A Comparative Study of Shock Absorption Capacities of Custom Fabricated Mouthguards Using a Triangulation Sensor

Abstract
:1. Introduction
- To manufacture five types of mouthguards with different designs from ethylene vinyl acetate (EVA), where two of them are single-layered and differ in thickness, the other three are laminated and have inserts in the frontal region (a hard insert, an air space and a nylon mesh insert);
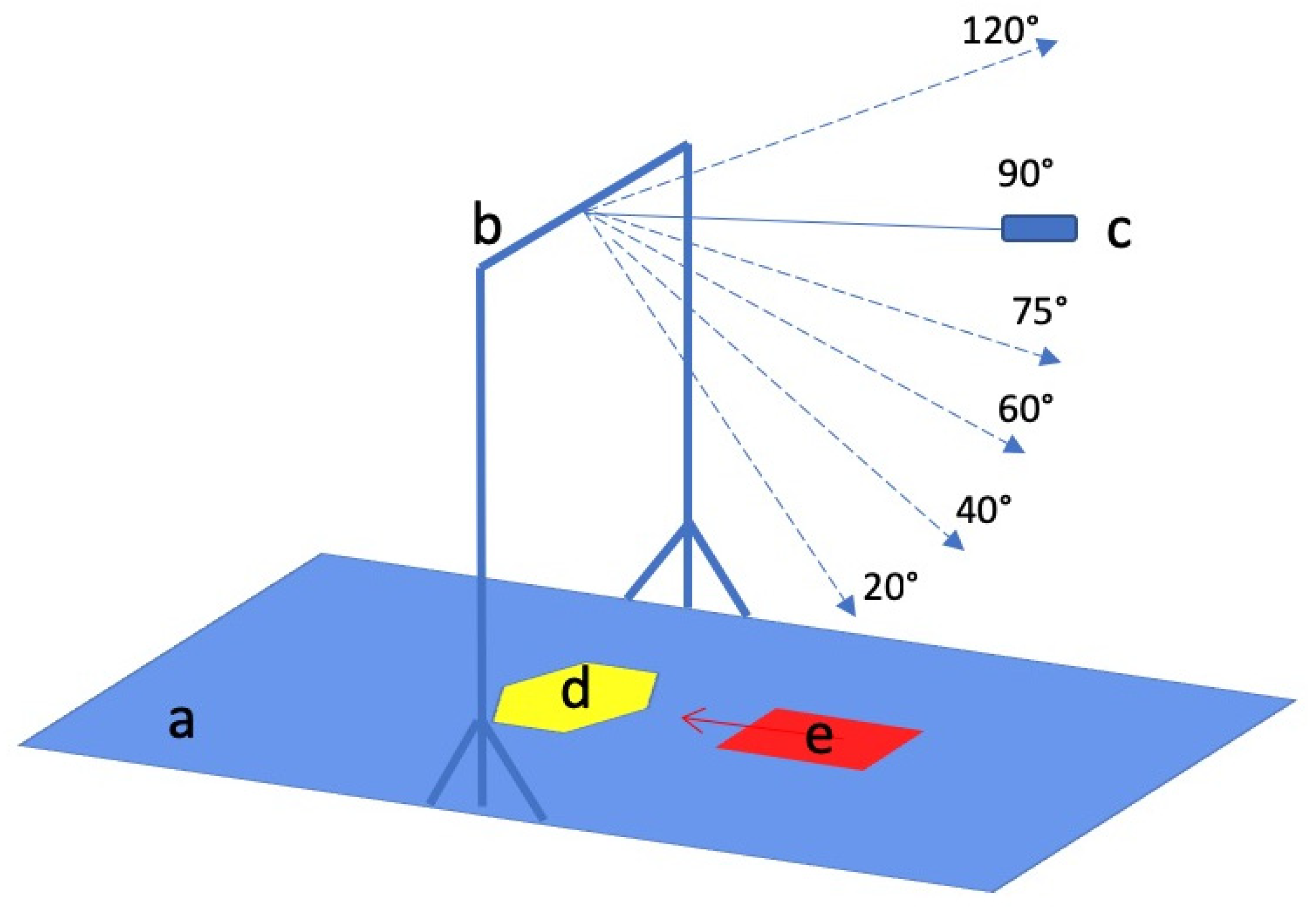
- to inflict different energy blows with a pendulum device on a pivoted tooth in an upper cast stainless steel model with and without a mouthguard;
- to ascertain the dental deflections with a triangulation laser sensor and to assess the preventive qualities of the different mouthguard designs.
2. Materials and Methods
2.1. Design of the Experiment
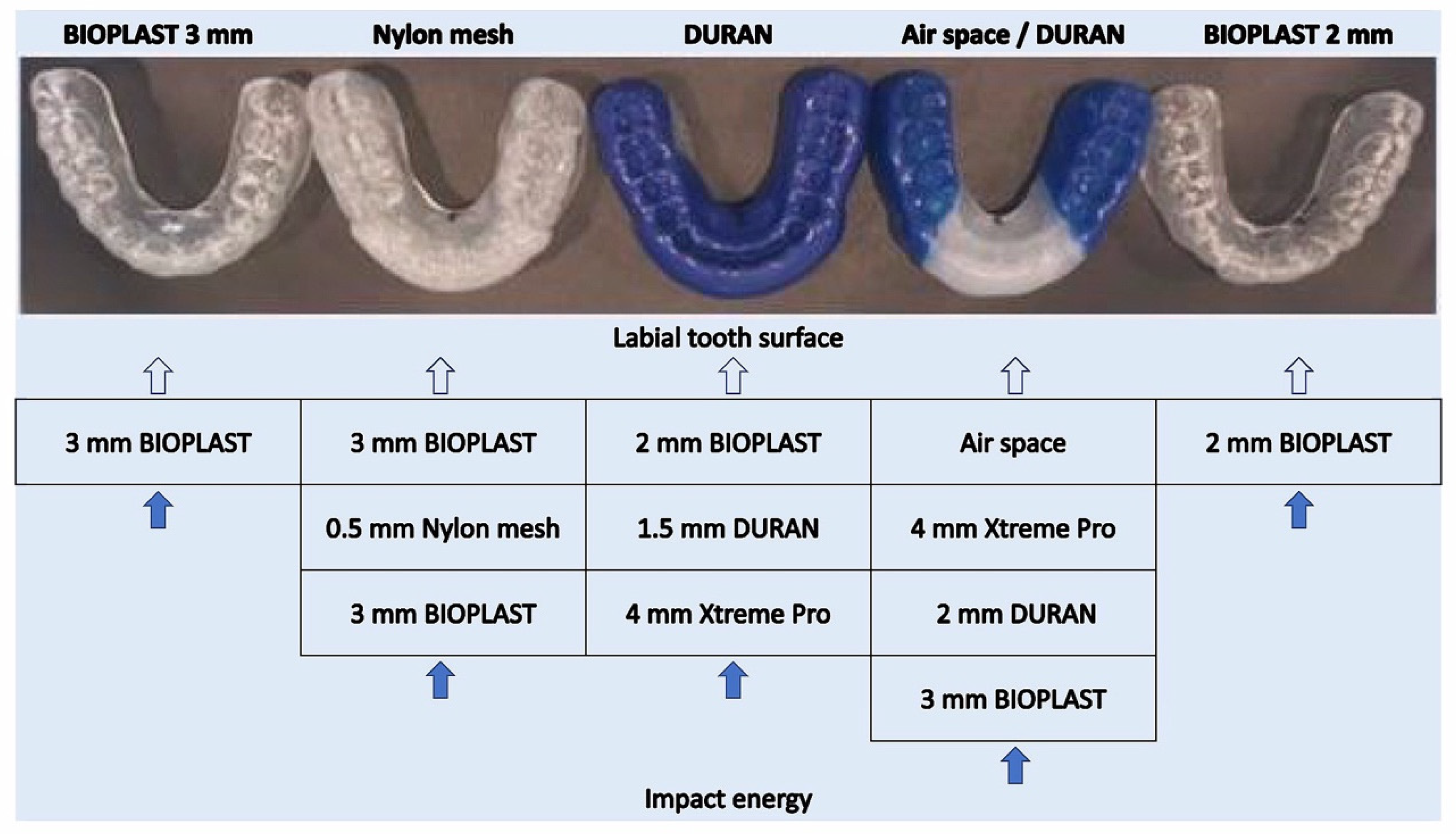
2.2. Mouthguard Production
- BIOPLAST 2 mm mouthguard (single-layer EVA mouthguard produced from Bioplast transparent 2 mm foil: Shore hardness A 85, Young’s modulus = 15 MPa, Item-No.: 3185, SCHEU-DENTAL GmbH, Iserlohn, Germany)
- BIOPLAST 3 mm mouthguard (single-layer EVA mouthguard produced from Bioplast transparent 3 mm foil: Shore hardness A 85, Young’s modulus = 15 MPa, Item-No.: 3187, SCHEU-DENTAL GmbH, Iserlohn, Germany)
- Air space/DURAN mouthguard (multi-layered EVA mouthguard produced from XTREME PRO 4 mm foil (BIOPLAST-XTREME PRO 4 mm: EVA, frontal segment (clear-transparent): Shore hardness A 92, tensile strength 20 MPa, Young’s modulus = 25 MPa; lateral segment (blue): Shore hardness A 85, tensile strength 18 MPa, Young’s modulus = 13 MPa, Item-No.: 3296, SCHEU-DENTAL GmbH, Iserlohn, Germany); and a layer of a BIOPLAST transparent 3 mm foil (EVA, Shore hardness A 85, Young’s modulus = 15 MPa, item-No.: 3354, SCHEU-DENTAL GmbH, Iserlohn, Germany) with an air space and a hard insert as a labial reinforcement (DURAN 2 mm foil (Polyethylenterephthalat-Glycol Copolyester (PET-G), Shore hardness D 78, Young’s modulus = 2200 MPa, Item-No.: 3436, SCHEU-DENTAL GmbH, Iserlohn, Germany)
- NYLON MESH mouthguard (multi-layered EVA mouthguard produced from two BIOPLAST 3 mm (transparent) layers (BIOPLAST transparent 3 mm: EVA, Shore hardness A 85, Young’s modulus = 15 MPa, Item-No.: 3187, SCHEU-DENTAL GmbH, Iserlohn, Germany) and a Nylon mesh (0.5 mm) as a labial reinforcement (Nylon mesh 0.5 mm: Nylon mesh insert 0.5 mm (between the two layers of Bioplast, REF 3224.1, SCHEU-DENTAL GmbH, Iserlohn, Germany))
- DURAN mouthguard (multi-layered EVA mouthguard produced from BIOPLAST 2 mm (blue) layer (BIOPLAST blue 2 mm: EVA Shore hardness A 85, Young’s modulus = 15 MPa, Item-No.: 3185, SCHEU-DENTAL GmbH, Iserlohn, Germany) and an XTREME PRO 4 mm (blue/transparent/blue) foil layer (BIOPLAST-XTREME PRO 4 mm: EVA, frontal segment (clear-transparent): Shore hardness A 92, tensile strength 20 MPa, Young’s modulus = 25 MPa; lateral segment (blue): Shore hardness A 85, tensile strength 18 MPa, Young’s modulus = 13 MPa, Item-No.: 3296, SCHEU-DENTAL GmbH, Iserlohn, Germany) with a hard labial reinforcement produced from DURAN 1.5 mm foil (DURAN 1.5 mm: Polyethylenterephthalat-Glycol Copolyester (PET-G), Shore hardness D 78, Young’s modulus = 2200 MPa, Item-No.: 3434, SCHEU-DENTAL GmbH, Iserlohn, Germany)
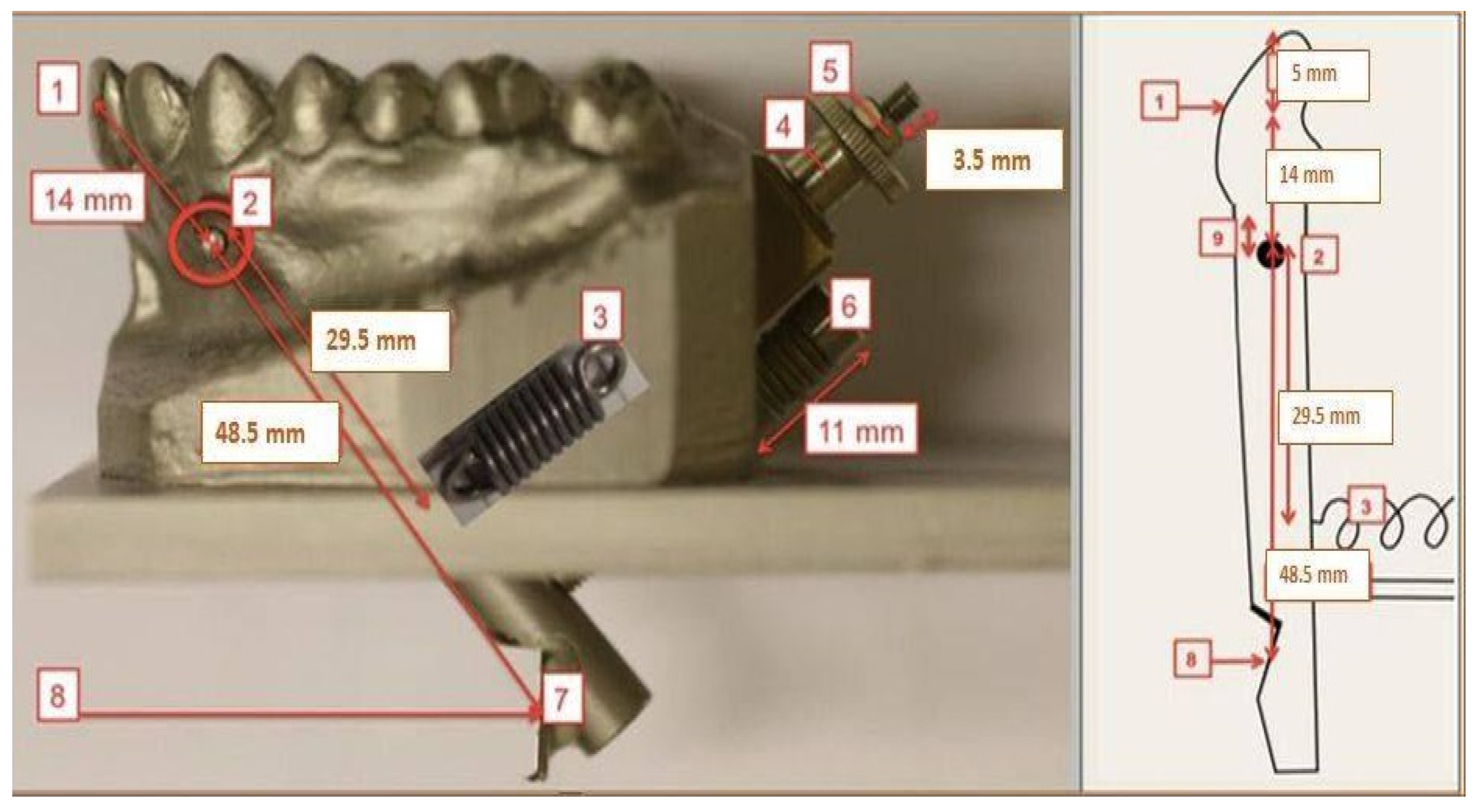
2.3. Pendulum Testing Device Construction, Triangulation Sensor Installment
2.4. Measurement Execution
2.5. Data Evaluation and Statistics
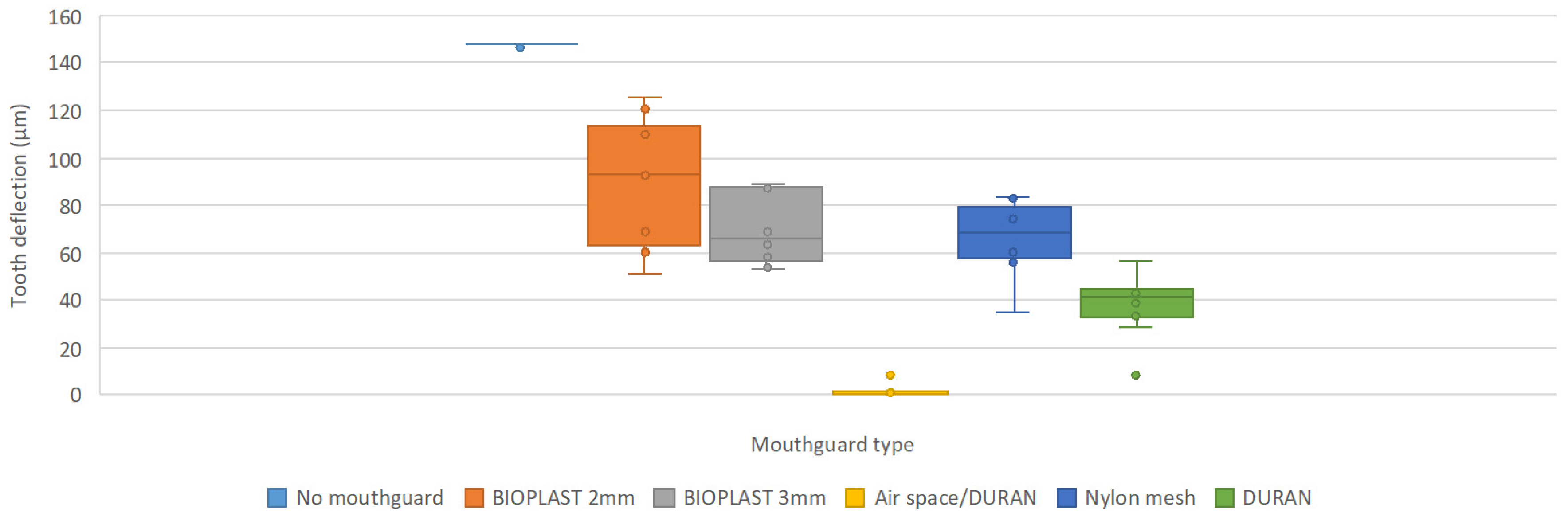
3. Results
4. Discussion

- It is an in-vitro study;
- Only one tooth was tested;
- No gingiva (intraorally there is flexibility of the surface of the gums).
5. Conclusions
- All manufactured mouthguards had preventive qualities as tooth deflection was significantly decreased with all tested mouthguards in comparison to impacts without mouthguard.
- BIOPLAST 2 mm and BIOPLAST 3 mm mouthguards revealed poor shock absorption capacities, their performance was not sufficient for dental trauma prevention: the deflection of the pivoted tooth was big even with low energy blows.
- Increasing mouthguard labial thickness by approximately 1 mm (50%; BIOPLAST 2 mm vs BIOPLAST 3 mm) improves protection towards small hard object collisions with low impact energies (<1.72 J).
- Combining different materials and using labial inserts improves mouthguard shock absorption capacities. Hard inserts for mouthguards (DURAN) serve better than soft inserts (Nylon mesh).
- Air space in the front region of the mouthguard significantly improves mouthguard shock absorption capacities in comparison to any other tested protective mouthguard design. It improved shock absorption by up to 95% in comparison with the DURAN mouthguard at 90° pendulum hits.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Horri, A.; Shojaeepoor, R.; Jahanimoghadam, F.; Bahador, A.; Pouradeli, S. Effect of mouthguard on sport-related orofacial injuries in adolescents in kerman, Iran. IJBR 2016, 7, 2228–2234. [Google Scholar]
- Badel, T.; Jerolimov, V.; Pandurić, J.; Carek, V. Custom-made mouthguards and prevention of orofacial injuries in sports (croatian). Acta Med. Croat. 2007, 6, 9–14. [Google Scholar]
- Newsome, P.R.H.; Tran, D.C.; Cooke, M.S. The role of the mouthguard in the prevention of sports-related dental injuries: A review. Int. J. Paediatr. Dent. 2001, 11, 396–404. [Google Scholar] [CrossRef] [PubMed]
- ADA Council on Access, Prevention and Interprofessional Relations; ADA Council on Scientific Affairs. Using mouthguards to reduce the incidence and severity of sports-related oral injuries. J. Am. Dent. Assoc. 2006, 137, 1712–1720. [Google Scholar] [CrossRef] [PubMed]
- Gould, T.E.; Piland, S.G.; Caswell, S.V.; Ranalli, D.; Mills, S.; Ferrara, M.; Courson, R. National athletic trainers‘ association position statement: Preventing and managing sport-related dental and oral injuries. J. Athl. Train 2016, 51, 821–839. [Google Scholar] [CrossRef]
- Rodd, H.; Noble, F. Psychosocial impacts relating to dental injuries in childhood: The bigger picture. Dent. J. 2019, 7, 23. [Google Scholar] [CrossRef]
- Clark, D.; Levin, L. Prognosis and complications of immature teeth following lateral luxation: A systematic review. Dent. Traumatol. 2018, 34, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Bochnig, M.S.; Oh, M.J.; Nagel, T.; Ziegler, F.; Jost-Brinkmann, P.G. Comparison of the shock absorption capacities of different mouthguards. Dent. Traumatol. 2017, 33, 205–213. [Google Scholar] [CrossRef]
- Sarac, R. A Comparative Study of Shock Absorption Capacities of Custom Fabricated Mouthguards Using a Triangulation Sensor. Master’s Thesis, Universitätsmedizin der Universität Greifswald, Greifswald, Germany, 21 Febuary 2019. [Google Scholar]
- Bochnig, M.S. Vergleich der Schlagdämpfung Verschiedener Sportmundschutze. Eine In-Vitro-Studie Mittels Laservibrometer und Beschleunigungssensoren (German). Ph.D. Thesis, Charité–Universitätsmedizin Berlin, Berlin, Germany, 25 June 2017. [Google Scholar]
- Kumar, S.; Nirmal, R. Mouthguards and its importance in prevention of sports related orofacial injuries: A review. IJPEJB 2015, 1, 18–19. [Google Scholar]
- Emshoff, R.; Schöning, H.; Röthler, G.; Waldhart, E. Trends in the incidence and cause of sport-related mandibular fractures: A retrospective analysis. J. Oral Maxillofac. Surg. 1997, 55, 585–592. [Google Scholar] [CrossRef]
- Flanders, R.; Bhat, M. The incidence of orofacial injuries in sports: A pilot study in illinois. J. Am. Dent. Assoc. 1995, 126, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Levin, L.; Friedlander, L.D.; Geiger, S.B. Dental and oral trauma and mouthguard use during sport activities in Israel. Dent. Traumatol. 2003, 19, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Pawar, P.G.; Suryawanshi, M.M.; Patil, A.K.; Purnale, P.S.; Ali, F.M. Importance of mouth guards in sports: A review. JEMDS 2013, 2, 8903–8908. [Google Scholar] [CrossRef]
- De Wet, F.A.; Heyns, M.; Pretorius, J.J. Shock absorption potential of different mouth guard materials. Prosthet. Dent. 1999, 82, 301–306. [Google Scholar] [CrossRef]
- McCrory, P. Do mouthguards prevent concussion? Br. J. Sports Med. 2001, 35, 81–82. [Google Scholar] [CrossRef] [Green Version]
- Wisniewski, J.; Guskiewicz, K.; Trope, M.; Sigurdsson, A. Incidence of cerebral concussions associated with type of mouthguard used in college football. Dent. Traumatol. 2004, 20, 143–149. [Google Scholar] [CrossRef]
- Yamada, T.; Sawaki, Y.; Tomida, S.; Tohnai, I.; Ueda, M. Oral injury and mouthguard usage by athletes in Japan. Dent. Traumatol. 1998, 14, 84–87. [Google Scholar] [CrossRef]
- Seshadri, D.R.; Li, R.T.; Voos, J.E.; Rowbottom, J.R.; Alfes, C.M.; Zorman, C.A.; Drummond, C.K. Wearable sensors for monitoring the internal and external workload of the athlete. NPJ Digit. Med. 2019, 2, 71. [Google Scholar] [CrossRef]
- Verissimo, C.; Costa, P.V.; Santos-Filho, P.C.; Tantbirojn, D.; Versluis, A.; Soares, C.J. Custom-fitted EVA mouthguards: What is the ideal thickness? A dynamic finite element impact study. Dent. Traumatol. 2016, 32, 95–102. [Google Scholar] [CrossRef]
- Bridgman, H.; Kwong, M.T.; Bergmann, J.H.M. Mechanical safety of embedded electronics for in-body wearables: A smart mouthguard study. Ann. Biomed. Eng. 2019, 47, 1725–1737. [Google Scholar] [CrossRef]
- McGlumphy, K.C.; Mendel, D.A.; Yilmaz, B.; Seidt, J.D. Pilot study of 3D image correlation photogrammetry to assess strain and deform. of mouthguard materials. Dent. Traumatol. 2014, 30, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Bemelmanns, P.; Pfeiffer, P. Häufigkeit von Zahn-, Mund- und Kieferverletzungen und Bewährung von Mundschutzen bei Spitzensportlern (German). Sportverletz. Sportschaden. 2000, 14, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Queiróz, A.F.; de Brito, R.B., Jr.; Ramacciato, J.C.; Motta, R.H.; Flório, F.M. Influence of mouthguards on the physical performance of soccer players. Dent. Traumatol. 2013, 29, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Westerman, B.; Stringfellow, P.M.; Eccleston, J.A. An improved mouthguard material. Aust. Dent. J. 1997, 42, 189–191. [Google Scholar] [CrossRef] [PubMed]
- Gould, T.; Piland, S.; Shin, J.; Hoyle, C.; Nazarenko, S. Characterization of mouthguard materials: Physical and mechanical properties of commercialized products. Dent. Mater. 2009, 25, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Westerman, B.; Stringfellow, P.M.; Eccleston, J.A. EVA mouthguards: How thick should they be? Dent. Traumatol. 2002, 18, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Westerman, B.; Stringfellow, P.M.; Eccleston, J.A. Beneficial effects of air inclusions on the performance of ethylene vinyl acetate (EVA) mouthguard material. Br. J. Sports Med. 2002, 36, 51–53. [Google Scholar] [CrossRef] [Green Version]
- Westerman, B.; Stringfellow, P.M.; Eccleston, J.A. The effect on energy absorption of hard inserts in laminated EVA mouthguards. Aust. Dent. J. 2000, 45, 21–23. [Google Scholar] [CrossRef] [Green Version]
- Takeda, T.; Ishigami, K.; Handa, J.; Naitoh, K.; Kurokawa, K.; Shibusawa, M. Does hard insertion and space improve shock absorption ability of mouthguard? Dent. Traumatol. 2006, 22, 77–82. [Google Scholar] [CrossRef]
- Verissimo, C.; Costa, P.; Santos-Filho, P.; Fernandes-Neto, A.; Tantbirojn, D.; Versluis, A. Evaluation of a dentoalveolar model for testing mouthguards: Stress and strain analyses. Dent. Traumatol. 2015, 32, 4–13. [Google Scholar] [CrossRef]
- Cummins, N.; Spears, I. The effect of mouthguard design on stresses in the tooth-bone complex. Med. Sci. Sports Exerc. 2002, 34, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Park, J.B.; Shaull, K.L.; Overton, B.; Donly, K.J. Improving mouth guards. J. Prosthet. Dent. 1994, 72, 373–380. [Google Scholar] [CrossRef]
- Lloyd, J.D.; Nakamura, W.S.; Maeda, Y.; Takeda, T.; Leesungbok, R.; Lazarchik, D.; Dorney, B.; Gonda, T.; Nakajima, K.; Yasui, T.; et al. Mouthguards and their use in sports: Report of the 1st international sports dentistry workshop, 2016. Dent. Traumatol. 2017, 33, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Westerman, B.; Stringfellow, P.M.; Eccleston, J.A. Forces transmitted through EVA mouthguard materials of different types and thickness. Aust. Dent. J. 1996, 40, 389–391. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pendulum Elongation Angle | Pivoted Tooth Deflection (µm) During the Pendulum Strikes | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 20° | 4.7 | 4.3 | 6.5 | 5.9 | 4.8 | 6.4 | 4.3 | 4.4 | 4.9 | 6.5 |
| 40° | 53.9 | 53.9 | 45.6 | 52.3 | 50.6 | 55.8 | 44.1 | 49.7 | 45.9 | 54.6 |
| 60° | 85.2 | 84.3 | 81.6 | 65.8 | 68.8 | 69.8 | 74.6 | 73.0 | 78.6 | 83.5 |
| 75° | 145.2 | 142.6 | 146.7 | 144.3 | 146.0 | 144.1 | 142.1 | 143.7 | 138.9 | 141.7 |
| 90° | 147.9 | 146.9 | 147.9 | 147.9 | 147.9 | 147.9 | 147.9 | 147.9 | 147.9 | 148.0 |
| Pendulum Elongation Angle | Pivoted Tooth Deflection (µm) During the Pendulum Strikes of 10 Mouthguard Samples (n = 10) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 20° | 2.0 | 1.8 | 2.0 | 1.5 | 1.9 | 1.6 | 1.6 | 1.9 | 1.7 | 2.1 |
| 40° | 12.8 | 20.2 | 14.8 | 12.4 | 14.9 | 10.1 | 11.1 | 8.9 | 8.3 | 12.4 |
| 60° | 40.9 | 30.5 | 22.7 | 31.7 | 33.3 | 23.8 | 35.3 | 38.1 | 40.7 | 37.6 |
| 75° | 123.4 | 127.2 | 124.2 | 127.5 | 127.0 | 124.8 | 123.5 | 126.0 | 128.0 | 127.5 |
| 90° | 68.6 | 60.5 | 63.6 | 52.2 | 51.0 | 92.4 | 93.9 | 125.2 | 120.9 | 109.6 |
| Pendulum Elongation Angle | Pivoted Tooth Deflection (µm) During Pendulum Strikes of 10 Mouthguard Samples (n = 10) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 20° | 1.2 | 1.7 | 1.8 | 1.6 | 1.8 | 1.5 | 1.8 | 1.1 | 1.9 | 1.6 |
| 40° | 2.7 | 2.1 | 2.3 | 2.4 | 2.1 | 2.1 | 2.1 | 2.1 | 2.3 | 2.1 |
| 60° | 31.4 | 11.4 | 12.5 | 10.6 | 11.6 | 10.3 | 12.1 | 11.8 | 9.0 | 11.9 |
| 75° | 116.3 | 103.2 | 114.5 | 115.6 | 114.4 | 119.1 | 114.1 | 117.7 | 117.3 | 116.8 |
| 90° | 57.7 | 53.7 | 60.3 | 63.1 | 53.2 | 68.6 | 87.8 | 89.0 | 71.5 | 86.9 |
| Pendulum Elongation Angle | Pivoted Tooth Deflection (µm) During Pendulum Strikes of 10 Mouthguard Samples (n = 10) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 20° | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 |
| 40° | 0.4 | 0.3 | 0.4 | 0.3 | 0.3 | 0.4 | 0.3 | 0.3 | 0.3 | 0.3 |
| 60° | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.4 | 0.4 | 0.4 |
| 75° | 0.6 | 0.6 | 1.1 | 0.8 | 0.7 | 0.7 | 0.6 | 0.5 | 0.4 | 0.5 |
| 90° | 0.9 | 0.8 | 0.7 | 0.9 | 0.8 | 8.0 | 0.7 | 1.2 | 0.5 | 0.7 |
| 120° | 6.2 | 2.1 | 1.8 | 1.9 | 2.2 | 2.0 | 1.1 | 2.5 | 0.7 | 0.8 |
| Pendulum Elongation Angle | Pivoted Tooth Deflection (µm) During Pendulum Strikes of 10 Mouthguard Samples (n = 10) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 20° | 0.9 | 1.2 | 0.8 | 0.5 | 1.1 | 1.3 | 1.1 | 0.4 | 1.1 | 0.3 |
| 40° | 1.6 | 1.7 | 1.0 | 0.4 | 1.3 | 0.9 | 1.0 | 0.5 | 1.1 | 0.5 |
| 60° | 28.9 | 29.6 | 5.4 | 17.2 | 22.8 | 21.5 | 23.2 | 1.0 | 24.9 | 4.3 |
| 75° | 44.8 | 69.7 | 52.7 | 56.1 | 60.1 | 63.8 | 50.1 | 11.5 | 69.5 | 40.6 |
| 90° | 58.3 | 82.6 | 55.8 | 74.8 | 63.0 | 74.3 | 77.3 | 36.1 | 83.0 | 60.0 |
| Pendulum Elongation Angle | Pivoted Tooth Deflection (µm) During Pendulum Strikes of 10 Mouthguard Samples (n = 10) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 20° | 0.6 | 1.0 | 0.5 | 0.5 | 0.9 | 0.7 | 0.6 | 0.5 | 0.5 | 1.0 |
| 40° | 1.0 | 0.6 | 0.7 | 1.1 | 0.9 | 2.7 | 1.2 | 1.1 | 1.1 | 0.9 |
| 60° | 4.9 | 12.8 | 0.9 | 13.1 | 5.3 | 22.2 | 9.6 | 8.4 | 7.7 | 5.9 |
| 75° | 19.5 | 31.1 | 2.2 | 36.9 | 33.3 | 50.1 | 36.8 | 37.4 | 32.6 | 35.2 |
| 90° | 33.3 | 42.6 | 8.0 | 45.0 | 42.6 | 56.1 | 43.5 | 28.2 | 40.4 | 38.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarac, R.; Helbig, J.; Dräger, J.; Jost-Brinkmann, P.-G. A Comparative Study of Shock Absorption Capacities of Custom Fabricated Mouthguards Using a Triangulation Sensor. Materials 2019, 12, 3535. https://doi.org/10.3390/ma12213535
Sarac R, Helbig J, Dräger J, Jost-Brinkmann P-G. A Comparative Study of Shock Absorption Capacities of Custom Fabricated Mouthguards Using a Triangulation Sensor. Materials. 2019; 12(21):3535. https://doi.org/10.3390/ma12213535
Chicago/Turabian StyleSarac, Rūta, Julia Helbig, Juliane Dräger, and Paul-Georg Jost-Brinkmann. 2019. "A Comparative Study of Shock Absorption Capacities of Custom Fabricated Mouthguards Using a Triangulation Sensor" Materials 12, no. 21: 3535. https://doi.org/10.3390/ma12213535
APA StyleSarac, R., Helbig, J., Dräger, J., & Jost-Brinkmann, P. -G. (2019). A Comparative Study of Shock Absorption Capacities of Custom Fabricated Mouthguards Using a Triangulation Sensor. Materials, 12(21), 3535. https://doi.org/10.3390/ma12213535