Materials for Hip Prostheses: A Review of Wear and Loading Considerations



Abstract
:1. Introduction
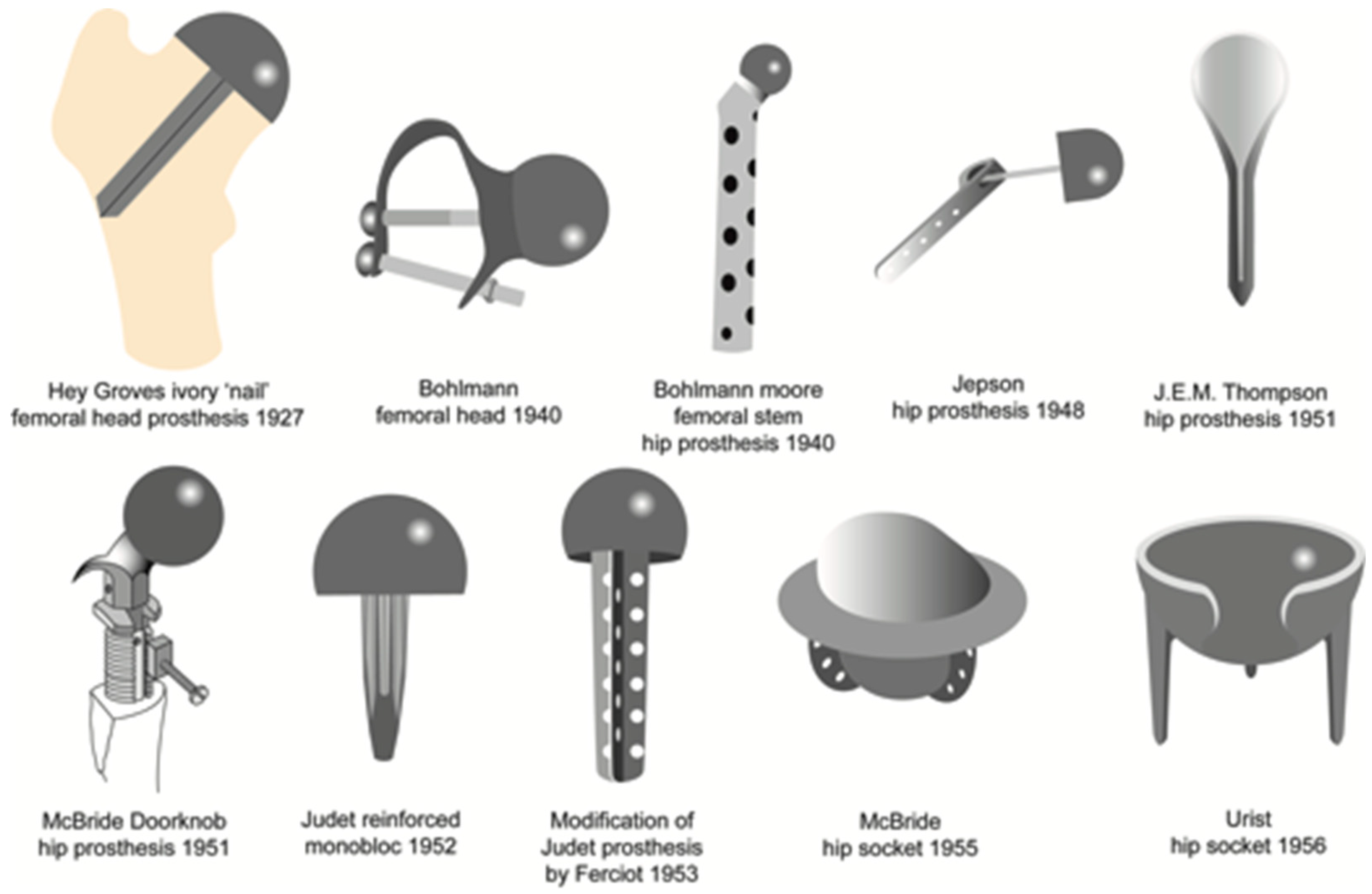
1.1. History
1.2. Current Materials
2. Polymers
2.1. PTFE
2.2. UHMWPE
2.3. PEEK
3. Metals
3.1. Cobalt Chromium Molybdenum Alloys
3.2. Other Metal Alloys
4. Ceramics
4.1. Alumina
4.2. Zirconia
4.3. Zirconia Toughened Alumina
5. Wear Behavior
5.1. Wear of Polyethylene
5.2. Wear of Metals
5.3. Wear of Ceramics
6. Discussion
7. Conclusions and Future Prospects
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| Alumina toughened | ATZ |
| Ceramic-on-ceramic | CoC |
| Ceramic-on-metal from | CoMplete |
| Cross-linked | XLPE |
| Metal-on-metal | MoM |
| Metal-on-polyethylene | MoP |
| Polytetrafluoroethylene | PTFE |
| Polyetheretherketone | PEEK |
| Total hip arthroplasty | THA |
| Ultra-high molecular weight polyethylene | UHMWPE |
| Zirconia toughened alumina | ZTA |
References
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef]
- Aherwar, A.; Singh, A.K.; Patnaik, A. Current and future biocompatibility aspects of biomaterials for hip prosthesis. AIMS Bioeng. 2015, 3, 23–43. [Google Scholar] [CrossRef]
- Affatato, S. Perspectives in Total Hip Arthroplasty: Advances in Biomaterials and Their Tribological Interactions; Affatato, S., Ed.; Elsevier Science: Amsterdam, The Netherlands, 2014; ISBN 1782420398. [Google Scholar]
- Gomez, P.; Morcuende, J.A. Early attempts at hip arthroplasty-1700s to 1950s. Iowa Orthop J. 2005, 25, 25–29. [Google Scholar] [PubMed]
- Pramanik, S.; Agarwal, A.K.; Rai, K.N. Chronology of Total Hip Joint Replacement and Materials Development. Trends Biomater. Artif. Organs 2005, 19, 15–26. [Google Scholar]
- Knight, S.R.; Aujla, R.; Biswas, S.P. Total Hip Arthroplasty - over 100 years of operative history. Orthop. Rev. (Pavia) 2011, 3. [Google Scholar] [CrossRef] [PubMed]
- Muster, D. Themistocles Gluck, Berlin 1890: A pioneer of multidisciplinary applied research into biomaterials for endoprostheses. Bull. Hist. Dent. 1990, 38, 3–6. [Google Scholar] [PubMed]
- Hernigou, P. Smith-Petersen and early development of hip arthroplasty. Int. Orthop. 2014, 38, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Zivic, F.; Affatato, S.; Trajanovic, M.; Schnabelrauch, M.; Grujovic, N. Biomaterials in Clinical Practice: Advances in Clinical Research and Medical Devices; Springer: Berlin, Germany, 2018; ISBN 3319680250. [Google Scholar]
- McKee, G.K. Total hip replacement - past, present and future. Biomaterials 1982, 3, 130–135. [Google Scholar] [CrossRef]
- Affatato, S.; Spinelli, M.; Squarzoni, S.; Traina, F.; Toni, A. Mixing and matching in ceramic-on-metal hip arthroplasty: an in-vitro hip simulator study. J. Biomech. 2009, 42, 2439–2446. [Google Scholar] [CrossRef]
- Fisher, J.; Firkins, P.J.; Tipper, J.L.; Ingham, E.; Stone, M.H.; Farrar, R. In-vitro wear performance of contemporary alumina: Alumina bearing couple under anatomically-relevant hip joint simulation. In Reliability and Long Term Results of Ceramics in Orthopedics; Toni, A., Willmann, G., Eds.; Thieme Verlag: Stuttgart, Germany, 2001; pp. 1291–1298. [Google Scholar]
- Triclot, P. Metal-on-metal: History, state of the art (2010). Int. Orthop. 2011, 2, 201–206. [Google Scholar] [CrossRef]
- Kumar, N.; Arora, G.N.C.; Datta, B. Bearing surfaces in hip replacement - Evolution and likely future. Med. J. Armed Forces India 2014, 70, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Molli, R.G.; Lombardi, A.V.; Berend, K.R.; Adams, J.B.; Sneller, M.A. Metal-on-metal vs Metal-on-improved polyethylene bearings in total hip arthroplasty. J. Arthroplast. 2011, 6, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Topolovec, M.; Cör, A.; Milošev, I. Metal-on-metal vs. metal-on-polyethylene total hip arthroplasty tribological evaluation of retrieved components and periprosthetic tissue. J. Mech. Behav. Biomed. Mater. 2014, 34, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.C.T.; Tatman, P.; Mehle, S.; Gioe, T.J. Cumulative revision rate is higher in metal-on-metal THA than metal-on-polyethylene THA: Analysis of survival in a community registry. Clin. Orthop. Relat. Res. 2013, 471, 1920–1925. [Google Scholar] [CrossRef] [PubMed]
- National Joint Registry for England, Wales and Northern Ireland. 11th Annual Report 2014. 2014. Available online: http://www.njrcentre.org.uk/njrcentre/News-and-Events/NJR-11th-Annual-Report (accessed on 1 February 2019).
- Fisher, J.; Hu, X.Q.; Stewart, T.D.; Williams, S.; Tipper, J.L.; Ingham, E.; Stone, M.H.; Davies, C.; Hatto, P.; Bolton, J.; Riley, M.; Hardaker, C.; Isaac, G.H.; Berry, G. Wear of surface engineered metal-on-metal hip prostheses. J. Mater. Sci. Mater. Med. 2004, 15, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Tie, K.; Yang, X.; Tan, Y.; Alaidaros, M.; Chen, L. Comparison of ceramic-on-ceramic to metal-on-polyethylene bearing surfaces in total hip arthroplasty: a meta-analysis of randomized controlled trials. J. Orthop. Surg. Res. 2015, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Bader, R.; Willmann, G. Ceramic cups for hip endoprostheses. 6: Cup design, inclination and antetorsion angle modify range of motion and impingement. Biomed. Tech. 1999, 44, 212–219. [Google Scholar]
- Henssge, E.J.; Bos, I.; Willman, G. Al2O3 against Al2O3 combination in hip endoprostheses. Histological investigations with semiquantitative grading of revision and autopsy cases and abrasion measures. J. Mater. Sci. Mater. Med. 1994, 5, 657–661. [Google Scholar] [CrossRef]
- Macchi, F.; Willman, G. Allumina Biolox forte: evoluzione, stato dell’arte e affidabilità. Lo Scalpello 2001, 15, 99–106. [Google Scholar]
- Morrison, J.C.; Ward, D.; Bierbaum, B.E.; Nairus, J.; Kuesis, D. Ceramic-on-ceramic bearings in total hip arthroplasty. Clin. Orthop. Relat. Res. 2002, 405, 158–163. [Google Scholar] [CrossRef]
- Barnes, C.L.; DeBoer, D.; Corpe, R.S.; Nambu, S.; Carroll, M.; Timmerman, I. Wear performance of large-diameter differential-hardness hip bearings. J. Arthroplast. 2008, 23, 56–60. [Google Scholar] [CrossRef]
- Sauvé, P.; Mountney, J.; Khan, T.; De Beer, J.; Higgins, B.; Grover, M. Metal ion levels after metal-on-metal Ring total hip replacement: a 30-year follow-up study. J. Bone Jt. Surg. Br. 2007, 89, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Toni, A.; Traina, F.; Stea, S.; Sudanese, A.; Visentin, M.; Bordini, B.; Squarzoni, S. Early diagnosis of ceramic liner fracture. Guidelines based on a twelve-year clinical experience. J. Bone Jt. Surg. Am. 2006, 88 (Suppl. 4), 55–63. [Google Scholar] [CrossRef]
- Affatato, S.; Spinelli, M.; Zavalloni, M.; Traina, F.; Carmignato, S.; Toni, A. Ceramic-on-metal for total hip replacement: mixing and matching can lead to high wear. Artif. Organs 2010, 34, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Orishimo, K.F.; Claus, A.M.; Sychterz, C.J.; Engh, C.A. Relationship between polyethylene wear and osteolysis in hips with a second-generation porous-coated cementless cup after seven years of follow-up. J. Bone Joint Surg. Am. 2003, 85-A, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Bozic, K.J.; Kurtz, S.M.; Lau, E.; Ong, K.; Vail, T.P.; Berry, D.J. The Epidemiology of Revision Total Hip Arthroplasty in the United States. J. Bone Jt. Surgery-American Vol. 2009, 91, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, S. Biomaterials: A Nano Approach; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- Stauffer, R.N. Ten-year follow-up study of total hip replacement. J. Bone Jt. Surg. Am. 1982, 64, 983–990. [Google Scholar] [CrossRef]
- Sinha, R.K. Hip Replacement: Current Trends and Controversies; Marcel Dekker: New York City, NY, USA, 2002. [Google Scholar]
- Maguire, J.K.; Coscia, M.F.; Lynch, M.H. Foreign Body Reaction to Polymeric Debris Following Total Hip Arthroplasty. Clin. Orthop. Relat. Res. 1987, 216, 213–223. [Google Scholar] [CrossRef]
- Charnley, J. Tissue reaction to the polytetrafluoroethylene. Lancet 1963, II, 1379. [Google Scholar] [CrossRef]
- Schreiber, A.; Huggler, A.H.; Dietschi, C.; Jacob, H. Complications After Joint Replacement — Longterm Follow-Up, Clinical Findings, and Biomechanical Research. In Engineering in Medicine; Springer: Berlin, Heidelberg, 1976; pp. 187–202. [Google Scholar]
- Wroblewski, B.M.; Fleming, P.A.; Siney, P.D. Charnley Low-Frictional Torque Arthroplasty of the Hip; Springer: Berlin, Germany, 1999; Volume 81. [Google Scholar]
- Sobieraj, M.C.; Rimnac, C.M. Ultra high molecular weight polyethylene: mechanics, morphology, and clinical behavior. J. Mech. Behav. Biomed. Mater. 2009, 2, 433–443. [Google Scholar] [CrossRef]
- ISO 11542-1:2001-Plastics—Ultra-High-Molecular-Weight Polyethylene (PE-UHMW) Moulding and Extrusion Materials—Part 1: Designation System and Basis for Specifications; International Organization for Standardization: Geneva, Switzerland, 2001.
- Harris, W.H. Wear and periprosthetic osteolysis: the problem. Clin. Orthop. Rel. Res. 2001, 393, 66–70. [Google Scholar] [CrossRef]
- Wroblewski, B.M.; Siney, P.D.; Dowson, D.; Collins, S.N. Prospective clinical and joint simulator studies of a new total hip arthroplasty using alumina ceramic heads and cross-linked polyethylene cups. J. Bone Jt. Surg. Br. 1996, 78, 280–285. [Google Scholar] [CrossRef] [PubMed]
- McKellop, H.; Shen, F.; Lu, B.; Campbell, P.; Salovey, R. Development of an extremely wear-resistant ultra high molecular weight polythylene for total hip replacements. J. Orthop. Res. 1999, 17, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Gul, R.M. Improved UHMWPE for Use in Total Joint Replacement; Dept. of Materials Science and Engineering, Massachusetts Institute of Technology: Cambridge, MA, USA, 1997. [Google Scholar]
- Shen, F.-W.; McKellop, H.A.; Salovey, R. Irradiation of chemically crosslinked ultrahigh molecular weight polyethylene. J. Polym. Sci. Part B Polym. Phys. 1996, 34, 1063–1077. [Google Scholar] [CrossRef]
- Muratoglu, O.K.; Bragdon, C.R. Highly Cross-Linked and Melted UHMWPE. In UHMWPE Biomaterials Handbook: Ultra High Molecular Weight Polyethylene in Total Joint Replacement and Medical Devices; Kurtz, S.M., Ed.; William Andrew: Norwich, NY, USA, 2015; ISBN 0323354351. [Google Scholar]
- Muratoglu, O.K.; Bragdon, C.R.; O’Connor, D.O.; Jasty, M.; Harris, W.H.; Gul, R.; McGarry, F. Unified wear model for highly crosslinked ultra-high molecular weight polyethylenes (UHMWPE). Biomaterials 1999, 20, 1463–1470. [Google Scholar] [CrossRef]
- Harris, W.H.; Muratoglu, O.K. A Review of Current Cross-linked Polyethylenes Used in Total Joint Arthroplasty. Clin. Orthop. Relat. Res. 2005, 430, 46–52. [Google Scholar] [CrossRef]
- Burnett, S.J.; Abos, D. Total hip arthroplasty: Techniques and results. BB Med. J. 2010, 52, 455–464. [Google Scholar]
- Oral, E.; Ghali, B.W.; Muratoglu, O.K. The elimination of free radicals in irradiated UHMWPEs with and without vitamin e stabilization by annealing under pressure. J. Biomed. Mater. Res. Part B Appl. Biomater. 2011, 97 B, 167–174. [Google Scholar] [CrossRef]
- Puppulin, L.; Miura, Y.; Casagrande, E.; Hasegawa, M.; Marunaka, Y.; Tone, S.; Sudo, A.; Pezzotti, G. Validation of a protocol based on Raman and infrared spectroscopies to nondestructively estimate the oxidative degradation of UHMWPE used in total joint arthroplasty. Acta Biomater. 2016, 38, 168–178. [Google Scholar] [CrossRef]
- Muratoglu, O.K.; Wannomae, K.K.; Rowell, S.L.; Micheli, B.R.; Malchau, H. Ex Vivo Stability Loss of Irradiated and Melted Ultra-High Molecular Weight Polyethylene. JBJS 2010, 92, 2809–2816. [Google Scholar] [CrossRef]
- Reinitz, S.D.; Currier, B.H.; Levine, R.A.; Van Citters, D.W. Crosslink density, oxidation and chain scission in retrieved, highly cross-linked UHMWPE tibial bearings. Biomaterials 2014, 35, 4436–4440. [Google Scholar] [CrossRef] [PubMed]
- Currier, B.H.; Currier, J.H.; Mayor, M.B.; Lyford, K.A.; Van Citters, D.W.; Collier, J.P. In Vivo Oxidation of γ-Barrier–Sterilized Ultra–High-Molecular-Weight Polyethylene Bearings. J. Arthroplast. 2007, 22, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-H.; Park, J.-W.; Kim, J.-S. Alumina Delta-on-Highly Crosslinked-Remelted Polyethylene Bearing in Cementless Total Hip Arthroplasty in Patients Younger than 50 Years. J. Arthroplast. 2016, 31, 2800–2804. [Google Scholar] [CrossRef] [PubMed]
- Takada, R.; Jinno, T.; Koga, D.; Miyatake, K.; Muneta, T.; Okawa, A. Comparison of wear rate and osteolysis between second-generation annealed and first-generation remelted highly cross-linked polyethylene in total hip arthroplasty. A case control study at a minimum of five years. Orthop. Traumatol. Surg. Res. 2017, 103, 537–541. [Google Scholar] [CrossRef] [PubMed]
- D’Antonio, J.A.; Capello, W.N.; Ramakrishnan, R. Second-generation annealed highly cross-linked polyethylene exhibits low wear. Clin. Orthop. Relat. Res. 2012, 470, 1696–1704. [Google Scholar] [CrossRef] [PubMed]
- Bhateja, S.K. Radiation-induced crystallinity changes in linear polyethylene: Influence of aging. J. Appl. Polym. Sci. 1983, 28, 861–872. [Google Scholar] [CrossRef]
- Muratoglu, O.K.; Bragdon, C.R.; O’Connor, D.O.; Skehan, H.; Delany, J.; Jasty, M.; Harris, W.H. The Effect Of Temperature On Radiation Crosslinking Of Uhmwpe For Use In Total Hip Arthroplasty. In 46th Annual Meeting; Orthopaedic Research Society: Orlando, FL, USA, 2000. [Google Scholar]
- Oral, E.; Beckos, C.G.; Muratoglu, O.K. Free Radical Elimination In Irradiated Uhmwpe Through Crystal Mobility In Phase Transition To The Hexagonal Phase. Polymer (Guildf) 2008, 49, 4733–4739. [Google Scholar] [CrossRef]
- Bracco, P.; Bellare, A.; Bistolfi, A.; Affatato, S. Ultra-High Molecular Weight Polyethylene: Influence of the Chemical, Physical and Mechanical Properties. Materials (Basel) 2017, 10, 791. [Google Scholar] [CrossRef]
- Deng, M.; Shalaby, S.W. Properties of self-reinforced ultra-high-molecular-weight polyethylene composites. Biomaterials 1997, 18, 645–655. [Google Scholar] [CrossRef]
- Dolezel, B.; Adamirova, L. Method of hygienically safe stabilization of polyolefines against thermoxidative and photooxidative degradation. Czechoslovakian Social. Repub. 1982, 221, 403. [Google Scholar]
- Brach del Prever, E.M.; Camino, G.; Costa, L.; Crova, M.; Dallera, A.; Gallianro, P. Impianto Protesico Contenente un Componente di Materiale Plastico. Italian Patent 1271590, May 1994. [Google Scholar]
- Bracco, P.; Oral, E. Vitamin E-stabilized UHMWPE for Total Joint Implants: A Review. Clin. Orthop. Relat. Res. 2011, 469, 2286–2293. [Google Scholar] [CrossRef] [PubMed]
- Affatato, S.; De Mattia, J.S.; Bracco, P.; Pavoni, E.; Taddei, P. Wear performance of neat and vitamin E blended highly cross-linked PE under severe conditions: The combined effect of accelerated ageing and third body particles during wear test. J. Mech. Behav. Biomed. Mater. 2016, 64, 240–252. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Bracco, P.; Costa, L. Vitamin-e-Blended UHMWPE Biomaterials. In UHMWPE Biomaterials Handbook; Elsevier: Amsterdam, The Netherlands, 2009; pp. 237–247. ISBN 9780123747211. [Google Scholar]
- Oral, E.; Rowell, S.L.; Muratoglu, O.K. The effect of α-tocopherol on the oxidation and free radical decay in irradiated UHMWPE. Biomaterials 2006, 27, 5580–5587. [Google Scholar] [CrossRef] [PubMed]
- Oral, E.; Wannomae, K.K.; Hawkins, N.; Harris, W.H.W.H.; Muratoglu, O.K.O.K. α-Tocopherol-doped irradiated UHMWPE for high fatigue resistance and low wear. Biomaterials 2004, 25, 5515–5522. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Bracco, P.; Costa, L.; Oral, E.; Muratoglu, O.K. Vitamin E-Blended UHMWPE Biomaterilas. In UHMWPE Biomaterials Handbook: Ultra High Molecular Weight Polyethylene in Total Joint Replacement and Medical Devices; Kurtz, S.M., Ed.; Elsevier: Norwich, NY, USA, 2015; p. 840. ISBN 0323354351. [Google Scholar]
- Anguiano-Sanchez, J.; Martinez-Romero, O.; Siller, H.R.; Diaz-Elizondo, J.A.; Flores-Villalba, E.; Rodriguez, C.A. Influence of PEEK Coating on Hip Implant Stress Shielding: A Finite Element Analysis. Comput. Math. Methods Med. 2016, 2016, 6183679. [Google Scholar] [CrossRef]
- Cowie, R.M.; Briscoe, A.; Fisher, J.; Jennings, L.M. PEEK-OPTIMA TM as an alternative to cobalt chrome in the femoral component of total knee replacement: A preliminary study. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2016, 230, 1008–1015. [Google Scholar] [CrossRef]
- Kurtz, S.; Devine, J.N. PEEK biomaterials in trauma, orthopedic, and spinal implants. Biomaterials 2007, 28, 4845–4869. [Google Scholar] [CrossRef]
- Kurtz, S. PEEK Biomaterials Handbook; Elsevier: Amsterdam, The Netherlands, 2012; ISBN 9781437744637. [Google Scholar]
- Wang, A.; Lin, R.; Polineni, V.K.; Essner, A.; Stark, C.; Dumbleton, J.H. Carbon fiber reinforced polyether ether ketone composite as a bearing surface for total hip replacement. Tribol. Int. 1998, 31, 661–667. [Google Scholar] [CrossRef]
- Grupp, T.M.; Utzschneider, S.; Schröder, C.; Schwiesau, J.; Fritz, B.; Maas, A.; Blömer, W.; Jansson, V. Biotribology of alternative bearing materials for unicompartmental knee arthroplasty. Acta Biomater. 2010, 6, 3601–3610. [Google Scholar] [CrossRef]
- Brockett, C.L.; Carbone, S.; Abdelgaied, A.; Fisher, J.; Jennings, L.M. Influence of contact pressure, cross-shear and counterface material on the wear of PEEK and CFR-PEEK for orthopaedic applications. J. Mech. Behav. Biomed. Mater. 2016, 63, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Affatato, S.; Traina, F.; Ruggeri, O.; Toni, A. Wear of metal-on-metal hip bearings: Metallurgical considerations after hip simulator studies. Int. J. Artif. Organs 2011, 34, 1155–1164. [Google Scholar] [CrossRef]
- Ihaddadene, R.; Affatato, S.; Zavalloni, M.; Bouzid, S.; Viceconti, M. Carbon composition effects on wear behaviour and wear mechanisms of metal-on-metal hip prosthesis. Comput. Methods Biomech. Biomed. Engin. 2011, 14, 33–34. [Google Scholar] [CrossRef]
- Davis, J.R. ASM Specialty Handbook: Nickel, Cobalt, and Their Alloys; ASM International: Almere, The Netherlands, 2000; ISBN 978-0-87170-685-0. [Google Scholar]
- Clemow, A.J.T.; Daniell, B.L. Solution treatment behavior of Co-Cr-Mo alloy. J. Biomed. Mater. Res. 1979, 13, 265–279. [Google Scholar] [CrossRef]
- Delaunay, C.; Petit, I.; Learmonth, I.D.; Oger, P.; Vendittoli, P.A. Metal-on-metal bearings total hip arthroplasty: The cobalt and chromium ions release concern. Orthop. Traumatol. Surg. Res. 2010, 96, 894–904. [Google Scholar] [CrossRef]
- Brodner, W.; Bitzan, P.; Meisinger, V.; Kaider, A.; Gottsauner-Wolf, F.; Kotz, R. Elevated serum cobalt with metal-on-metal articulating surfaces. J. Bone Jt. Surg. Br. 1997, 79, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Hallab, N.J.; Anderson, S.; Stafford, T.; Glant, T.; Jacobs, J.J. Lymphocyte responses in patients with total hip arthroplasty. J. Orthop. Res. 2005, 23, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.J.; Hallab, N.J.; Skipor, A.K.; Urban, R.M. Metal degradation products: a cause for concern in metal-metal bearings? Clin. Orthop. Relat. Res. 2003, 417, 139–147. [Google Scholar] [CrossRef]
- Yang, X.; Hutchinson, C.R. Corrosion-wear of β-Ti alloy TMZF (Ti-12Mo-6Zr-2Fe) in simulated body fluid. Acta Biomater. 2016, 42, 429–439. [Google Scholar] [CrossRef]
- Good, V.; Ries, M.; Barrack, R.L.; Widding, K.; Hunter, G.; Heuer, D. Reduced Wear With Oxidized Zirconium Femoral Heads. J. Bone Jt. Surgery-american Vol. 2003, 85, 105–110. [Google Scholar] [CrossRef]
- Langton, D.J.; Jameson, S.S.; Joyce, T.J.; Hallab, N.J.; Natu, S.; Nargol, A.V.F. Early failure of metal-on-metal bearings in hip resurfacing and large-diameter total hip replacement. J. Bone Jt. Surg. Br. 2010, 92-B, 38–46. [Google Scholar] [CrossRef]
- Underwood, R.J.; Zografos, A.; Sayles, R.S.; Hart, A.; Cann, P. Edge loading in metal-on-metal hips: low clearance is a new risk factor. Proc. Inst. Mech. Eng. H 2012, 226, 217–226. [Google Scholar] [CrossRef]
- Kingery, W.D. Introduction to Ceramics; John Wiley: Hoboken, NJ, USA, 2016; ISBN 047155460X. [Google Scholar]
- Hsu, S.M.; Shen, M.C. Ceramic Wear Maps. Wear 1996, 200, 154–175. [Google Scholar] [CrossRef]
- Cuckler, J.M.; Bearcroft, J.; Asgian, C.M. Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin. Orthop. Relat. Res. 1995, 317, 57–63. [Google Scholar]
- Willman, G. Ceramics for total hip replacement - what a surgeon should know. Orthopedics 1998, 21, 173–177. [Google Scholar]
- Boutin, P. [Alumina and its use in surgery of the hip. (Experimental study)]. Press. Med. 1971, 79, 639–640. [Google Scholar]
- Boutin, P.; Blanquaert, D. A study of the mechanical properties of alumina-on-alumina total hip prosthesis. Rev. Chir. Orthop. Reparatrice Appar. Mot. 1981, 67, 279–287. [Google Scholar]
- Hamadouche, M.; Sedel, L. Ceramics in orthopaedics. J. Bone Jt. Surg. Br. 2000, 82, 1095–1099. [Google Scholar] [CrossRef]
- Piconi, C.; Maccauro, G.; Muratori, F.; Branch Del Prever, E. Alumina and zirconia ceramics in joint replacements. JABB 2003, 1, 19–32. [Google Scholar]
- Affatato, S.; Ruggiero, A.; Merola, M. Advanced biomaterials in hip joint arthroplasty. A review on polymer and ceramics composites as alternative bearings. Compos. Part B Eng. 2015, 83, 276–283. [Google Scholar] [CrossRef]
- Affatato, S.; Jaber, S.A.; Taddei, P. Ceramics for hip joint replacement. In Biomaterials in Clinical Practice; Zivic, F., Ed.; Springer: Berlin, Germany, 2017. [Google Scholar]
- Affatato, S.; Traina, F.; Mazzega-Fabbro, C.; Sergo, V.; Viceconti, M. Is ceramic-on-ceramic squeaking phenomenon reproducible in vitro? A long-term simulator study under severe conditions. J. Biomed Mater Res. B Appl. Biomater 2009, 91, 264–271. [Google Scholar] [CrossRef]
- Jacobs, B.C.A.; Greenwald, A.S.; Oxon, D.; Anderson, P.A.; Matthew, J.; Mihalko, W.M. Squeaky Hips Make Media, Medical Noise; American Academy of Orthopaedic Surgeons: Rosemont, IL, USA, 2008. [Google Scholar]
- Wu, G.L.; Zhu, W.; Zhao, Y.; Ma, Q.; Weng, X.S. Hip squeaking after ceramic-on-ceramic total hip arthroplasty. Chin. Med. J. (Engl.) 2016, 129, 1861–1866. [Google Scholar] [CrossRef]
- De Aza, A.H.; Chevalier, J.; Fantozzi, G.; Schehl, M.; Torrecillas, R. Crack growth resistance of alumina, zirconia and zirconia toughened alumina ceramics for joint prostheses. Biomaterials 2002, 23, 937–945. [Google Scholar] [CrossRef]
- Rahaman, M.N.; Yao, A.; Bal, B.S.; Garino, J.P.; Ries, M.D. Ceramics for Prosthetic Hip and Knee Joint Replacement. J. Am. Ceram. Soc. 2007, 90, 1965–1988. [Google Scholar] [CrossRef]
- Kelly, J.R.; Denry, I. Stabilized zirconia as a structural ceramic: An overview. Dent. Mater. 2008, 24, 289–298. [Google Scholar] [CrossRef]
- VanValzah, J.R.; Eaton, H.E. Cooling rate effects on the tetragonal to monoclinic phase transformation in aged plasma-sprayed yttria partially stabilized zirconia. Surf. Coat. Technol. 1991, 46, 289–300. [Google Scholar] [CrossRef]
- Platt, P.; Frankel, P.; Gass, M.; Howells, R.; Preuss, M. Finite element analysis of the tetragonal to monoclinic phase transformation during oxidation of zirconium alloys. J. Nucl. Mater. 2014, 454, 290–297. [Google Scholar] [CrossRef]
- Maccauro, G.; Rossi Iommetti, P.; Raffaelli, L.; Manicone, P.F. Alumina and Zirconia Ceramic for Orthopaedic and Dental Devices. In Biomaterials Applications for Nanomedicine; Pignatello, R., Ed.; InTech: London, UK, 2011; Volume 3, p. 485. ISBN 9533076615. [Google Scholar]
- Pitto, R.P.; Blanquaert, D.; Hohmann, D. Alternative bearing surfaces in total hip arthroplasty: Zirconia-alumina pairing. Contribution or caveat? Acta Orthop. Belg. 2002, 68, 242–250. [Google Scholar]
- Affatato, S.; Testoni, M.; Cacciari, G.L.; Toni, A. Mixed oxides prosthetic ceramic ball heads. Part 2: effect of the ZrO2 fraction on the wear of ceramic on ceramic joints. Biomaterials 1999, 20, 971–975. [Google Scholar] [CrossRef]
- Affatato, S.; Goldoni, M.; Testoni, M.; Toni, A. Mixed oxides prosthetic ceramic ball heads. Part 3: Effect of the ZrO2 fraction on the wear of ceramic on ceramic hip joint prostheses. A long-term in vitro wear study. Biomaterials 2001, 22, 717–723. [Google Scholar] [CrossRef]
- Piconi, C.; Burger, W.; Richter, H.G.; Cittadini, A.; Maccauro, G.; Covacci, V.; Bruzzese, N.; Ricci, G.A.; Marmo, E. Y-TZP ceramics for artificial joint replacements. Biomaterials 1998, 19, 1489–1494. [Google Scholar] [CrossRef]
- Chevalier, J. What future for zirconia as a biomaterial? Biomaterials 2006, 27, 535–543. [Google Scholar] [CrossRef]
- Affatato, S.; Torrecillas, R.; Taddei, P.; Rocchi, M.; Fagnano, C.; Ciapetti, G.; Toni, A. Advanced nanocomposite materials for orthopaedic applications. I. A long-term in vitro wear study of zirconia-toughened alumina. J. Biomed. Mater. Res. Part B Appl. Biomater. 2006, 78, 76–82. [Google Scholar] [CrossRef]
- Gadow, R.; Kern, F. Novel zirconia-alumina nanocomposites combining high strength and toughness. In Advanced Engineering Materials; John Wiley & Sons: Hoboken, NJ, USA, 2010; Volume 12, pp. 1220–1223. [Google Scholar]
- Dickinson, A.; Browne, M.; Jeffers, J.; Taylor, A. Development of a Ceramic Acetabular Cup Design for Improved in vivo Stability and Integrity. In BIOLOX Symposium; Sprimger: Edinburgh, UK, 2009; Volume 13, p. 227. [Google Scholar]
- Merkert, P. Next generation ceramic bearings. In Bioceramics in Joint Arthroplasty; Springer: Berlin, Germany, 2003; pp. 123–125. [Google Scholar]
- Affatato, S.; Modena, E.; Toni, A.; Taddei, P. Retrieval analysis of three generations of Biolox®femoral heads: Spectroscopic and SEM characterisation. J. Mech. Behav. Biomed. Mater. 2012, 13, 118–128. [Google Scholar] [CrossRef]
- Deville, S.; Chevalier, J.; Fantozzi, G.; Bartolomé, J.F.; Requena, J.; Moya, J.S.; Torrecillas, R.; Díaz, L.A. Low-temperature ageing of zirconia-toughened alumina ceramics and its implication in biomedical implants. J. Eur. Ceram. Soc. 2003, 23, 2975–2982. [Google Scholar] [CrossRef]
- Gutknecht, D.; Chevalier, J.; Garnier, V.; Fantozzi, G. Key role of processing to avoid low temperature ageing in alumina zirconia composites for orthopaedic application. J. Eur. Ceram. Soc. 2007, 27, 1547–1552. [Google Scholar] [CrossRef]
- Massin, P.; Achour, S. Wear products of total hip arthroplasty: The case of polyethylene Produits d ’ usure des arthroplasties totales de hanche: le cas du polyéthylène. Morphologie 2017, 101, 1–8. [Google Scholar] [CrossRef]
- Guy, R.; Nockolds, C.; Phillips, M.; Roques-Carmes, C. Implications of Polishing Techniques in Quantitative X-Ray Microanalysis. J. Res. Natl. Inst. Stand. Technol. 2002, 107, 639–662. [Google Scholar]
- Butler, M.F.; Donald, A.M.; Ryan, A.J. Time resolved simultaneous small- and wide-angle x-ray scattering during polyethylene deformation-II. Cold drawing of linear polyethylene. Polymer1 1998, 39, 781–792. [Google Scholar] [CrossRef]
- Lewis, G. Polyethylene wear in total hip and knee arthroplasties. J. Biomed. Mater. Res. 1997, 38, 55–75. [Google Scholar] [CrossRef]
- Landolt, D.; Mischler, S.; Stemp, M. Electrochemical methods in tribocorrosion: A critical appraisal. Electrochim. Acta 2001, 46, 3913–3929. [Google Scholar] [CrossRef]
- Hodgson, A.W.E.; Kurz, S.; Virtanen, S.; Fervel, V.; Olsson, C.-O.A.; Mischler, S. Passive and transpassive behaviour of CoCrMo in simulated biological solutions. Electrochim. Acta 2004, 49, 2167–2178. [Google Scholar] [CrossRef]
- Suñer, S.; Tipper, J.L.; Emami, N. Biological effects of wear particles generated in total joint replacements: trends and future prospects. Tribol. Mater. Surfaces Interfaces 2012, 6, 39–52. [Google Scholar] [CrossRef]
- StanDIN 50320 Wear; Terms, Systematic Analysis of Wear Processes, Classification of Wear Phenomenadards; Beuth-Verlag: Berlin, Germany, 1979.
- Chevalier, J.; Taddei, P.; Gremillard, L.; Deville, S.; Fantozzi, G.; Bartolomé, J.F.; Pecharroman, C.; Moya, J.S.; Diaz, L.A.; Torrecillas, R.; Affatato, S. Reliability assessment in advanced nanocomposite materials for orthopaedic applications. J. Mech. Behav. Biomed. Mater. 2011, 4, 303–314. [Google Scholar] [CrossRef]
- Garino, J.P. Ceramic component fracture: trends and recommendations with modern components based on improved reporting methods. In Bioceramics and Alternative Bearings in Joint Arthroplasty: Proceedings; D’Antonio, J.A., Dietrich, M., Eds.; Steinkopff: Heidelberg, Germany, 2005; p. 218. ISBN 3798515409. [Google Scholar]
- Weisse, B.; Affolter, C.; Stutz, A.; Terrasi, G.P.; Köbel, S.; Weber, W. Influence of contaminants in the stem—ball interface on the static fracture load of ceramic hip joint ball heads. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2008, 222, 829–835. [Google Scholar] [CrossRef]
- Rehmer, A.; Bishop, N.E.; Morlock, M.M. Influence of assembly procedure and material combination on the strength of the taper connection at the head-neck junction of modular hip endoprostheses. Clin. Biomech. (Bristol, Avon) 2012, 27, 77–83. [Google Scholar] [CrossRef]
- Nevelos, J.E.; Ingham, E.; Doyle, C.; Nevelos, A.B.; Fisher, J. Wear of HIPed and non-HIPed alumina-alumina hip joints under standard and severe simulator testing conditions. Biomaterials 2001, 22, 2191–2197. [Google Scholar] [CrossRef]
- Dorlot, J.-M.; Christel, P.; Meunier, A. Wear analysis of retrieved alumina heads and sockets of hip prostheses. J. Biomed. Mater. Res. 1989, 23, 299–310. [Google Scholar] [CrossRef]
- Mittelmeier, H.; Heisel, J. Sixteen-years’ Experience With Ceramic Hip Prostheses. Clin. Orthop. Relat. Res. 1992, 282, 64–72. [Google Scholar] [CrossRef]
- Brandt, J.-M.; Vecherya, A.; Guenther, L.E.; Koval, S.F.; Petrak, M.J.; Bohm, E.R.; Wyss, U.P. Wear testing of crosslinked polyethylene: Wear rate variability and microbial contamination. J. Mech. Behav. Biomed. Mater. 2014, 34, 208–216. [Google Scholar] [CrossRef]
- Grupp, T.M.; Holderied, M.; Mulliez, M.A.; Streller, R.; Jäger, M.; Blömer, W.; Utzschneider, S. Biotribology of a vitamin E-stabilized polyethylene for hip arthroplasty—Influence of artificial ageing and third-body particles on wear. Acta Biomater. 2014, 10, 3068–3078. [Google Scholar] [CrossRef]
- Moro, T.; Takatori, Y.; Kyomoto, M.; Ishihara, K.; Kawaguchi, H.; Hashimoto, M.; Tanaka, T.; Oshima, H.; Tanaka, S. Wear resistance of the biocompatible phospholipid polymer-grafted highly cross-linked polyethylene liner against larger femoral head. J. Orthop. Res. 2015, 33, 1103–1110. [Google Scholar] [CrossRef]
- Zietz, C.; Fabry, C.; Baum, F.; Bader, R.; Kluess, D. The Divergence of Wear Propagation and Stress at Steep Acetabular Cup Positions Using Ceramic Heads and Sequentially Cross-Linked Polyethylene Liners. J. Arthroplast. 2015, 30, 1458–1463. [Google Scholar] [CrossRef]
- Gremillard, L.; Martin, L.; Zych, L.; Crosnier, E.; Chevalier, J.; Charbouillot, A.; Sainsot, P.; Espinouse, J.; Aurelle, J.-L. Combining ageing and wear to assess the durability of zirconia-based ceramic heads for total hip arthroplasty. Acta Biomater. 2013, 9, 7545–7555. [Google Scholar] [CrossRef]
- Reinders, J.; Sonntag, R.; Heisel, C.; Reiner, T.; Vot, L.; Kretzer, J.P. Wear performance of ceramic-on-metal hip bearings. PLoS ONE 2013, 8, e73252. [Google Scholar] [CrossRef]
- Williams, S.; Al-Hajjar, M.; Isaac, G.H.; Fisher, J. Comparison of ceramic-on-metal and metal-on-metal hip prostheses under adverse conditions. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101B, 770–775. [Google Scholar] [CrossRef]
- Halma, J.J.; Señaris, J.; Delfosse, D.; Lerf, R.; Oberbach, T.; van Gaalen, S.M.; de Gast, A. Edge loading does not increase wear rates of ceramic-on-ceramic and metal-on-polyethylene articulations. J. Biomed. Mater. Res. Part B Appl. Biomater. 2014, 102, 1627–1638. [Google Scholar] [CrossRef]
- Al-Hajjar, M.; Jennings, L.M.; Begand, S.; Oberbach, T.; Delfosse, D.; Fisher, J. Wear of novel ceramic-on-ceramic bearings under adverse and clinically relevant hip simulator conditions. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101, 1456–1462. [Google Scholar] [CrossRef]
- Al-Hajjar, M.; Carbone, S.; Jennings, L.M.; Begand, S.; Oberbach, T.; Delfosse, D.; Fisher, J. Wear of composite ceramics in mixed-material combinations in total hip replacement under adverse edge loading conditions. J. Biomed. Mater. Res. Part B Appl. Biomater. 2017, 105, 1361–1368. [Google Scholar] [CrossRef]
- Al-Hajjar, M.; Fisher, J.; Tipper, J.L.; Williams, S.; Jennings, L.M. Wear of 36-mm BIOLOX ® delta ceramic-on-ceramic bearing in total hip replacements under edge loading conditions. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2013, 227, 535–542. [Google Scholar] [CrossRef]
- Chan, F.W.; Bobyn, J.D.; Medley, J.B.; Krygier, J.J.; Tanzer, M. The Otto Aufranc Award. Wear and lubrication of metal-on-metal hip implants. Clin. Orthop. Relat. Res. 1999, 10–24. [Google Scholar] [CrossRef]
- RIPO Annual Report 2016. 2018. Available online: https://www.riotinto.com/documents/RT_2016_Annual_report.pdf (accessed on 1 February 2019).
- Mayor, S. Registry data show increase in joint replacement surgery. BMJ 2017, 358, 1. [Google Scholar] [CrossRef]
- Kurtz, S.; Ong, K.L.; Schmier, J.; Mowat, F.; Saleh, K.; Dybvik, E.; Kärrholm, J.; Garellick, G.; Havelin, L.I.; Furnes, O.; Malchau, H.; Lau, E. Future clinical and economic impact of revision total hip and knee arthroplasty. J. Bone Joint Surg. Am. 2007, 89, 144–151. [Google Scholar] [CrossRef]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg Am 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Rajeshshyam, R.; Chockalingam, K.; Gayathri, V.; Prakash, T. Reduction of metallosis in hip implant using thin film coating. In AIP Conference Proceedings; AIP Publishing LLC: Melville, NY, USA, 2018; Volume 1943, p. 020090. [Google Scholar]
- Bijukumar, D.R.; Segu, A.; Souza, J.C.M.; Li, X.; Barba, M.; Mercuri, L.G.; Jacobs, J.J.; Mathew, M.T. Systemic and local toxicity of metal debris released from hip prostheses: A review of experimental approaches. Nanomed. Nanotechnol. Biol. Med. 2018, 14, 951–963. [Google Scholar] [CrossRef]
- Neuwirth, A.L.; Ashley, B.S.; Hardaker, W.M.; Sheth, N.P. Metal-on-Metal Hip Implants: Progress and Problems. In Biomedical Applications of Metals; Springer International Publishing: Cham, Switzerland, 2018; pp. 73–93. [Google Scholar]
- Abdel Jaber, S.; Affatato, S. An overview of In Vitro Mechanical and Structural Characterization of Hip Prosthesis Components; Springer: Berlin, Germany, 2017; ISBN 9783319680255. [Google Scholar]
- Lee, J.-M. The Current Concepts of Total Hip Arthroplasty. Hip Pelvis 2016, 28, 191–200. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Soft Bearings | Paired Materials * | Overall Wear Rate (mm3/Mc) | Ref. |
|---|---|---|---|
| MoP | CoCr—XLPE | 6.71 ± 1.03 | [135] |
| Biolox®Delta—XLPE | 2.0 ± 0.3 ** | [136] | |
| CoP | CoCrMo—XLPE | 4.09 ± 0.64 | [137] |
| Alumina—XLPE | 3.35 ± 0.29 | [138] | |
| Alumina—PE | 34 | [139] | |
| ZTA—PE | 80 | [140] |
| Hard Bearings | Paired Materials * | Overall Wear Rate (mm3/Mc) | Ref. |
|---|---|---|---|
| CoM | CoMplete | 0.129 ± 0.096 | [141] |
| Biolox®Delta - CoCrMo | 0.02 ± 0.01 | [142] | |
| Biolox®Delta-CoCrMo | 0.87 | [28] | |
| CoC | Biolox®Forte-Biolox®Forte | 0.052 | [28] |
| Alumina-Alumina | 0.03 | [143] | |
| ATZ-ATZ | 0.024 | [143] | |
| ATZ-ATZ | 0.06 ± 0.004 | [144] | |
| ZTA-ZTA | 0.14 ± 0.10 | [144] | |
| ATZ-ZTA | 0.18 | [145] | |
| ATZ-Alumina | 0.20 | [145] | |
| Alumina-Alumina | 0.74 ± 1.73 | [144] | |
| Biolox®Delta-Biolox®Delta | 0.10 | [146] | |
| MoM | CoCrMo-CoCrMo | 0.60 ± 0.18 | [142] |
| CoCrMo-CoCrMo | 0.11 ± 0.055 | [147] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merola, M.; Affatato, S. Materials for Hip Prostheses: A Review of Wear and Loading Considerations. Materials 2019, 12, 495. https://doi.org/10.3390/ma12030495
Merola M, Affatato S. Materials for Hip Prostheses: A Review of Wear and Loading Considerations. Materials. 2019; 12(3):495. https://doi.org/10.3390/ma12030495
Chicago/Turabian StyleMerola, Massimiliano, and Saverio Affatato. 2019. "Materials for Hip Prostheses: A Review of Wear and Loading Considerations" Materials 12, no. 3: 495. https://doi.org/10.3390/ma12030495
APA StyleMerola, M., & Affatato, S. (2019). Materials for Hip Prostheses: A Review of Wear and Loading Considerations. Materials, 12(3), 495. https://doi.org/10.3390/ma12030495