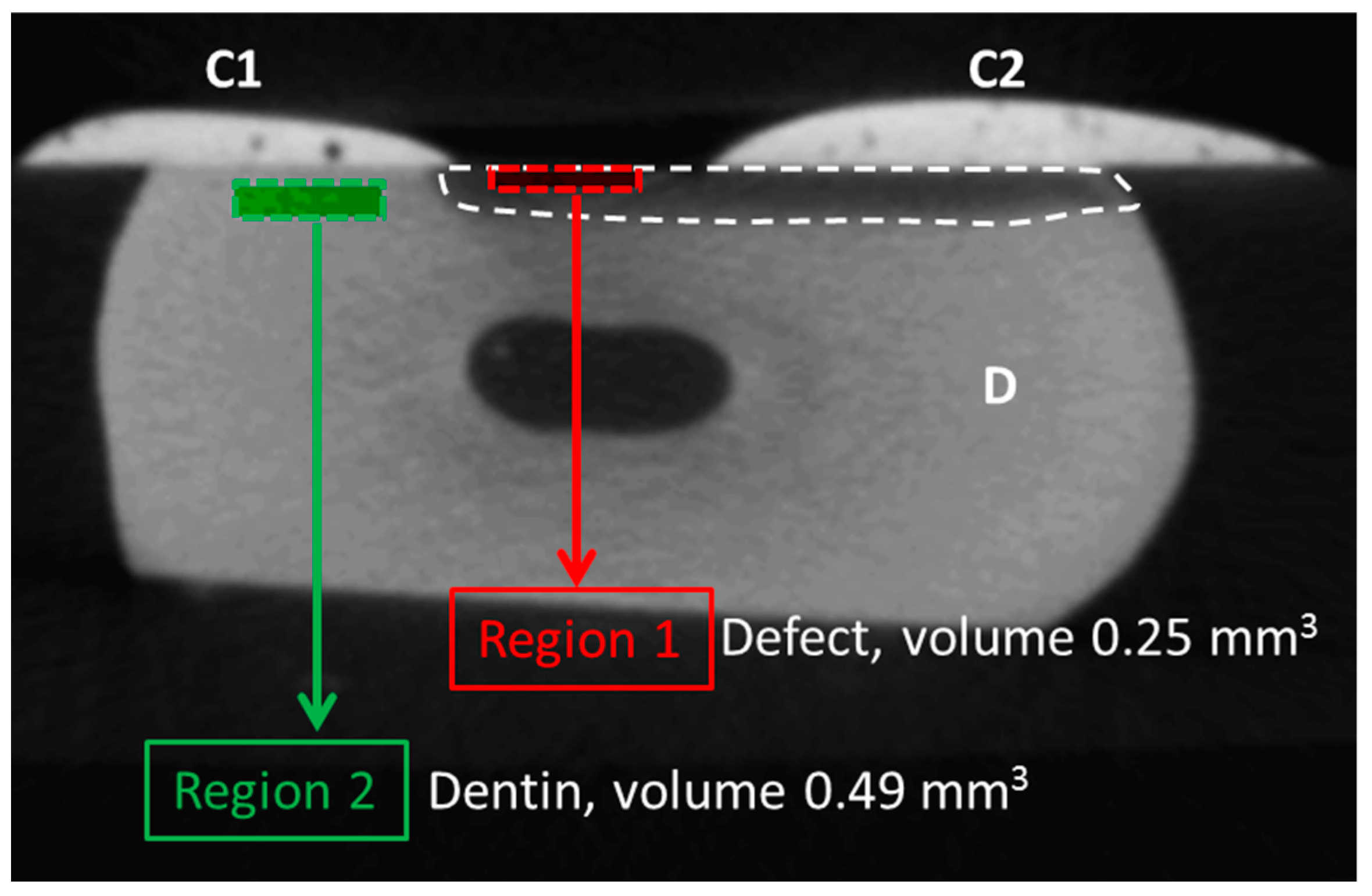
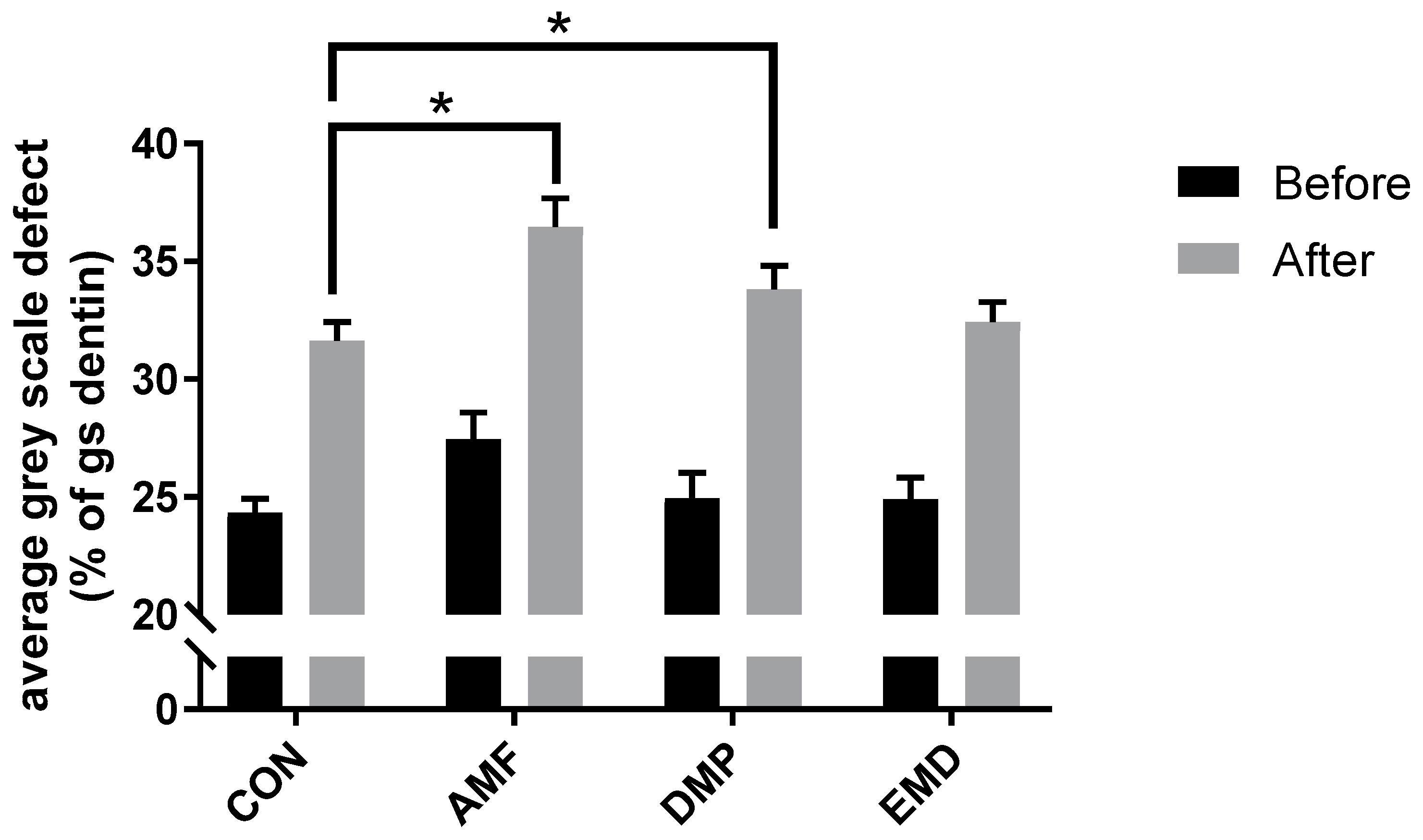
2.5. Data Analysis and Statistics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fure, S.; Zickert, I. Prevalence of root surface caries in 55, 65, and 75-year-old Swedish individuals. Community Dent. Oral Epidemiol. 1990, 18, 100–105. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Chen, L.; Hu, X.; Shimada, Y.; Otsuki, M.; Tagami, J.; Ruan, S. Mechanical properties and molecular structure analysis of subsurface dentin after Er:YAG laser irradiation. J. Mech. Behav. Biomed. Mater. 2017, 74, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Abou Neel, E.A.; Aljabo, A.; Strange, A.; Ibrahim, S.; Coathup, M.; Young, A.M.; Bozec, L.; Mudera, V. Demineralization-remineralization dynamics in teeth and bone. Int. J. Nanomed. 2016, 11, 4743–4763. [Google Scholar] [CrossRef] [PubMed]
- Mazzoni, A.; Tjäderhane, L.; Checchi, V.; Di Lenarda, R.; Salo, T.; Tay, F.R.; Pashley, D.H.; Breschi, L. Role of dentin MMPs in caries progression and bond stability. J. Dent. Res. 2015, 94, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Arola, D.D.; Reprogel, R.K. Tubule orientation and the fatigue strength of human dentin. Biomaterials 2006, 27, 2131–2140. [Google Scholar] [CrossRef] [PubMed]
- Weiner, S.; Veis, A.; Beniash, E.; Arad, T.; Dillon, J.W.; Sabsay, B.; Siddiqui, F. Peritubular dentin formation: crystal organization and the macromolecular constituents in human teeth. J. Struct. Biol. 1999, 126, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Butler, W.T.; Ritchie, H. The nature and functional significance of dentin extracellular matrix proteins. Int. J. Dev. Biol. 1995, 39, 169–179. [Google Scholar]
- Ravindran, S.; George, A. Dentin Matrix Proteins in Bone Tissue Engineering. Adv. Exp. Med. Biol. 2015, 881, 129–142. [Google Scholar] [Green Version]
- Fernández, C.E.; Tenuta, L.M.; Cury, J.A. Validation of a Cariogenic Biofilm Model to Evaluate the Effect of Fluoride on Enamel and Root Dentine Demineralization. PLoS One 2016, 11, e0146478. [Google Scholar] [CrossRef]
- Qi, Y.P.; Li, N.; Niu, L.N.; Primus, C.M.; Ling, J.Q.; Pashley, D.H.; Tay, F.R. Remineralization of artificial dentinal caries lesions by biomimetically modified mineral trioxide aggregate. Acta Biomater. 2012, 8, 836–842. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, N.; Nyvad, B. Ecological Hypothesis of Dentin and Root Caries. Caries Res. 2016, 50, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Grandin, H.M.; Gemperli, A.C.; Dard, M. Enamel matrix derivative: a review of cellular effects in vitro and a model of molecular arrangement and functioning. Tissue Eng. Part B Rev. 2012, 18, 181–202. [Google Scholar] [CrossRef] [PubMed]
- Schmidlin, P.; Zobrist, K.; Attin, T.; Wegehaupt, F. In vitro re-hardening of artificial enamel caries lesions using enamel matrix proteins or self-assembling peptides. J. Appl. Oral Sci. 2016, 24, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Bratthall, D.; Hänsel-Petersson, G.; Sundberg, H. Reasons for the caries decline: what do the experts believe? Eur. J. Oral Sci. 1996, 104, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Augello, M. Osteoinduktive Wirkung von Dentinpartikel, Säureextrakt und Dentinmatrixproteine auf humane Knochenzellen. Ph.D. Thesis, Zentrum für Zahn-, Mund- und Kieferheilkunde der Universität Zürich, Zürich, Switzerland, 2003. [Google Scholar]
- Schlagenhauf, U. Mesenchymale Zellen der humanen Zahnpulpa, Beobachtungen und Experimente an einem Zellkulturmodell. Ph.D. Thesis, Eberhard-Karls Universität, Tübingen, Germany, 1992. [Google Scholar]
- Buskes, J.A.; Christoffersen, J.; Arends, J. Lesion formation and lesion remineralization in enamel under constant composition conditions. A new technique with applications. Caries Res. 1985, 19, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Clementino-Luedemann, T.N.; Kunzelmann, K.H. Mineral concentration of natural human teeth by a commercial micro-CT. Dent. Mater. J. 2006, 25, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Lo, E.C.; Zhi, Q.H.; Itthagarun, A. Comparing two quantitative methods for studying remineralization of artificial caries. J. Dent. 2010, 38, 352–359. [Google Scholar] [CrossRef]
- Nakata, K.; Nikaido, T.; Nakashima, S.; Nango, N.; Tagami, J. An approach to normalizing micro-CT depth profiles of mineral density for monitoring enamel remineralization progress. Dent. Mater. J. 2012, 31, 533–540. [Google Scholar] [CrossRef]
- Magalhães, A.C.; Moron, B.M.; Comar, L.P.; Wiegand, A.; Buchalla, W.; Buzalaf, M.A. Comparison of cross-sectional hardness and transverse microradiography of artificial carious enamel lesions induced by different demineralising solutions and gels. Caries Res. 2009, 43, 474–483. [Google Scholar] [CrossRef]
- Bedran-Russo, A.K.; Ravindran, S.; George, A. Imaging analysis of early DMP1 mediated dentine remineralization. Arch. Oral Biol. 2013, 58, 254–260. [Google Scholar] [CrossRef]
- Liu, W.; Cao, Y.; Shen, J.; Xu, Q.; Zhu, Z.; Li, Q. Design and evaluation of a kind of biomimetic peptides of dentin matrix protein-1. West China J. Stomatology 2013, 31, 341–344. [Google Scholar]
- Widbiller, M.; Eidt, A.; Wölflick, M.; Lindner, S.R.; Schweikl, H.; Hiller, K.A.; Buchalla, W.; Galler, K.M. Interactive effects of LPS and dentine matrix proteins on human dental pulp stem cells. Int. Endod. J. 2018, 51, 877–888. [Google Scholar] [CrossRef] [PubMed]
- Thanatvarakorn, O.; Islam, M.S.; Nakashima, S.; Sadr, A.; Nikaido, T.; Tagami, J. Effects of zinc fluoride on inhibiting dentin demineralization and collagen degradation in vitro: A comparison of various topical fluoride agents. Dent. Mater. J. 2016, 35, 769–775. [Google Scholar] [CrossRef] [PubMed]





© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bächli, K.; Schmidlin, P.R.; Wegehaupt, F.; Paqué, F.; Ramenzoni, L.; Botter, S. Remineralization of Artificial Dentin Caries Using Dentin and Enamel Matrix Proteins. Materials 2019, 12, 2116. https://doi.org/10.3390/ma12132116
Bächli K, Schmidlin PR, Wegehaupt F, Paqué F, Ramenzoni L, Botter S. Remineralization of Artificial Dentin Caries Using Dentin and Enamel Matrix Proteins. Materials. 2019; 12(13):2116. https://doi.org/10.3390/ma12132116
Chicago/Turabian StyleBächli, Katja, Patrick R. Schmidlin, Florian Wegehaupt, Frank Paqué, Liza Ramenzoni, and Sander Botter. 2019. "Remineralization of Artificial Dentin Caries Using Dentin and Enamel Matrix Proteins" Materials 12, no. 13: 2116. https://doi.org/10.3390/ma12132116
APA StyleBächli, K., Schmidlin, P. R., Wegehaupt, F., Paqué, F., Ramenzoni, L., & Botter, S. (2019). Remineralization of Artificial Dentin Caries Using Dentin and Enamel Matrix Proteins. Materials, 12(13), 2116. https://doi.org/10.3390/ma12132116