Comparison of Dental Stone Models and Their 3D Printed Acrylic Replicas for the Accuracy and Mechanical Properties

 ,
,  , ,
, , 

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Plaster Models
2.2. The Diagnostic Value of Plaster and Acrylic Models
2.3. Sample Preparation for Mechanical Testing
2.4. The Impact Strength Evaluation
2.5. The Shore D Hardness Test
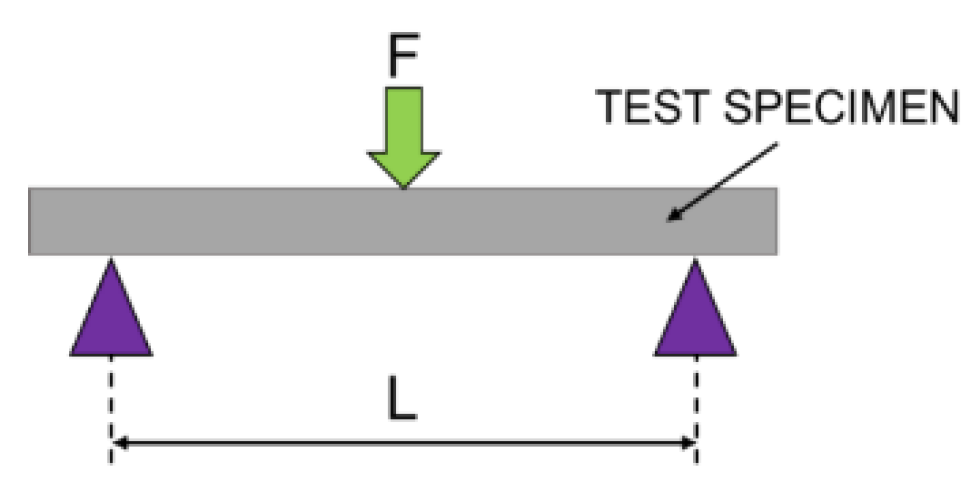
2.6. The Flexural Strength Evaluation
2.7. The Static Compression Test
2.8. Statistical Analysis
3. Results
3.1. The Diagnostic Value between Stone and Acrylic Models
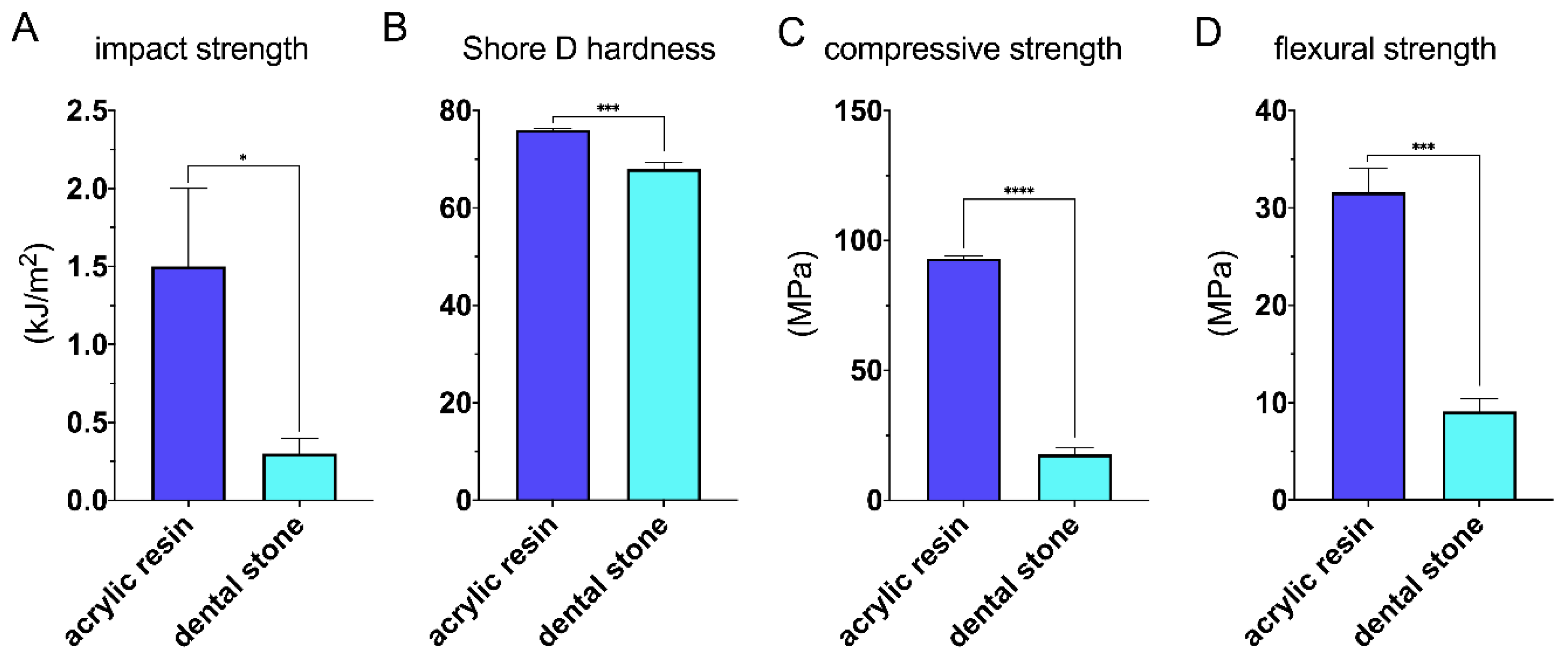
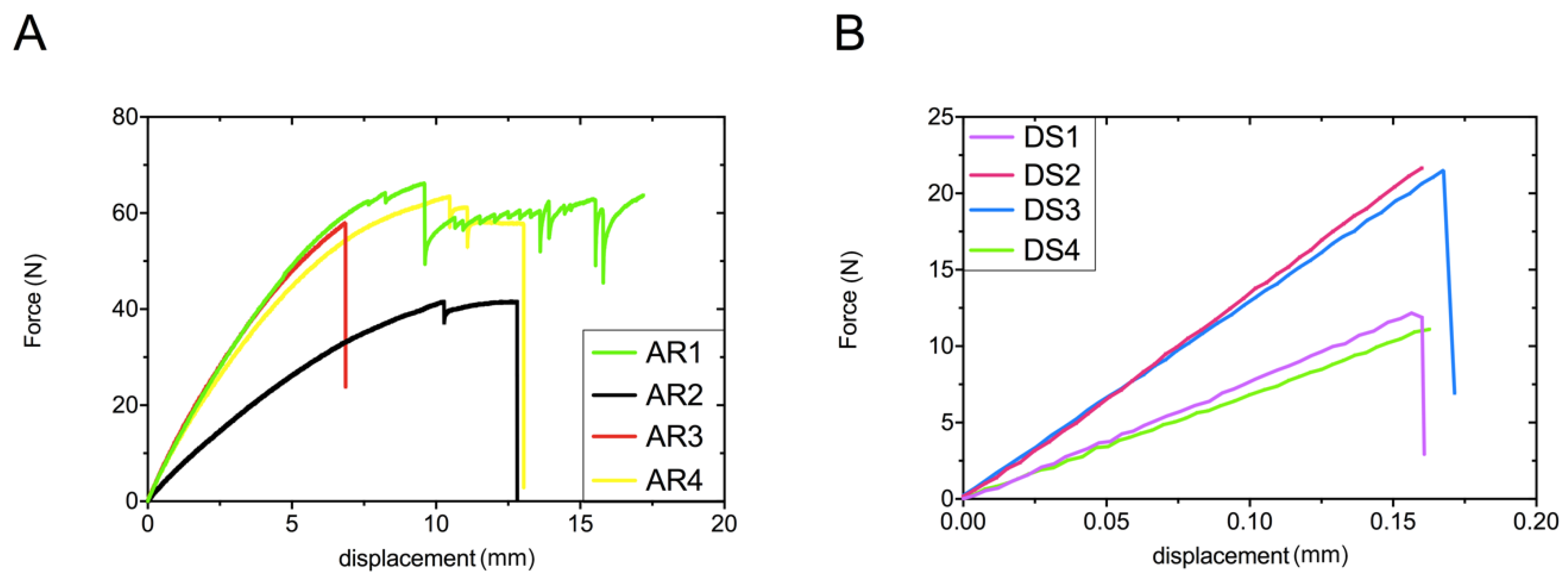
3.2. Mechanical Properties
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bolton, W.A. The clinical application of a tooth size analysis. Am. J. Orthod. 1962, 48, 504–529. [Google Scholar] [CrossRef]
- Martinson, B.; Ryden, H. The holodent system, a new technique for measurement and storage of dental casts. Am. J. Orthod. Dentofac. Orthop. 1992, 102, 113–119. [Google Scholar] [CrossRef]
- Rheude, B.; Sadowsky, P.L.; Ferriera, A.; Jacobson, A. An evaluation of the use of digital study models in orthodontic diagnosis and treatment planning. Angle Orthod. 2005, 75, 300–304. [Google Scholar] [PubMed]
- Ellis, P.E.; Benson, P.E. Does articulating study casts make a difference to treatment planning? J. Orthod. 2014, 30, 45–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romeo, A.; Canal, F.; Roma, M.; De la Higuera, B.; Ustrell, J.M.; Von Arx, J.D. Holograms in orthodontics: A universal system for the production, development, and illumination of holograms for storage and analysis of dental casts. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 443–447. [Google Scholar] [CrossRef]
- Kuroda, T.; Motohashi, N.; Tominaga, R.; Iwata, K. Three-dimensional dental cast analyzing system using laser scanning. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 365–369. [Google Scholar] [CrossRef]
- Santoro, M.; Galkin, S.; Teredesai, M.; Nicolay, O.; Cangialosi, T. Comparison of measurements made on digital and plaster models. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 101–105. [Google Scholar] [CrossRef]
- Phan, X.; Ling, P.H. Clinical limitations of Invisalign. J. Can. Dent. Assoc. 2007, 73, 263–266. [Google Scholar]
- Kravitz, N.D.; Kusnoto, B.; BeGole, E.; Obrez, A.; Agran, B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 27–35. [Google Scholar] [CrossRef]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef] [Green Version]
- Ko, H.C.; Liu, W.; Hou, D.; Torkan, S.; Spiekerman, C.; Huang, G.J. Recommendations for clear aligner therapy using digital or plaster study casts. Prog. Orthod. 2018, 19, 22. [Google Scholar] [CrossRef]
- Groth, C.; Kravitz, N.D.; Jones, P.E.; Graham, J.W.; Redmond, R. Three-dimensional printing technology. J. Clin. Orthod. 2014, 8, 475–485. [Google Scholar]
- PN-EN ISO 179-1:2010. Plastics—Determination of Charpy Impact Properties—Part 1: Non-Instrumented Impact Test; Polish Committee for Standardization: Warszawa, Poland, 2010. [Google Scholar]
- PN-EN ISO 178:2011. Plastics—Determination of Flexural Properties; Polish Committee for Standardization: Warszawa, Poland, 2011. [Google Scholar]
- PN-EN ISO 604:2006. Plastics—Determination of Compressive Properties; Polish Committee for Standardization: Warszawa, Poland, 2006. [Google Scholar]
- Azari, A.; Nikzad, S. The evolution of rapid prototyping in dentistry: A review. Rapid Prototyp. J. 2009, 15, 216–225. [Google Scholar] [CrossRef]
- Camardella, L.T.; De Vasconcellos Vilella, O.; Breuning, H. Accuracy of printed dental models made with 2 prototype technologies and different designs of model bases. Am. J. Orthod. Dentofac. Orthop. 2017, 6, 1178–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jindal, P.; Juneja, M.; Siena, F.L.; Bajaj, D.; Breedonb, P. Mechanical and geometric properties of thermoformed and 3D printed clear dental aligners. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 694–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rungrojwittayakul, O.; Kan, J.Y.; Shiozaki, K.; Rajesh, S.S.; Goodacre, B.J.; Lozada, J.L. Accuracy of 3D Printed Models Created by Two Technologies of Printers with Different Designs of Model Base. J. Prosthodont. 2020, 29, 124–128. [Google Scholar] [CrossRef]
- Rebong, R.E.; Stewart, K.T.; Utreja, A.; Ghoneima, A.A. Accuracy of three-dimensional dental resin models created by fused deposition modeling, stereolithography, and polyjet prototype technologies: A comparative study. Angle Orthod. 2018, 33, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Hazeveld, A.; Huddleston Slater, J.J.; Renc, Y. Accuracy and reproducibility of dental replica models reconstructed by different rapid prototyping techniques. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 108–115. [Google Scholar] [CrossRef]
- Lee, S.J.; Betensky, R.A.; Gianneschi, G.E.; Gallucci, G.O. Accuracy of digital versus conventional implant impressions. Clin. Oral. Implant. Res. 2015, 26, 715–719. [Google Scholar] [CrossRef]
- Favero, C.S.; English, J.D.; Cozad, B.E.; Wirthlin, J.O.; Short, M.M.; Kasper, F.K. Effect of print layer height and printer type on the accuracy of 3-dimensional printed orthodontic models. Am. J. Orthod. Dentofac. Orthop. 2017, 4, 557–565. [Google Scholar] [CrossRef] [Green Version]
- Nam, S.E.; Park, Y.S.; Lee, W.; Ahn, S.J.; Lee, S.P. Making three-dimensional Monson’s sphere using virtual dental models. J. Dent. 2013, 41, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Babu, K.S.; Kumar, A.N.; Kommi, P.B.; Krishnan, P.H.; Kumar, M.S.; Sabapathy, R.S.; Kumar, V.V. Evaluating the correlation between anteroposterior and mediolateral compensatory curves and their influence on dentoskeletal morphology—An in vitro CBCT study. J. Clin. Diagn. Res. 2017, 11, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Ledingham, A.D.; English, J.D.; Akyalcin, S.; Cozad, B.E.; Ontiveros, J.C.; Kurtis Kasper, F. Accuracy and mechanical properties of orthodontic models printed 3-dimensionally from calcium sulfate before and after various postprinting treatments. Am. J. Orthod. Dentofac. Orthop. 2016, 6, 1056–1062. [Google Scholar] [CrossRef]
- Mangano, F.G.; Admakin, O.; Bonacina, M.; Biaggini, F.; Farronato, D.; Lerner, H. Accuracy of 6 Desktop 3D Printers in Dentistry: A Comparative In Vitro Study. Eur. J. Prosthodont. Restor. Dent. 2020, 28, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Park, G.S.; Kim, S.K.; Heo, S.J.; Koak, J.Y.; Seo, D.G. Efects of printing parameters on the fit of implant-supported 3D printing resin prosthetics. Materials 2019, 12, 2533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.W.; Ahn, J.J.; Son, K.; Huh, J.B. Three-dimensional evaluation on accuracy of conventional and milled gypsum models and 3D printed photopolymer models. Materials 2019, 12, 3499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quan, H.; Zhang, T.; Xu, H.; Luo, S.; Nie, J.; Zhu, X. Photo-curing 3D printing technique and its challenges. J. Bioactmat. 2020, 5, 110–115. [Google Scholar] [CrossRef]
- Gao, Y.; Xu, L.; Zhao, Y.; Guan, Q. 3D printing preview for stereo-lithography based on photopolymerization kinetic models. J. Bioactmat. 2020, 4, 798–807. [Google Scholar] [CrossRef]
- Kadry, H.; Wadnap, S.; Xu, C.; Ahsan, F. Digital light processing (DLP) 3D-printing technology and photoreactive polymers in fabrication of modified-release tablets. Eur. J. Pharm. Sci. 2019, 135, 60–67. [Google Scholar] [CrossRef]
- Joda, T.; Matthisson, L.; Zitman, N.U. Impact of aging on the accuracy of 3D-printed dental models: An in vitro investigation. J. Clin. Med. 2020, 9, 1436. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Manufacturer |
|---|---|
| Chromatic alginate (class-a, type 1) | Kromopan USA Inc., Morton Grove, IL, USA |
| Elite HD + putty soft silicone | Zhermack SpA, Badia Polesine, Italy |
| Type 3 stone | Zhermack SpA, Badia Polesine, Italy |
| Modified acrylic resin | EnvisionTEC Inc., Dearborn, MI, USA |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czajkowska, M.; Walejewska, E.; Zadrożny, Ł.; Wieczorek, M.; Święszkowski, W.; Wagner, L.; Mijiritsky, E.; Markowski, J. Comparison of Dental Stone Models and Their 3D Printed Acrylic Replicas for the Accuracy and Mechanical Properties. Materials 2020, 13, 4066. https://doi.org/10.3390/ma13184066
Czajkowska M, Walejewska E, Zadrożny Ł, Wieczorek M, Święszkowski W, Wagner L, Mijiritsky E, Markowski J. Comparison of Dental Stone Models and Their 3D Printed Acrylic Replicas for the Accuracy and Mechanical Properties. Materials. 2020; 13(18):4066. https://doi.org/10.3390/ma13184066
Chicago/Turabian StyleCzajkowska, Marta, Ewa Walejewska, Łukasz Zadrożny, Monika Wieczorek, Wojciech Święszkowski, Leopold Wagner, Eitan Mijiritsky, and Jarosław Markowski. 2020. "Comparison of Dental Stone Models and Their 3D Printed Acrylic Replicas for the Accuracy and Mechanical Properties" Materials 13, no. 18: 4066. https://doi.org/10.3390/ma13184066
APA StyleCzajkowska, M., Walejewska, E., Zadrożny, Ł., Wieczorek, M., Święszkowski, W., Wagner, L., Mijiritsky, E., & Markowski, J. (2020). Comparison of Dental Stone Models and Their 3D Printed Acrylic Replicas for the Accuracy and Mechanical Properties. Materials, 13(18), 4066. https://doi.org/10.3390/ma13184066