3.4.1. Unit Cell Geometry
Metamaterials can be rationally designed by changing their geometry at the microscale of the constituting unit cells of the porous structure. In this systematic search, a total of 169 porous scaffolds were identified as a rationally designed and fabricated for bone implant applications. It was found that there are three preferred strategies for fabricating bio-metamaterials: beam-based, sheet-based, and including irregular porous structures [
172].
According to
Figure 6, the preferred design approach was beam-based, which represent 74.6% of the total scaffolds produced in the selected studies. The beam-based bio-metamaterials’ micro-architecture is composed of a lattice structure created using unit cells based on platonic solids, Archimedean solids, prisms and anti-prisms, and Archimedean duals [
173,
174,
175,
176,
177] to mimic bone porous macro structure and mechanical properties such as modulus of elasticity. Nevertheless, the biological performance of bio-metamaterials created with beam-based geometries is limited by their inaccurate description of complex natural shapes due to their straight edges and sharp turns [
109].
The unit cells of sheet-based geometries, on the other hand, are based on triply periodic minimal surfaces (TPMS), which are present in different organisms and cellular structures [
178]. Therefore, it is no surprising that the second most used design strategy identified in this systematic search was sheet-based representing 20.1% of the total scaffolds produced, from which all used a TPMS as unit cell. Bio-metamaterials based on TPMS can mimic the various properties of bone to an unprecedented level of multi-physics detail in terms of mechanical properties and transport properties [
79,
172]. Moreover, the bone-mimicking mean surface curvature of zero of TPMS eliminates the effect of stress concentrators at nodal points [
120].
In the case of irregular porous structures, are created in a random way to generate irregular porous structures that mimic trabecular bone geometry and mechanical properties [
179]. These irregular structures are generated using the Voronoi and Delaunay tessellation methods. Irregular structures have been found to further enhance scaffold’s permeability and bone ingrowth compared with porous structures designed with regular unit cells [
180]. According to our results only 5.3% of the studies used a randomised design approach to create irregular porous structures to mimic trabecular bone. This result was surprising considering that irregular porous structures were the first additively manufactured coatings used for orthopaedic implants in the medical industry. However, unlike random porous scaffolds, the great advantage of using regular repeating arrays of unit cells made of beam or sheet-based geometries is that they allow the creation of metamaterials with properties that can accurately be predicted [
181]. This explain why these design strategies are preferred in research.
From all the different possible unit cells that can be used to produce metamaterials, a total of 17 types of unit cell were used by the selected studies, as presented in
Figure 7. According to
Figure 7, the beam-based diamond unit cell (59 studies) was the most used, followed by the cubic (18 studies), and the gyroid TPMS (17 studies). These results correlate with the opinion of different experts who have stated that the diamond unit cell is the most studied for the development of metamaterials due to its biomimetic mechanical properties [
121,
182]. The high mechanical properties and self-supporting properties of the diamond unit cell are due to its unique geometrical arrangement, where one node is tetrahedrally surrounded by four other nodes coming from the crystal structure of the diamond crystal [
113], as shown in
Figure 8a. Moreover, this arrangement gives 48 symmetry elements to the diamond structure, making this unit cell invariant to different symmetry operations such as translations, reflections, rotations, and inversion [
183]. Similarly, extensive research for bone regeneration has been performed to study the cubic unit cell (
Figure 8b). The research interest in the cubic unit cell is because it is based on one of the simplest and easy–to–manufacture platonic solids thanks to its struts at an angle of 90° [
62]. In the case of porous metamaterials based on the gyroid TPMS (
Figure 8c), they have been found to exhibit similar topology to human trabecular bone, and also superior mechanical properties compared with metamaterials based on other types of TPMS [
120]. For example, according to Yang et al. [
184] metamaterials based on the gyroid TPMS have a more homogeneous stress distribution, which can provide equal mechanical stimulation to bone cells.
In the case of random or stochastic structures, Kou et al. [
185] suggested that scaffolds based on this structures are more realistic; that is, they look more like natural bone with random non-uniform pore distribution and pore size [
185]. Such structures are believed to provide benefits such as improved mechanical properties, including strength, fluid dynamics, surface area, and surface-to-weight ratio. They combine advantages of small and large pores without necessarily decreasing the mechanical strength or reducing the bone in-growth to levels that are inappropriate in application [
186].
Figure 8 presents the five most representative unit cells identified in this study.
3.4.2. Porosity
It is known that the degree of micro-porosity in bone implants directly affects their biological and mechanical properties. The porosity of natural bone is crucial for vascularisation, diffusion of cell nutrients and metabolic waste, and cell migration [
187], and in a similar way it is important for metal bone implants. Moreover, several studies have considered porosity as the main parameter affecting stiffness and strength of porous biomaterials. Increased porosity reduces the strength of the implant [
187,
188]. As a result, porous metallic biomaterials are used as coatings in many medical applications, but more recently porous biomaterials have been proposed for load-bearing applications beyond surface coatings [
138,
142]. Ti and Ti alloys are commonly used for load-bearing implant applications due to their relatively low elastic modulus fatigue resistance, high strength to weight ratio, and corrosion resistance [
82,
94]. However, bulk Ti and Ti alloys do not completely match all the mechanical properties of natural bone such as modulus of elasticity. Therefore, it is a need of the hour to accomplish specific mechanical properties for Ti or Ti-based alloys by controlling the porosity and pore characteristics for customised implants [
131]. However, the ideal porosity for medical implants seems controversial in the literature [
181].
In this systematic review a total of 49 articles out of 50 recorded porosity of various degrees, as shown in
Figure 9. For example, Stamp et al. [
186] recommend using a porosity above 65% in medical implants whereas Ghanaati et al. [
189] found that vascularisation increased in vivo when reducing the porosity from 80 to 40%. Sarhadi et al. [
190] and Schiefer et al. [
191] have recommended using a porosity of approximately 50%. According to Will et al. [
192], the porosity that best promotes vascularization in porous scaffolds is 40–60%. Pattanayak et al. [
193] manufactured porous Ti implants and reported an increase in compressive strength from 35 MPa to 120 MPa when reducing the porosity from 75 to 55%. Murr et al. reduced the porosity from 88 to 59% with an increase in stiffness from 0.58 GPa to 1.03 GPa [
131]. As mentioned, natural cancellous bone has a porosity of 50–90% [
85,
86].
Zou et al. [
102] designed three implants with similar pore size and shape. By reducing the porosity from 72 to 53% they achieved a compressive strength of 200 MPa and Young’s modulus of 4.3 GPa, instead of a compressive strength of 60 MPa and Young’s modulus of 2 GPa. Even though both implants achieved a stiffness close to that of human bone, only the implant with 53% porosity achieved a compressive strength greater than human bone. Hence, the implant with 72% porosity would not qualify as a load-bearing bone implant. These results, along with previous research by Pattanyak et al. and Murr et al., confirm the influence of porosity on mechanical properties [
193]. They also show that the implant porosity may be adjusted within limits to increase strength and adjust bone stiffness, which varies for each patient’s characteristics.
From a medical regulatory perspective, the U.S Food and Drug Administration (FDA) only approves implant porosities of 30–70% for porous coatings on solid Ti implants [
194]. The range is relatively large but can be used to one’s advantage since both the elastic modulus and strength of the implant can be adjusted by adjusting the porosity. Implants with porosity outside of this range do not comply with FDA regulations and cannot enter the market. It is known that medical regulations, especially for implantable medical devices, are based on strong scientific evidence. Therefore, it is vital to adhere to these regulations when designing bone implants.
Taking into consideration the medical regulations for porous implants, we selected a porosity range of 30–70% as the IQA for porous metal implants to identify studies in the systematic search that fabricated Ti scaffolds with porosity values within this range. From the 49 articles that recorded porosity of various degrees, a total of 167 results were extracted and compared with the selected IQA porosity range. The results of this comparison are presented in
Figure 9. According to our results, 56.6% of the porous scaffolds studied in the 49 selected articles had porosity values within the acceptable porosity range (30–70%) required to satisfy medical regulations such as the FDA. By contrast, a total of 26 studies explored the properties of porous scaffolds with porosity values above the acceptable porosity range representing 37.3% of the total results extracted in this systematic literature review. There were several reasons for these studies to explore porosity levels higher than 70%. For example, Zhang et al. [
100] and Amin Yavari et al. [
106] fabricated different porous structures with various porosities to explore their mechanical properties and deformation mechanisms. Moreover, porous Ti scaffolds with high levels of porosity can serve as storage for mesenchymal stem cells to facilitate bone tissue regrowth, and also to improve cell oxygenation and nutrition [
100]. On the other hand, Ti porous scaffolds with porosity levels lower than 30% can provide similar mechanical properties to cortical bone [
98,
100].
3.4.3. Macropore Size
Since macro pore size is directly related to the strength, porosity, and stiffness of the implant, it is an important property for implant design [
195]. Pore size has a profound effect on the behaviour of osteogenic cells even in an organ culture system [
196]. The implant’s macro porosity determines whether bone cells can successfully penetrate and grow within the structure, and many studies have discussed the influence of pore size on the biological properties of implants [
197]. Furthermore, several studies have shown that a minimum pore size of 100 µm is required for vascularization and bone ingrowth, but pores larger than 100 µm increase bone in-growth by allowing improved vascularization and oxygenation [
86,
91,
193]. A minimum macropore size limit of 100 µm is supported by further research as vascular penetration has been found to be restricted in smaller pore interconnections [
85,
168,
188,
192].
Studies have found that pores greater than 300 µm are required for vascularisation and bone ingrowth [
86,
168]. Tang et al. [
188] found that 200–350 µm is the optimal macropore size, and various studies have found that bone ingrowth is less likely to occur beyond 400 µm [
90,
195,
198]. However, research that used pore sizes of 300, 600, and 900 µm in porous Ti scaffolds found that those with macropores sizes of 600 and 900 µm had much higher bone ingrowth compared with the scaffolds with 300 µm pores [
101]. Bose et al. [
85] suggested that all macropore sizes between 100 and 600 µm are osteoconductive. Fukuda et al. [
199] experienced greater results in 500 and 600 µm pores compared with 900 and 1200 µm pores. Xue et al.’s [
98] results showed that macropore sizes in the range of 100–600 μm possess the optimum ability for cell growth into the pore structure of porous titanium.
According to the FDA regulations, macropore sizes of 100–1000 um are approved for coatings for Ti implants [
194]. Large macropores have a smaller surface area than do small pores, decreasing the cell attachment on the implant [
86]. However, large macropores increase scaffold vascularisation, which is vital for supplying oxygen and nutrients to the tissue as well as osteoblast proliferation and migration [
80], but they decrease the mechanical strength of the material. The limit of how much the macropore size can be increased while maintaining sufficient mechanical strength depends on both the material and the processing conditions. Therefore, regulatory guidelines for surface coating may be misleading for fully macroporous implants, since the strength-to-weight ratio differs between a porous and solid structure. Since the porosity decreases the strength of the implant, and large pore sizes decrease the strength of the internal architecture, large pore sizes must be avoided to increase the structure’s strength. A more defined pore size range is therefore sought [
86].
In this study, the macroporosity used in different studies was explored. It was found that no consensus currently exists on what upper limit to macropore size that is ideal, but somewhat of a consensus on the lower limit exists (100 µm). According to FDA regulations, porous implants should have macropore sizes between 100 and 1000 µm [
194]. It has further been found that macropores start to lose their osteogenic functionality when larger than 500–600 µm [
8,
16,
85,
98,
199]. Considering that a fully porous structure is weaker than a solid structure, and that high strength is vital for implants, it can be assumed that there is no need to design a structure with pores larger than what is needed to cater for all functions within the implant.
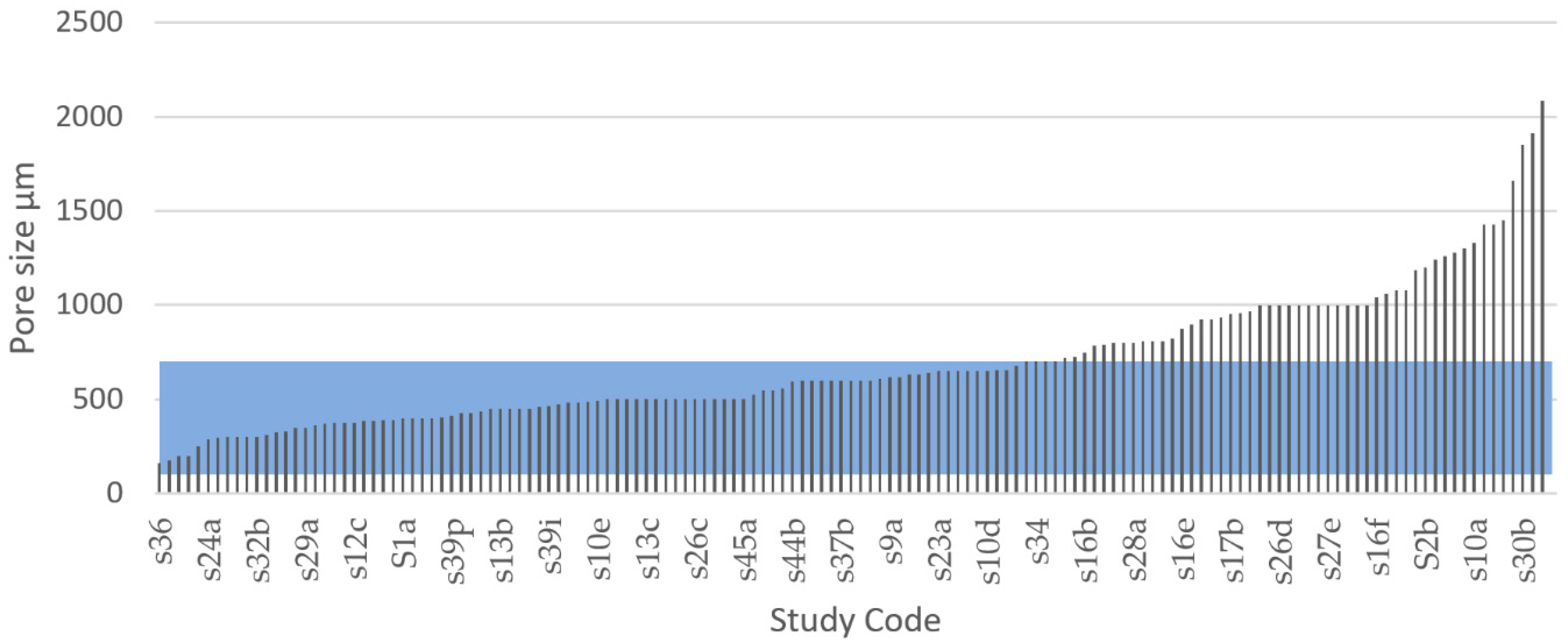
These findings made us choose a macropore size range of 100–600 µm as the IQA for porous metal implants to identify the studies in the systematic search that fabricated Ti scaffolds with pore size values within this range. From the 42 articles that recorded pore size of various degrees, a total of 144 results were extracted and compared with the selected IQA pore size range, as seen in
Figure 10. According to our results, 51.4% of the results of all studies had a macropore size within 100–600 µm. It was further noted that 86.8% of the experimental results of all studies had a macropore size within the FDA recommended range of 100–1000 µm. From these results, we could infer that most of the research studies identified through the systematic search somewhat considered the macroporosity range required to satisfy medical regulations.
By contrast, a total of 68 results out 144 showed pore size values above the acceptable macropore size range representing 48.6% of the total results extracted in this systematic literature review. There were several reasons for these studies to explore pore sizes above 600 µm. For example, the FDA approves macropore sizes between 100 and 1000 µm [
194]. Hara et al. [
96] tested four porous structures with different macropore size to explore their mechanical properties. Taniguchi tested 300, 600, and 900 µm pore sizes and found that the structures with 600 and 900 µm pore size exhibited higher bone ingrowth. Large macropores increase scaffold vascularisation, which is vital for supplying oxygen and nutrients to the tissue as well as osteoblast proliferation and migration [
80]; however, larger pores also have a smaller surface area compared with small pores, decreasing the cell attachment on the implant [
86]. Larger macropores also result in higher porosity, and this reduces the strength of the implant [
187,
188].
The ideal macropore size for bone implants is controversial and undefined, and according to Otsuki et al., a reason for the varied pore size data may be that the interconnectivity of pores was not considered [
198]. Macropore size regulations have been developed for the first generation of porous implants, which use a single-scaled porous network with repeated, equally sized, and shaped pores. However, bone grows in a naturally random structure with pores of different sizes, shapes, and directions similar to the structure of a sponge [
130,
155]. The use of a multiscale porous scaffold that combines smaller and larger pore sizes within the same structure is a recent strategy to optimise the internal architecture of implants [
142,
188]. This method combines advantages of both small and large macropores without decreasing the strength or reducing the bone in-growth to levels that are inappropriate in application [
188]. According to our results, a total of 8 out of 50 studies used some sort of multiscale pore approach, but it was observed that the design method varied, and that the researchers failed to provide the percentage of the total structure that used each pore size. It was further observed that a multiscale porous structure occurred in some implants where the manufacturing of a single-scaled structure resulted in varying pore sizes due to unprecise manufacturing tolerances.
3.4.4. Pore Inter Connectivity
According to our results, 46% of the collected studies registered pore interconnectivity. Interestingly, all of these studies designed their porous scaffolds with an interconnectivity of 100%. The pores in a porous bone implant must be interconnected to ensure movement and the supply of necessary nutrients through ingrowth of tissue and bone [
200]. Interconnected pores tend to facilitate the flow of fluids and biological cells through the structure which is essential for bone tissue formation [
185]. According to Nyberg et al. [
201] the integration of artificial material tissue with native tissue can be improved by interconnected pores. Tang et al. [
188] suggested that an increased pore interconnectivity increases the number and size of blood vessels formed in scaffolds. The interconnectivity is also a critical factor for ensuring that all cells within the structure are within a 200 µm range from a blood supply to provide transfer of nutrients and oxygen [
202]. According to the FDA’s recommendations for porous metal coatings, pores in such structures must be interconnected [
194]. Although this requirement is for surface coatings, it also indicates the importance of an interconnected porosity for fully porous implants. In the systematic review, it appears as though a vast majority of studies had indicated the importance of an interconnected porosity. Therefore, to guarantee all processes and fluid movements necessary for tissue and bone ingrowth, the selected IQA for pore interconnectivity would ideally be 100%.
3.4.5. Elastic Modulus
It was observed in this systematic review that an elastic modulus is a property commonly reported in AM porous scaffolds studies (by 89% of all studies). A controlled modulus of elasticity has proved to be critical in prostheses and scaffolds to avoid stress shielding [
81,
82]. Stress shielding occurs when there is a stiffness mismatch between the implant and surrounding bone, and it can cause inflammation and the need for revision surgery [
197]. Ti and common implant Ti alloys have an elastic modulus of roughly 100–120 GPa [
81,
84,
138,
197]. A reduced modulus is necessary to avoid stress shielding and can be achieved by designing implants with a porous structure [
90].
Defining an ideal specific modulus of elasticity for porous bone implants is not practical because Since the mechanical properties of human bone, especially the elastic modulus, change drastically with factors, such as age, physical activity, and health. For example, femoral bone specimens from patients aged 3, 5, and 35 years had an elastic modulus of 7, 12.8, and 16.7 GPa, respectively, indicating a dramatic change with age [
90]. As previously shown in
Table 6, the elastic modulus of human bone varies in the literature. Chen and Thouas [
57] estimated the elastic modulus of cortical bone to be approximately 11–21 GPa in the longitudinal direction, whereas Lee et al. [
147] suggested 18–22 GPa. Wang et al. [
81] suggested a wider range of 3–30 GPa. These findings indicate that the stiffness of an implant may need to be adjusted specifically for the person it is intended for, and that the target value for the elastic modulus may be specific to each patient. Therefore, it is more practical to think that for the design of porous scaffolds, an ideal target area exists for the modulus of elasticity. Based on this, the IQA for elastic modulus is proposed to be 3–30 GPa for fully porous Ti implants.
Figure 11 and
Figure 12 show the elastic modulus that was reported in the reviewed articles and these values were compared with the proposed IQA. From the extracted of elastic modulus results, 55.5% reached the target area of 3–30 GPa. These implants achieved an elastic modulus within the range of natural bone and would therefore eliminate risk of stress shielding. By contrast, 40% of the results exhibited an elastic modulus below 3 GPa, and only 3.6% of the results reported an elastic modulus higher than 30 GPa. These results clearly demonstrated that most studies are aiming towards a modulus of elasticity closer to the bone modulus.
The elastic modulus of metals such as titanium and its alloys naturally have a much higher elastic modulus compared with bone [
81]. However, research shows that the elastic modulus of metals can be readily adjusted by modifying their porosity. Porous metals with a low modulus of elasticity correspond to high levels of porosity. For example, Wang et al. [
84] explored five types of porous structures using the same material (TiNbZr) and pore size (550 µm) but ranging porosity. His results revealed that four of the implants with porosities ranging from 42% to 69% all achieved an elastic modulus within the approved range of 3–30 GPa; however, the implant with the highest porosity (74%) achieved the lowest elastic modulus of 1.6 GPa. Similarly, Li et al. [
203] used a porosity of 91% resulting in a low elastic modulus of 0.8 GPa. Furthermore, Chen et al. [
204] received an elastic modulus of 44.4 GPa for a porous titanium structure using 30% porosity but by increasing the porosity to 40% the elastic modulus was reduced to 24.7 GPa.
Using the data obtained through the systematic literature search we calculated two multiple linear regressions to predict the modulus of elasticity of beam and TPMS-based AMd Ti scaffolds. The regression model used the independent variables of pore size, relative density (porosity), and the interaction of pore size–porosity. According to our results, a regression equation was found for beam-based AMd Ti scaffolds (F(3,75) = 54.139,
p < 0.0001), with an R
2 adj of 0.671, as shown in
Figure 13a. The residuals of the multiple linear regression are randomly scattered around the centre line of zero with no obvious pattern. The predicted compressive yield strength of beam-based scaffolds is equal to 27.738 – 0.078 (pore size) – 27.417 (porosity) + 0.0689 (pore size*porosity), where pore size is coded or measured in µm, and relative density expressed as porosity as a percentage. The beam-based scaffolds’ modulus of elasticity decreased 0.078 MPa for each µm, 27.417 MPa per 1% of porosity increment, and increased 0.0689 MPa for the interaction pore size*porosity. Both pore size (
p < 0.0005) and porosity (
p < 0.0001) were significant predictors of beam-based scaffolds’ modulus of elasticity, including the interaction between pore size and porosity (
p < 0.0001).
In the case of the multiple linear regression of TPMS based AMd Ti scaffolds a significant regression equation was also found (F(3,28) = 4.897,
p < 0.0073), with an R
2 adj of 0.273, as shown in
Figure 13b. The residuals of the multiple linear regression are randomly scattered around the centre line of zero with no obvious pattern. The scaffolds’ predicted modulus of elasticity is equal to 0.008 − 0.002 (pore size)–2.342 (porosity) + 0.002 (pore size*porosity). The TPMS based scaffolds’ modulus of elasticity decreased 0.002 MPa for each µm, 2.342 MPa per 1% of porosity increment, and 0.002 MPa for the interaction pore size*porosity. Pore size was a significant predictor of TPMS-based scaffolds’ modulus of elasticity with a
p-values < 0.0563. However, porosity was not a significant predictor with
p-values < 0.553 and 0.843, respectively. Moreover, no interaction between pore size and porosity was found regarding to modulus of the elasticity.
3.4.6. Compressive Yield Strength
For an adequate functioning of any load-bearing implant, it is vital that its design withstand the required forces and loading cycles. Mechanical strength is one of the implant’s most crucial features for avoiding implant failure. To withstand the loads of daily activities, load-bearing implants must have at least the same yield strength as the bone that they replace [
81]. The yield point of bone represents the threshold from where the structure accumulates irreversible deformation. Unlike bulk metals such as steel, the yield point of bones cannot be clearly distinguished; it is rather associated with a continuous transition zone [
160]. Strain beyond the yield point will deform the structure beyond its point of resilience causing material damage, usually occurring as micro-cracks [
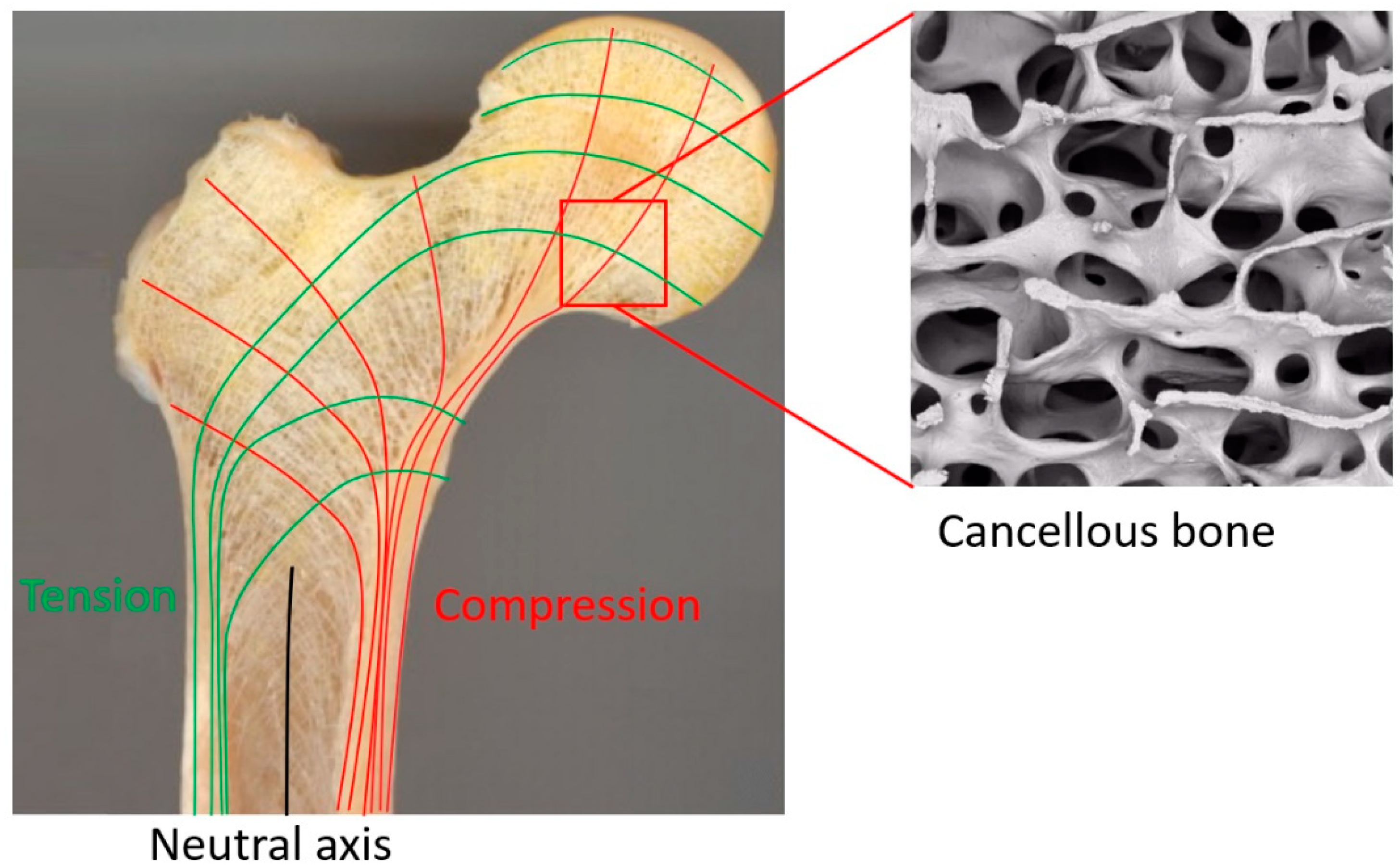
205]. Bone tissue has evolved to mainly support compressive stress [
206,
207]. Bone is 30% weaker under tensile stress, and 65% weaker under shear stress [
208]. Therefore, load-bearing implant scaffolds require a high compressive strength to prevent fractures and improve functional stability [
209]. The compressive yield strength of cortical bone varies in the literature. As previously shown in
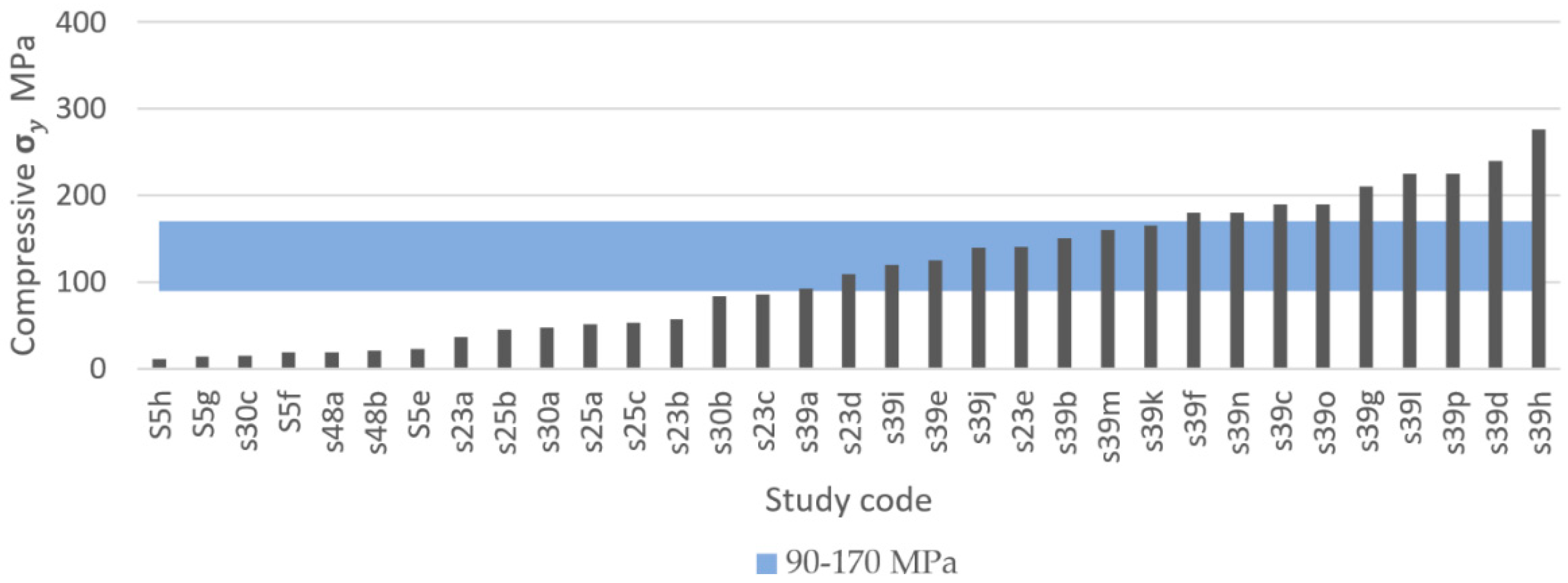
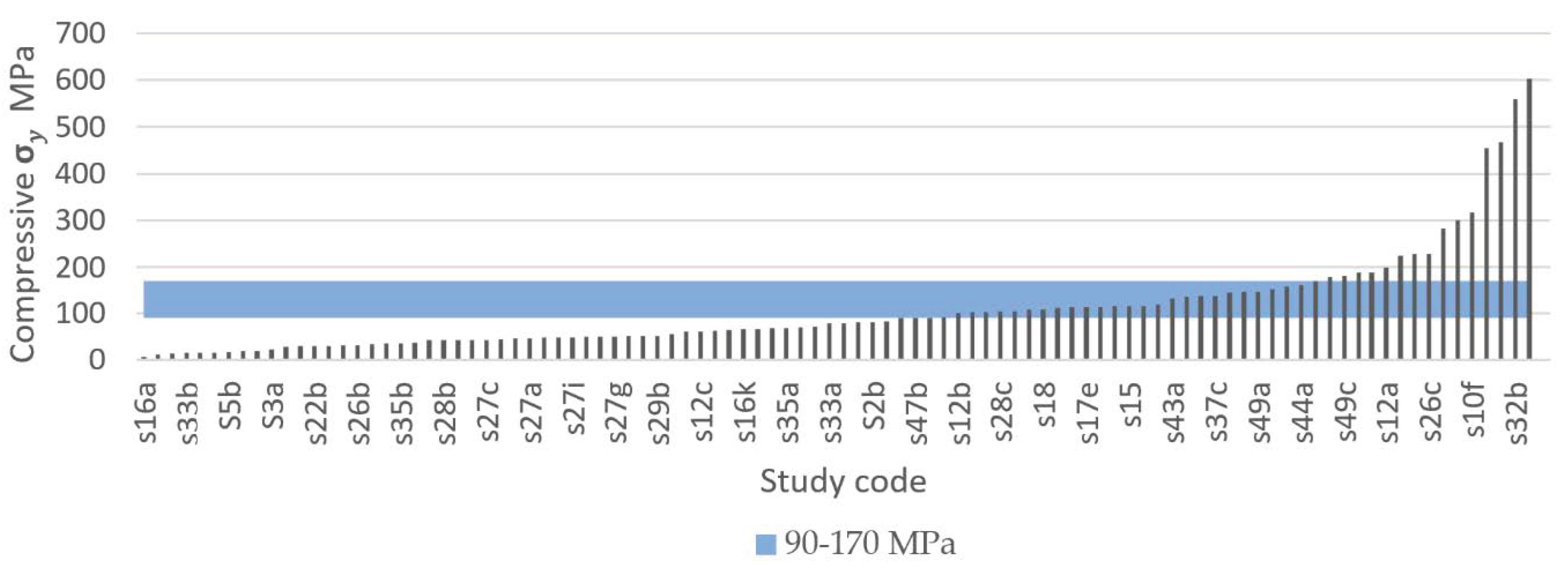
Table 6, the compressive yield strength of cortical bone varies approximately between 90 and 170 MPa. To replace like with like, using a biomimetic approach for comparison purposes, a minimum and a maximum compressive yield strength of 90 MPa and 170 MPa were selected as the IQA for fully porous Ti implants.
The systematic search identified that 37 out of 50 studies recorded compressive yield strength, from which a total of 133 experimental results were extracted and compared, as shown in
Figure 14 and
Figure 15.
Figure 14 presents the results of studies using TPMS structures and
Figure 15 presents the results of studies using porous beam-based metamaterials. Both comparisons show high numbers of studies resulting in a compressive yield strength below 90 MPa. A total of 55.7% of all results had a compressive yield strength below the defined IQA target and 25% of the studies achieved a compressive yield strength within the bone region. On the other hand, only 19% of the extracted experimental results had a strength above the bone region. Such implants would have strengths similar to or higher than cortical bone and are expected to not experience permanent deformation caused by the expected bone compressive loading conditions in the human body.
Decreased strength of a porous implant can result from high porosity and large pore sizes, [
81,
188]. For example, Zhang et al. [
113] fabricated porous scaffolds based on the TPMS diamond unit cell with a wide range of compressive yield strengths from 36 MPa to 140 MPa just by varying the scaffolds’ porosity and maintaining the pore size constant. The type of unit cell used to design porous scaffolds can also drastically change it mechanical properties. For example, Zhao et al. [
116] fabricated four porous scaffolds with the same pore size and similar porosities using two different unit cells (tetrahedron and octahedron). However, the scaffolds based on the octahedron unit cell registered almost double the compressive strength compared with those based on the tetrahedron unit cell [
116]. The compressive yield strength of porous metals can also be enhanced by gradually changing the porosity level along the radial direction of the scaffold. This was demonstrated by Zhang et al. [
100], who reported functionally graded porous scaffolds based on the diamond unit cell with superior comprehensive mechanical properties to the biomaterials with uniform porous structures.
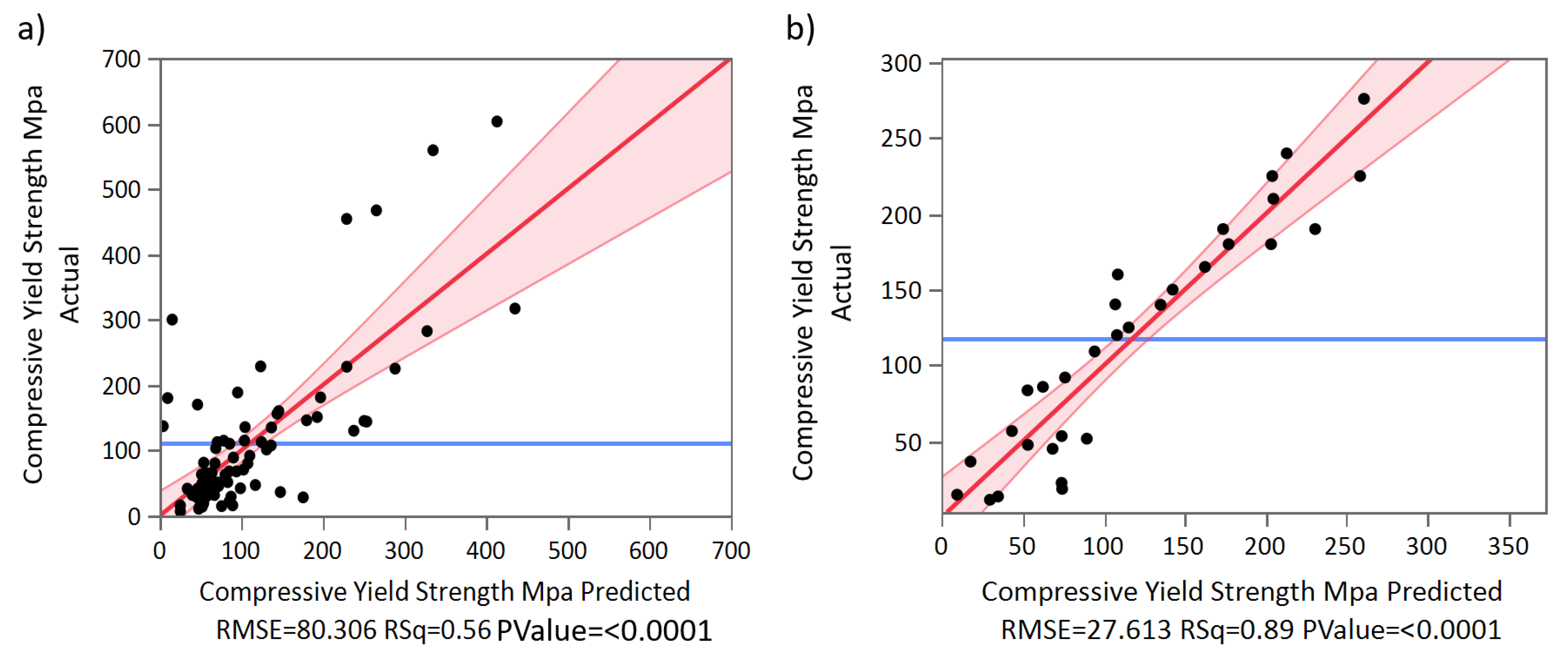
Using the data obtained through the systematic literature search, we calculated two multiple linear regressions to predict compressive yield strength based on pore size, porosity, and the interaction of size–porosity for beam-based and TPMS-based AMd Ti scaffolds, respectively.
According to our results, a regression equation was found for beam-based AMd Ti scaffolds (F(3,75) = 31.452,
p < 0.0001), with an R
2 adj of 0.539, as shown in
Figure 16a. The residuals of the multiple linear regression are randomly scattered around the centre line of zero, with no obvious pattern. The scaffolds’ predicted compressive yield strength is equal to 380.557 − 0.075(pore size)–350.828 (porosity) + 0.557 (pore size*porosity), where pore size is coded or measured in µm, and porosity is measured as a percentage. The beam-based scaffolds’ compressive yield strength decreased 0.075 MPa for each µm, 350.828 MPa per 1% of porosity increment, and increased 0.557 MPa for the interaction of pore size*porosity. Both pore size (
p < 0.0378), porosity (
p < 0.001), and the interaction between pore size and porosity (
p < 0.0048) were significant predictors of beam-based scaffolds’ compressive yield strength. The interaction between pore size and porosity was found to be significant with a
p-value < 0.0048.
Regarding the multiple linear regression of TPMS-based AMd Ti scaffolds, a significant regression equation was also found (F(3,27) = 65.547,
p < 0.0001), with an R
2 adj of 0.872, as shown in
Figure 16b. The residuals of the multiple linear regression are randomly scattered around the centre line of zero, with no obvious pattern. The scaffolds’ predicted compressive yield strength is equal to 524.780 − 0.008(pore size)–625.266 (porosity) + 0.183 (pore size*porosity). The TPMS-based scaffolds’ compressive yield strength decreased 0.008 MPa for each µm, 625.266 MPa per each 1% of porosity increment, and increased 0.183 MPa for the interaction of pore size*porosity. Porosity was a significant predictor of TPMS based scaffolds’ compressive yield strength with
p-values < 0.0001. However, pore size and the interaction between pore size and porosity were non-significant, with
p-values < 0.7018 and 0.3260, respectively.
3.4.7. Ultimate Compressive Strength
If loading surpasses the yield point of bone, it will eventually reach the ultimate point. This point represents the maximum compressive strength that a material can withstand without irreversible strains and damage occurring. Past this point, macrocracks are formed and fracture occurs [
160]. Bone implants in load-bearing applications must withstand high stress within the body, to a degree where no permanent deformation occurs during the load that the implant is expected to be exposed to. Hence, controlled ultimate compressive strength is a crucial property to study in bone implant research. Natural bone is estimated to have an ultimate compressive strength of 180–200 MPa [
84]. However, results vary in the literature. For example, Calori et al. [
8] suggested a more widespread range of 130–290 MPa, whereas Henkel et al. suggested 100–230 MPa [
168]. To replace like with like using a biometric approach, bone implants should have an ultimate compressive strength similar to that of bone [
8]. Taking into consideration the compressive yield strength suggested previously and the three results presented in
Table 5, the proposed IQA region for the ultimate compressive strength is between 180 MPa and 290 MPa.
In this systematic search a total of 60 experimental results of ultimate compressive strength from 19 different studies were extracted.
Figure 17 and
Figure 18 show the ultimate compressive strength of the different studies compared with the defined IQA target of between 180 MPa and 290MPa.
Figure 17 corresponds to experimental results of porous scaffolds composed of TPMS unit cells compared with the IQA target. According to
Figure 17, only one study with three different experimental results measured the ultimate strength of porous scaffolds based on TPMS unit cells. In this study by Yanez et al. [
120], three ultimate compressive strengths of 17, 47.5, and 83.5 MPa were achieved using the gyroid unit cell. Dramatic improvement in the ultimate compressive strength of the scaffold was achieved. This improvement in mechanical properties was possible by slightly changing the gyroid unit cell into an elongated gyroid. However, none of the experimental results obtained by Yanez et al. [
120] were able to reach the minimum IQA ultimate compressive strength proposed in this study. The low strength of Yanez at al.’s [
120] samples can be attributed to their high porosity values which ranged between 75% and 90%. This increased the stress concentration, reducing the ultimate compressive strength.
Figure 18 is composed of 19 different studies on beam-based unit cells where 57 experimental results are compared with the IQA target. According to
Figure 18, 10 experimental results reached higher ultimate compressive strengths than bone. The highest ultimate compressive strength (830 MPa) recorded was achieved with a scaffold based on the diamond unit cell by Zhang et al. [
100]. From all results recorded, a total of 16.7% achieved an ultimate compressive strength above the proposed IQA ultimate compressive strength; 10% had similar ultimate compressive strengths to bone; and 73.3% had lower ultimate compressive strengths than bone. The scaffolds that did not fulfil the required IQA ultimate compressive strength would risk fracturing due to macrocracks occurring during high loads. Porosity within a structure has been proven to decrease the strength of a structure [
81,
188], which may explain the high number of scaffolds with low ultimate strength.
The goal of designing a porous structure with enough porosity and pore size without diminishing strength is a difficult task, and as researchers aim to create highly porous structures with low elastic modulus, many structures experienced low ultimate strength. Attar et al. [
111] manufactured a porous titanium structure by SLM with rectangular pores and 17% porosity and achieved an ultimate compressive strength of 747 MPa. Using the same material, manufacturing method, and unit cell, a different structure with 37% porosity achieved an ultimate strength of 235 MPa. In a similar manner, Chen et al. [
204] designed three structures of the same material and manufacturing method. Using porosities of 30%, 40%, and 50%, the ultimate compressive strengths recorded were 524, 301.7, and 120.3 MPa, respectively, indicating that increased porosity reduces the strength of the structure.
3.4.8. Fatigue Strength
During normal daily activities, load-bearing implants experience just a fraction of the material’s ultimate stress [
209,
210,
211]. However, after years of use, the high cyclic loading to which load-bearing implants are subjected eventually leads to the accumulation of small stresses, causing progressive and localised material damage that results in implant failure [
212]. For instance, one of the most critical mechanical properties for load-bearing implants is fatigue strength. However, fatigue strength is the most difficult mechanical property to determine [
213].
The required fatigue resistance of a load bearing implant and its components mainly depends on their cyclic loading conditions and the required life span. For example, it is estimated that lower limb prostheses are subjected to up to 2 million gait cycles per year [
214], and in the case of orthodontic prostheses these can reach up to 300,000 loading cycles per year [
213]. Therefore, a large variety of medical standards exist for testing fatigue strength. Some of these fatigue tests differ depending on the type of load applied such as tension–tension, compression–compression, and tension–compression. In the case of load-bearing bones, their loading conditions in real-life activities are complex [
135]. However, bone is mainly loaded in compression [
206,
207]. Therefore, to test the fatigue life of metamaterials for bone implant applications, compression fatigue tests are preferred due to the simplicity of the test setups [
215].
Regarding the number of cycles that load bearing implants and their components need to have tested for fatigue strength, all the different medical standards agree that such products need to have a fatigue life within the high-cycle fatigue region (N > 10
4 cycles). For example, the ASTM standard F2777 – 16 recommends testing tibial inserts’ endurance and deformation under high flexion with a minimum number of cycles of 2.2 × 10
5, and in the case of dental implants they are typically tested up to 5 million cycles [
213,
216]. Nevertheless, for a component of a load-bearing implant to have at least 25 years of life span [
217], the highest number of cycles that must be tested is 10
7 cycles [
213,
216]. Taking into consideration current medical standards for load-bearing implants, the high-cycle fatigue region between 10
4 cycles and 10
7 cycles was selected as the IQA fatigue life for porous titanium metamaterials for bone regeneration.
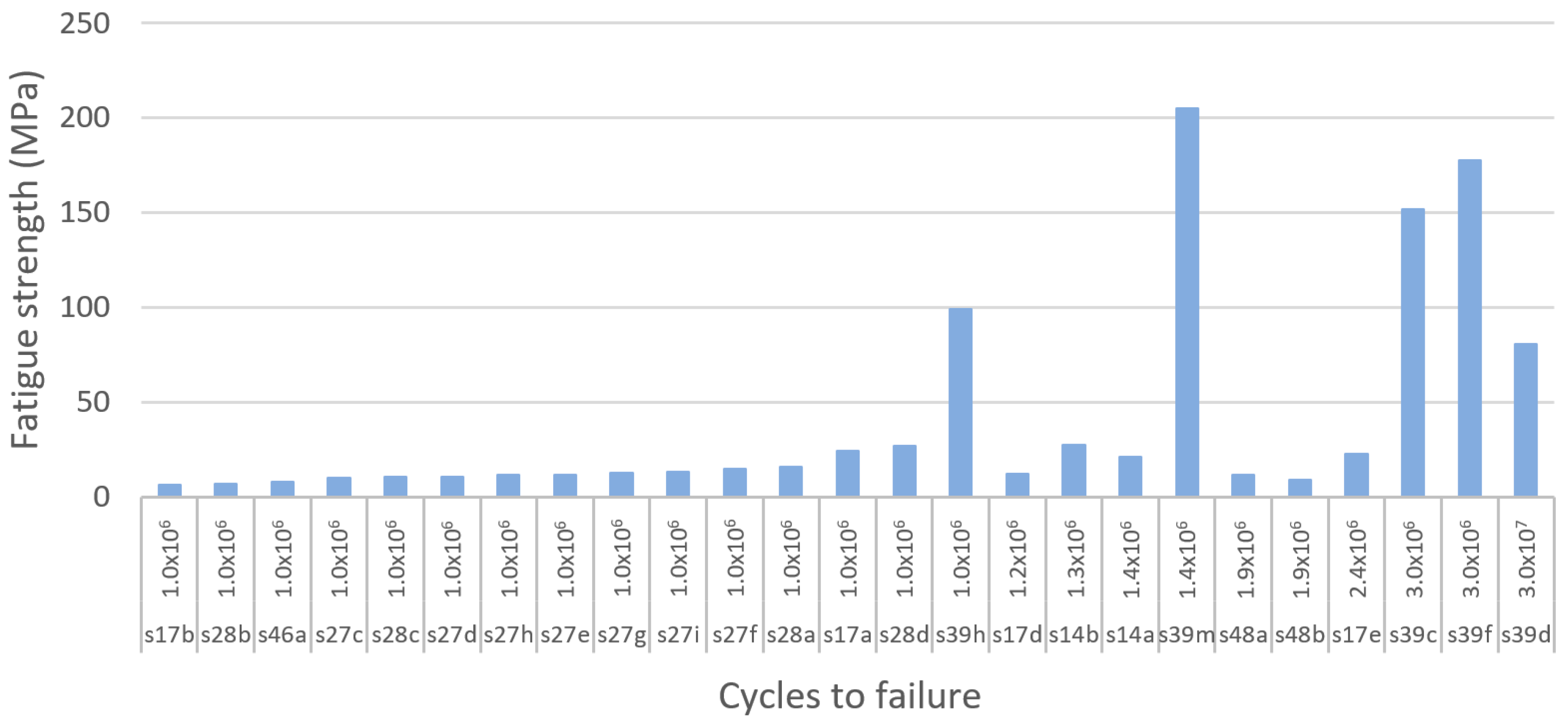
Using the selected high-cycle fatigue region, this systematic literature search identified a total of 13 different studies on fatigue resistance, among which 11 studies performed compression–compression fatigue tests. Then, for comparison purposes, a total of 51 experimental results were extracted and compared. Moreover, to facilitate the comparison of the results of the studies, they were classified according to the type of unit cell used to produce porous structures as beam and TPMS-based as resented in
Figure 19,
Figure 20 and
Figure 21. According to our results, the TPMS porous structures that withstood the highest stresses at the high-cycle fatigue region were achieved by Bobbert et al. [
79]. The primitive TPMS structure presented the highest stress within the high-cycle fatigue region, with 232 MPa at 3 × 10
4 cycles, as shown in
Figure 19. The TPMS porous structures that were able to withstand the second and third highest stresses within the high-cycle fatigue region were the I-WP and diamond structures, with 227 MPa at 3 × 10
5 cycles and 204 MPa at 3 × 10
6 cycles as shown in
Figure 19 and
Figure 20. Remarkably, the primitive TPMS structure was the only one to pass the 10
7 threshold with 80 MPa at 3 × 10
7 cycles, as presented in
Figure 20.
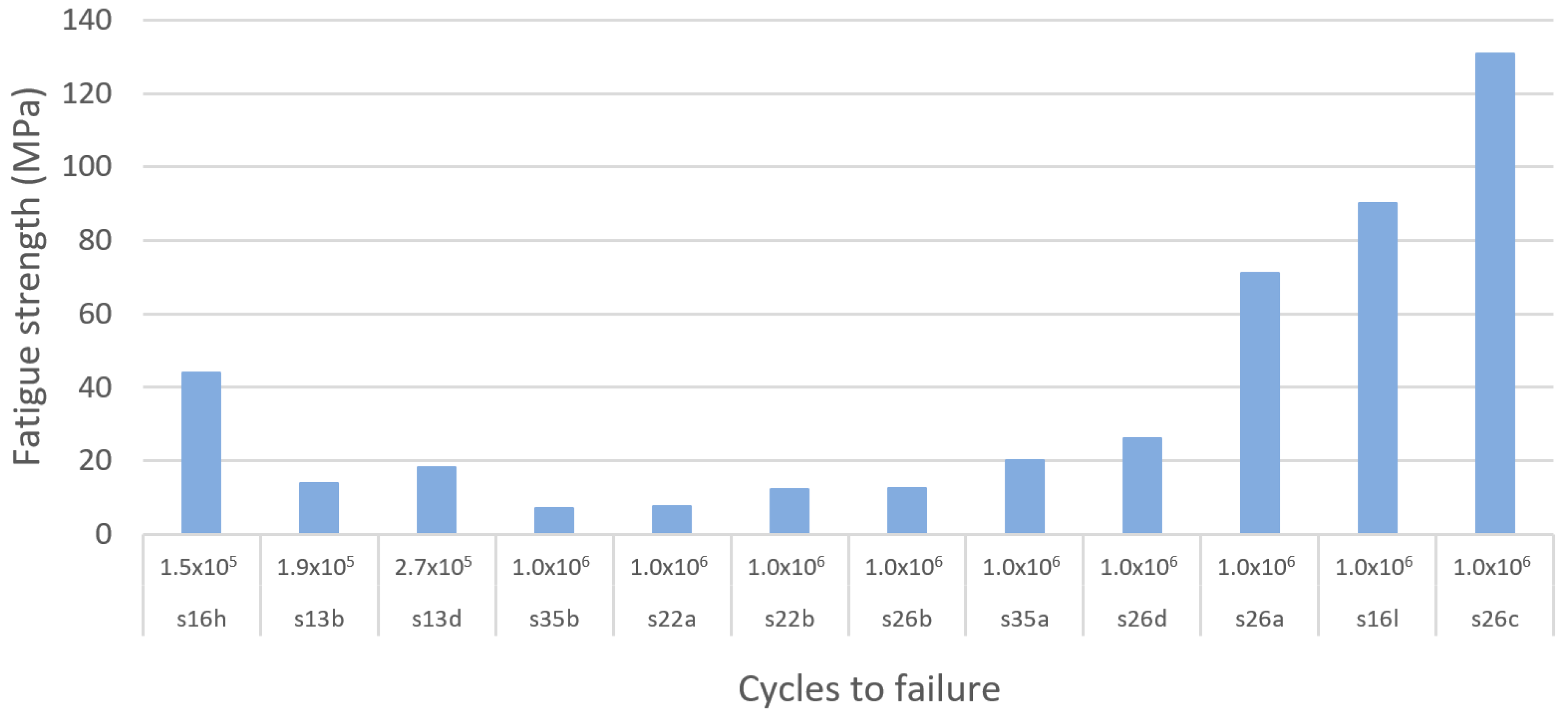
In the case of beam-based metamaterials the study performed by Zhao et al. [
116] achieved the highest fatigue strength with 130 MPa at 10
6 cycles using a lattice structure based on the octahedron unit cell, as shown in
Figure 21. In second and third place with the highest fatigue strength are the tetrahedron and the cubic porous lattice structures with 90 MPa at 1 × 10
6 cycles and 90 MPa at 1 × 10
6 cycles fabricated by Amin Yavari et al. [
106] and Zhao et al. [
116], as presented in
Figure 21.
According to the results of this systematic search it could be seen that TPMS structures provide superior fatigue strength to porous bio-metamaterials compared with beam-based unit cells. Moreover, in terms of fatigue resistance, it was identified that the primitive, I-WP, and diamond TPMS provided the best performance, whereas the octahedron, cubic, and tetrahedron are the best-performing lattice unit cells. However, it is crucial to note that several factors can affect the fatigue life of additively manufactured Ti metamaterials. Some of these factors are residual stresses and stress concentrators caused by high surface roughness and manufacturing defects [
218]. Moreover, the fatigue strength of bulk materials significantly degrades when they are in porous form or when voids and pores are developed during fabrication [
219]. In the case of additively manufactured components, it has been proven that their fatigue strength is extremely sensitive to localised and nonuniform heat and uncontrolled cooling cycles during fabrication [
220,
221].





























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}