In Vitro Simulation and In Vivo Assessment of Tooth Wear: A Meta-Analysis of In Vitro and Clinical Research





Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Registration and Reporting
2.2. Eligibility Criteria
- -
- Study design: Clinical studies comprising randomized controlled (RCTs) studies or controlled clinical trials as well as in vitro simulation studies with extracted teeth as control groups;
- -
- Participants: For clinical studies, participants of both sexes and of any age range were included. Prosthetic–enamel or enamel–enamel tooth interfaces were considered. For in vitro research, intact extracted human teeth of any type were considered eligible. Enamel laboratory-produced surface or cut enamel, enamel slabs, or plates were excluded;
- -
- Intervention: Intact enamel of teeth;
- -
- Comparator: Any type of prosthetic material or enamel antagonist; and
- -
- Outcome(s): Enamel tooth wear was the primary outcome considered. This included assessment methods within the range of but not confined to volume loss, vertical wear, height loss, and depth wear. Roughness changes in enamel surface were not considered.
2.3. Search Strategy
2.4. Data Extraction
2.5. Risk of Bias Assessment within Individual Studies
2.6. Summary Measures and Data Synthesis
2.7. Risk of Bias Across Studies
2.8. Additional Analyses
3. Results
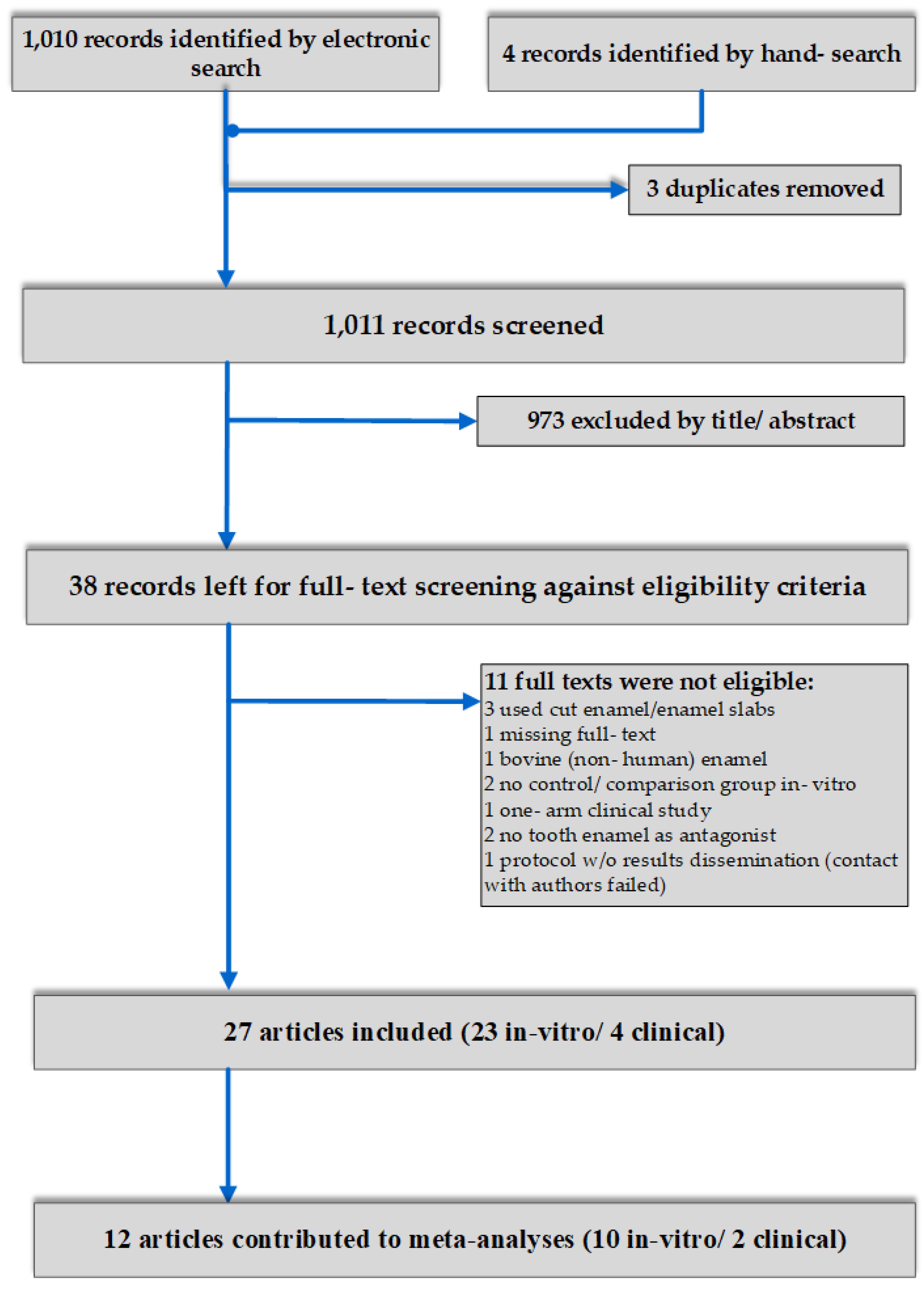
3.1. Search Details
3.2. Study Design and Characteristics
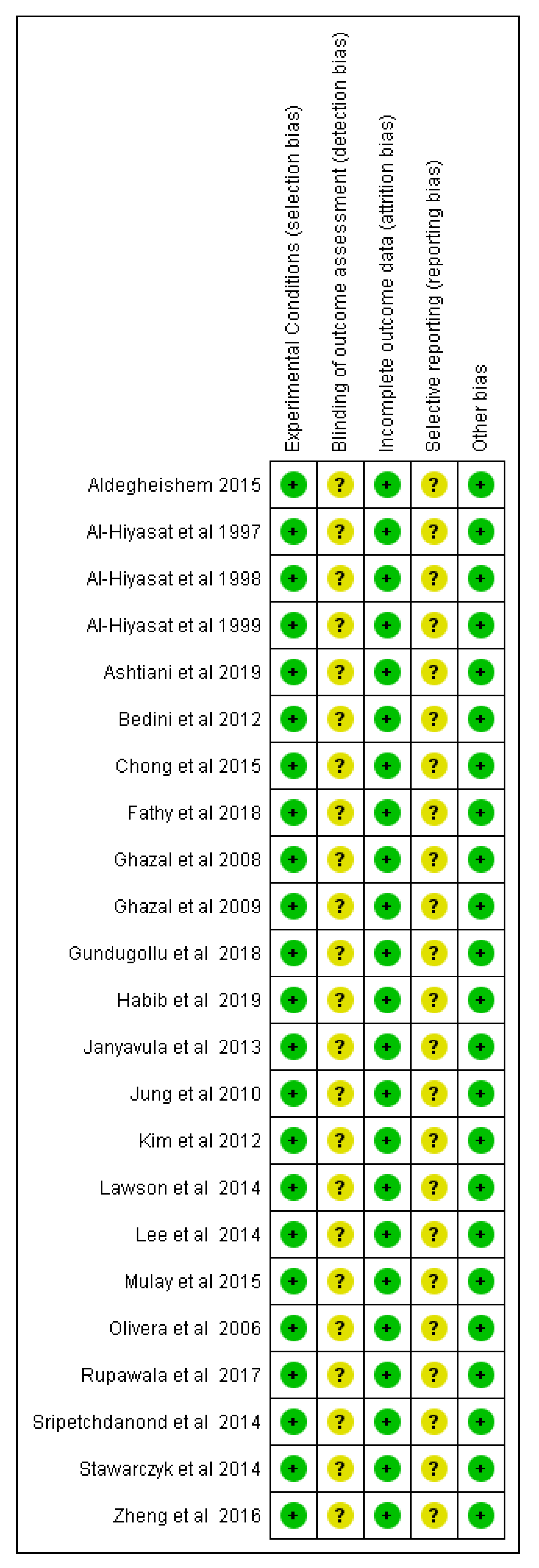
3.3. Risk of Bias within Studies
3.4. Effects of Interventions, Meta-Analyses, and Additional Analyses
4. Discussion
4.1. Summary of the Evidence
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Lucas, P.W.; Omar, R.; Al-Fadhalah, K.; Almusallam, A.S.; Henry, A.G.; Michael, S.; Thai, L.A.; Watzke, J.; Strait, D.S.; Atkins, A.G. Mechanisms and causes of wear in tooth enamel: Implications for hominin diets. J. R. Soc. Interface 2013, 10, 20120923. [Google Scholar] [CrossRef]
- Mundhe, K.; Jain, V.; Pruthi, G.; Shah, N. Clinical study to evaluate the wear of natural enamel antagonist to zirconia and metal ceramic crowns. J. Prosthet. Dent. 2015, 114, 358–363. [Google Scholar] [CrossRef]
- Oh, W.-S.; Delong, R.; Anusavice, K.J. Factors affecting enamel and ceramic wear: A literature review. J. Prosthet Dent. 2002, 87, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Olley, R.C.; Sehmi, H. The rise of dentine hypersensitivity and tooth wear in an ageing population. Br. Dent. J. 2017, 223, 293–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterenborg, B.A.M.M.; Kalaykova, S.I.; Loomans, B.A.C.; Huysmans, M.-C.D.N.J.M. Impact of tooth wear on masticatory performance. J. Dent. 2018, 76, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Habib, S.R.; Alotaibi, A.; Al Hazza, N.; Allam, Y.; AlGhazi, M. Two-body wear behavior of human enamel versus monolithic zirconia, lithium disilicate, ceramometal and composite resin. J. Adv. Prosthodont. 2019, 11, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Makvandi, P.; Gu, J.T.; Zare, E.N.; Ashtari, B.; Moeini, A.; Tay, F.R.; Niu, L.-N. Polymeric and inorganic nanoscopical antimicrobial fillers in dentistry. Acta Biomater. 2019. [Google Scholar] [CrossRef] [PubMed]
- Heintze, S.D.; Cavalleri, A.; Forjanic, M.; Zellweger, G.; Rousson, V. Wear of ceramic and antagonist—A systematic evaluation of influencing factors in vitro. Dent. Mater. 2008, 24, 433–449. [Google Scholar] [CrossRef]
- Zandparsa, R.; El Huni, R.M.; Hirayama, H.; Johnson, M.I. Effect of different dental ceramic systems on the wear of human enamel: An in vitro study. J. Prosthet. Dent. 2016, 115, 230–237. [Google Scholar] [CrossRef]
- Shimane, T.; Endo, K.; Zheng, J.H.; Yanagi, T.; Ohno, H. Wear of opposing teeth by posterior composite resins—Evaluation of newly developed wear test methods. Dent. Mater. J. 2010, 29, 713–720. [Google Scholar] [CrossRef]
- Sripetchdanond, J.; Leevailoj, C. Wear of human enamel opposing monolithic zirconia, glass ceramic, and composite resin: An in vitro study. J. Prosthet. Dent. 2014, 112, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- He, L.H.; Swain, M.V. Nanoindentation derived stress-strain properties of dental materials. Dent. Mater. 2007, 23, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Constantino, P.J.; Borrero-Lopez, O.; Pajares, A.; Lawn, B.R. Simulation of enamel wear for reconstruction of diet and feeding behavior in fossil animals: A micromechanics approach. BioEssays 2016, 38, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Lawn, B.R. Indentation of Ceramics with Spheres: A Century after Hertz. J. Am. Ceram. Soc. 2005, 81, 1977–1994. [Google Scholar] [CrossRef]
- Stawarczyk, B.; Özcan, M.; Schmutz, F.; Trottmann, A.; Roos, M.; Hämmerle, C.H.F. Two-body wear of monolithic, veneered and glazed zirconia and their corresponding enamel antagonists. Acta Odontol. Scand. 2013, 71, 102–112. [Google Scholar] [CrossRef]
- Chong, B.J.; Thangavel, A.K.; Rolton, S.B.; Guazzato, M.; Klineberg, I.J. Clinical and laboratory surface finishing procedures for zirconia on opposing human enamel wear: A laboratory study. J. Mech. Behav. Biomed. Mater. 2015, 50, 93–103. [Google Scholar] [CrossRef]
- Mulay, G.; Dugal, R.; Buhranpurwala, M. An evaluation of wear of human enamel opposed by ceramics of different surface finishes. J. Indian Prosthodont. Soc. 2015, 15, 111–118. [Google Scholar] [CrossRef]
- Esquivel-Upshaw, J.F.; Kim, M.J.; Hsu, S.M.; Abdulhameed, N.; Jenkins, R.; Neal, D.; Ren, F.; Clark, A.E. Randomized clinical study of wear of enamel antagonists against polished monolithic zirconia crowns. J. Dent. 2018, 68, 19–27. [Google Scholar] [CrossRef]
- Yang, S.-W.; Kim, J.-E.; Shin, Y.; Shim, J.-S.; Kim, J.-H. Enamel wear and aging of translucent zirconias: In vitro and clinical studies. J. Prosthet. Dent. 2019, 121, 417–425. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Egger, M.; Moher, D. Addressing reporting biases, Cochrane Handbook for Systematic Reviews of Intervention. In Cochrane Collaboration; Version 5.1.0; Chichester, UK, 2011; Available online: http://www.handbook.cochrane.org (accessed on 20 October 2019).
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Stober, T.; Bermejo, J.L.; Rammelsberg, P.; Schmitter, M. Enamel wear caused by monolithic zirconia crowns after 6 months of clinical use. J. Oral. Rehabil. 2014, 41, 314–322. [Google Scholar] [CrossRef]
- Aldegheishem, A.; Alfaer, A.; Brezavšček, M.; Vach, K.; Eliades, G.; Att, W. Wear behavior of zirconia substrates against different antagonist materials. Int. J. Esthet. Dent. 2015, 10, 468–485. [Google Scholar]
- Sulong, M.Z.; Aziz, R.A. Wear of materials used in dentistry: A review of the literature. J. Prosthet. Dent. 1990, 63, 342–349. [Google Scholar] [CrossRef]
- Anusavice, K.J.; Shen, C.; Rawls, R. Phillips’ Science of Dental Materials, 12th ed.; Elsevier: St Louis, MO, USA, 2013. [Google Scholar]
- Kurt, M.; Turhan Bal, B. Effects of accelerated artificial aging on the translucency and color stability of monolithic ceramics with different surface treatments. J. Prosthet. Dent. 2019, 121, 712.e1–712.e8. [Google Scholar] [CrossRef]
- Ratledge, D.K.; Smith, B.G.; Wilson, R.F. The effect of restorative materials on the wear of human enamel. J. Prosthet. Dent. 1994, 72, 194–203. [Google Scholar] [CrossRef]
- Ashtiani, A.H.; Azizian, M.; Rohani, A. Comparison the degree of enamel wear behavior opposed to Polymer-infiltrated ceramic and feldspathic porcelain. Dent. Res. J. 2019, 16, 71–75. [Google Scholar]
- Lambrechts, P.; Braem, M.; Vuylsteke-Wauters, M.; Vanherle, G. Quantitative in vivo wear of human enamel. J. Dent. Res. 1989, 68, 1752–1754. [Google Scholar] [CrossRef] [PubMed]
- Heintze, S.D.; Faouzi, M.; Rousson, V.; Ozcan, M. Correlation of wear in vivo and six laboratory wear methods. Dent. Mater. 2012, 28, 961–973. [Google Scholar] [CrossRef] [PubMed]
- de Gee, A.J.; Pallav, P. Occlusal wear simulation with the ACTA wear machine. J. Dent. 1994, 22 (Suppl. 1), S21–S27. [Google Scholar] [CrossRef]
- Leinfelder, K.F.; Beaudreau, R.W.; Mazer, R.B. An in vitro device for predicting clinical wear. Quint. Int. 1989, 20, 755–761. [Google Scholar]
- Mehl, A.; Gloger, W.; Kunzelmann, K.H.; Hickel, R. A new optical 3-D device for the detection of wear. J. Dent. Res. 1997, 76, 1799–1807. [Google Scholar] [CrossRef] [PubMed]
- Zantner, C.; Kielbassa, A.M.; Martus, P.; Kunzelmann, K.-H. Sliding wear of 19 commercially available composites and compomers. Dent. Mater. 2004, 20, 277–285. [Google Scholar] [CrossRef]
- Condon, J.R.; Ferracane, J.L. Evaluation of composite wear with a new multi-mode oral wear simulator. Dent. Mater. 1996, 12, 218–226. [Google Scholar] [CrossRef]
- Krejci, I.; Reich, T.; Lutz, F.; Albertoni, M. In-vitro-Testverfahren zur Evaluation dentaler Restaurationssysteme. 1. Computergesteuerter Kausimulator. Quint. Int. 1990, 100, 953–960. [Google Scholar]
- Wulfman, C.; Koenig, V.; Mainjot, A.K. Wear measurement of dental tissues and materials in clinical studies: A systematic review. Dent. Mater. 2018, 34, 825–850. [Google Scholar] [CrossRef]
- Heintze, S.D.; Zellweger, G.; Sbicego, S.; Rousson, V.; Muñoz-Viveros, C.; Stober, T. Wear of two denture teeth materials in vivo-2-year results. Dent. Mater. 2013, 29, e191–e204. [Google Scholar] [CrossRef] [PubMed]
- Stober, T.; Geiger, A.; Rues, S.; Dreyhaupt, J.; Rammelsberg, P.; Ohlmann, B. Factors affecting wear of composite resin denture teeth—24-month results from a clinical study. Clin. Oral. Investig. 2012, 16, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Esquivel-Upshaw, J.F.; Young, H.; Jones, J.; Yang, M.; Anusavice, K.J. In vivo wear of enamel by a lithia disilicate-based core ceramic used for posterior fixed partial dentures: First-year results. Int. J. Prosthodont. 2006, 19, 391–396. [Google Scholar] [PubMed]
- Clarke, M.; Williamson, P.R. Core outcome sets and systematic reviews. Syst. Rev. 2016, 5, 11. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference | Randomization Process | Deviations from Intended Interventions | Mising Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall |
|---|---|---|---|---|---|---|
| Esquivel- Upshaw 2018 | Low | Low | Low | Someconcerns | Someconcerns | Some concerns |
| Mundhe 2015 | Some concerns | Low | Low | Some concerns | Some concerns | Some concerns |
| Yang 2014 | Some concerns | Low | Low | Some concerns | Some concerns | Some concerns |
| Bias due to / in… | ||||||||
|---|---|---|---|---|---|---|---|---|
| Confounding | Selection of Participants into the Study | Classification of Interventions | Deviations from Intended Interventions | Missing Data | Measurement of Outcomes | Selection of the Reported Result | Overall | |
| Stober 2014 | Moderate | No Information | Low | Low | Low | Moderate | Moderate | Moderate |
| # | Study ID | Outcome | Comparison | SMD (95% CIs) | p-value | Heterogeneity (I2 %) |
|---|---|---|---|---|---|---|
| In vitro | ||||||
| 1 | Two studies | Volume wear (mm3) | E- PZ | 1.06 (0.39, 1.73) | 0.002 | 0 |
| 2 | Two studies | Volume wear (mm3) | E- PGZ | –0.41 (–3.12, 2.30) | 0.77 | 92.7 |
| 3 | Two studies | Vertical wear (μm) | PZ- PGZ | 0.0 (–0.59, 0.59) | 0.99 | 0 |
| 4 | Two studies | Volume wear (mm3) | PZ- PGZ | –3.03 (–9.20, 3.14) | 0.34 | 95.4 |
| 5 | Two studies | Volume wear (mm3) | PZ- GZ | –2.85 (–6.86, 1.15) | 0.16 | 92.5 |
| 6 | Two studies | Volume wear (mm3) | MZ- LD | –0.93 (–2.17, 0.32) | 0.14 | 67.7 |
| 7 | Two studies | Vertical wear (μm) | MZ- LD | –1.59 (–5.51, 2.33) | 0.43 | 92.1 |
| 8 | Two studies | Vertical wear (μm) | MZ- CR | 0.36 (–0.39, 1.11) | 0.34 | 0 |
| 9 | Two studies | Vertical wear (μm) | LD- CR | 1.84 (–1.97, 5.64) | 0.34 | 91.1 |
| 10 | Two studies | Vertical wear (mm) | CP- LFC | 1.45 (–0.72, 3.62) | 0.19 | 87.9 |
| 11 | Two studies | Vertical wear (mm) | CP-MC | 2.18 (1.34, 3.02) | <0.001 | 8.4 |
| 12 | Two studies | Vertical wear (mm) | LFC- MC | 0.34 (–1.7, 2.41) | 0.75 | 89.5 |
| Clinical | ||||||
| Study ID | Outcome | Comparison | WMD (95% CIs) | p-value | Heterogeneity (I2 %) | |
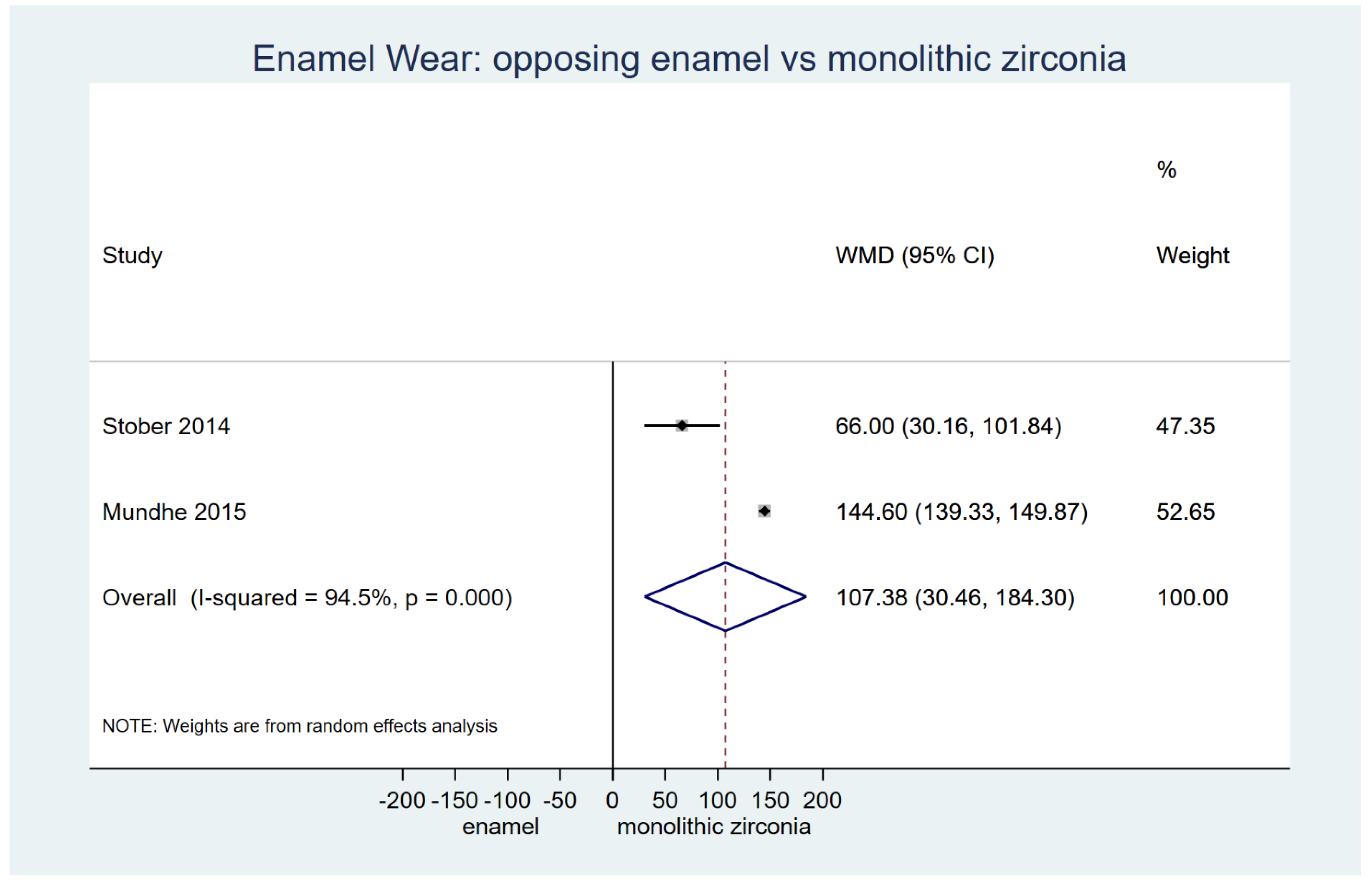
| 13 | Two studies | Vertical wear (μm) | MZ- E | 107.38 (30.46, 184.30) | 0.01 | 94.5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koletsi, D.; Iliadi, A.; Eliades, T.; Eliades, G. In Vitro Simulation and In Vivo Assessment of Tooth Wear: A Meta-Analysis of In Vitro and Clinical Research. Materials 2019, 12, 3575. https://doi.org/10.3390/ma12213575
Koletsi D, Iliadi A, Eliades T, Eliades G. In Vitro Simulation and In Vivo Assessment of Tooth Wear: A Meta-Analysis of In Vitro and Clinical Research. Materials. 2019; 12(21):3575. https://doi.org/10.3390/ma12213575
Chicago/Turabian StyleKoletsi, Despina, Anna Iliadi, Theodore Eliades, and George Eliades. 2019. "In Vitro Simulation and In Vivo Assessment of Tooth Wear: A Meta-Analysis of In Vitro and Clinical Research" Materials 12, no. 21: 3575. https://doi.org/10.3390/ma12213575
APA StyleKoletsi, D., Iliadi, A., Eliades, T., & Eliades, G. (2019). In Vitro Simulation and In Vivo Assessment of Tooth Wear: A Meta-Analysis of In Vitro and Clinical Research. Materials, 12(21), 3575. https://doi.org/10.3390/ma12213575