Does the Addition of Zinc Oxide Nanoparticles Improve the Antibacterial Properties of Direct Dental Composite Resins? A Systematic Review

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Focus Question
2.5. Search Strategy
2.6. Study Selection
2.7. Data Collection Process
2.8. Data Items
- Author (year)—presents the author(s) of the article and the year of publication
- Sample—describes the study sample (i.e., type of composite resin)
- Treatment group—describes the treatment group(s), including the average size of zinc oxide nanoparticles used
- Experiment—names the test conducted (N.B: only data for the tests that assessed the antibacterial properties of the ZnO-NP composites were included and tabulated)
- Methodology—describes pertinent information on the corresponding test and the variable(s) measured
- Outcome—describes the outcome(s) of the experiment(s). All outcomes presented are statistically significant unless specified otherwise.
2.9. Quality and Risk of Bias in Individual Studies
3. Results
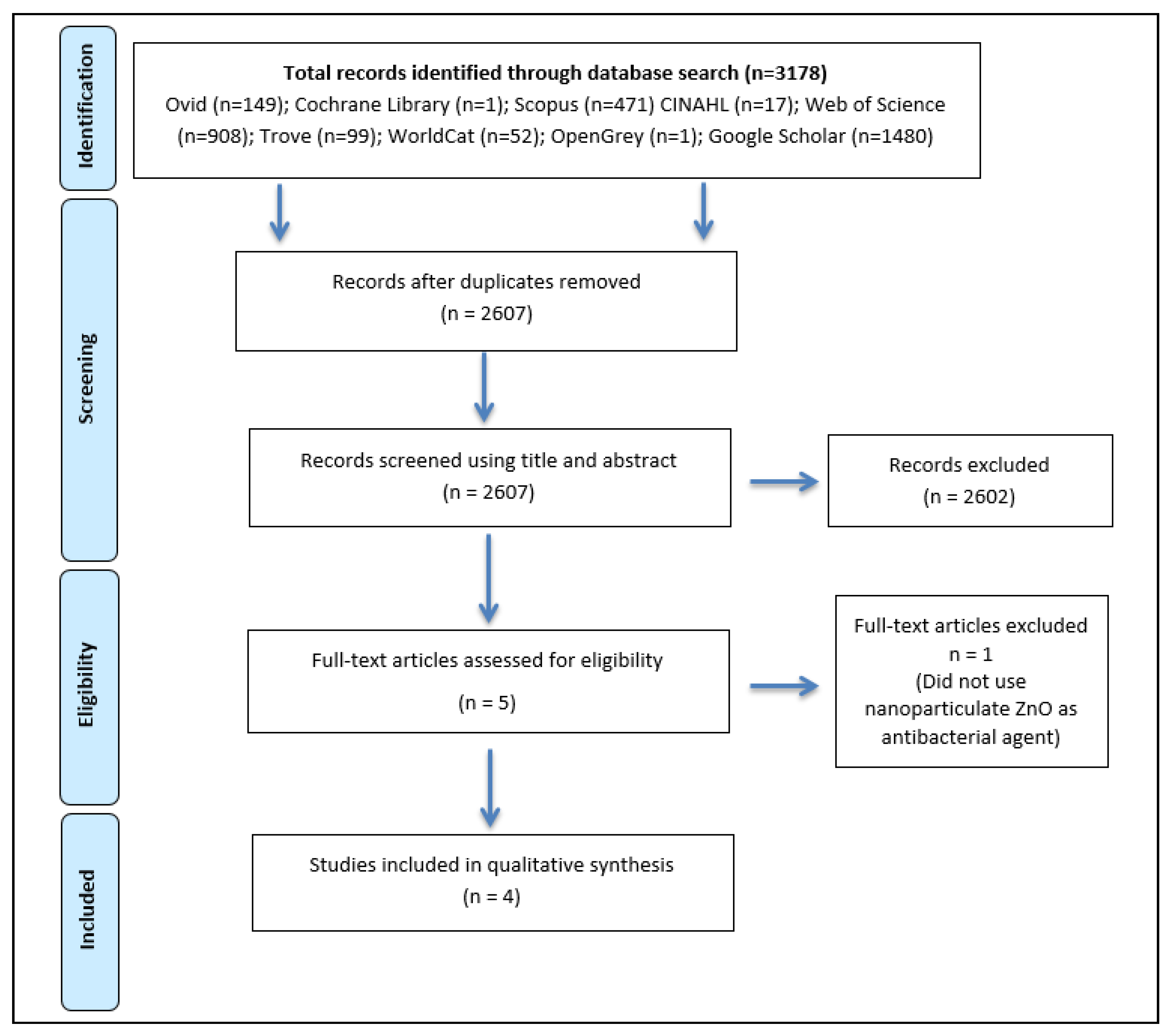
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality and Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smales, R.J.; Hawthorne, W.S. Long-term survival and cost-effectiveness of five dental restorative materials used in various classes of cavity preparations. Int. Dent. J. 1996, 46, 126–130. [Google Scholar] [PubMed]
- Bayne, S.C.; Ferracane, J.L.; Marshall, G.W.; Marshall, S.J.; van Noort, R. The Evolution of Dental Materials over the Past Century: Silver and Gold to Tooth Color and Beyond. J. Dent. Res. 2019, 98, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Opdam, N.J.; Bronkhorst, E.M.; Roeters, J.M.; Loomans, B.A. A retrospective clinical study on longevity of posterior composite and amalgam restorations. Dent. Mater. 2007, 23, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Zalkind, M.M.; Keisar, O.; Ever-Hadani, P.; Grinberg, R.; Sela, M.N. Accumulation of Streptococcus mutans on light-cured composites and amalgam: An in vitro study. J. Esthet Dent. 1998, 10, 187–190. [Google Scholar] [CrossRef]
- Beyth, N.; Domb, A.J.; Weiss, E.I. An in vitro quantitative antibacterial analysis of amalgam and composite resins. J. Dent. 2007, 35, 201–206. [Google Scholar] [CrossRef]
- Gunyakti, N.; Gur, G.; Misirligil, A. In vivo adhesion of Streptococcus mutans on amalgam and composite restorative materials. Ankara Univ. Hekim. Fak. Derg. 1990, 17, 83–86. [Google Scholar]
- Auschill, T.M.; Arweiler, N.B.; Brecx, M.; Reich, E.; Sculean, A.; Netuschil, L. The effect of dental restorative materials on dental biofilm. Eur. J. Oral Sci. 2002, 110, 48–53. [Google Scholar] [CrossRef]
- Kubo, S.; Kawasaki, A.; Hayashi, Y. Factors associated with the longevity of resin composite restorations. Dent. Mater. J. 2011, 30, 374–383. [Google Scholar] [CrossRef] [Green Version]
- Dijken, J.W.V.v.; Sunnegårdh-Grönberg, K.; Lindberg, A. Clinical long-term retention of etch-and-rinse and self-etch adhesive systems in non-carious cervical lesions: A 13 years evaluation. Dent. Mater. 2007, 23, 1101–1107. [Google Scholar] [CrossRef]
- Sousa, R.P.; Zanin, I.C.; Lima, J.P.; Vasconcelos, S.M.; Melo, M.A.; Beltrao, H.C.; Rodrigues, L.K. In situ effects of restorative materials on dental biofilm and enamel demineralisation. J. Dent. 2009, 37, 44–51. [Google Scholar] [CrossRef]
- Ahn, S.J.; Lee, S.J.; Kook, J.K.; Lim, B.S. Experimental antimicrobial orthodontic adhesives using nanofillers and silver nanoparticles. Dent. Mater. 2009, 25, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Farrugia, C.; Camilleri, J. Antimicrobial properties of conventional restorative filling materials and advances in antimicrobial properties of composite resins and glass ionomer cements—A literature review. Dent. Mater. 2015, 31, e89–e99. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.F.; Wu, R.; Fan, Y.; Liao, S.; Wang, Y.; Wen, Z.T.; Xu, X. Antibacterial dental composites with chlorhexidine and mesoporous silica. J. Dent. Res. 2014, 93, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Weir, M.D.; Xu, H.H.; Antonucci, J.M.; Kraigsley, A.M.; Lin, N.J.; Lin-Gibson, S.; Zhou, X. Antibacterial amorphous calcium phosphate nanocomposites with a quaternary ammonium dimethacrylate and silver nanoparticles. Dent. Mater. 2012, 28, 561–572. [Google Scholar] [CrossRef] [Green Version]
- Glasspoole, E.A.; Erickson, R.L.; Davidson, C.L. A fluoride-releasing composite for dental applications. Dent. Mater. 2001, 17, 127–133. [Google Scholar] [CrossRef]
- J, L.S.; Szynkowska, M.I.; Kleczewska, J.; Kowalski, Z.; Sobczak-Kupiec, A.; Pawlaczyk, A.; Sokolowski, K.; Lukomska-Szymanska, M. Evaluation of resin composites modified with nanogold and nanosilver. Acta Bioeng. Biomech. 2014, 16, 51–61. [Google Scholar]
- Schnaider, L.; Ghosh, M.; Bychenko, D.; Grigoriants, I.; Ya’ari, S.; Shalev Antsel, T.; Matalon, S.; Sarig, R.; Brosh, T.; Pilo, R.; et al. Enhanced Nanoassembly-Incorporated Antibacterial Composite Materials. ACS Appl. Mater. Interfaces 2019, 11, 21334–21342. [Google Scholar] [CrossRef]
- Chen, L.; Suh, B.I.; Yang, J. Antibacterial dental restorative materials: A review. Am. J. Dent. 2018, 31, 6B–12B. [Google Scholar]
- Tavassoli Hojati, S.; Alaghemand, H.; Hamze, F.; Ahmadian Babaki, F.; Rajab-Nia, R.; Rezvani, M.B.; Kaviani, M.; Atai, M. Antibacterial, physical and mechanical properties of flowable resin composites containing zinc oxide nanoparticles. Dent. Mater. 2013, 29, 495–505. [Google Scholar] [CrossRef]
- Mirhosseini, F.; Amiri, M.; Daneshkazemi, A.; Zandi, H.; Javadi, Z.S. Antimicrobial effect of different sizes of nano zinc oxide on oral microorganisms. Front. Dent. 2019, 16, 105–112. [Google Scholar] [CrossRef]
- Fatemeh, K.; Mohammad Javad, M.; Samaneh, K. The effect of silver nanoparticles on composite shear bond strength to dentin with different adhesion protocols. J. Appl. Oral Sci. 2017, 25, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Syafiuddin, T.; Hisamitsu, H.; Toko, T.; Igarashi, T.; Goto, N.; Fujishima, A.; Miyazaki, T. In vitro inhibition of caries around a resin composite restoration containing antibacterial filler. Biomaterials 1997, 18, 1051–1057. [Google Scholar] [CrossRef]
- Turkun, L.S.; Celik, E.U. Noncarious class V lesions restored with a polyacid modified resin composite and a nanocomposite: A two-year clinical trial. J. Adhes Dent. 2008, 10, 399–405. [Google Scholar] [PubMed]
- Mitra, S.B.; Wu, D.; Holmes, B.N. An application of nanotechnology in advanced dental materials. J. Am. Dent. Assoc. 2003, 134, 1382–1390. [Google Scholar] [CrossRef] [Green Version]
- Aydin Sevinc, B.; Hanley, L. Antibacterial activity of dental composites containing zinc oxide nanoparticles. J. Biomed. Mater. Res. B Appl. Biomater. 2010, 94, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Mudiyanselage, D.A.; Beni, C.; Arun, D.; Mohamed, R.G.; Liddell, M. Does the Addition of Zinc Oxide Nanoparticles Improve the Antimicrobial Properties of Direct Dental Resin Composites? A Systematic Review. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=131383 (accessed on 20 June 2020).
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Shen, M.; Liang, G.; Gu, A.; Yuan, L. Development of high performance dental resin composites with outstanding antibacterial activity, high mechanical properties and low polymerization shrinkage based on a SiO2 hybridized tetrapod-like zinc oxide whisker with C [double bond, length as m-dash] C bonds. RSC Adv. 2016, 6, 56353–56364. [Google Scholar]
- Kasraei, S.; Sami, L.; Hendi, S.; Alikhani, M.Y.; Rezaei-Soufi, L.; Khamverdi, Z. Antibacterial properties of composite resins incorporating silver and zinc oxide nanoparticles on Streptococcus mutans and Lactobacillus. Restor. Dent. Endod. 2014, 39, 109–114. [Google Scholar] [CrossRef] [Green Version]
- Brandão, N.L.; Portela, M.B.; Maia, L.C.; Antônio, A.; Silva, E.M.D. Model resin composites incorporating ZnO-NP: Activity against S. mutans and physicochemical properties characterization. J. Appl. Oral Sci. 2018, 26, e20170270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira-Cenci, T.; Cenci, M.S.; Fedorowicz, Z.; Azevedo, M. Antibacterial agents in composite restorations for the prevention of dental caries. Cochrane Database Syst. Rev. 2013, 12, CD007819. [Google Scholar] [CrossRef] [PubMed]
- Davies, D. Understanding biofilm resistance to antibacterial agents. Nat. Rev. Drug Discov. 2003, 2, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, R.; Garcia-Garcia, F.J.; Reller, A. Rapid degradation of zinc oxide nanoparticles by phosphate ions. Beilstein J. Nanotechnol. 2014, 5, 2007–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghallab, A. In vitro test systems and their limitations. EXCLI J. 2013, 12, 1024–1026. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Database(s) | MeSH Terms/Subject Headings and/or Keyword Search |
|---|---|
| Medline (Ovid) | exp Antibacterial Agents/ (bacteriostatic or bacteristatic or bactericidal* or bacteriocidal* or anti-bacterial or antibacterial or bacteriocidal or anti-microbial* or antimicrobial*).mp. 1 or 2 exp Composite Resins/ (composite*).mp. 4 or 5 exp Zinc Oxide/ (“zinc oxide” or zinc-oxide or ZnO or ZnO-NP or Nano-ZnO or “Nano ZnO” or nano-zinc-oxide or “nano zinc oxide”).mp. 7 or 8 exp Nanoparticles/ (nanoparticle* or nanoparticle*).mp. 10 and 11 3 and 6 and 9 and 12 |
| Cochrane Library | (antibacterial OR anti-bacterial OR bactericidal OR bacteriocidal OR bacteriostatic OR bacteriostatic OR anti-microbial OR antimicrobial) in All Text AND composite in All Text AND (Zinc-Oxide OR “Zinc Oxide” OR ZnO OR ZnO-NP OR Nano-ZnO OR “Nano zinc oxide” OR Nano-zinc-oxide) in All Text AND (nanoparticle OR nano-particle) in All Text—(Word variation have been searched) |
| SCOPUS | (TITLE-ABS-KEY (zno OR “zinc oxide” OR zinc-oxide OR zno-np OR “Nano ZnO” OR nano-zno OR “Nano zinc oxide” OR nano-zinc-oxide) AND TITLE-ABS-KEY (composite) AND TITLE-ABS-KEY (antibacterial OR bacteriostatic OR bacteriocidal OR anti-microbial* OR antimicrobial* OR anti-bacterial* OR bactericidal* OR bacteristatic) AND TITLE-ABS-KEY (nanoparticle* OR nano-particle*)) |
| CINAHL | (ZnO OR “zinc oxide” OR Zinc-Oxide OR ZnO-NP OR “Nano ZnO OR Nano-ZnO OR “Nano zinc oxide” OR Nano-zinc-oxide) AND composite* AND ((Antibacterial OR bacteriostatic OR bacteriocidal OR anti-microbial* OR antimicrobial* OR Anti-bacterial OR Bactericidal* OR bacteristatic)) AND ((nanoparticle* OR nano-particle)) |
| Web of Science | TS = (Antibacterial OR Anti-bacterial OR Bactericidal* OR Bacteriostatic OR Bacteristatic OR Anti-microbial* OR Antimicrobial*) TS = (Composite*) TS = (Zinc-Oxide OR “Zinc Oxide” OR ZnO OR ZnO-NP OR “Nano ZnO” OR Nano-ZnO OR “Nano zinc oxide” OR Nano-zinc-oxide) TS = (Nanoparticle* OR Nano-particle*) #4 AND #3 AND #2 AND #1 |
| Trove | (ZnO OR “zinc oxide” OR Zinc-Oxide OR ZnO-NP OR “Nano ZnO OR Nano-ZnO OR “Nano zinc oxide” OR Nano-zinc-oxide) AND composite* AND ((Antibacterial OR bacteriostatic OR bacteriocidal OR anti-microbial* OR antimicrobial* OR Anti-bacterial OR Bactericidal* OR bacteristatic)) AND ((nanoparticle* OR nano-particle)) N.B. Search was carried out in the Journals, articles and data sets tab |
| Google Scholar | Dental resin composite antibacterial inhibit biofilm nanoparticle “zinc oxide” |
| World Cat | Dental resin composite antibacterial nanoparticle “zinc oxide” |
| OpenGrey | (ZnO OR “zinc oxide” OR Zinc-Oxide OR ZnO-NP OR “Nano ZnO OR Nano-ZnO OR “Nano zinc oxide” OR Nano-zinc-oxide) AND composite* AND ((Antibacterial OR bacteriostatic OR bacteriocidal OR anti-microbial* OR antimicrobial* OR Anti-bacterial OR Bactericidal* OR bacteristatic)) AND ((nanoparticle* OR nano-particle)) |
| Methodological Items for Non-Randomized Studies (Modified Version) | Score * |
|---|---|
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
|
| Author (Year) | Sample | Treatment Group(s) | Experiment | Quantification (Variables) | Outcome |
|---|---|---|---|---|---|
| Sevinç et al. (2010) [25] | Microhybrid composite resin (AElite All-purpose body) Nanofilled composite resin (Filtek Supreme Plus Universal Restorative) | 1, 5, and 10 wt % uncoated ZnO-NPs (40–100 nm) in microhybrid composite resin 1 wt % polar coated ZnO-NPs (40–100 nm) in microhybrid composite resin 1 wt % non-polar coated ZnO-NPs (40–100 nm) in microhybrid composite resin 10 wt % ZnO-NPs (40–100 nm) in nanofilled composite resin | Direct contact test | Viable colony-forming units (CFUs) after 48 h. S. sobrinus biofilm. | Reduced CFUs in 5 and 10 wt % ZnO-NP composites compared to controls. |
| Aged direct contact test | Viable CFUs after each cycle. Three cycles of 72 h growth of S. sobrinus biofilms. | Reduced biofilm growth in the 3rd cycle for 10 wt % ZnO-NP composite compared to the 3rd cycle of the unmodified composite resin. | |||
| Three species biofilm direct contact test | Viable CFUs after 72 h of biofilm growth. Bacterial culture of S. oralis, S. gordonii, and A. naeslundii was used. | No statistically significant reduction in CFUs between 10 wt % ZnO-NP composite resin and controls. | |||
| Scanning electron microscopy (SEM) and confocal laser scanning microscopy (CLSM) of direct contact test | Qualitative description of composite discs via scanning electron microscopy and confocal laser microscopy. Age of S. sobrinus biofilm was 24 h. | S. Sobrinus attachment and biofilm coverage was qualitatively lower on the 10 wt % ZnO-NP composites compared to unmodified control composites in both SEM and CLSM. Both SEM and CLSM visualization revealed qualitatively less dense biofilm formation and greater space between microbes in the 10 wt % ZnO-NP composite compared to the control. | |||
| Kinetic measurement of bacterial growth | Well suspension culture plates were coated with composite resins and inoculated with bacterial culture for 6 h. The per hour absorbance measurements were recorded using a plate reader (490 nm at 1 h intervals for 12 h). | There was no statistically significant difference between the 1, 5, and 10 wt % ZnO-NP composites at the 14th h. However, all of these composites showed a reduction in absorbance measurements compared to the control composites. | |||
| Agar diffusion test | The inhibition zones around the composite discs were measured after 48 h incubation of bacteria inoculated BHI agar plates. | There was no zone of inhibition around either the ZnO-NP composites or the unmodified composites. In addition, bacterial colonies were observed on the bottom surfaces of these composites. | |||
| Hojati et al. (2013) [19] | Flowable composite resin (Heliomolar Flow) | 1, 2, 3, 4 and 5 wt % ZnO-NPs (20 nm) in flowable composite resin | Direct contact test | Visual counting of number of viable CFUs after 24 h incubation. Age of the S. Mutans biofilms were 3, 6, 12, and 24 h. | There was a reduction in the number of CFUs with an increasing percentage of ZnO-NPs in all of the ZnO-NP composites compared to control. The 4 and 5 wt % ZnO-NP composites completely inhibited bacterial colony formation. |
| Aged direct contact test | Visual counting of number of viable CFUs after 3, 6, 12, and 24 h. All samples were incubated for 24 h. All samples were pre-aged with phosphate-buffered saline (PBS) for 48 h, 1 week, and 4 weeks. | In 48 h aged samples, there was a reduction in CFUs in 1, 2, 3, 4, and 5 wt % ZnO-NP composites compared to the control. However, there was no statistically significant difference between the 1, 2, 3, 4, and 5 wt % ZnO-NP composites. In the 1-week and 4-week aged samples, there was no statistically significant difference between the 1, 2, 3, 4, and 5 wt % ZnO-NP composites and the control. | |||
| Agar diffusion test | The inhibition zones around the composite discs were measured after 24 h incubation of bacteria inoculated BHI agar plates. | There were no inhibition zones around any of the composite resin discs containing ZnO-NPs or the control composite resin discs. | |||
| Scanning electron microscopy (SEM) of direct contact test | Qualitative description of visualized samples of composite discs via SEM. Age of S. Mutans biofilms were 1 h and 24 h. | For 1 h incubated samples, there was a qualitatively lower number of and smaller bacterial colonies in composite resins containing higher concentration of ZnO-NPs (3, 4 and 5 wt %) compared to the composite resins containing a lower concentration of ZnO-NPs (0, 1, and 2 wt %). The results were similar for samples incubated for 24 h. | |||
| Kasraei et al. (2014) [31] | Flowable composite resin (Opallis) | 1 wt % ZnO-NPs (50 nm) in flowable composite resin | Direct contact test | Visual counting of number of viable CFUs after 48 h. Age of S. Mutans or Lactobacillus biofilms were 12 h for both. | There was a reduction in CFUs of in both the S. mutans and Lactobacillus groups, for the 1% ZnO-NP composites compared to control. |
| Brandão et al. (2017) [32] | Model composite resin prepared by researchers (BisGMA 70 wt % and TEGDMA 30 wt %; 70% barium borosilicate glass filler) | 0.5, 1, 2, 5, and 10 wt % ZnO-NPs (40–100 nm) in model composite resin. | Evaluation of metabolic activity via an MTT [3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide] assay | Based on the enzymatic reduction of yellow tetrazolium into purple formazan. Absorbance values of samples were recorded using a microplate reader (540 nm). Age of S. Mutans biofilm was 72 h. | One, 2, 5, and 10 wt % ZnO-NP composites decreased the metabolic activity of the S. mutans biofilm compared to the control. The 0.5 wt % ZnO-NP composite did not show a statistically significant difference compared to the control. |
| Lactic acid production | Lactic acid analysis of 3 h incubated samples via the use of a lactate dehydrogenase (LDH) reaction (measured in µM). Age of S. mutans biofilm was 72 h. | Only 5 and 10 wt % ZnO-NP composites reduced the production of lactic acid by the S. mutans biofilm. | |||
| Scanning electron microscopy (SEM) of direct contact test | Qualitative description of visualized samples of composite discs via SEM (5000× magnification). | A qualitative decrease in the number of bacterial colonies was noted in the 1, 2, 5, and 10 wt % ZnO-NP composites compared to control. There was a significant decrease in the number of colonies as ZnO-NP concentration increased. |
| Study | MINORS Item | Total Score | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||
| Sevinç et al. (2010) | 1 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 18 |
| Hojati et al. (2013) | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 19 |
| Kasraei et al. (2014) | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 19 |
| Brandão et al. (2017) | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arun, D.; Adikari Mudiyanselage, D.; Gulam Mohamed, R.; Liddell, M.; Monsur Hassan, N.M.; Sharma, D. Does the Addition of Zinc Oxide Nanoparticles Improve the Antibacterial Properties of Direct Dental Composite Resins? A Systematic Review. Materials 2021, 14, 40. https://doi.org/10.3390/ma14010040
Arun D, Adikari Mudiyanselage D, Gulam Mohamed R, Liddell M, Monsur Hassan NM, Sharma D. Does the Addition of Zinc Oxide Nanoparticles Improve the Antibacterial Properties of Direct Dental Composite Resins? A Systematic Review. Materials. 2021; 14(1):40. https://doi.org/10.3390/ma14010040
Chicago/Turabian StyleArun, Divya, Dulanja Adikari Mudiyanselage, Rumana Gulam Mohamed, Michael Liddell, Nur Mohammad Monsur Hassan, and Dileep Sharma. 2021. "Does the Addition of Zinc Oxide Nanoparticles Improve the Antibacterial Properties of Direct Dental Composite Resins? A Systematic Review" Materials 14, no. 1: 40. https://doi.org/10.3390/ma14010040
APA StyleArun, D., Adikari Mudiyanselage, D., Gulam Mohamed, R., Liddell, M., Monsur Hassan, N. M., & Sharma, D. (2021). Does the Addition of Zinc Oxide Nanoparticles Improve the Antibacterial Properties of Direct Dental Composite Resins? A Systematic Review. Materials, 14(1), 40. https://doi.org/10.3390/ma14010040