Comparative Analysis of Biofilm Removal Efficacy by Multisonic Ultracleaning System and Passive Ultrasonic Activation

Abstract
:1. Introduction
2. Materials and Methods
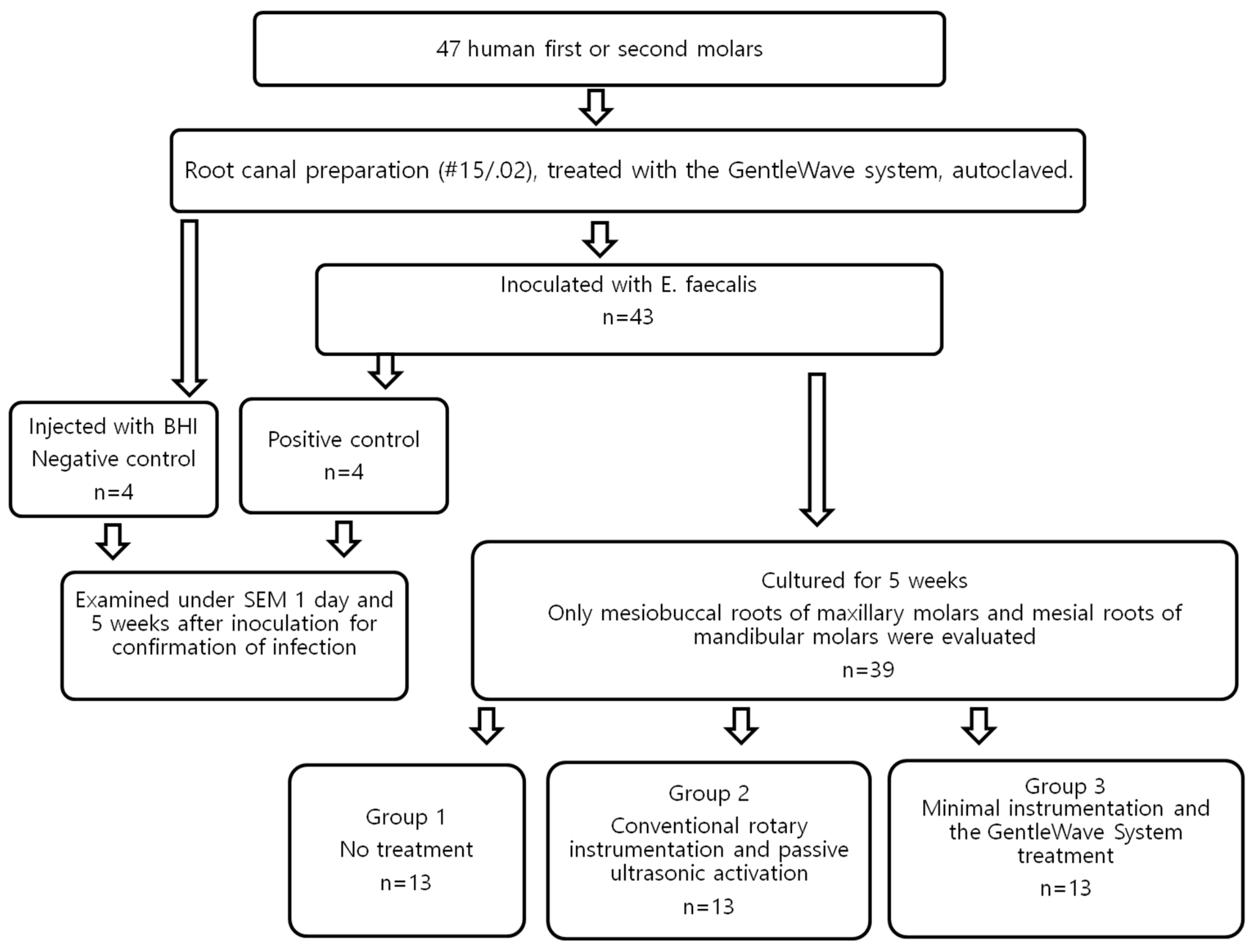
2.1. Sample Selection
2.2. Sample Preparation
2.3. Sample Inoculation
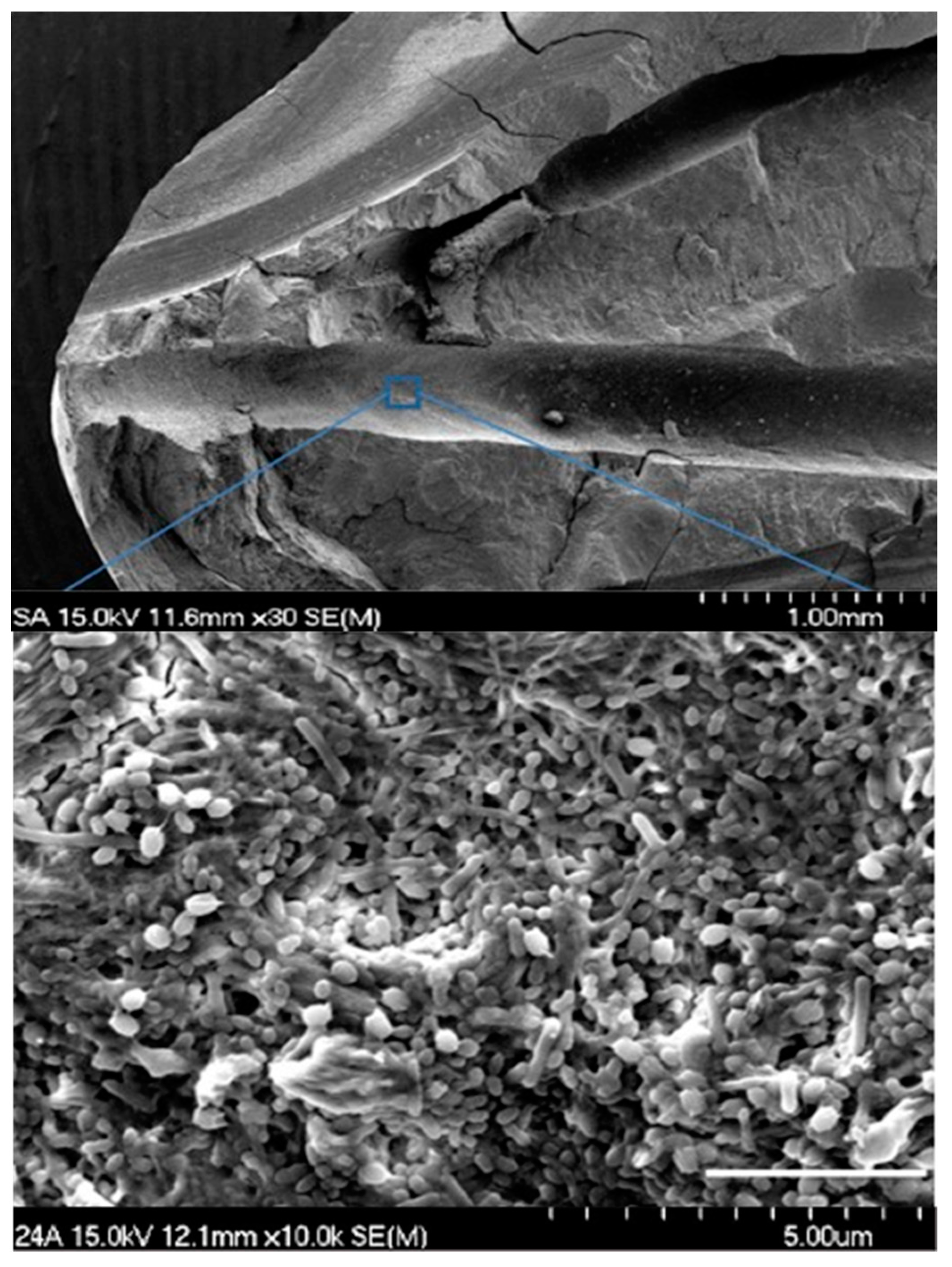
2.4. Confirmation of Infection
2.5. Treatment Groups
- (1)
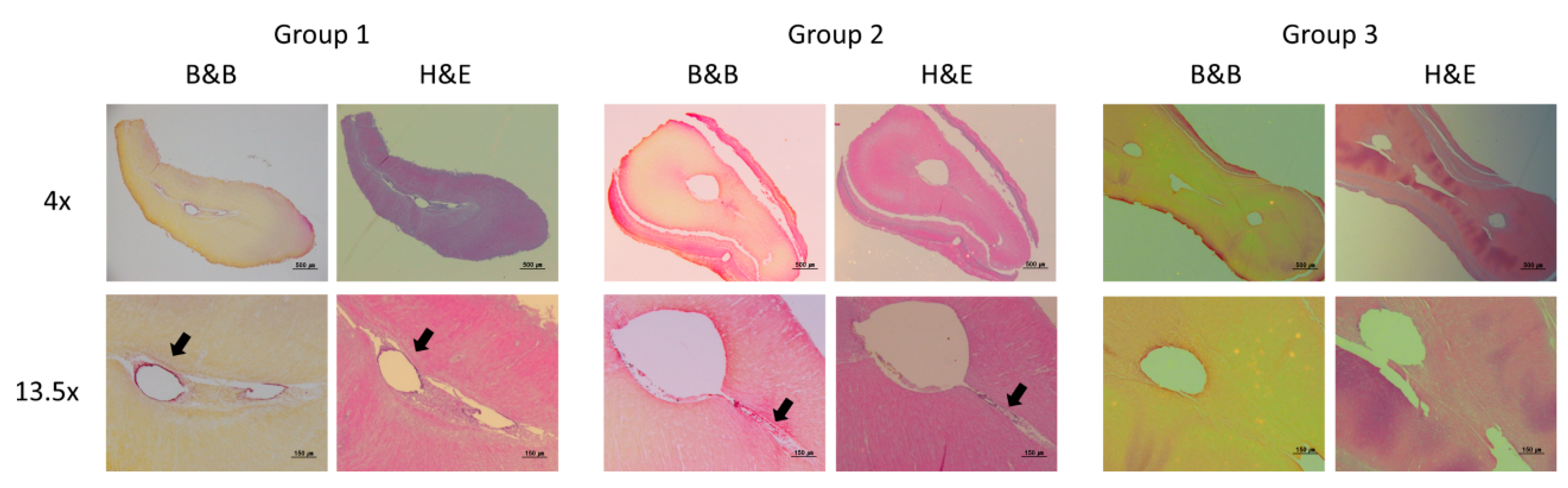
- Group 1—No treatment (n = 13): Teeth in the control group did not undergo any endodontic treatment after inoculation with E. faecalis.
- (2)
- Group 2—Conventional rotary instrumentation and passive ultrasonic activation with the PiezonMaster™ 700 ESI tip (n = 13): The canals were instrumented to a size #20 K-file to reach the working length. The canals were further instrumented with Protaper rotary filing system (Protaper, Irvine, CA, USA) in a sequence of S1/S2/F1/F2 followed by #35/.04 EndoSequence rotary file (Brasseler, Savannah, GA, USA) to working length. 1 mL of 3% Sodium hypochlorite (NaOCl) was again delivered in between each instrument using a syringe and 30G Max-i-Probe needle to flush out the dentin debris created during instrumentation. The canals were irrigated with 3% NaOCl at a flow rate of 3 mL/min for 10 s per canal. Each canal was activated for 60 s per canal at maximum power in Endo mode using PiezonMaster 700 with an ESI tip (Electro Medical Systems, Nyon, Switzerland) [15,17,18,19]. This irrigation-activation process was repeated once for all the canals at the end of root canal instrumentation. The canals were then irrigated with sterile distilled water using a Max-i-Probe needle for 10 s per canal. This was followed by irrigation with 17% EDTA for 10 s per canal at a flow rate of 3 mL/min. The needle was placed 2 mm from the apical foramen. Final activation was performed with sterile distilled water for 10 s per canal. All canals were dried with sterile paper points.
- (3)
- Group 3—Minimal instrumentation and the GentleWave treatment (n = 13): The canals were instrumented with #15/.04 EndoSequence rotary files. 1 mL of saline was delivered in between each instrument using a syringe and 30G Max-i-Probe needle to flush out the dentin debris created during instrumentation. For the GentleWave treatments, the handpiece tip was placed inside the pulp chamber of the accessed tooth. According to the manufacturer’s instruction for use, the treatment consisted of 3% NaOCl for 5 min, sterile-distilled water for 30 s, 8% EDTA for 2 min, and sterile-distilled water for 15 s, sequentially [11,12,13,14,20]. All the canals were dried with sterile paper points. Only 8% EDTA was used, as recommended by the manufacturer. All the treatment flows are illustrated in Figure 1.
2.6. Sample Processing
2.7. Data Analysis
2.8. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mohammadi, Z.; Palazzi, F.; Giardino, L.; Shalavi, S. Microbial biofilms in endodontic infections: An update review. Biomed. J. 2013, 36, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D.; Siqueira, J. Biofilms and apical periodontitis: Study of prevalence and association with clinical and histopathologic findings. JOE 2010, 36, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Carpio-Perochena, A.E.; Bramante, C.M.; Duarte, M.A.H.; Cavenago, B.C.; Villas-Boas, M.H.; Graeff, M.S.; Bernardineli, N.; de Andrade, F.B.; Ordinola-Zaata, R. Biofilm dissolution and cleaning ability of different irrigant solutions on intraorally infected dentin. JOE 2011, 37, 1134–1138. [Google Scholar] [CrossRef] [PubMed]
- Svensäter, G.; Bergenholtz, G. Biofilms in endodontic infections. Endod. Top. 2004, 9, 27–36. [Google Scholar] [CrossRef]
- Nair, P.N.R.; Henry, S.; Cano, V.; Vera, J. Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after one-visit endodontic treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 99, 231–252. [Google Scholar] [CrossRef]
- Paiva, S.S.M.; Siqueira, J.F.; Rôças, I.N.; Carmo, F.L.; Leite, D.C.A.; Ferreira, D.C.; Rachid, C.T.C.; Rosado, A.S. Molecular microbiological evaluation of passive ultrasonic activation as a supplementary disinfecting step: A clinical study. JOE 2013, 39, 190–194. [Google Scholar] [CrossRef]
- Mozo, S.; Llena, C.; Forner, L. Review of ultrasonic irrigation in endodontics: Increasing action of irrigating solutions. Med. Oral Patol. Oral Cir. Bucal 2012, 17, 512–516. [Google Scholar] [CrossRef]
- Ordinola-Zapata, R.; Bramante, C.M.; Aprecio, R.M.; Handysides, R.; Jaramillo, D.E. Biofilm removal by 6% sodium hypochlorite activated by different irrigation techniques. Int. Endod. J. 2013, 47, 659–666. [Google Scholar] [CrossRef]
- Case, P.D.; Bird, P.S.; Kahler, W.A.; George, R.; Walsh, L.J. Treatment of root canal biofilms of Enterococcus faecalis with ozone gas and passive ultrasound activation. JOE 2012, 38, 523–526. [Google Scholar] [CrossRef]
- Joy, J.; Mathias, J.; Sagir, V.M.M.; Babu, B.P.; Chirayath, K.J.; Hameed, H. Bacterial Biofilm Removal Using Static and Passive Ultrasonic Irrigation. JIOH 2015, 7, 42–47. [Google Scholar]
- Haapasalo, M.; Wang, Z.; Shen, Y.; Curtis, A.; Patel, P.; Khakpour, M. Tissue dissolution by a novel multisonic ultracleaning system and sodium hypochlorite. JOE 2014, 40, 1178–1181. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Shen, Y.; Yang, Y.; Gao, Y.; Wan, P.; Gan, Y.; Patel, P.; Curtis, A.; Khakpour, M.; Haapasalo, M. In vitro study of calcium hydroxide removal from mandibular molar root canals using a GentleWave™System. JOE 2015, 41, 553–558. [Google Scholar] [PubMed]
- Charara, K.; Friedman, S.; Sherman, A.; Kishen, A.; Malkhassian, G.; Khakpour, M.; Basrani, B. Assessment of apical extrusion during root canal procedure with the novel GentleWave System in a simulated apical environment. JOE 2016, 42, 135–139. [Google Scholar] [PubMed]
- Molina, B.; Glickman, G.; Vandrangi, P.; Khakpour, M. Evaluation of root canal debridement of human molars using the GentleWave™ System. JOE 2015, 41, 1701–1705. [Google Scholar] [CrossRef] [PubMed]
- Yoo, Y.; Lee, W.; Kim, H.; Shon, W.; Baek, S. Multivariate analysis of the cleaning efficacy of different final irrigation techniques in the canal and isthmus of mandibular posterior teeth. RDE 2013, 38, 154–159. [Google Scholar] [CrossRef]
- Garg, N.; Garg, A. Textbook of Endodontics, 1st ed.; Boydell & Brewer Ltd.: Suffolk, UK, 2010. [Google Scholar]
- Paragliola, R.; Franco, V.; Fabiani, C.; Mazzoni, A.; Naot, F.; Tay, F.R.; Breschi, L.; Grandini, S. Final rinse optimization: Influence of different agitation protocols. JOE 2010, 36, 282–285. [Google Scholar] [CrossRef]
- Böttcher, D.E.; Rahde, N.D.; Grecca, F.S. Calcium hydroxide removal: Effectiveness of ultrasonic and manual techniques. Rev. Odonto Ciência 2012, 27, 152–155. [Google Scholar] [CrossRef]
- Wiseman, A.; Cox, T.C.; Paranjpe, A.; Flake, N.M.; Cohenca, N.; Johnson, J.D. Efficacy of sonic and ultrasonic activation for removal of calcium hydroxide from mesial canals of mandibular molars: A microtomographic study. JOE 2011, 37, 235–238. [Google Scholar] [CrossRef]
- Sigurdsson, A.; Garland, R.W.; Le, K.T.; Woo, S.M. Twelve-month healing rates after endodontic therapy using the novel GentleWave System: The PURE prospective multi-center clinical study. JOE 2016, 42, 1040–1048. [Google Scholar] [PubMed]
- Pinheiro, S.L.; Frasson, A.D.; Bincelli, I.N.; Barros, P.P.; Silva, G.H. Study of a morphometric model for histological evaluation of the collagen in dentin carious lesions. J. Ped. Dent. 2009, 33, 123–126. [Google Scholar] [CrossRef]
- Berkovitz, B.K.B.; Holland, G.R.; Moxham, B.J. Oral Anatomy, Histology and Embryology, 3rd ed.; Mosby: St. Louis, MO, USA, 2002. [Google Scholar]
- Fouad, A.F.; Zerella, J.; Barry, J.; Spangberg, L.S. Molecular detection of Enterococcus species in root canals of therapy-resistant endodontic infections. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 99, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Bystrom, A.; Sundqvist, G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int. Endod. J. 1985, 18, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Ørstavik, D.; Haapasalo, M. Disinfection by endodontic irrigants and dressings of experimentally infected dentinal tubules. Endod Dent. Trauma 1990, 6, 142–149. [Google Scholar] [CrossRef]
- Kovac, J.; Kovac, D. Effect of irrigating solutions in endodontic therapy. Bratisl. Lek. Listy 2011, 112, 410–415. [Google Scholar] [PubMed]
- Jaju, S.; Jaju, P. Newer root canal irrigants in horizon: A review. Int. J. Dent. 2011, 851359, 9. [Google Scholar] [CrossRef]
- Vera, J.; Siqueira, J.F.; Ricucci, D.; Loghin, S.; Fernandez, N.; Flores, B.; Cruz, A.G. One- versus two-visit endodontic treatment of teeth with apical periodontitis: A histobacteriologic study. JOE 2012, 38, 1040–1052. [Google Scholar] [CrossRef]
- Bhuva, B.; Patel, S.; Wilson, R.; Niazi, S.; Beighton, D.; Mannocci, F. The effectiveness of passive ultrasonic irrigation on intraradicular Enterococcus faecalis biofilms in extracted single-rooted human teeth. Int. Endod. J. 2010, 43, 241–250. [Google Scholar] [CrossRef]
- Ma, J.; Wang, Z.; Shen, Y.; Haapasalo, M. A new noninvasive model to study the effectiveness of dentin disinfection by using confocal laser scanning microscopy. JOE 2011, 37, 1380–1385. [Google Scholar] [CrossRef]
- Zhang, D.; Shen, Y.; Fuente-Nunez, C.; Haapasalo, M. In vitro evaluation by quantitative real-time PCR and culturing of the effectiveness of disinfection of multispecies biofilms in root canals by two irrigation systems. Clin. Oral Investig. 2019 23, 913–920. [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
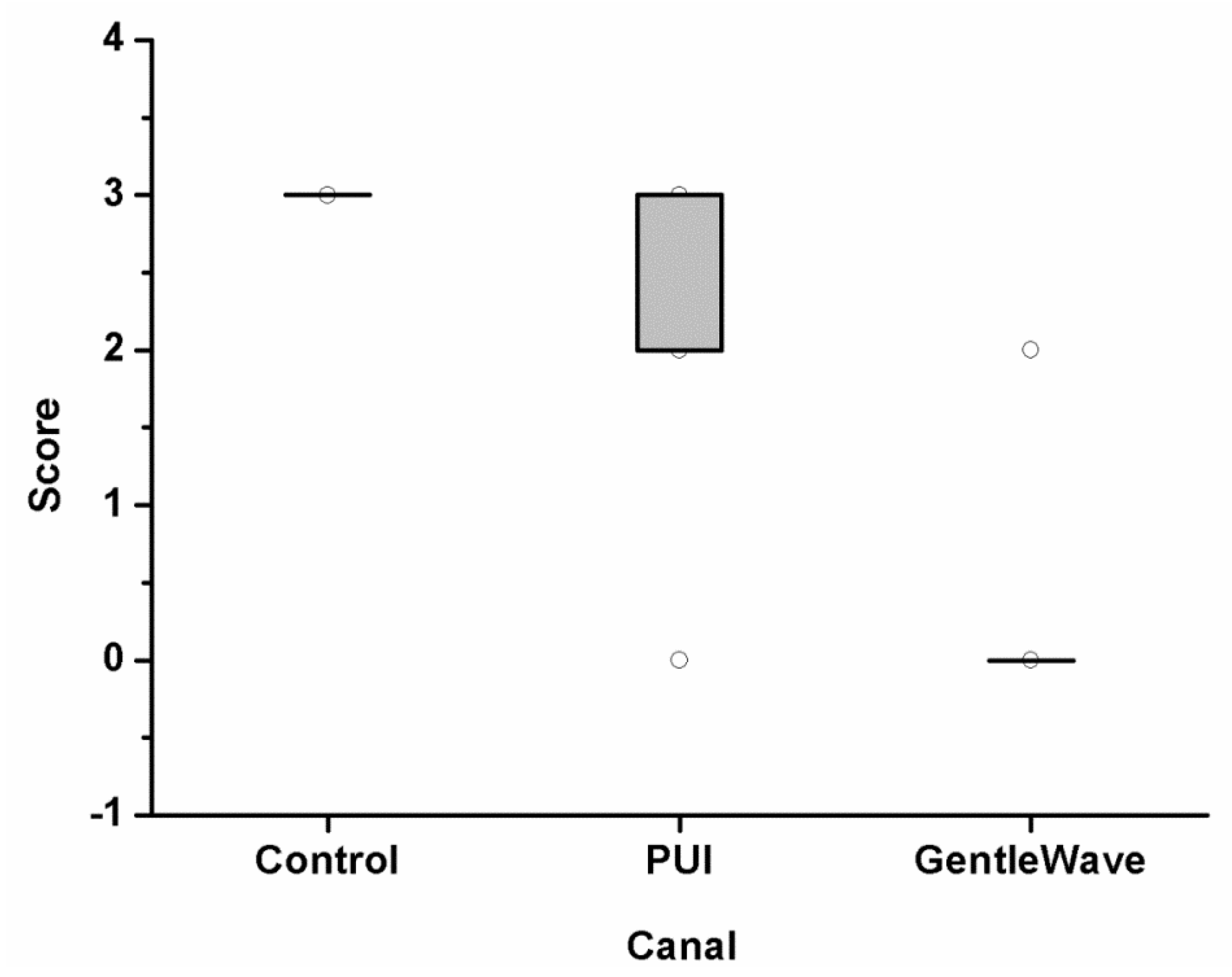
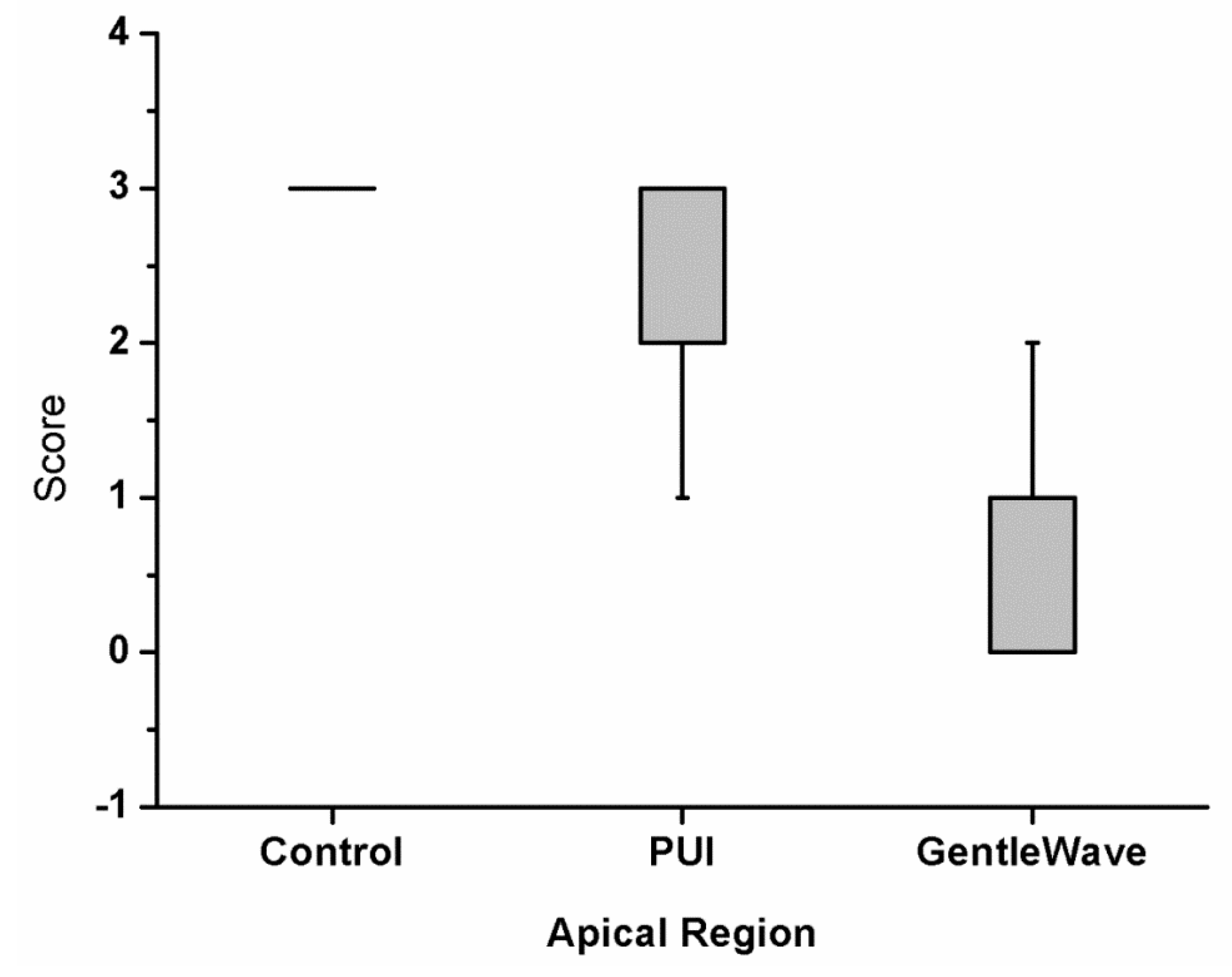
| Control | PUI | GentleWave | p-Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Canal | Isthmus | Canal | Isthmus | Canal | Isthmus | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| 3w | 0 | 3a | 0 | 1.94x | 1.20 | 2.75b | 0.39 | 0.15y | 0.55 | 0.33c | 0.74 | p < 0.05 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.W.; Park, S.Y.; Kang, M.K.; Shon, W.J. Comparative Analysis of Biofilm Removal Efficacy by Multisonic Ultracleaning System and Passive Ultrasonic Activation. Materials 2019, 12, 3492. https://doi.org/10.3390/ma12213492
Choi HW, Park SY, Kang MK, Shon WJ. Comparative Analysis of Biofilm Removal Efficacy by Multisonic Ultracleaning System and Passive Ultrasonic Activation. Materials. 2019; 12(21):3492. https://doi.org/10.3390/ma12213492
Chicago/Turabian StyleChoi, Hae Won, Seong Yeon Park, Mo Kwan Kang, and Won Jun Shon. 2019. "Comparative Analysis of Biofilm Removal Efficacy by Multisonic Ultracleaning System and Passive Ultrasonic Activation" Materials 12, no. 21: 3492. https://doi.org/10.3390/ma12213492
APA StyleChoi, H. W., Park, S. Y., Kang, M. K., & Shon, W. J. (2019). Comparative Analysis of Biofilm Removal Efficacy by Multisonic Ultracleaning System and Passive Ultrasonic Activation. Materials, 12(21), 3492. https://doi.org/10.3390/ma12213492