Evaluation of New Octacalcium Phosphate-Coated Xenograft in Rats Calvarial Defect Model on Bone Regeneration

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Animals
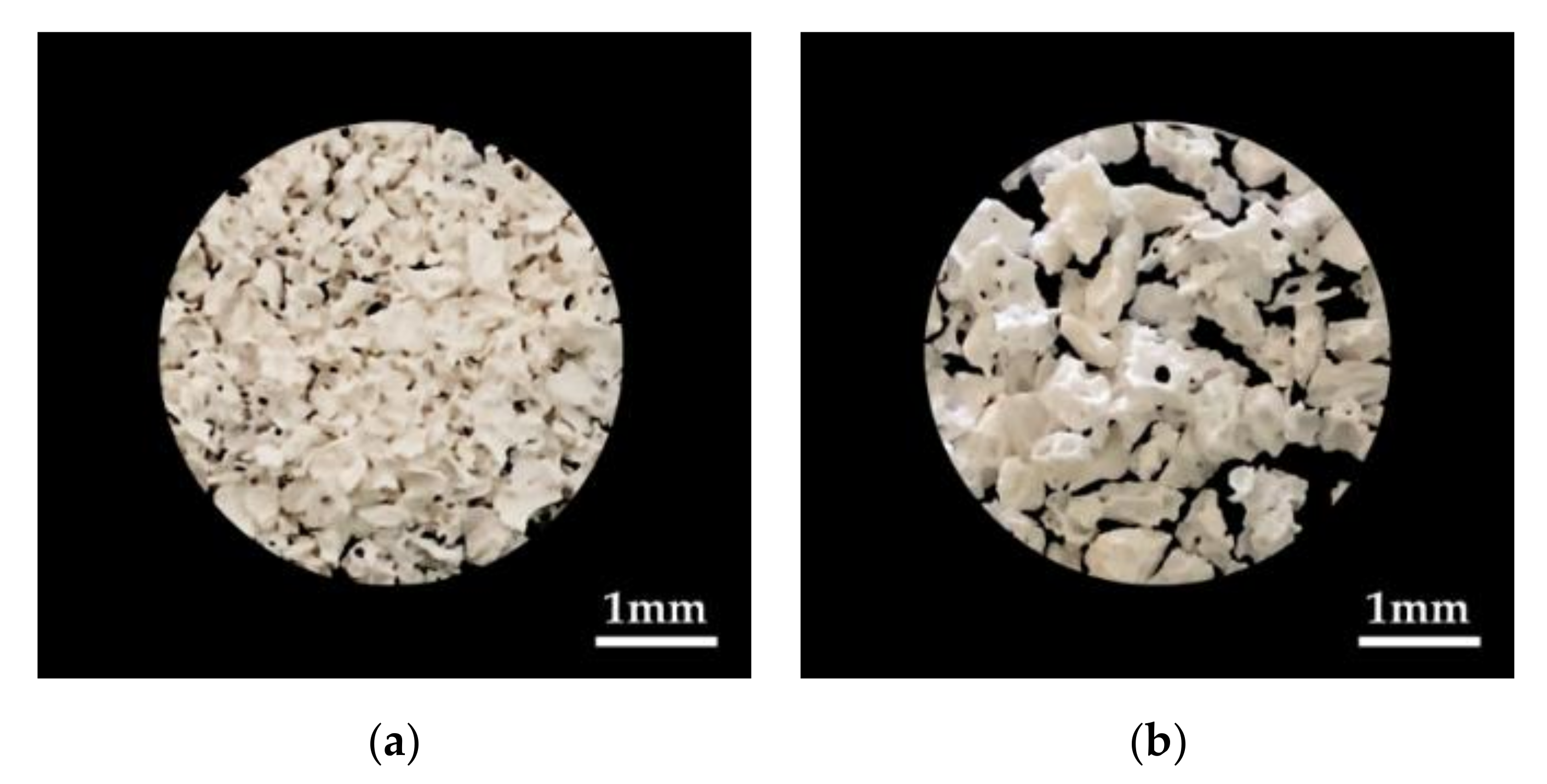
2.2. Specimen Preparation
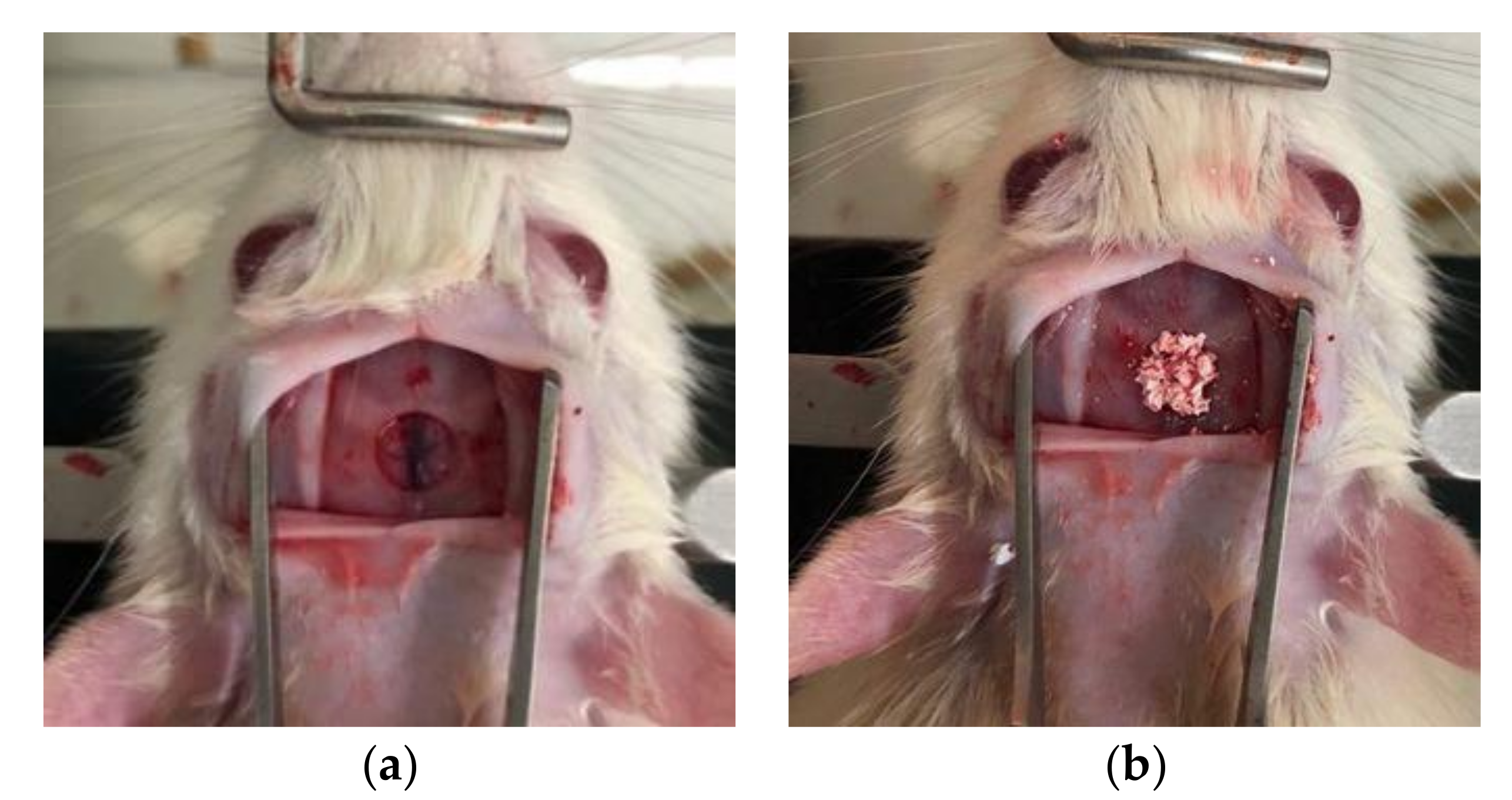
2.3. Surgical Procedures
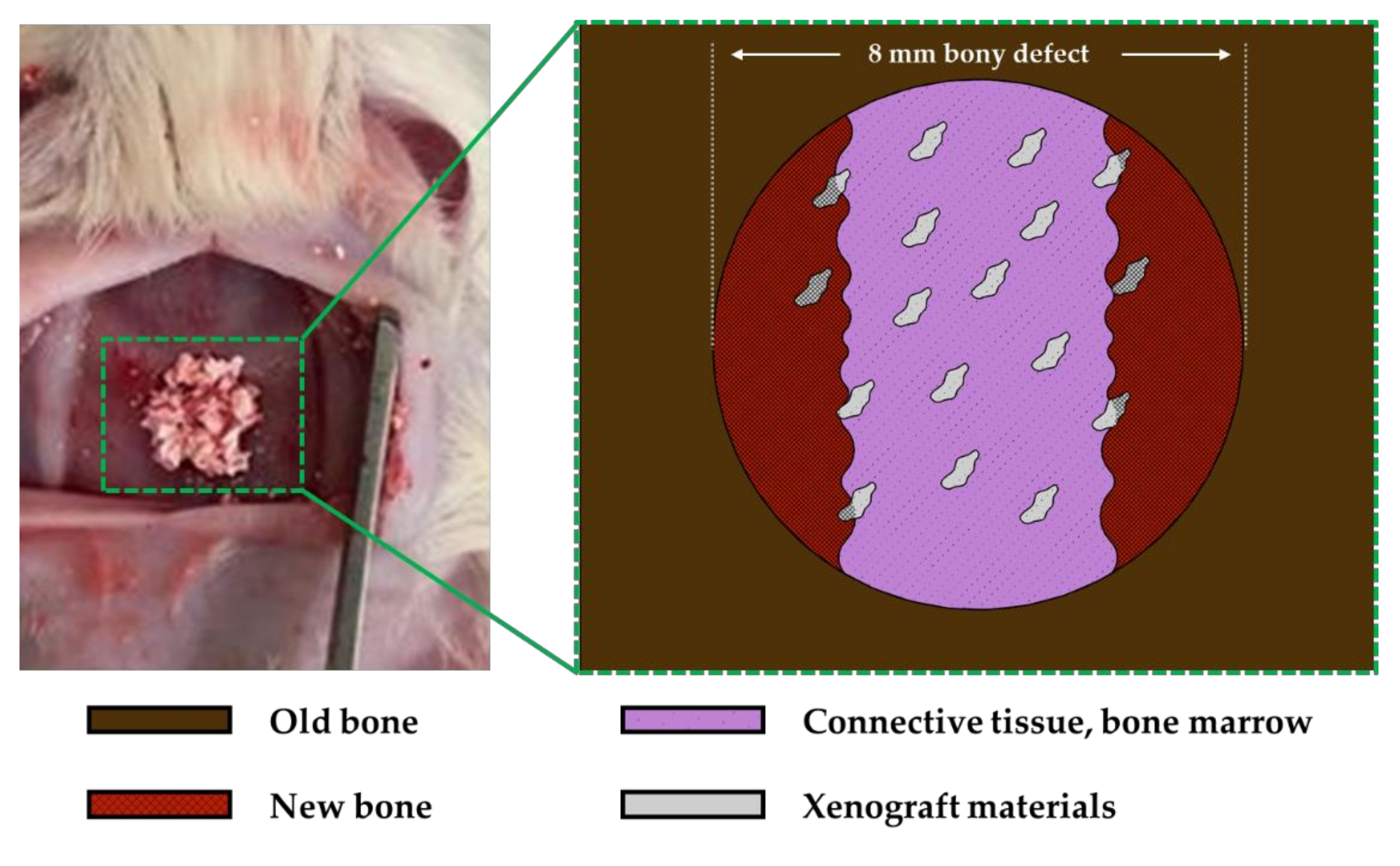
2.4. Specimen Preparation and Histomorphormetric Analysis
2.5. Statistical Analysis
3. Results
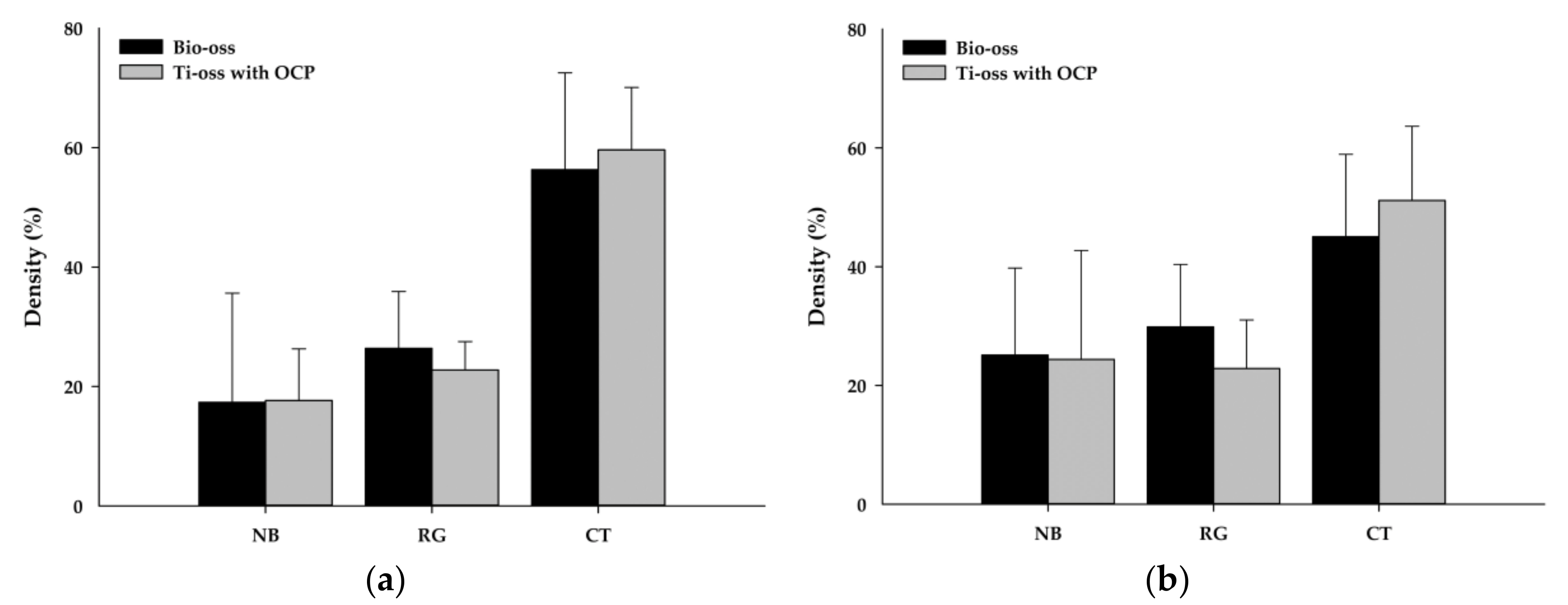
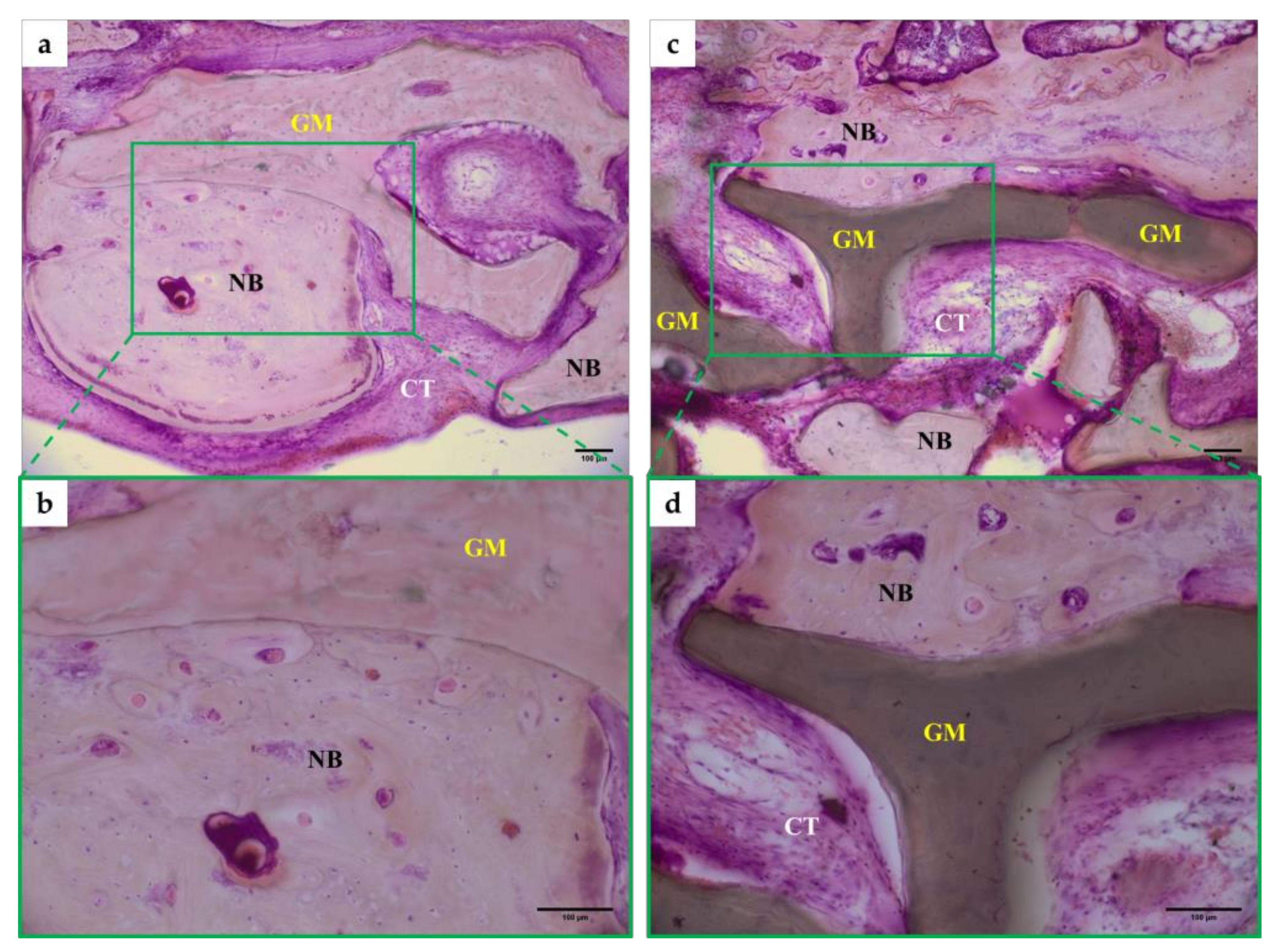
Tissue Morphology Analysis Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Boyce, T.; Edwards, J.; Scarborough, N. Allograft bone. The influence of processing on safety and performance. Orthop. Clin. North. Am. 1999, 30, 571–581. [Google Scholar] [CrossRef]
- Hollinger, J.O.; Kleinschmidt, J.C. The critical size defect as an experimental model to test bone repair materials. J. Craniofac. Surg. 1990, 1, 60–68. [Google Scholar] [CrossRef]
- Spicer, P.P.; Kretlow, J.D.; Young, S.; Jansen, J.A.; Kasper, F.K.; Mikos, A.G. Evaluation of bone regeneration using the rat critical size calvarial defect. Nat. Protoc. 2012, 7, 1918–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wetzel, A.C.; Stich, H.; Caffesse, R.G. Bone apposition onto oral implants in the sinus area filled with different grafting materials. A histological study in beagle dogs. Clin. Oral Implants Res. 1995, 6, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Klinge, B.; Alberius, P.; Isaksson, S.; Jönsson, J. Osseous response to implanted natural bone mineral and synthetic hydroxylapatite ceramic in the repair of experimental skull bone defects. J. Oral Maxillofac. Surg. 1992, 50, 241–249. [Google Scholar] [CrossRef]
- Froum, S.J.; Wallace, S.S.; Elian, N.; Cho, S.C.; Tarnow, D.P. Comparison of mineralized cancellous bone allograft (Puros) and anorganic bovine bone matrix (Bio-Oss) for sinus augmentation: Histomorphometry at 26 to 32 weeks after grafting. Int. J. Periodontics Restor. Dent. 2006, 26, 543–551. [Google Scholar]
- Skoglund, A.; Hising, P.; Young, C. A clinical and histologic examination in humans of the osseous response to implanted natural bone mineral. Int. J. Oral Maxillofac. Implants 1997, 12, 194–199. [Google Scholar]
- Piattelli, M.; Favero, G.A.; Scarano, A.; Orsini, G.; Piattelli, A. Bone reactions to anorganic bovine bone (Bio-Oss) used in sinus augmentation procedures: A histologic long-term report of 20 cases in humans. Int. J. Oral Maxillofac. Implants 1999, 14, 835–840. [Google Scholar]
- Zhao, H.; Hu, J.; Zhao, L. Histological analysis of socket preservation using DBBM. A systematic review and meta-analysis. J. Stomatol. Oral Maxillofac. Surg. 2020, 30093–30098. [Google Scholar] [CrossRef]
- Kim, H.-W. Recent research and development status of biomaterials for bone regeneration and tissue engineering. J. Korean Dent. Assoc. 2006, 44, 534–555. [Google Scholar]
- Brown, W.E. Crystal growth of bone mineral. Clin. Orthop. Relat. Res. 1966, 44, 205–220. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.E.; Smith, J.P.; Lehr, J.R.; Frazier, A.W. Octacalcium Phosphate and Hydroxyapatite: Crystallographic and Chemical Relations between Octacalcium Phosphate and Hydroxyapatite. Nature 1962, 196, 1050–1055. [Google Scholar] [CrossRef]
- Barradas, A.M.; Yuan, H.; van Blitterswijk, C.A.; Habibovic, P. Osteoinductive biomaterials: Current knowledge of properties, experimental models and biological mechanisms. Eur. Cell Mater. 2011, 21, 407–429. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, J.H.; Jeon, J.H. Bone regeneration of macropore octacalcium phosphate-coated deproteinized bovine bone materials in sinus augmentation: A prospective pilot study. Implant Dent. 2015, 24, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Sasano, Y.; Kamakura, S.; Homma, H.; Suzuki, O.; Mizoguchi, I.; Kagayama, M. Implanted octacalcium phosphate (OCP) stimulates osteogenesis by osteoblastic cells and/or committed osteoprogenitors in rat calvarial periosteum. Anat. Rec. 1999, 256, 1–6. [Google Scholar] [CrossRef]
- Suzuki, Y.; Kamakura, S.; Honda, Y.; Anada, T.; Hatori, K.; Sasaki, K.; Suzuki, O. Appositional bone formation by OCP-collagen composite. J. Dent. Res. 2009, 88, 1107–1112. [Google Scholar] [CrossRef]
- Habibovic, P.; Li, J.; Van Der Valk, C.M.; Meijer, G.; Layrolle, P.; Van Blitterswijk, C.A.; De Groot, K. Biological performance of uncoated and octacalcium phosphate-coated Ti6Al4V. Biomaterials 2005, 26, 23–36. [Google Scholar] [CrossRef]
- Suzuki, O.; Imaizumi, H.; Kamakura, S.; Katagiri, T. Bone regeneration by synthetic octacalcium phosphate and its role in biological mineralization. Curr. Med. Chem. 2008, 15, 305–313. [Google Scholar] [CrossRef]
- LeGeros, R.Z. Preparation of octacalcium phosphate (OCP): A direct fast method. Calcif. Tissue Int. 1985, 37, 194–197. [Google Scholar] [CrossRef]
- Ekaterina, K.; Kim, Y.; Kim, J.-Y.; Kim, M.-R.; Kim, S.O.; Kim, S.-J. Histomorphometric study on healing of critical sized defect in rat calvaria using tree different bovine grafts. Tissue Eng. Regener. Med. 2012, 9, 276–281. [Google Scholar] [CrossRef]
- Tencer, A.F.; Woodard, P.L.; Swenson, J.; Brown, K.L. Mechanical and bone ingrowth properties of a polymer-coated, porous, synthetic, coralline hydroxyapatite bone-graft material. Ann. N. Y. Acad. Sci. 1988, 523, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Mellonig, J.T.; Bowers, G.M.; Cotton, W.R. Comparison of bone graft materials. Part II. New bone formation with autografts and allografts: A histological evaluation. J. Periodontol. 1981, 52, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Ryu, M.Y.; Baek, H.R.; Lee, K.M.; Seo, J.H.; Lee, H.K. Fabrication and evaluation of porous beta-tricalcium phosphate/hydroxyapatite (60/40) composite as a bone graft extender using rat calvarial bone defect model. Sci. World J. 2013, 481789. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.-S.; Bae, J.-H.; Kim, S.-E.; Bae, E.-B.; Kim, S.-Y.; Choi, K.-H.; Moon, K.-O.; Jeong, C.-M.; Huh, J.-B. The Effect of Bisphasic Calcium Phosphate Block Bone Graft Materials with Polysaccharides on Bone Regeneration. Materials 2017, 10, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charan, J.; Kantharia, N.D. How to calculate sample size in animal studies? J. Pharmacol. Pharmacother. 2013, 4, 303–306. [Google Scholar] [CrossRef] [Green Version]
- Kempen, D.H.; Lu, L.; Heijink, A.; Hefferan, T.E.; Creemers, L.B.; Maran, A.; Yaszemski, M.J.; Dhert, W.J. Effect of local sequential VEGF and BMP-2 delivery on ectopic and orthotopic bone regeneration. Biomaterials 2009, 30, 2816–2825. [Google Scholar] [CrossRef]
- Takagi, K.; Urist, M.R. The reaction of the dura to bone morphogenetic protein (BMP) in repair of skull defects. Ann. Surg. 1982, 196, 100–109. [Google Scholar] [CrossRef]
- Schmitz, J.P.; Hollinger, J.O. The critical size defect as an experimental model for craniomandibulofacial nonunions. Clin. Orthop. Relat. Res. 1986, 205, 299–308. [Google Scholar] [CrossRef]
- Yildirim, M.; Spiekermann, H.; Biesterfeld, S.; Edelhoff, D. Maxillary sinus augmentation using xenogenic bone substitute material Bio-Oss in combination with venous blood. A histologic and histomorphometric study in humans. Clin. Oral Implants Res. 2000, 11, 217–229. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.-M. Biocompatibility of bone substitutes. J. Kor. Dent. Assoc. 2006, 44, 556–560. [Google Scholar]
- Kim, Y.-K.; Kim, S.-G.; Lim, S.-C. The comparative study of guided bone regeneration using various of bone graft materials. J. Kor. Oral Maxillofac. Surg. 2007, 33, 350–358. [Google Scholar]
- Rokn, A.R.; Khodadoostan, M.A.; Reza Rasouli Ghahroudi, A.A.; Motahhary, P.; Kharrazi Fard, M.J.; Bruyn, H.D.; Afzalifar, R.; Soolar, E.; Soolari, A. Bone formation with two types of grafting materials: A histologic and histomorphometric study. Open Dent. J. 2011, 5, 96–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takauti, C.A.; Futema, F.; Brito, R.B.J.; Abrahão, A.C.; Costa, C.; Queiroz, C.S. Assessment of bone healing in rabbit calvaria grafted with three different biomaterials. Braz. Dent. J. 2014, 25, 379–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, O. Octacalcium phosphate (OCP)-based bone substitute materials. Jpn. Dent. Sci. Rev. 2013, 49, 58–271. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.-S.; Tsuang, Y.-H.; Li, J.; Liu, H.-C.; Lin, F.-H. Effect of hydroxyapatite particle size on myoblasts and fibroblasts. Biomaterials 1997, 18, 683–690. [Google Scholar] [CrossRef]
- Beuvelot, J.; Pascaretti-Grizon, F.; Filmon, R.; Moreau, M.F.; Basle, M.F.; Chappard, D. In vitro assessment of osteoblast and macrophage mobility in presence of beta-TCP particles by videomicroscopy. J Biomed. Mater. Re.s A 2010, 96, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Lu, Z.; Zreiqat, H. Beta-tricalcium phosphate exerts osteocon-ductivity through alpha2beta1 integrin and down-stream MAPK/ERK signaling pathway. Biochem. Biophys. Res. Commun. 2010, 394, 323–329. [Google Scholar] [CrossRef]
- Honda, Y.; Anada, T.; Kamakura, S.; Morimoto, S.; Kuriyagawa, T.; Suzuki, O. The effect of microstructure of octacalcium phosphate on the bone regenerative property. Tissue Eng. Part A 2009, 15, 1965–1973. [Google Scholar] [CrossRef]
- Ban, S.; Jinde, T.; Hasegawa, J. Phase transformation of octacalcium phosphate in vivo and in vitro. Dent. Mater. J. 1992, 11, 130–140. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, O.; Kamakura, S.; Katagiri, T.; Nakamura, M.; Zhao, B.; Honda, Y.; Kamijo, R. Bone formation enhanced by implanted octacalcium phosphate involving conversion into Ca-deficient hydroxyapatite. Biomaterials 2006, 27, 2671–2681. [Google Scholar] [CrossRef]
- Suzuki, O.; Nakamura, M.; Miyasaka, Y.; Kagayama, M.; Sakurai, M. Bone formation on synthetic precursors of hydroxyapatite. Tohoku J. Exp. Med. 1991, 164, 37–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, O.; Nakamura, M.; Miyasaka, Y.; Kagayama, M.; Sakurai, M. Maclura pomifera agglutinin-binding glycoconjugates on converted apatite from synthetic octacalcium phosphate implanted into subperiosteal region of mouse calvaria. Bone Miner. 1993, 20, 151–166. [Google Scholar] [CrossRef]
- Suzuki, O.; Kamakura, S.; Katagiri, T. Surface chemistry and biological responses to synthetic octacalcium phosphate. J. Biomed. Mater. Res. B Appl. Biomater. 2006, 77, 201–212. [Google Scholar] [CrossRef]
- Mura-Galelli, M.J.; Narusawa, H.; Shimada, T.; Iijima, M.; Aoba, T. Effects of fluoride on precipitation and hydrolysis of octacalcium phosphate in an experimental model simulating enamel mineralization during amelogenesis. Cells Mater. 1992, 2, 221–230. [Google Scholar]
- Kaneko, H.; Kamiie, J.; Kawakami, H.; Anada, T.; Honda, Y.; Shiraishi, N.; Kamakura, S.; Terasaki, T.; Shimauchi, H.; Suzuki, O. Proteome analysis of rat serum proteins adsorbed onto synthetic octacalcium phosphate crystals. Anal. Biochem. 2011, 418, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T.; Nishimura, I. Genes differentially expressed in titanium implant healing. J. Dent. Res. 2006, 85, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Honda, Y.; Anada, T.; Handa, T.; Miyatake, N.; Takahashi, A.; Hosaka, M.; Imaizumi, H.; Itoi, E.; Suzuki, O. Stimulatory capacity of an octacalcium phosphate/ gelatin composite on bone regeneration. Phosphor Res. Bull. 2012, 26, 53–58. [Google Scholar] [CrossRef]
- Handa, T.; Anada, T.; Honda, Y.; Yamazaki, H.; Kobayashi, K.; Kanda, N.; Kamakura, S.; Echigo, S.; Suzuki, O. The effect of an octacalcium phosphate co-precipitated gelatin composite on the repair of critical-sized rat calvarial defects. Acta Biomater. 2012, 8, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Kim, R.W.; Kim, J.H.; Moon, S.Y. Effect of hydroxyapatite on critical-sized defect. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Kikawa, T.; Kashimoto, O.; Imaizumi, H.; Kokubun, S.; Suzuki, O. Intramembranous bone tissue response to biodegradable octa-calcium phosphate implant. Acta Biomater. 2009, 5, 1756–1766. [Google Scholar] [CrossRef]
- Sugihara, F.; Onishi, H.; Kushitani, S.; Iwaki, N.; Mandai, Y.; Minami-gawa, K. Bone tissue reaction of octacalcium phosphate. Bioceramics 1995, 8, 89–91. [Google Scholar]
- Barrere, F.; Van Der Valk, C.M.; Dalmeijer, R.A.J.; Van Blitterswijk, C.A.; De Groot, K.; Layrolle, P. In vitro and in vivo degradation of biomimetic octacalcium phosphate and carbonate apatite coatings on titanium implants. J. Biomed. Mater. Res. A 2003, 64, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Honda, Y.; Anada, T.; Shimauchi, H.; Suzuki, O. Comparative study on bone regeneration by synthetic octacalcium phosphate with various granule sizes. Acta Biomater. 2010, 6, 1542–1548. [Google Scholar] [CrossRef] [PubMed]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, Y.; Kim, W.-H.; Lee, S.-H.; Ju, K.W.; Jang, E.-H.; Kim, S.-O.; Kim, B.; Lee, J.-H. Evaluation of New Octacalcium Phosphate-Coated Xenograft in Rats Calvarial Defect Model on Bone Regeneration. Materials 2020, 13, 4391. https://doi.org/10.3390/ma13194391
Jung Y, Kim W-H, Lee S-H, Ju KW, Jang E-H, Kim S-O, Kim B, Lee J-H. Evaluation of New Octacalcium Phosphate-Coated Xenograft in Rats Calvarial Defect Model on Bone Regeneration. Materials. 2020; 13(19):4391. https://doi.org/10.3390/ma13194391
Chicago/Turabian StyleJung, Yoona, Won-Hyeon Kim, Sung-Ho Lee, Kyung Won Ju, Eun-Hee Jang, Sung-O Kim, Bongju Kim, and Jong-Ho Lee. 2020. "Evaluation of New Octacalcium Phosphate-Coated Xenograft in Rats Calvarial Defect Model on Bone Regeneration" Materials 13, no. 19: 4391. https://doi.org/10.3390/ma13194391
APA StyleJung, Y., Kim, W. -H., Lee, S. -H., Ju, K. W., Jang, E. -H., Kim, S. -O., Kim, B., & Lee, J. -H. (2020). Evaluation of New Octacalcium Phosphate-Coated Xenograft in Rats Calvarial Defect Model on Bone Regeneration. Materials, 13(19), 4391. https://doi.org/10.3390/ma13194391