1. Introduction
The introduction of Charnley’s low friction arthroplasty was a technological revolution and has become the most successful total hip arthroplasty (THA) [
1]. Charnley made three major contributions to the evolution of THA: (1) the concept of low friction torque arthroplasty, (2) the use of acrylic cement to fix components to living bone, and (3) the introduction of high-density polyethylene as a bearing material [
2]. The excellent clinical long-term results of Charnley’s low friction arthroplasty have been reported in many studies [
3,
4], and the fundamental concepts of Charnley’s THA still exist today. The Exeter (Stryker, Mahwah, NJ, USA) is a new stem with a collarless tapered shape that was introduced because the existing collars could not regularly and reliably transmit load to the femoral neck. The taper-slip concept allows the stem to subside and become lodged as a wedge in the cement mantle during loading [
5]. In vitro, polished stems have been shown to provide greater potential to develop “taper-lock” fixation [
6,
7] and stem subsidence in polished stems results in compressive force on cement and cement creep [
8]. Ling et al. reported 94% survival of the original Exeter stem at a 35 years follow up, with aseptic loosening as the endpoint [
9]. Currently, “collarless, tapered, polished” stems have become widely used and they are considered the “golden standard” of cemented stems. In short, the design of cemented stems involves two concepts: a composite-beam or shape-closed design originated by Charnley and a taper-slip or force-closed design rooted in Exeter [
10].
Periprosthetic femoral fractures (PPFs) following THA are devastating complications that are associated with functional limitations and increased overall mortality [
11]. The Nordic Arthroplasty Register Association database reported a 7-fold increase in the incidence of PPF with uncemented stems compared to cemented stems [
12], despite the fact that use of uncemented fixation in THA is increasing worldwide [
13]. However, with cemented stems, some authors have reported that the risk of PPF for taper-slip stems was high compared to composite-beam stems and that there was a difference among taper-slip stems [
12,
14,
15,
16]. Using the Exeter or CPT (Zimmer, Warsaw, IN, USA) stem, Grammatopoulos et al. demonstrated the different fracture patterns among well-fixed cemented taper-slip stems and highlighted a specific fracture pattern with both splitting and spiral elements [
17]. Biomechanically, the C-stem (DePuy International, Leeds, UK) and the CPT stem created a different fracture pattern under the same loading condition [
18]. These results enable speculation that the excessive taper-slip possibly causes PPF, although experimentally, the taper-slip stem can support substantially greater loads before failure than the composite beam [
19]. Furthermore, the effect of the surface appearance on the stem–cement interface may be different for each metal because the subsidence is different for each taper-slip stem and the metal implant surface appearance is only defined by human beings [
20,
21]. The question “what is polished?” is ultimately posed and there have been a few reports that have specifically assessed the effect of the polished material on the stem–cement interface. The aim of this study was to evaluate the relationship between the surface roughness of metallic material and bone cement. We hypothesised that the effect of the surface appearance on the stem–cement interface will be different for each metal, even if the roughness of the implant surface is equal.
4. Discussion
Types of cemented stem fixation are classified as composite-beam design and taper-slip design [
10]. Implants relying on a composite beam principle typically have a “satin” or “matte” surface finish to maximise the mechanical strength of the bond between the cement mantle and the stem. The taper-slip concept uses a dual-tapered or triple-tapered stem geometry typically with a “smooth” or “polished” surface finish allowing the implant to wedge into the cement mantle [
25]. However, the effect of the surface appearance on the stem–cement interface may be different for each metal because the extent of subsidence is extremely sensitive to interface friction [
26]. For the taper-slip design, the adequacy and safety of the “polished” surface finish of each metal remains unknown, with the average surface roughness (Ra, μm) of “polish” ranging from 0 to 0.1 (
Table 5). Therefore, we assessed the effect of metallic surface roughness on the bone cement.
Commonly, there are three types of materials that are used for cemented stems—CoCr alloy, SUS, and titanium alloy. In polished stems, stems made of titanium alloy are not favoured because they are associated with early failure and two disadvantages: a stiffness of about 50% of that of CoCr alloy or SUS and a susceptibility of the material to crevice corrosion [
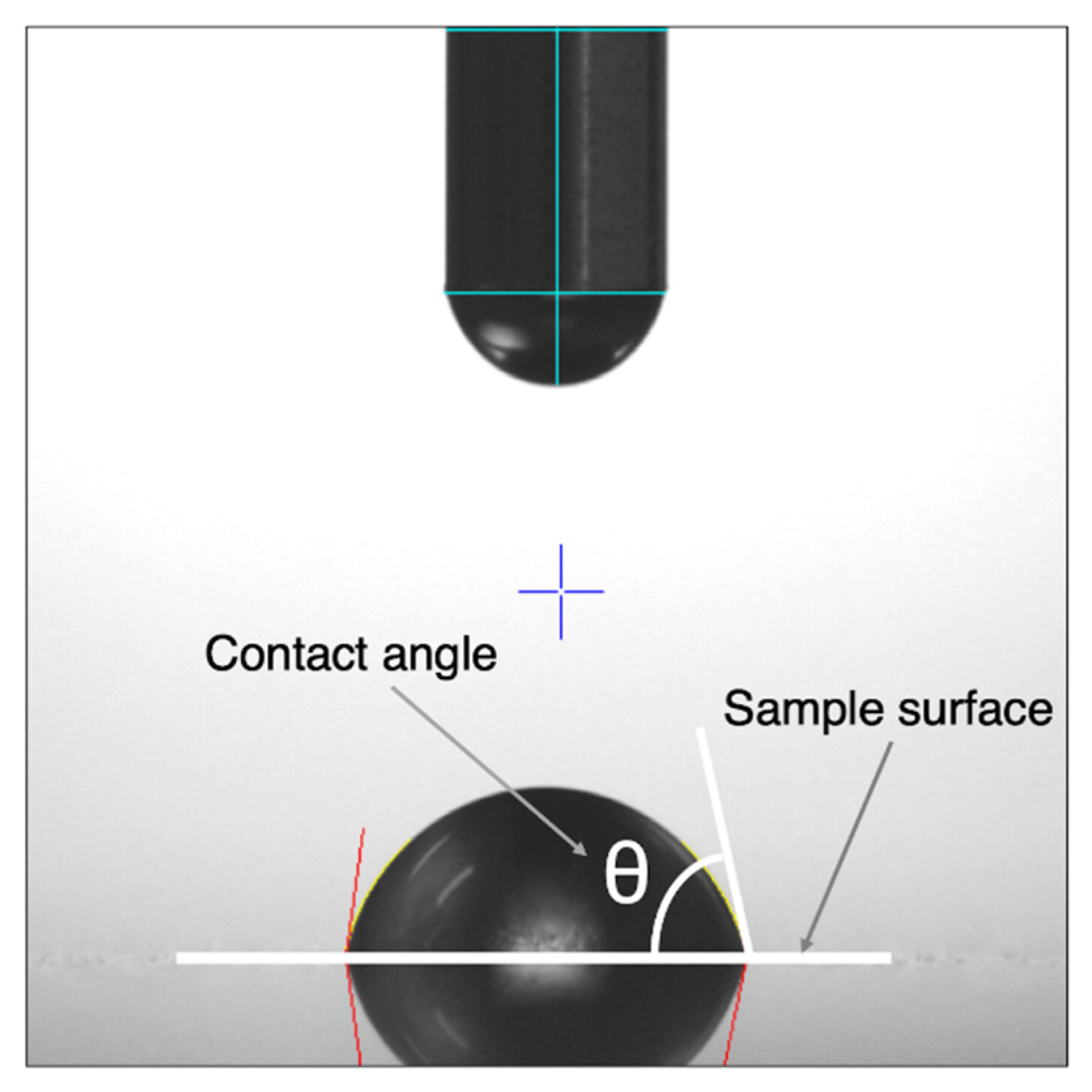
27]. Conversely, CoCr alloy has been considered to behave similarly to SUS because they have a similar Young’s modulus and Poisson coefficient. However, Borruto et al. demonstrated that the surface wettability of the material has an effect on friction factors and the different surface wettability causes a different distribution of the drops of water [
22]. Indeed, in this study, the hydrophobic nature of each metal increased with decreasing surface roughness because the contact angle of each metal increased with decreasing surface roughness. This means that the surface wettability of a metal is decreased in accordance with greater polishing. With a surface roughness of Ra = 0.06 μm, the contact angle of CoCr was larger than that of SUS. Consequently, CoCr had a lower surface wettability than SUS and tended not to adhere to bone cement. Furthermore, with a surface roughness of Ra = 0.06 μm, the frictional coefficient of CoCr was lower than that of SUS, particularly when using Endurance. These results indicate that, in CoCr, the low adhesion effect with low frictional coefficient may result in the excessive taper-slip. Using imitated stems made of CoCr (Ra < 0.02 μm) and SUS (Ra < 0.02 μm), Tsuda also demonstrated that the subsidence into the bone cement was significantly greater in CoCr than SUS [
28]. He concluded that CoCr alloy and SUS alloy showed different mechanical behaviour within the bone cement and this difference can be caused by a difference in surface wettability between the two materials. In addition, Nelissen et al. reported that at the 2 year follow-up, the subsidence of the Exeter stem using low viscosity bone cement was greater than with high viscosity bone cement [
29]. Although there were no differences in clinical revision rates based on viscosity [
30], bone cement viscosity affected the frictional coefficient of the surface roughness in the current study. Excessively “polished” CoCr may not be compatible with the stem–cement interface using moderate viscosity bone cement.
Clinically, there is a difference among taper-slip stems in terms of the incidence of PPF. According to the National Joint Registry of England, Wales, and Northern Ireland database on 257,202 THAs, analysis of the four cemented femoral stem brands showed a PPF incidence of 0.12% in Exeter V40, 0.07% in the Charnley stem (DePuy International, Leeds, UK), 0.46% in the CPT stem, and 0.14% in the C-stem [
16]. The incidence was lowest with the composite-beam stem (Charnley stem) and, of note, the PPF incidence with a CPT stem was the highest. Other authors have also reported that CPT stems are associated with a higher incidence of PPF [
15,
31]. The list of the major available cemented stems is shown in
Table 6 and, of the taper-slip stems, only the CPT stem is made of CoCr. Although the difference in stem design may be involved in the higher incidence of PPF, the stem material or surface finish may also be one of the causes of PPF. A polish-tapered stem made of CoCr potentially results in PPF.
Some limitations of our study must be noted. First, the sample size was small. Although statistically significant data were acquired, the Ra parameters that could be compared were limited. Ideally, more samples should have been included. Second, the frictional coefficient between the metal and bone cement is dependent on the environment, that is, whether the condition is wet or dry [
32]. In this study, however, only saline was used to simulate the body environment in both experiments. Furthermore, the surface finish of the pin made by bone cement could not be evaluated because the diameter was 5 mm and, therefore, too small. Third, this study was a biomaterial study, so results could differ in clinical practice. In order to confirm the relationship between the surface roughness of metallic material and bone cement, a biomechanical study, including a stem subsidence test and torsional stability test at a variety of degrees of surface roughness, should be considered.


 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}