1. Introduction
Cutting tissue with drills and saws results in heat formation that may damage the surrounding tissues, leading to impaired bone regeneration [
1,
2,
3]. In contrast, laser ablation (a laser used as an osteotomy tool) works without contact force, thereby reducing the severe mechanical vibrations and heat damage generated by conventional cutting tools [
2,
4]. Avoiding heat damage improves the healing of the cut bone, making laser ablation a highly desired innovation in the field of maxillo-facial-, neuro- and orthopedic surgery [
2]. Moreover, lasers cut with greater precision than conventional tools [
5,
6,
7]. When irradiating bone and teeth with the Er:YAG laser (2.94 μm), water and hydroxyapatite absorb most of the laser energy. Teeth (with a composition close to bone) consist of 85–95% carbonated hydroxyapatite, 8–12% water, and 2–3% protein and lipids [
8,
9,
10]. Because the water content and Amide I/II bands in bone absorb so much IR radiation, different lasers for cutting bone in surgical applications have been investigated, including the holmium-doped yttrium aluminum garnet (Ho:YAG), carbon dioxide (CO
2) lasers, the erbium-doped yttrium aluminum garnet (Er:YAG) pulsed laser, and free-electron lasers (FEL) [
11,
12,
13,
14,
15,
16,
17]. The Er:YAG laser has a wavelength of 2.94 μm, corresponding to one of the absorption peaks of water and hydroxyapatite, the main component of bone [
1,
7], and corresponding to the wavelength where bone or teeth are ablated by means of photo-thermal vaporization.
The laser ablation process has been optimized for bone tissue and relies on a photothermic mechanism that results in thermal damage to the surrounding tissue unless a cooling system is used [
18,
19,
20,
21]. Recent investigations have shown that water on the exposed area prevents the carbonization of tissues around craters, thereby improving the ablation efficiency [
22,
23,
24] and increasing the ablation rate [
25,
26]. It has been argued that a high laser energy density improves the radiation ablation efficiency in wet conditions by confining the laser-generated plasma in the liquid layer, leading to a greater emission of acoustic and shock waves as compared to ambient air conditions [
26,
27]. However, high-energy laser systems are not suitable for tissue ablation and regeneration under dry conditions, as they produce a greater temperature dissipation around the exposed zone, which can lead to carbonization and a long wound-recovery time.
Long-pulsed fiber lasers may be more practical in an operating room because of their fiber-coupled output, and their smaller footprint and robustness to environmental vibrations than short-pulsed lasers [
28]. Long-pulsed lasers, such as millisecond-pulsed lasers, with several joules of energy, are also much less costly than ultra-short-pulsed lasers, such as femto or nanosecond pulsed ones, with millijoule energy. In addition, fiber lasers with a wavelength of 1.07 μm have a low absorption in water as compared to the Er:YAG lasers [
29,
30]. To minimize the energy loss in a wet environment, a laser wavelength of 1.07 µm may be appropriate as its absorption is lower than for the wavelength of the Er:YAG lasers [
3]. Because the absorption coefficient for a fiber laser at 1.07 µm is low in water (approximately 0.4cm
−1), the transmission through a 14 mm water layer is around 80% [
27,
31,
32]. Therefore, when a bone is covered with water and irradiated by a fiber laser at 1.07 µm, it does not significantly reduce the energy reaching the bone. In contrast to a wavelength of 2.94 μm, this well-established wavelength for metal welding in the industry (1.07 µm) could be clinically studied for its suitability for knee surgery in a wet environment. Previous investigations were mainly conducted on metals and substrate samples for laser-welding applications [
33,
34].
However, in addition to being fast and accurate when cutting bone, lasers need to be safe as well. A tissue differentiation method could improve the safety of lasers as an osteotomy tool. This is particularly true if a laser system can be controlled by an
in situ and real-time automatic feedback system that not only differentiates specific types of human tissues but additionally stops automatically when the laser encounters tissues that are not meant to be ablated [
2,
4,
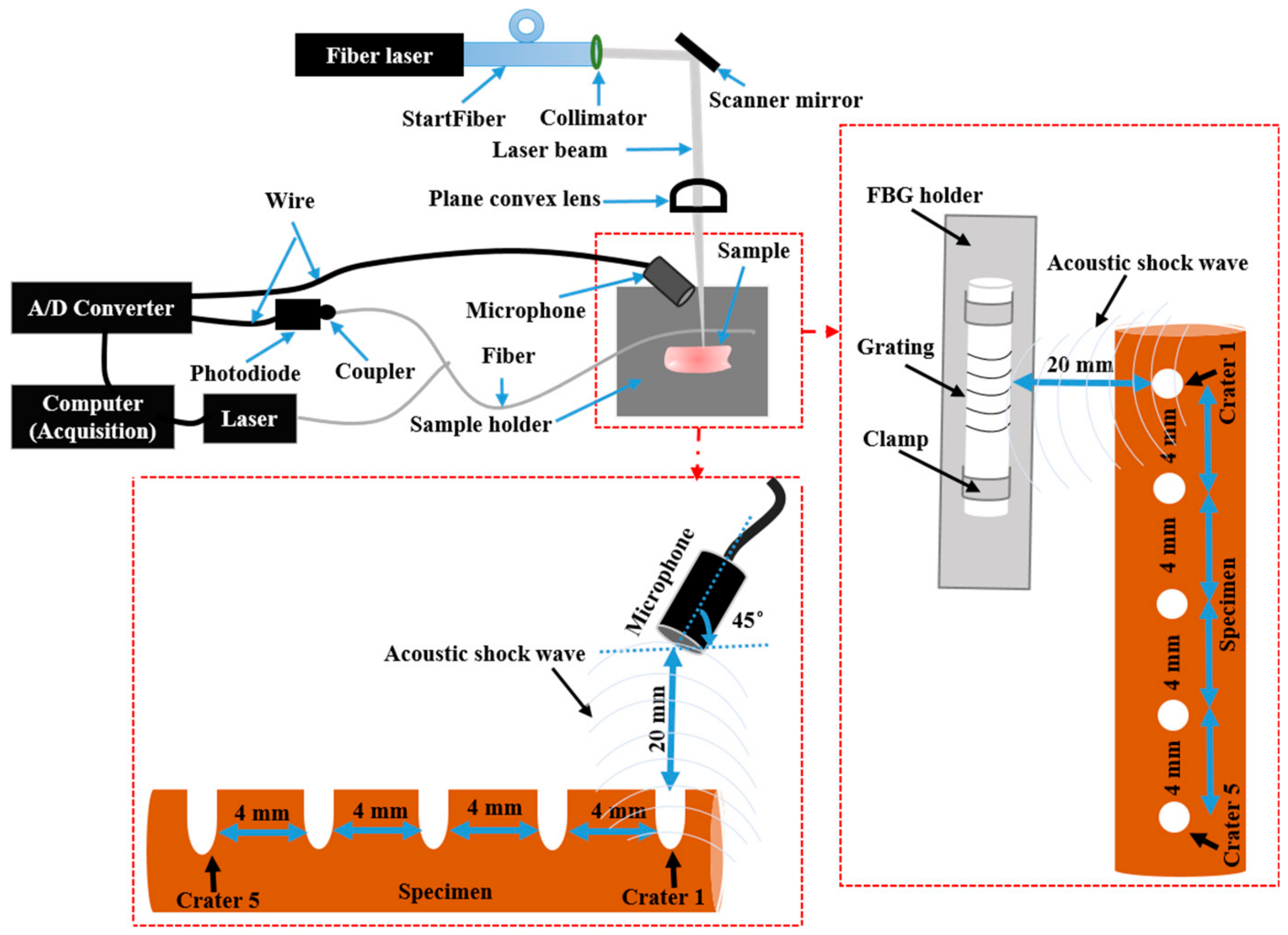
35]. Acoustic shock waves (ASWs) are generated when ablating material with a laser and can be measured using microphone and Fiber Bragg Grating (FBG) sensors [
4,
36,
37,
38]. Compared to standard microphones, FBG sensors are smaller, more sensitive, lightweight and immune to electromagnetic interference [
39,
40]. In this work, we investigate the laser tissue ablation of muscle and bone, using a long-pulsed laser with a center wavelength of 1.07 μm and pulse energies in the range of 0.75–15 J, under different ablation conditions (in terms of the ablation efficiency of bone and the impact of water on carbonization). We simultaneously recorded (with a microphone and an FBG) and differentiated the acoustic signals generated by the ablation of porcine bone and muscle. We used a Principle Component Analysis (PCA) to reduce the dimensionality of the ASWs measured from each specimen and the Mahalanobis distances method to differentiate the scores of the measured ASWs. Such a set-up has the potential to act as an optoacoustic feedback sensor for laser osteotomy.
4. Discussion
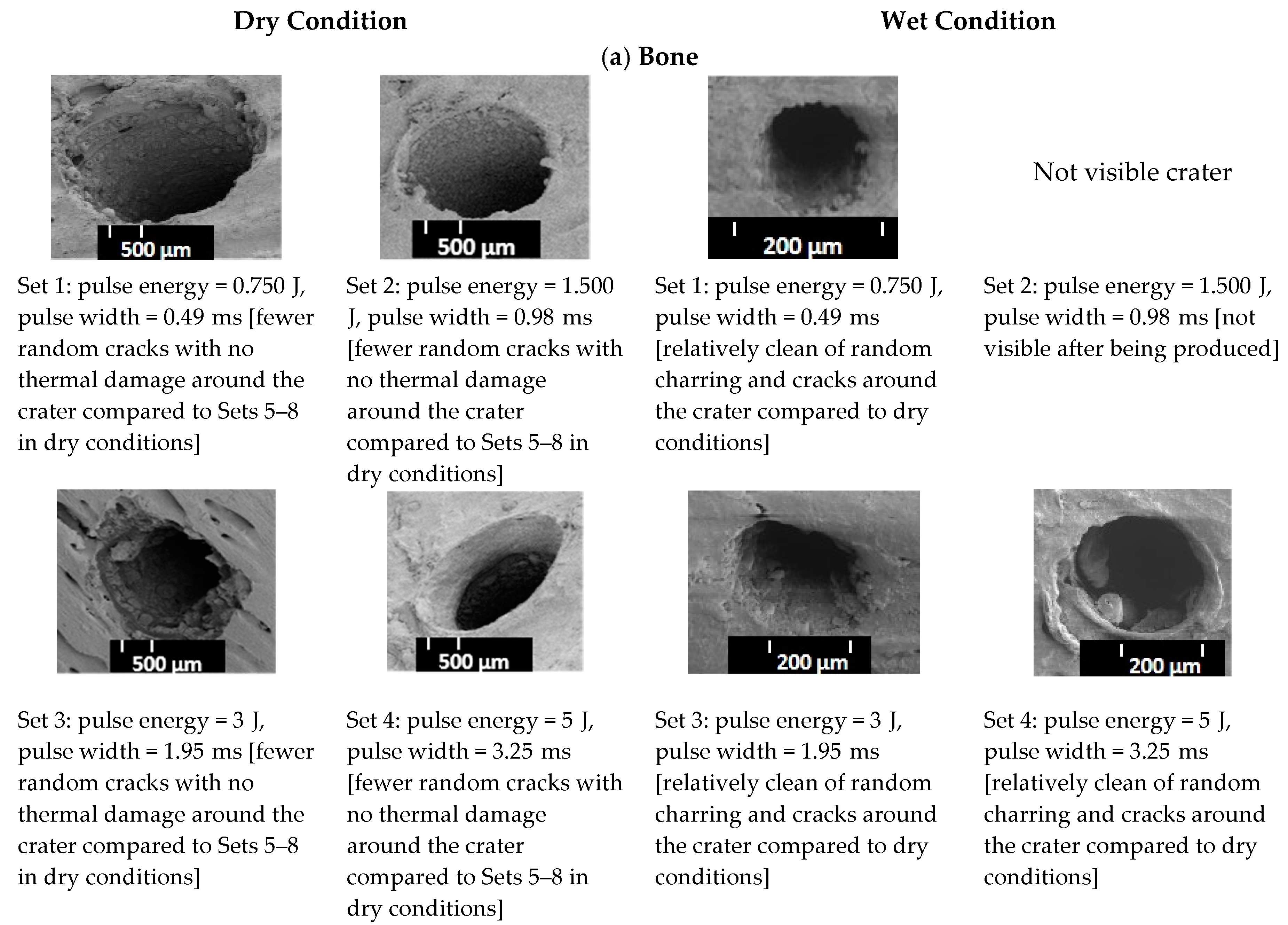
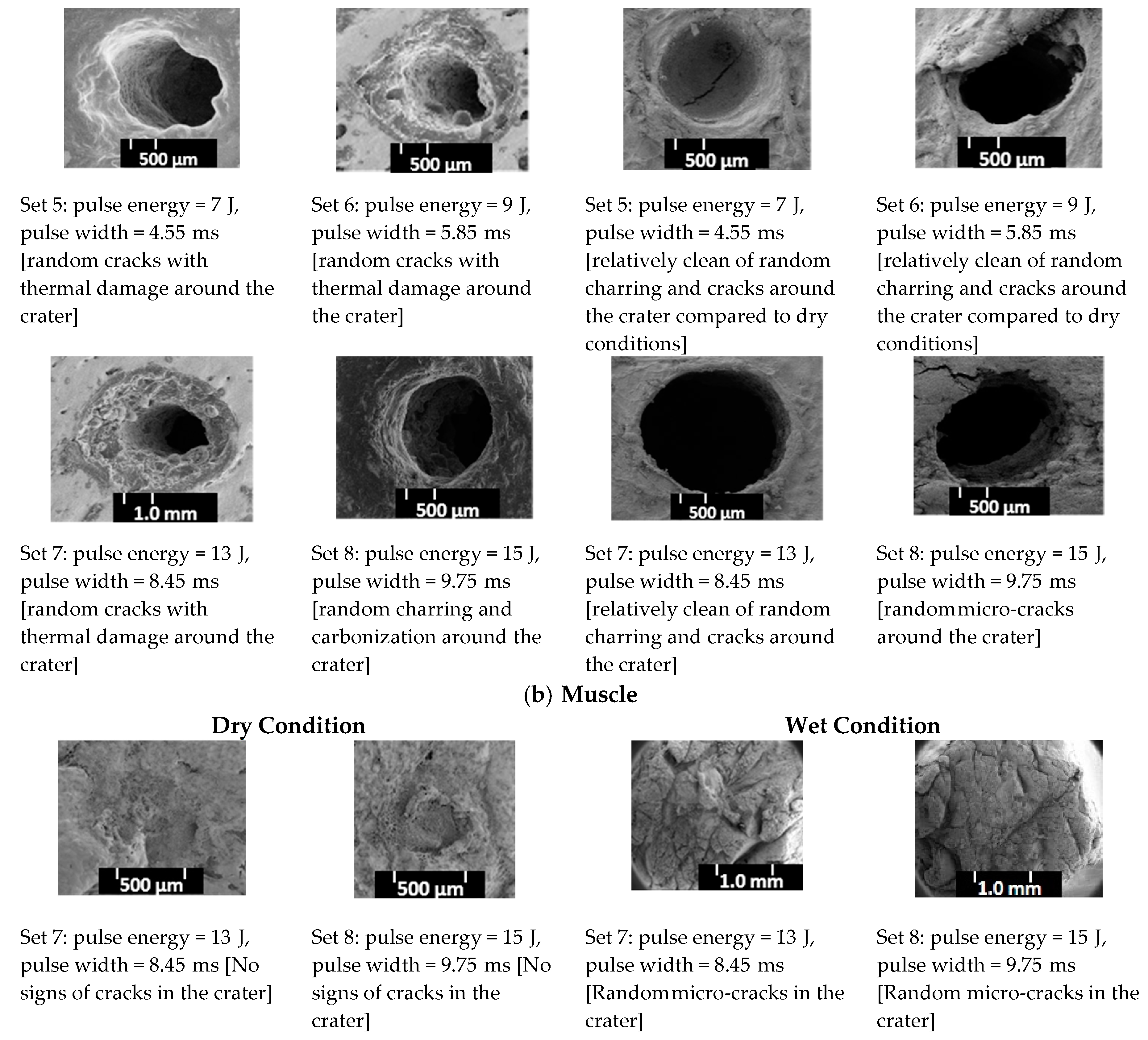
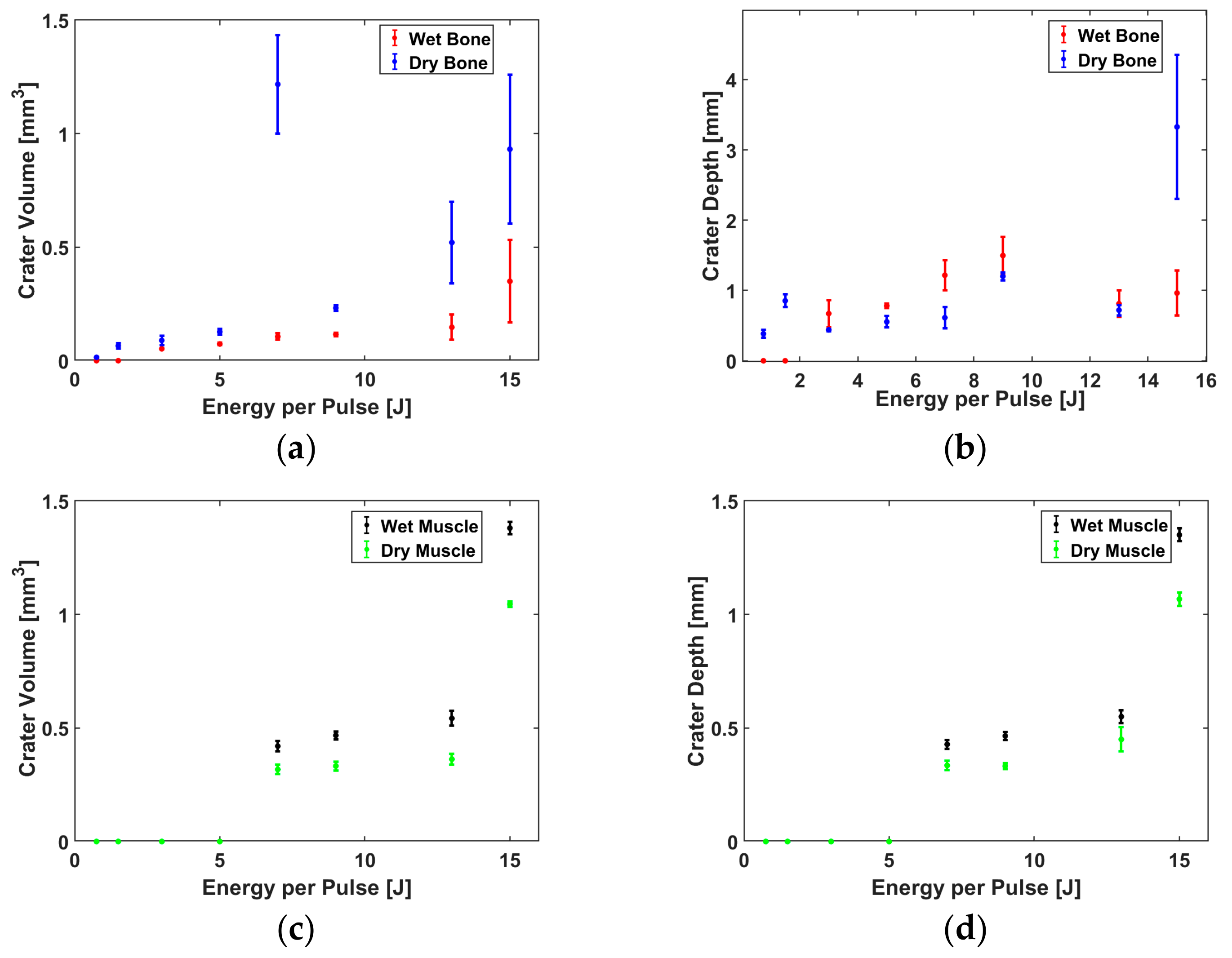
Under the wet conditions, Sets 1 to 7 showed craters with less random charring, fewer cracks around the ablated contours and without any signs of thermal damage, as compared to the dry condition. This is because the water partially hydrates the exposed surface and thus partially prevents the carbonization of healthy tissue, leading to an improvement in the ablation efficiency of the muscle, as compared to the dry conditions (
Figure 5c,d).
In contrast to the muscle, the volume of the craters made in the bone under the dry conditions was higher than those made in the wet conditions, except for a pulse energy of 0.75 J (
Figure 5a). One possible reason for this outcome is that, in the absence of a water-cooling system, the pulse energy applied in the dry conditions causes more random cracks around the crater compared to those created in the wet conditions, thereby increasing the width and inducing a higher crater volume. In other words, the dry bone at the surface is ablated due to a higher temperature and possible phase transformation taking place in the wet conditions, induced by large temperature gradients inside the exposed material [
4]. Apart from the crater volume in the bone created under the dry conditions,
Figure 5b and the two-way ANOVA test (
Appendix,
Table A2) showed that the difference in the mean depth of the craters made in the dry versus wet conditions was not statistically significant (
p > 0.05). This is due to the fact that bone rehydration was not sufficiently abundant to prevent an extensive heat diffusion [
44]. In this experiment, the laser energy was increased by prolonging the laser pulse; with longer pulse durations, there was more time for the heat to diffuse and create carbonization at the bottom of the craters and saturate the depth of the craters. That is why Sets 4 to 8 presented some random cracks and thermal damage around the craters in the bone, created under the dry conditions. These phenomena are mainly caused by an excessive heat accumulation during and after an exposure to a high laser energy within the range of 7–15 J. Therefore, the range of the laser pulse duration, from approximately 0.5 to 10 ms, is likely to influence the amount of heat spread during the laser pulse [
44,
45]. The SEM pictures of the craters in the muscle for Sets 7 and 8, created in the dry conditions, presented no signs of random cracks around the craters.
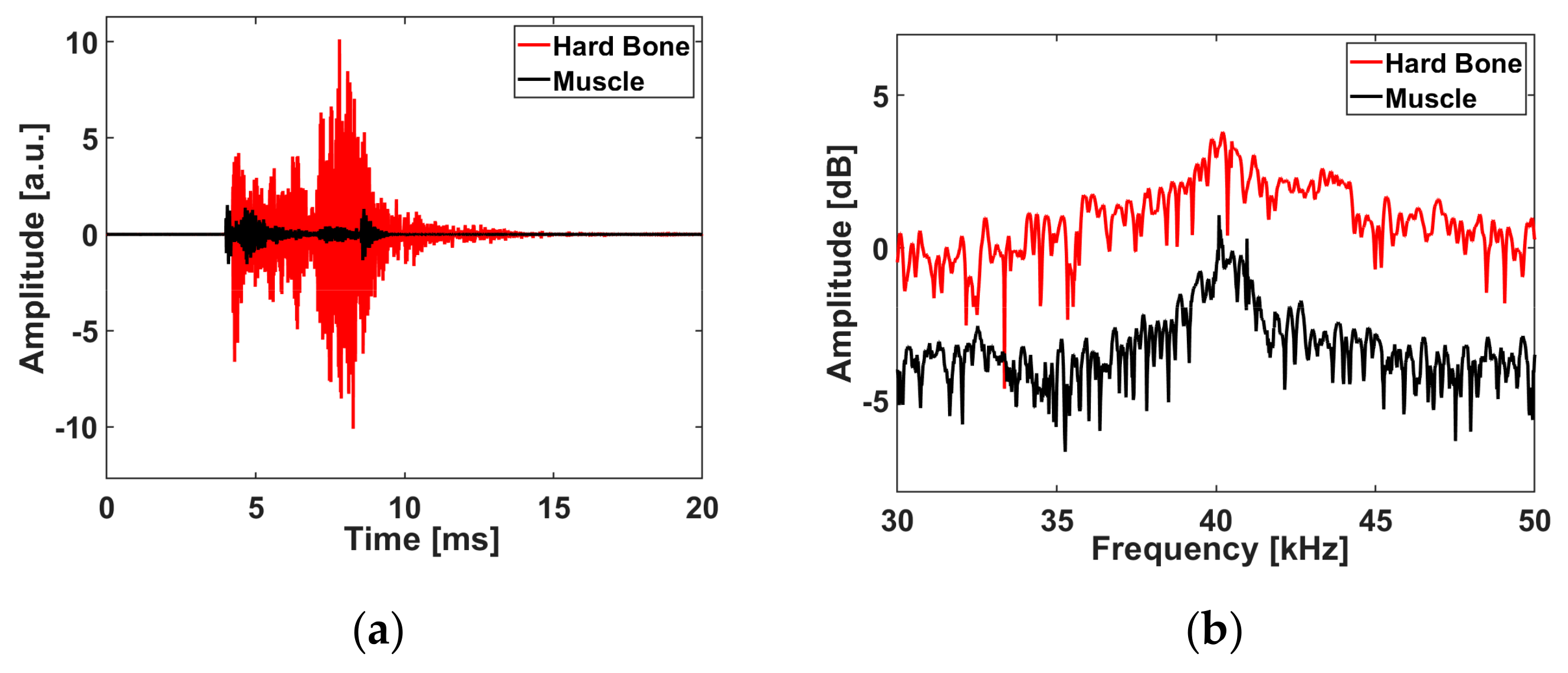
However, when ablated under the wet conditions, these sets presented some signs of random cracks and the depths of the craters made in the muscle were lower than those in the bone (under both conditions). This is probably because the muscle tissue started to shrink directly after the ablation. In Set 5, we observed that the maximum amplitude of the acoustic signal efrom th bone ablated in the wet conditions was higher than that from the muscle. Muscle is composed of 79% water, while hard bone or teeth consist of 85–95% carbonated hydroxyapatite, 8–12% water, and 2–3% protein and lipids. Therefore, we believe that the carbonated hydroxyapatite component in bone produces greater amplitudes of sound, as it is a compact component compared to muscle, which is mostly made of water [
8,
9,
10].
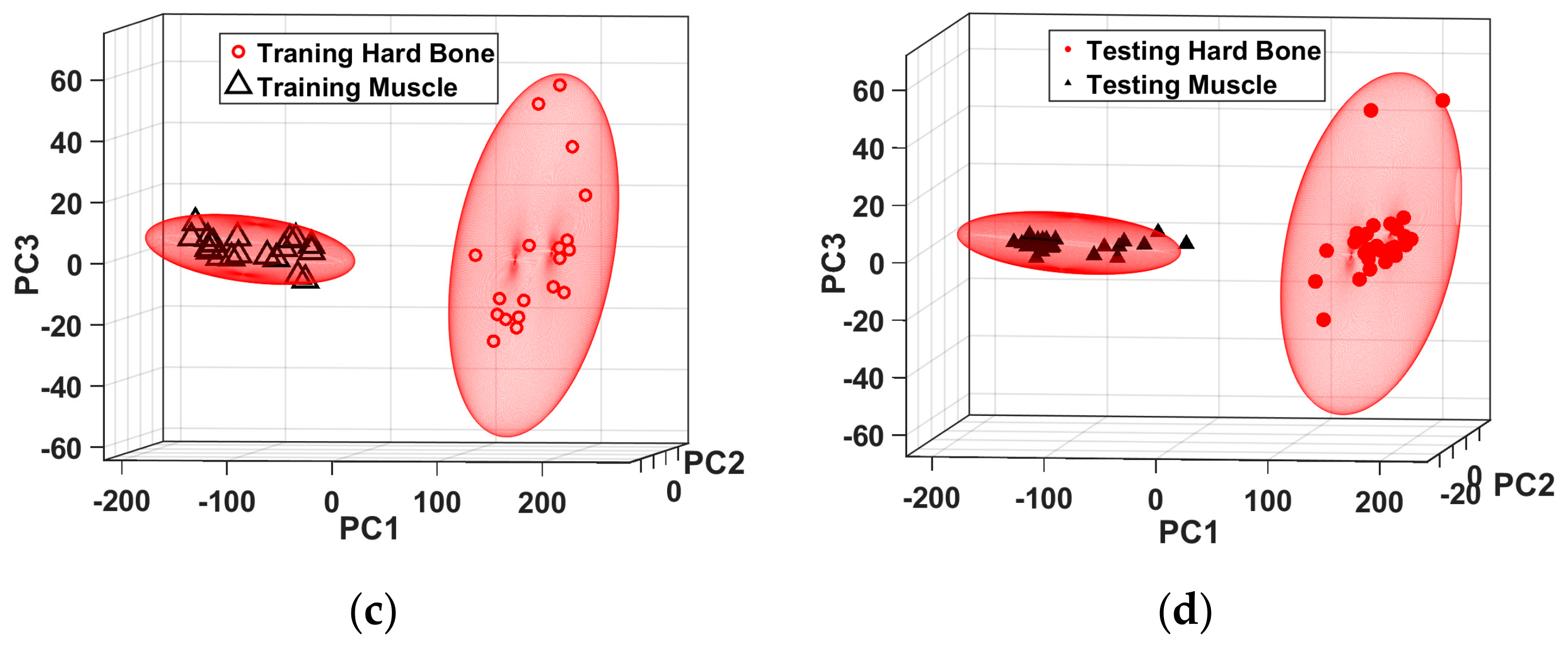
The resonant frequencies for bone and muscle cannot be used as parameters for tissue differentiation in the current stage of the project. This is mainly due to the limitation of the usable bandwidth (39–42 kHz) of the microphone that we used in this experiment. The spectrums of the acoustic pulses with shocks can extend beyond 1 MHz [
46]. Thus, precise frequency measurements of broadband acoustic signals generated during ablation, using broadband pressure sensors, will measure acoustic shock waves with higher frequency components [
35,
47,
48], which could then be used as frequency parameters to distinguish between ablated tissues. That is why the FBG, combined with a photodiode with a bandwidth of 2.5 MHz, resulted in a better classification error than the one measured by a microphone (
Table 2 and
Table 3).
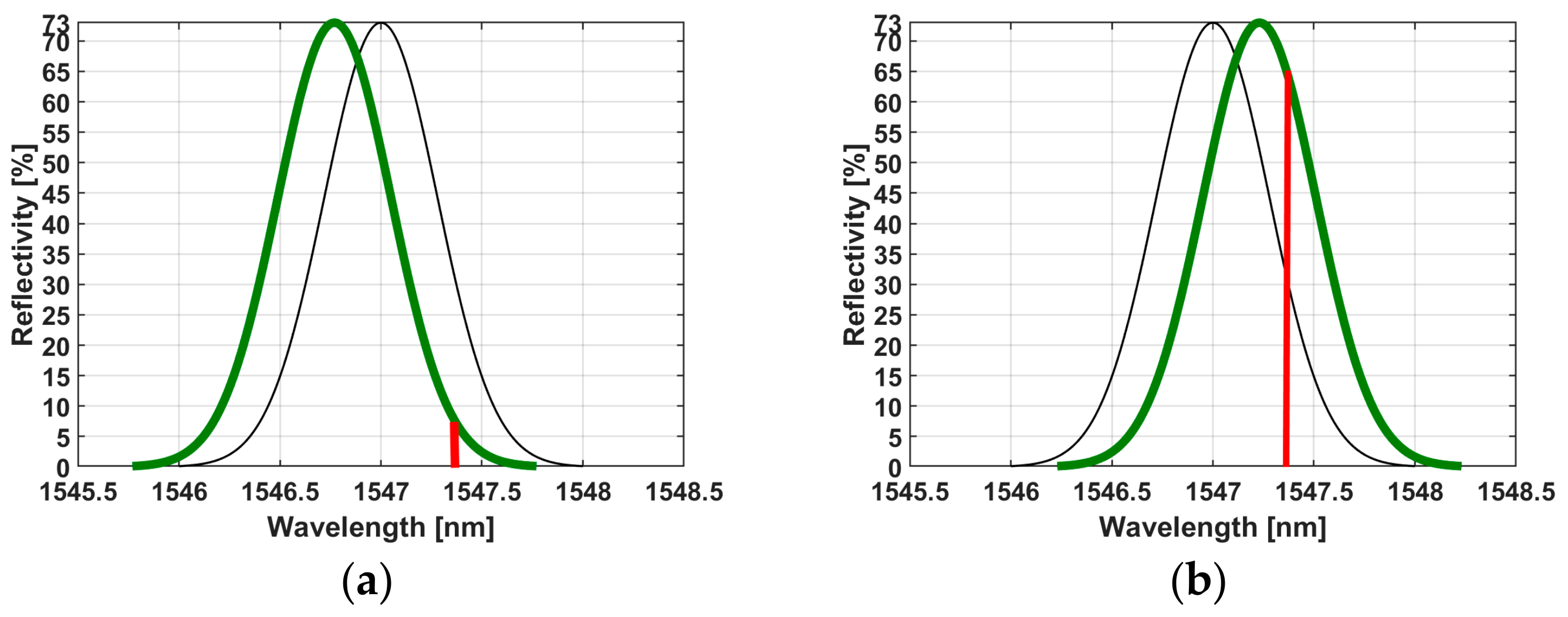
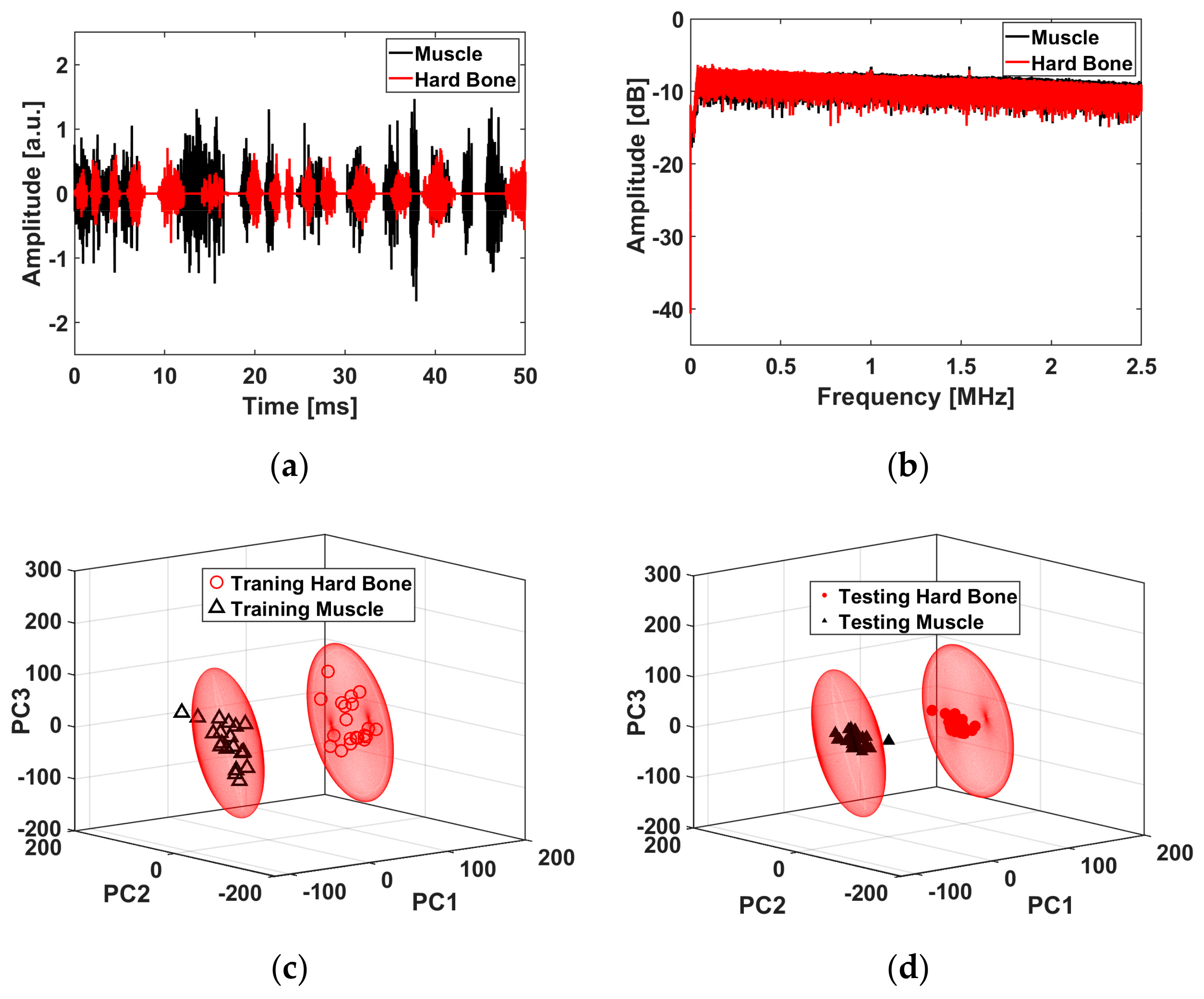
In contrast to the microphone, the FBG measurements show that the bone tissues have a lower maximum amplitude of measured light than the muscle (
Figure 7a,b). This was expected, as the higher amplitudes of ASWs from the bone might cause more distortion of the FBG, and more distortion creates more oscillation of the reflected light; thus, the measured reflected light intensity is low. The light intensity measured by the photodiode is reflected from the nonlinear regime of the near-Gaussian function (
Figure 3a,b). Thus, the reflected light intensity measured by the photodiode is inferior during the ablation of the bone compared to the ablation of the muscle, which is situated in the linear regime. We measured the stretch and compression of the fiber that is converted into the measured intensity in the time domain (in real-time with an up to sub-nanosecond resolution) of the back-reflected light from the FBG structure. Consequently, the intensity is proportional to the compression strain on the FBG that is caused by acoustic shock waves.
5. Conclusions
The long-pulsed (from 0.5 to 10 ms) laser ablation of bone at a wavelength of 1.07 µm in wet and dry conditions was the focus of this study. The acoustic shock wave characteristics of bone and muscle during a laser ablation were also investigated in an attempt to differentiate between tissues. The tissue ablated with a spray irrigation produced very few cracks and thermal damage around the craters, which would ultimately lead to accelerated bone healing. For the bone and muscle tissue differentiation, we focused on the acoustic signal measured at Set 5 (7 J and 4.55 ms), under wet conditions. At this specific pulse energy, the mean depth of the crater in bone, created under wet conditions, was higher than that created in dry conditions; we also observed a lower ablation volume for craters created under wet conditions, compared to dry conditions. In Set 5, the craters in bone were relatively clean of random charring and showed fewer cracks than he craters made in higher energy sets in either condition. Keeping the ablation volume as small as possible, with less thermal damage and fewer cracks, could potentially improve the ablation efficiency and bone healing time. Using the best laser parameters (Set 5) to generate acoustic waves for tissue differentiation, the peak amplitude of the acoustic signals measured by a microphone for the bone was higher than the ones for muscle, in both dry and wet conditions. The classification error of the experiment, based on the spectral acoustic wave detection of bone and muscle in wet conditions, was less than 6.66% and 3.33%, as measured by a microphone and by FBG, respectively. By quantifying the measured acoustic shock waves, we guarantee an efficient tissue differentiation as feedback to reduce the probability of undesirable cutting of tissues at different depths and pulse energies.
The promising results of this approach motivate us for further improvements. Future work will include a histological study of the bones in a cross-section after the laser ablation, in order to fully evaluate the potentials of the technique in terms of the reduction of bone damage compared to other techniques. Furthermore, the advanced precision in signal differentiation, combined with an extension of the number of involved tissues and ablating regimes, needs to be investigated. This formulation leads to more complex data, and in order to reach efficiency in processing we plan to involve a cutting-edge machine learning technique, simultaneously providing a high temporal resolution and real-time operation of the methods involved. The challenges in this formulation reside in the contradiction between computational complexity, computational speed, and precision. The solution to this problem is planned as the continuation of this work.

 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








