Pure Mandibular Incisor Intrusion: A Finite Element Study to Evaluate the Segmented Arch Technique

 and
and
Abstract
:1. Introduction
2. Materials and Methods
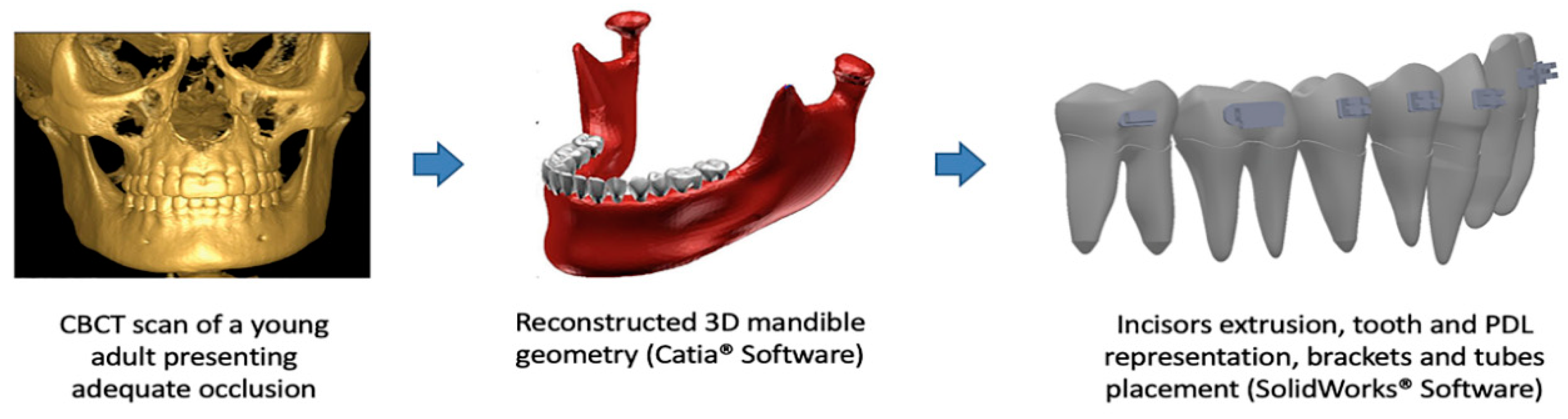
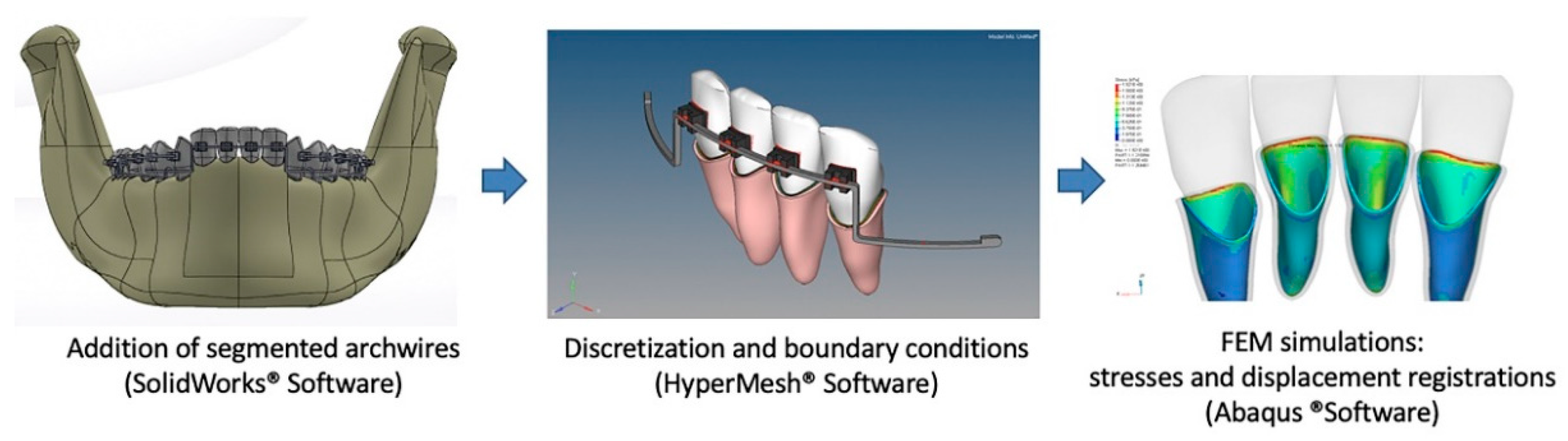
2.1. Modeling
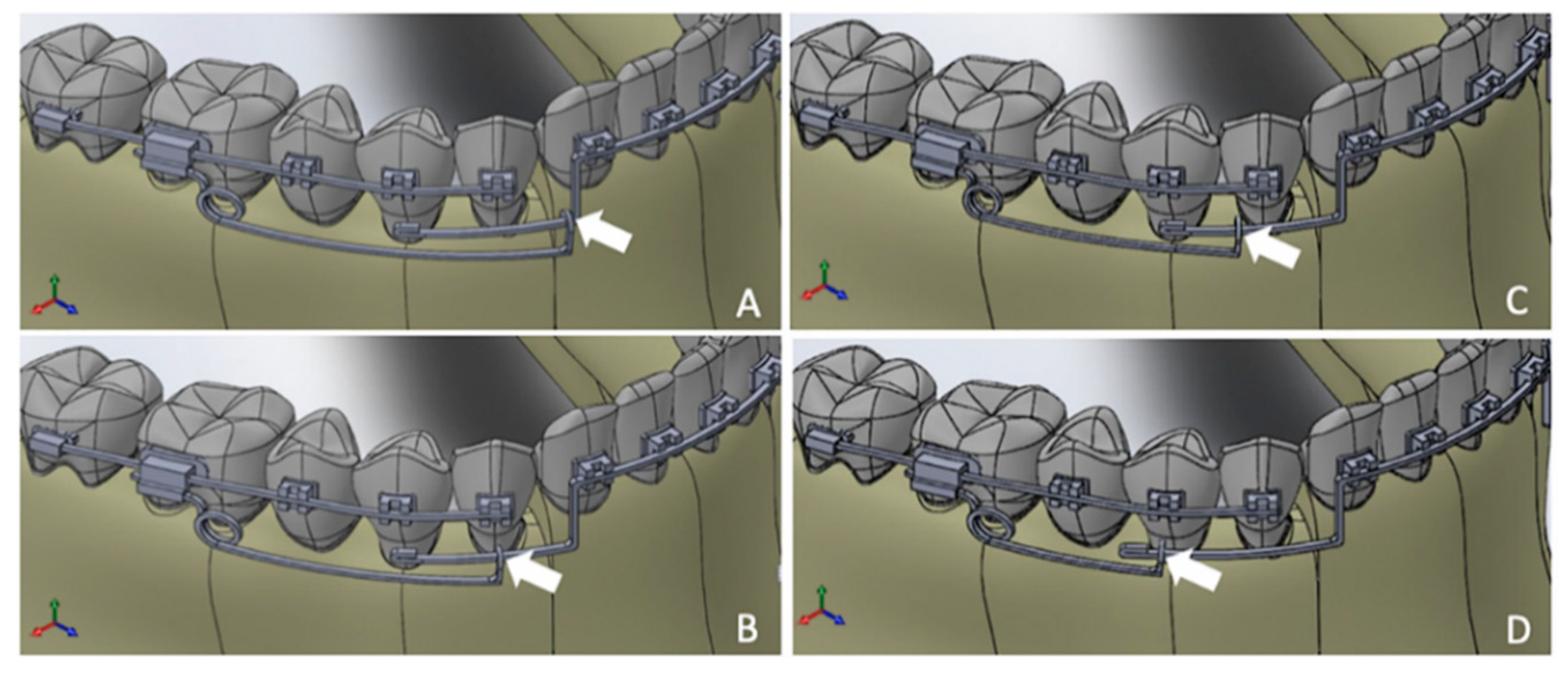
2.2. Simulated Points of Force Application
2.3. Discretization and Boundary Conditions
3. Results
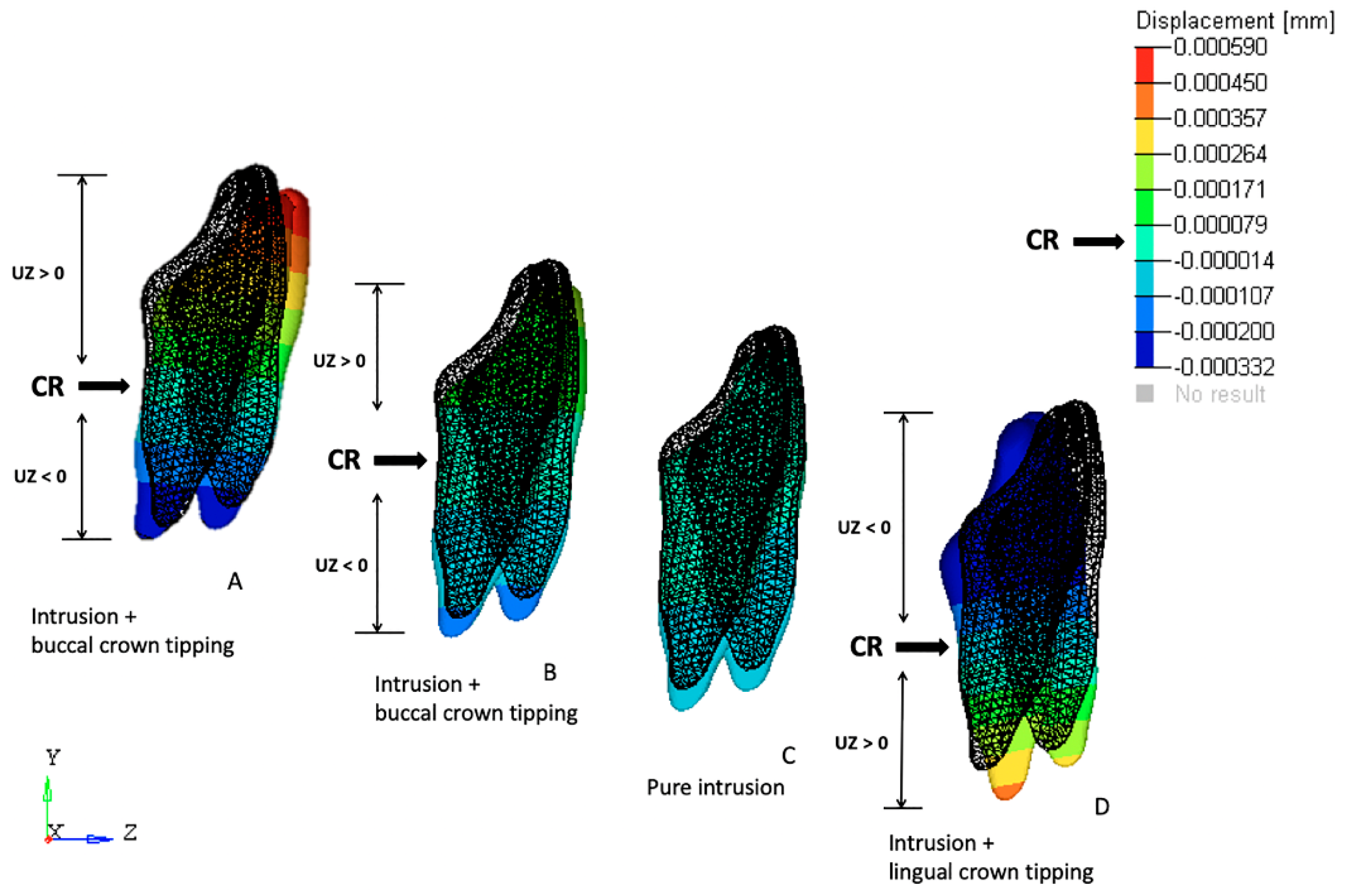
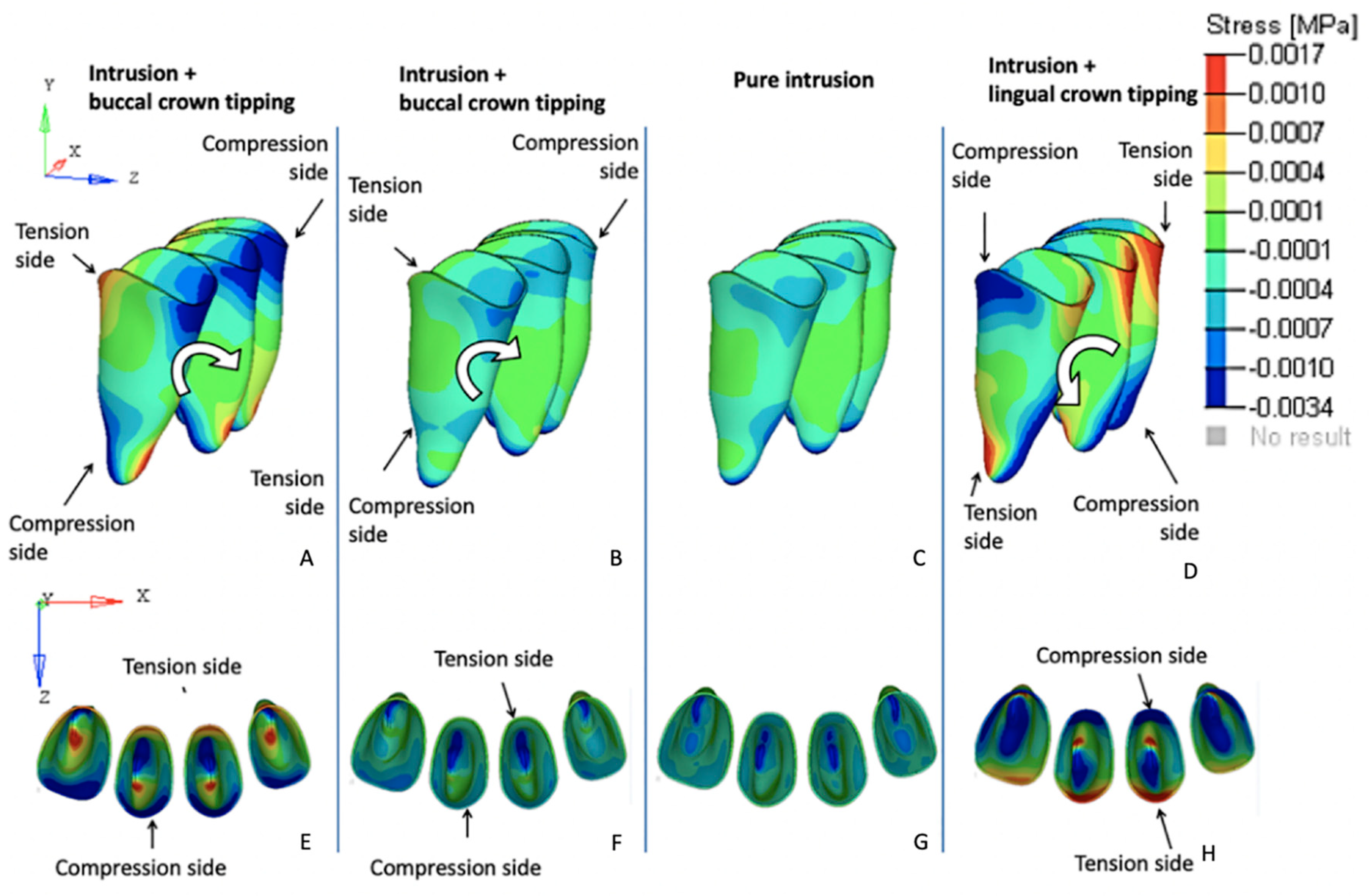
3.1. Effects on the Mandibular Incisors
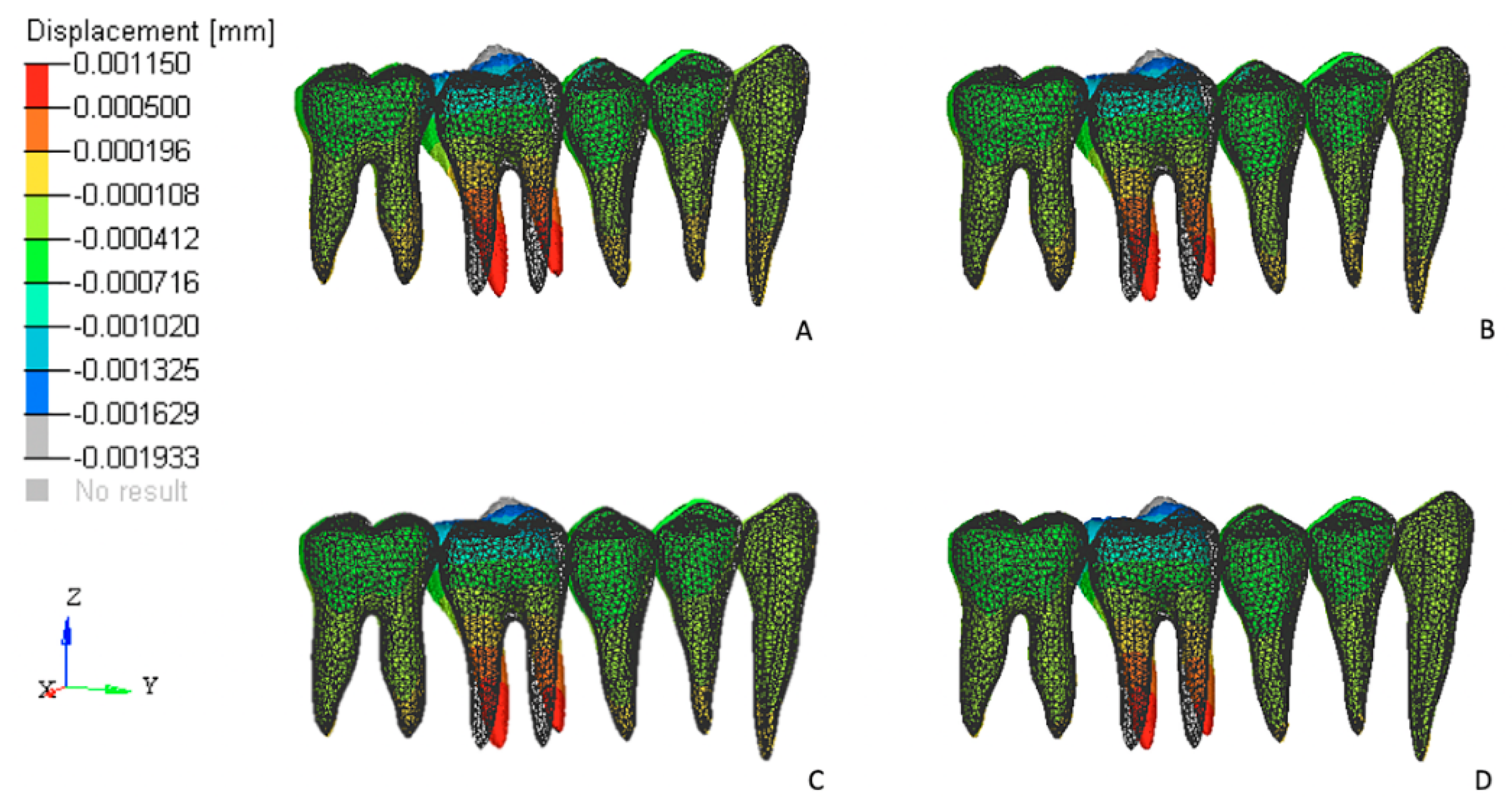
3.2. Effects on the Posterior Anchorage Segment
4. Discussion
5. Conclusions
- 1
- The FEM simulations indicated that pure mandibular incisor intrusion was registered when the point of force application on IBA was 2 mm distal to the center of the canine crown in this individual model. Intrusive forces applied mesially to this reference point generated labial crown tipping tendencies while forces applied more than 2 mm distally to the center of the canine resulted in lingual crown tipping of the mandibular incisors.
- 2
- The majority of the reaction forces registered on the posterior segments were concentrated on the first molar, and their effects were reduced when compared with the adjacent teeth on the anchorage unit.
Author Contributions
Funding
Conflicts of Interest
References
- Greig, D.G. Bioprogressive therapy: Overbite reduction with the lower utility arch. Br. J. Orthod. 1983, 10, 214–216. [Google Scholar] [CrossRef] [PubMed]
- Burstone, C.R. Deep overbite correction by intrusion. Am. J. Orthod. 1977, 72, 1–22. [Google Scholar] [CrossRef]
- Caballero, G.M.; de Carvalho Filho, O.A.; Hargreaves, B.O.; de A Brito, H.H.; Magalhães, P.A.A.; Oliveira, D.D. Mandibular canine intrusion with the segmented arch technique: A finite element method study. Am. J. Orthod. Dentofac. Orthop. 2015, 14, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.H.; Lim, S.H.; Gang, S.N. Reference points suitable for evaluation of the additional arch length required for leveling the curve of Spee. Korean J. Orthod. 2016, 46, 356–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thote, A.M.; Sharma, K.; Uddanwadiker, R.V.; Shrivastana, S. Optimum pure intrusion of mandibular canine with the segmented arch in lingual orthodontics. Bio-Med. Mater. Eng. 2017, 28, 247–256. [Google Scholar] [CrossRef]
- Braun, S.; Hnat, W.P.; Johnson, B.E. The curve of spee revisited. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 206–210. [Google Scholar] [CrossRef]
- Tweed, C.H. Clinical Orthodontics; C.V. Mosby: St Louis, MO, USA, 1966; pp. 461–547. [Google Scholar]
- Ricketts, R.M. Bioprogressive therapy as an answer to orthodontic needs. Part I. Am. J. Orthod. 1976, 70, 241–268. [Google Scholar] [CrossRef]
- Shioya, S.; Arai, K. Dentoskeletal morphology of adult Class II division 1 and severe deep overbite malocclusions. Orthod. Waves 2017, 76, 97–104. [Google Scholar] [CrossRef]
- Salehi, P.; Gerami, A.; Najafi, A.; Torkan, S. Evaluating stress distribution pattern in periodontal ligament of maxillary incisors during intrusion assessed by the finite element method. Dent. Shiraz Univ. Med. Sci. 2015, 16, 314–322. [Google Scholar]
- Veli, I.; Ozturk, M.A.; Uysal, T. Curve of Spee and its relationship to vertical eruption of teeth among different malocclusion groups. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 305–312. [Google Scholar] [CrossRef]
- Nayar, S.; Dinakarsamy, V.; Santhosh, S. Evaluation depth of the curve of Spee in class I, class II, and class III malocclusion: A cross sectional study. J. Pharm. Bioallied Sci. 2015, 7, 92–94. [Google Scholar] [CrossRef] [PubMed]
- Sayar, G.; Oktak, H. Assessment of curve of Spee in different malocclusions. Eur. Oral Res. 2018, 52, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Fattahi, H.; Pakshir, H.; Afzali, B.N.; Shahian, J.S. Skeletal and dentoalveolar features in patients with deep overbite malocclusion. J. Dent. (Tehran) 2014, 11, 629–638. [Google Scholar]
- Weiland, F.J.; Bantleon, H.P.; Droschl, H. Evaluation of continuous arch and segmented arch leveling techniques in adult patients-A clinical study. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 647–652. [Google Scholar] [CrossRef]
- Woods, M.G. The mechanics of lower incisor intrusion: Experiments in nongrowing baboons. Am. J. Orthod. Dentofac. Orthop. 1988, 93, 186–195. [Google Scholar] [CrossRef]
- Aydogdu, E.; Ozsoy, O.P. Effects of mandibular incisor intrusion obtained using a conventional utility arch vs. bone anchorage. Angl. Orthod. 2011, 81, 767–775. [Google Scholar] [CrossRef]
- Burstone, C.J. Rationale of the segmented arch. Am. J. Orthod. 1962, 48, 805–822. [Google Scholar] [CrossRef]
- Burstone, C.J. The mechanics of the segmented arch techniques. Angl. Orthod. 1966, 36, 99–120. [Google Scholar] [CrossRef]
- Shroff, B.; Lindauer, S.J.; Burstone, C.J.; Leiss, J.B. Segmented approach to simultaneous intrusion and space closure: Biomechanics of the three-Piece base arch appliance. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 136–143. [Google Scholar] [CrossRef]
- Shroff, B.; Yoon, W.M.; Lindauer, S.J.; Burstone, C.J. Simultaneous intrusion and retraction using a three-Piece base arch. Angl. Orthod. 1997, 67, 455–461. [Google Scholar] [CrossRef]
- Atik, E.; Gorucu-Coskuner, H.; Akarsu-Guven, B.; Taner, T. Evaluation of changes in the maxillary alveolar bone after incisor intrusion. Korean J. Orthod. 2018, 48, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Yared, K.F.; Zenobio, E.G.; Pacheco, W. Periodontal status of mandibular central incisors after orthodontic proclination in adults. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Chung, C.J.; Kim, K.H. Periodontal consequences of mandibular incisor proclination during presurgical orthodontic treatment in Class III malocclusion patients. Angl. Orthod. 2015, 85, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Sondhi, A. Anterior interferences: Their impact on anterior inclination and orthodontic finishing procedures. Semin. Orthod. 2003, 9, 204–215. [Google Scholar] [CrossRef]
- Rozzi, M.; Mucedero, M.; Pezzuto, C.; Lione, R.; Cozza, P. Long-Term stability of curve of Spee levelled with continuous arch wires in subjects with different vertical patterns: A retrospective study. Eur. J. Orthod. 2019, 41, 286–293. [Google Scholar] [CrossRef]
- Kojima, Y.; Fukui, H. A numerical simulation of tooth movement by wire bending. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 452–459. [Google Scholar] [CrossRef] [PubMed]
- McGrath, M.G.C.; Araujo-Monsalvo, V.M.; Murayama, N.; Martinez-Cruz, M.; Justus-Doczi, R.; Domínguez-Hermandez, V.M.; Ondarza-Rovira, R. Mandibular anterior intrusion using miniscrew for skeletal anchorage: A 3-Dimensional finite element analysis. Am. J. Orthod. Dentalfac. Orthop. 2018, 154, 469–476. [Google Scholar] [CrossRef]
- Ahuja, S.; Gupta, S.; Bhambri, E.; Ahuja, V.; Jaura, B.S. Comparison of conventional methods of simultaneous intrusion and retraction of maxillary anterior: A finite element analysis. J. Orthod. 2018, 45, 243–249. [Google Scholar] [CrossRef]
- Kojima, Y.; Kawamura, J.; Fukui, H. Finite element analysis of the effect of force directions on tooth movement in extraction space closure with miniscrew sliding mechanics. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 501–508. [Google Scholar] [CrossRef]
- Kim, K.Y.; Bayome, M.; Park, J.H.; Kim, K.B.; Mo, S.S.; Kook, Y.A. Displacement and stress distribution of the maxillofacial complex during maxillary protraction with buccal versus palatal plates: Finite element analysis. Eur. J. Orthod. 2015, 37, 275–283. [Google Scholar] [CrossRef]
- Gomes de Oliveira, S.; Seraidarian, P.I.; Landre, J., Jr.; Oliveira, D.D.; Cavalcanti, B.N. Tooth displacement due to occlusal contacts: A three-Dimensional finite element study. J. Oral Rehabil. 2006, 33, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, R.C. Textbook of Dental Anatomy and Physiology; W.B. Saunders: Philadelphia, PA, USA, 1949. [Google Scholar]
- Ishihara, Y.; Kuroda, S.; Sugawara, Y.; Balam, T.A.; Takano-Yamamoto, T.; Yamashiro, T. Indirect usage of miniscrew anchorage to intrude overerupted mandibular incisors in a Class II patient with a deep overbite. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 113–124. [Google Scholar] [CrossRef] [PubMed]
- El Namrawy, M.M.; El Sharaby, F.; Bushnak, M. Intrusive arch vesus miniscrew-Supported intrusion for the deep bite correction. Meced J. Med. Sci. 2019, 13, 1841–1846. [Google Scholar] [CrossRef]
- Pisek, P.; Manosupdprasit, M.; Wanngsrimogkol, T.; Keinprasit, C.; Wongpetch, R. Treatment of severe Class II Division 1 malocclusion combined with surgical miniscrew anchorage. Am. J. Orthod. Dentalfac. Orthop. 2019, 155, 572–583. [Google Scholar] [CrossRef] [PubMed]
- Jung, M.H. Vertical control of Class II deep bite malocclusion with the use of orthodontic mini-implants. Am. J. Orthod. Dentalfac. Orthop. 2019, 155, 264–275. [Google Scholar] [CrossRef] [PubMed]
- Senisik, N.E.; Turkkahraman, H. Treatment effects of intrusion arches and mini-Implant systems in deepbite patients. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Tweed, C.H. The frankfort-mandibular plane angle in orthodontic diagnosis, classification, treatment planning, and prognosis. Am. J. Orthod. Oral Surg. 1946, 32, 175–230. [Google Scholar] [CrossRef]
- Chiqueto, K.; Martins, D.R.; Janson, G. Effects of accentuated and reversed curve of Spee on apical root resorption. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 261–268. [Google Scholar] [CrossRef]
- Costopoulos, G.; Nanda, R. An evaluation of root resorption incident to orthodontic intrusion. Am. J. Orthod. Dentofac. Orthop. 1996, 109, 543–548. [Google Scholar] [CrossRef] [Green Version]
- Lindauer, S.J.; Isaacson, R.J. One-couple orthodontic appliance systems. Semin. Orthod. 1995, 1, 12–24. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Elastic Modulus (E) (Mpa) | Poisson‘s Ratio (v) | |
|---|---|---|
| Tooth | 20.000 | 0.30 |
| PDL | 0.71 | 0.40 |
| Bone | 345 | 0.30 |
| SS | 200.000 | 0.30 |
| TMA | 69.000 | 0.30 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Brito, G.M.; Brito, H.H.d.A.; Marra, G.G.M.; Freitas, L.R.P.; Hargreaves, B.O.; Magalhães, P.A.A., Jr.; Oliveira, D.D. Pure Mandibular Incisor Intrusion: A Finite Element Study to Evaluate the Segmented Arch Technique. Materials 2019, 12, 2784. https://doi.org/10.3390/ma12172784
de Brito GM, Brito HHdA, Marra GGM, Freitas LRP, Hargreaves BO, Magalhães PAA Jr., Oliveira DD. Pure Mandibular Incisor Intrusion: A Finite Element Study to Evaluate the Segmented Arch Technique. Materials. 2019; 12(17):2784. https://doi.org/10.3390/ma12172784
Chicago/Turabian Stylede Brito, Gabriela Meyge, Hélio Henrique de Araújo Brito, Gabriel Goulart Mendes Marra, Laíze Rosa Pires Freitas, Bernardo Oliveira Hargreaves, Pedro Américo Almeida Magalhães, Jr., and Dauro Douglas Oliveira. 2019. "Pure Mandibular Incisor Intrusion: A Finite Element Study to Evaluate the Segmented Arch Technique" Materials 12, no. 17: 2784. https://doi.org/10.3390/ma12172784
APA Stylede Brito, G. M., Brito, H. H. d. A., Marra, G. G. M., Freitas, L. R. P., Hargreaves, B. O., Magalhães, P. A. A., Jr., & Oliveira, D. D. (2019). Pure Mandibular Incisor Intrusion: A Finite Element Study to Evaluate the Segmented Arch Technique. Materials, 12(17), 2784. https://doi.org/10.3390/ma12172784