
Evaluation of Stress Distribution during Insertion of Tapered Dental Implants in Various Osteotomy Techniques: Three-Dimensional Finite Element Study

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
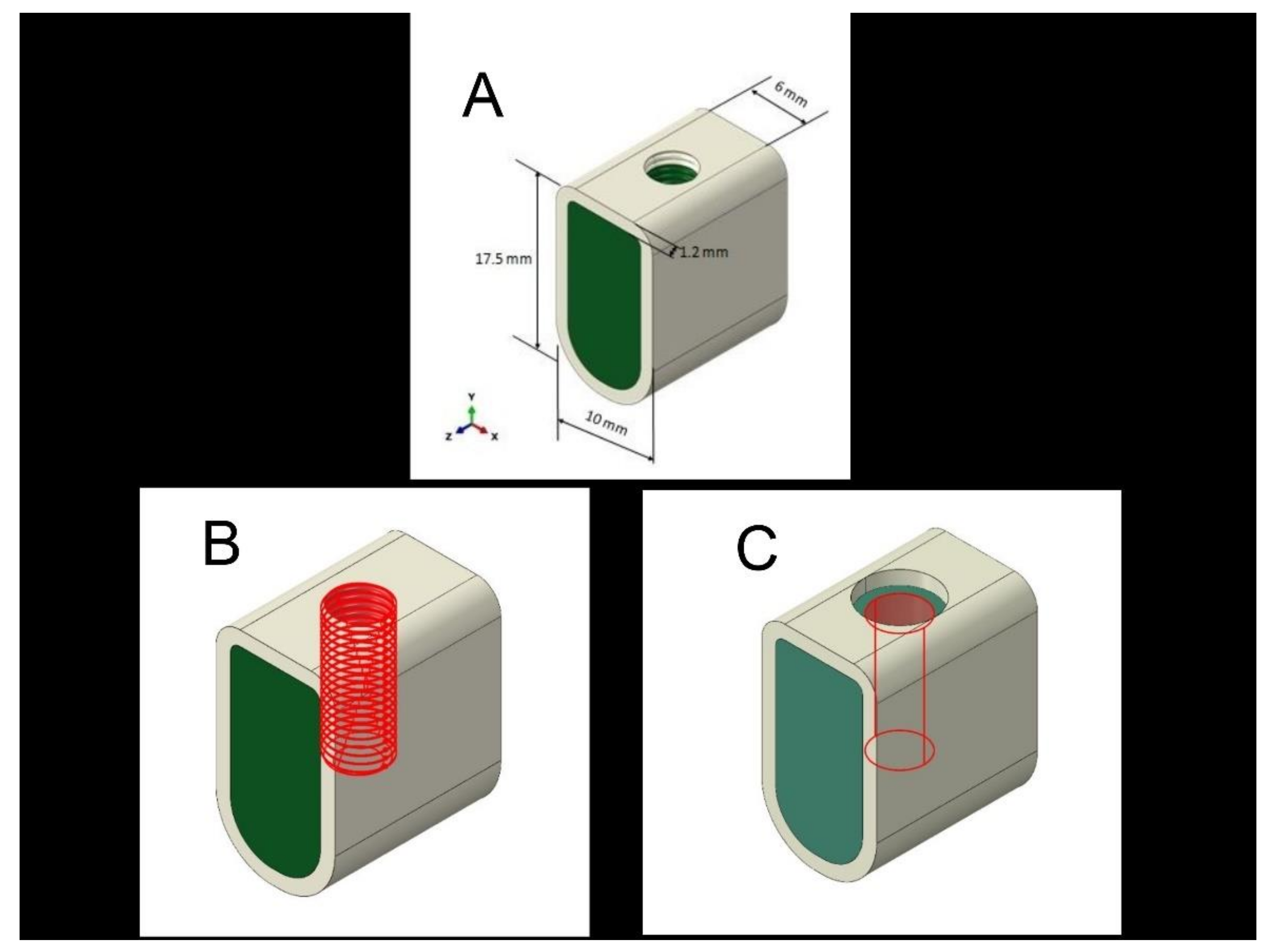
2.1. Preparation of Models
2.2. Structure of FEM
2.3. Simulation of the Implant Insertion
2.4. Stress Measurement
2.5. Statistical Analysis
3. Results
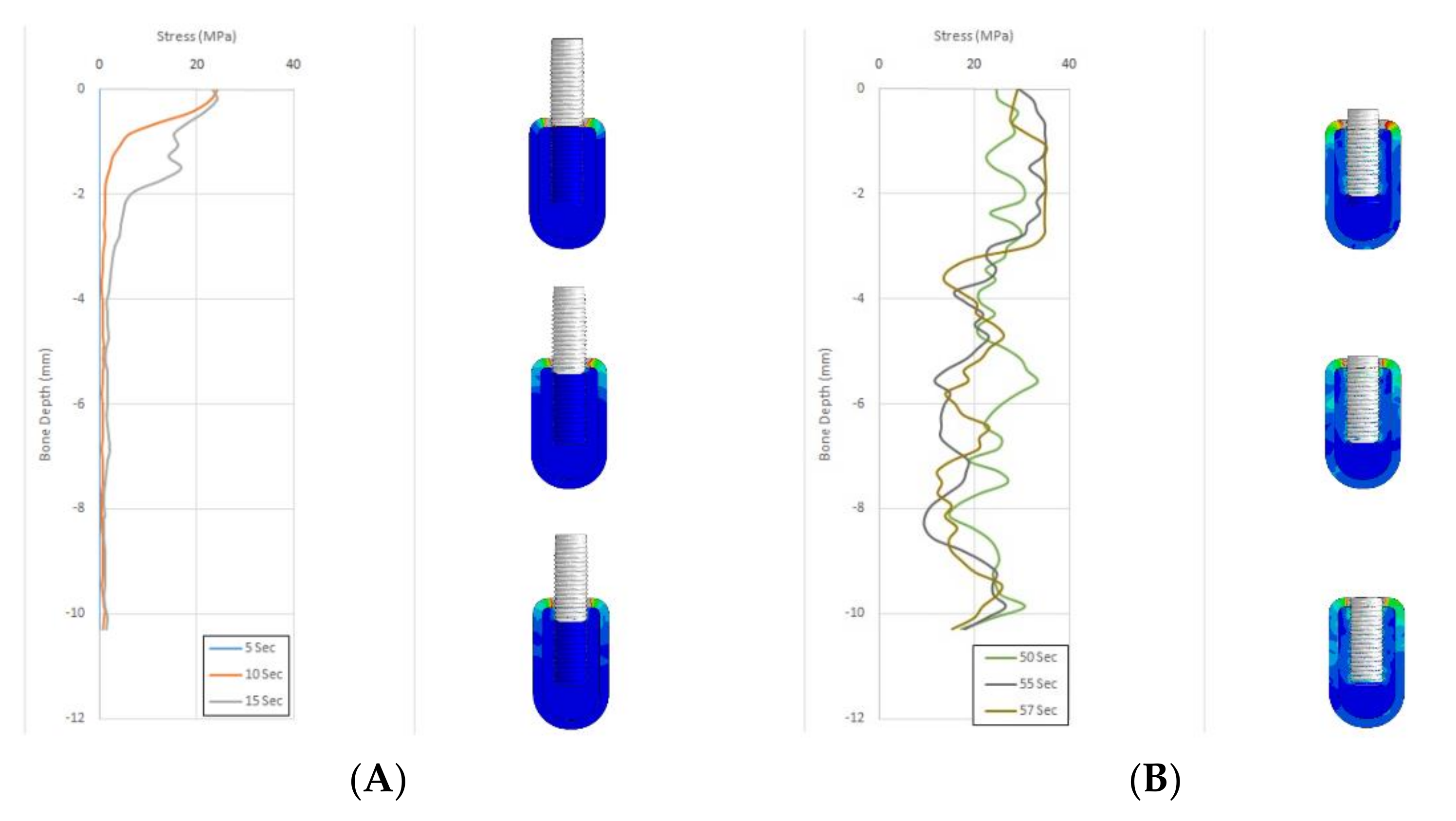
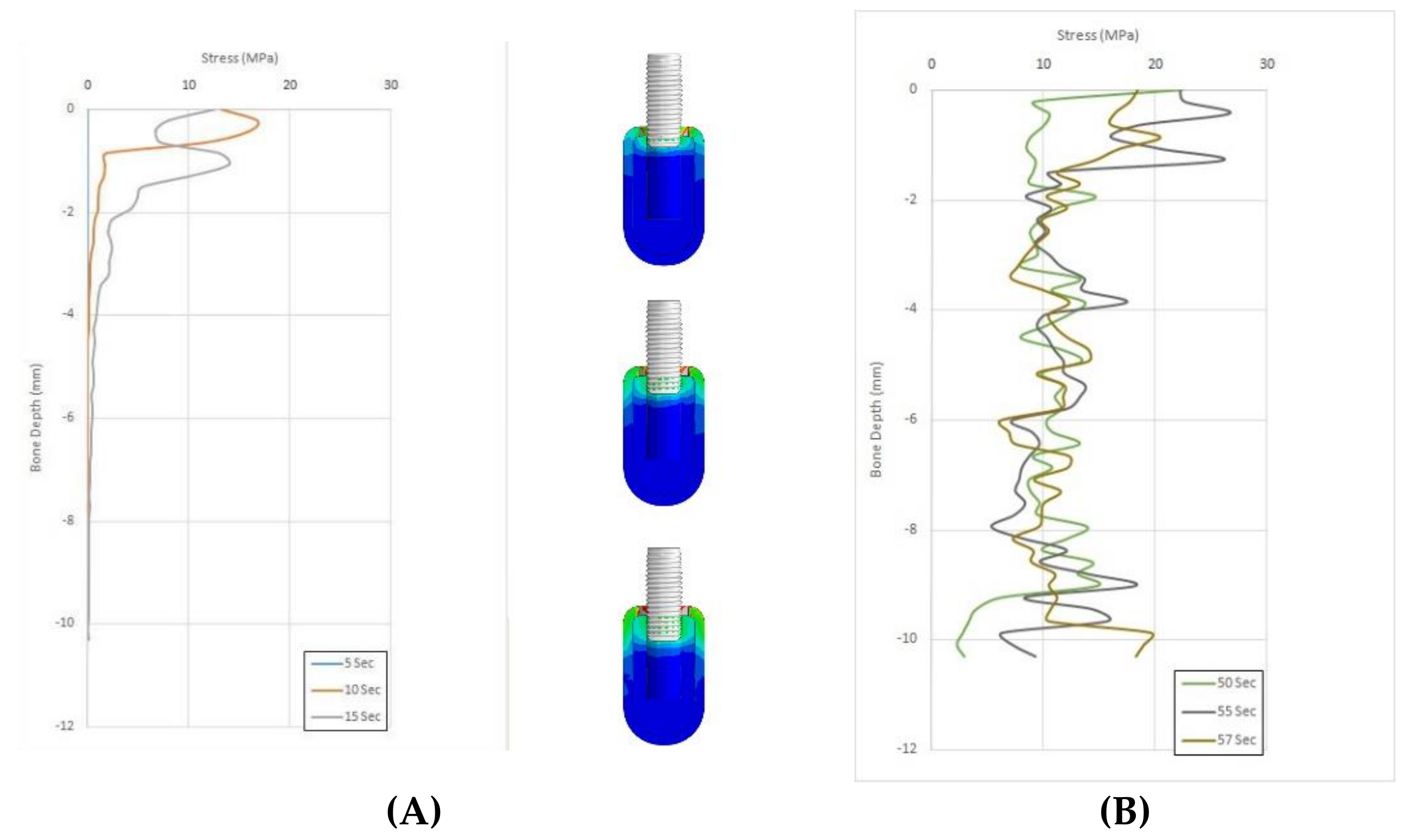
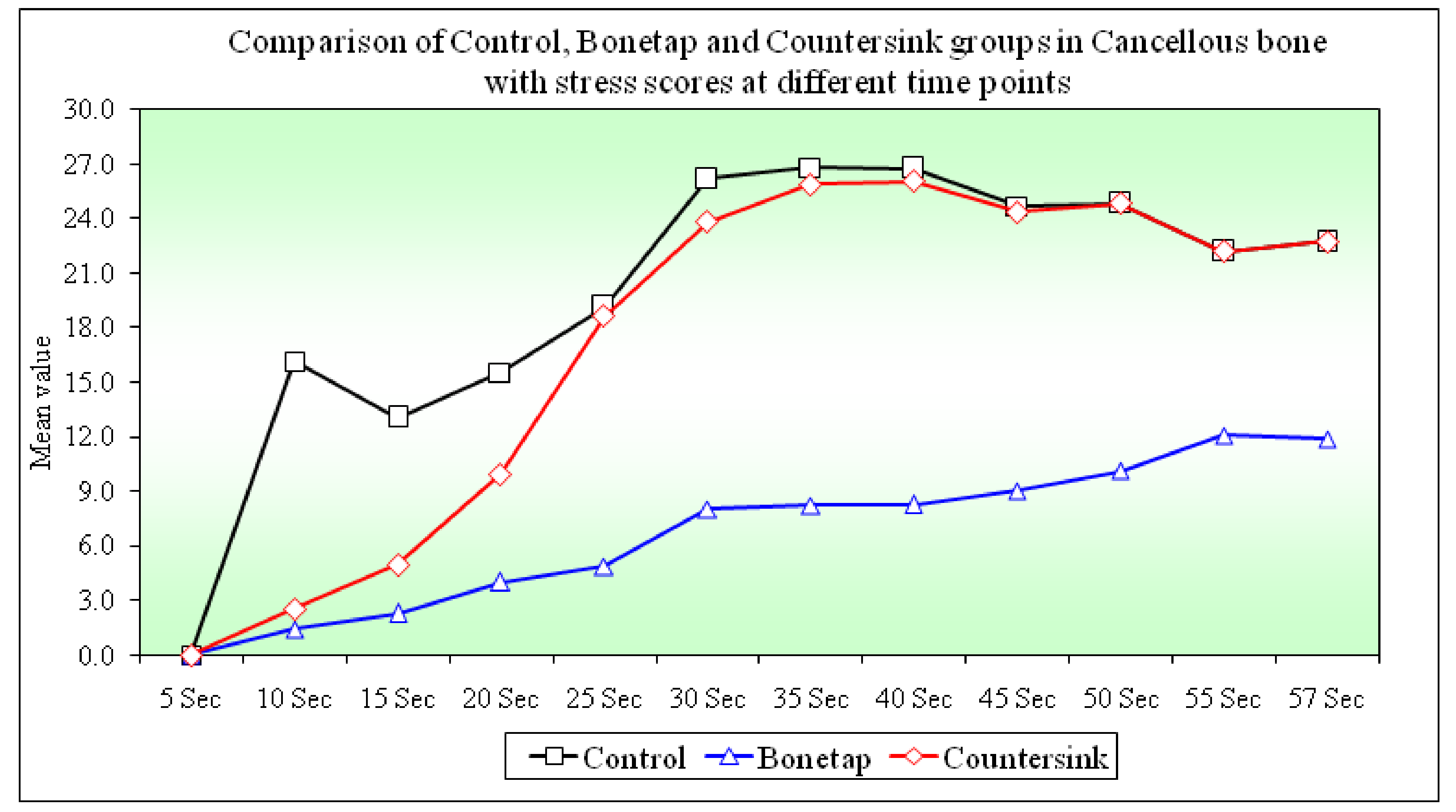
3.1. Comparison of Stress Scores in the Cancellous Bone between B1, B2, and B3 Groups at Different Time Points
3.2. Evaluation of Stress Scores in the Cancellous Bone between B1, B2, and B3 Groups at Different Time Points Compared with 10 s as the Time Interval
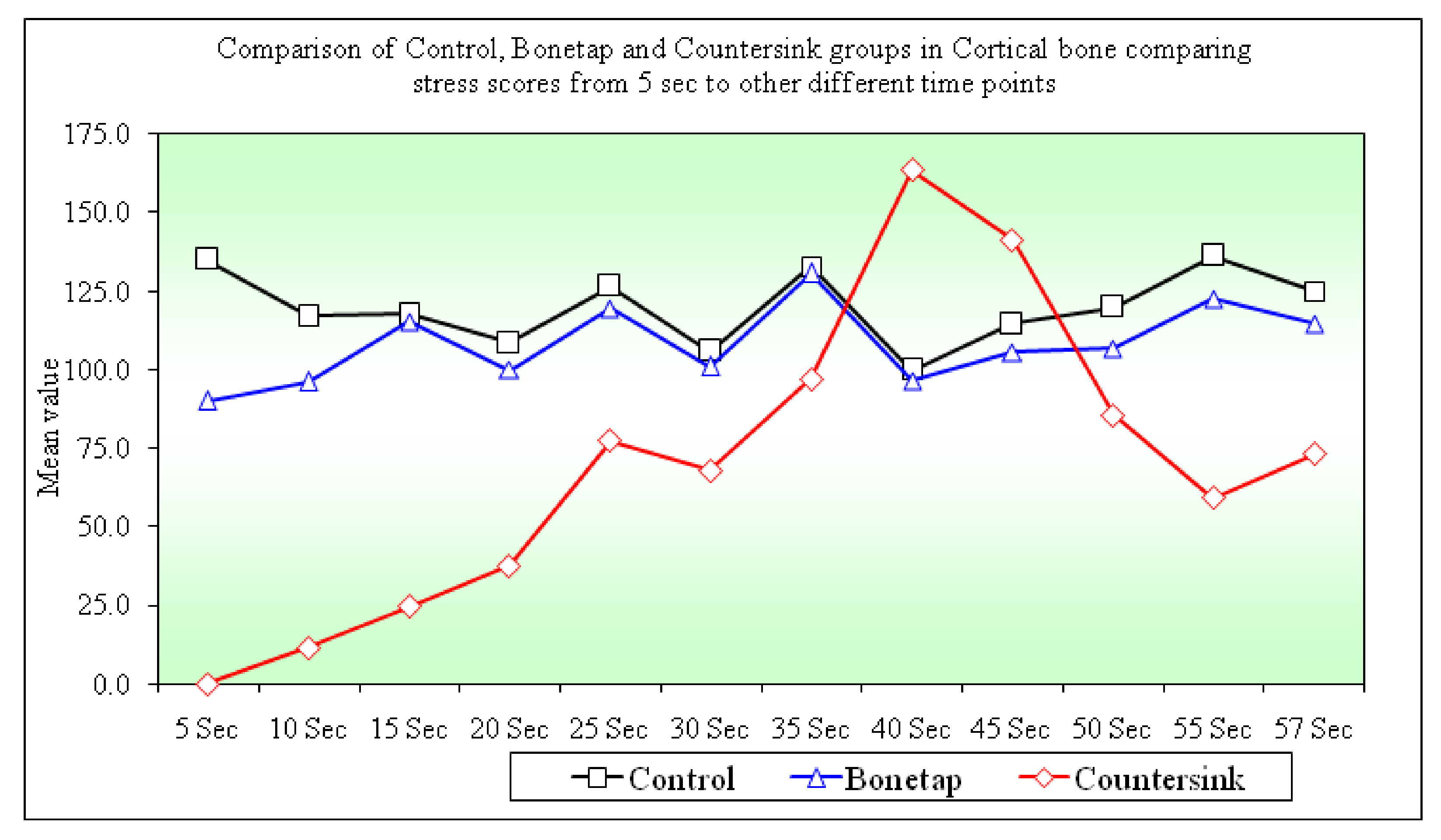
3.3. Comparison of Stress Scores in the Cortical Bone between B1, B2, and B3 Groups at Different Time Points
3.4. Evaluation of Stress Scores in the Cortical Bone between B1, B2, and B3 Groups at Different Time Points Compared with 5 s as the Time Interval
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Oftadeh, R.; Perez-Viloria, M.; Villa-Camacho, J.C.; Vaziri, A.; Nazarian, A. Biomechanics and Mechanobiology of Trabecular Bone: A Review. J. Biomech. Eng. 2015, 137. [Google Scholar] [CrossRef] [Green Version]
- Glauser, R.; Sennerby, L.; Meredith, N.; Rée, A.; Lundgren, A.; Gottlow, J.; Hämmerle, C.H.F. Resonance Frequency Analysis of Implants Subjected to Immediate or Early Functional Occlusal Loading. Successful vs. Failing Implants. Clin. Oral Implant. Res. 2004, 15, 428–434. [Google Scholar] [CrossRef]
- Amini, A.R.; Laurencin, C.T.; Nukavarapu, S.P. Bone Tissue Engineering: Recent Advances and Challenges. Crit. Rev. Biomed. Eng. 2012, 40, 363–408. [Google Scholar] [CrossRef] [Green Version]
- Kuzyk, P.R.; Schemitsch, E.H. The Basic Science of Peri-Implant Bone Healing. Indian J. Orthop. 2011, 45, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Kapoor, D. The Dynamic Interface: A Review. J. Int. Soc. Prev. Community Dent. 2015, 5, 354–358. [Google Scholar] [CrossRef] [Green Version]
- Brisman, D.L. The Effect of Speed, Pressure, and Time on Bone Temperature during the Drilling of Implant Sites. Int. J. Oral Maxillofac. Implant. 1996, 11, 35–37. [Google Scholar]
- Manz, M.C. Radiographic Assessment of Peri-Implant Vertical Bone Loss: DICRG Interim Report No. 9. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 1997, 55, 62–71. [Google Scholar] [CrossRef]
- Hoar, J.E.; Beck, G.H.; Crawford, E.A.; Resnik, R. Prospective Evaluation of Crestal Bone Remodeling of a Bone Density Based Dental System. Compend. Contin. Educ. Dent. 1998, 19, 17–24. [Google Scholar]
- Brand, R.A. Biographical Sketch: Julius Wolff, 1836-1902. Clin. Orthop. Relat. Res. 2010, 468, 1047–1049. [Google Scholar] [CrossRef] [Green Version]
- Mavčič, B.; Antolič, V. Optimal Mechanical Environment of the Healing Bone Fracture/Osteotomy. Int. Orthop. 2012, 36, 689–695. [Google Scholar] [CrossRef] [Green Version]
- Geng, J.P.; Tan, K.B.; Liu, G.R. Application of Finite Element Analysis in Implant Dentistry: A Review of the Literature. J. Prosthet. Dent. 2001, 85, 585–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chand, Y.B.; Mahendra, J.; Jigeesh, N.; Mahendra, L.; Shivasubramanian, L.; Perika, S.B. Comparison of Stress Distribution and Deformation of Four Prosthetic Materials in Full-Mouth Rehabilitation with Implants: A Three-Dimensional Finite Element Study. J. Contemp. Dent. Pract. 2020, 21, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Bennardo, F.; Brancaccio, Y.; Barone, S.; Femiano, F.; Nucci, L.; Minervini, G.; Fortunato, L.; Attanasio, F.; Giudice, A. Can Bone Compaction Improve Primary Implant Stability? An In Vitro Comparative Study with Osseodensification Technique. Appl. Sci. 2020, 10, 8623. [Google Scholar] [CrossRef]
- Kosior, P.; Kuropka, P.; Janeczek, M.; Mikulewicz, M.; Zakrzewski, W.; Dobrzyński, M. The Influence of Various Preparation Parameters on the Histological Image of Bone Tissue during Implant Bed Preparation—An In Vitro Study. Appl. Sci. 2021, 11, 1916. [Google Scholar] [CrossRef]
- Djebbar, N.; Serier, B.; Bouiadjra, B.B.; Benbarek, S.; Drai, A. Analysis of the Effect of Load Direction on the Stress Distribution in Dental Implant. Mater. Des. 2010, 31, 2097–2101. [Google Scholar] [CrossRef]
- Quaresma, S.E.T.; Cury, P.R.; Sendyk, W.R.; Sendyk, C. A Finite Element Analysis of Two Different Dental Implants: Stress Distribution in the Prosthesis, Abutment, Implant, and Supporting Bone. J. Oral Implantol. 2008, 34, 1–6. [Google Scholar] [CrossRef]
- Eskitascioglu, G.; Usumez, A.; Sevimay, M.; Soykan, E.; Unsal, E. The Influence of Occlusal Loading Location on Stresses Transferred to Implant-Supported Prostheses and Supporting Bone: A Three-Dimensional Finite Element Study. J. Prosthet. Dent. 2004, 91, 144–150. [Google Scholar] [CrossRef]
- Yemineni, B.C.; Mahendra, J.; Nasina, J.; Mahendra, L.; Shivasubramanian, L.; Perika, S.B. Evaluation of Maximum Principal Stress, Von Mises Stress, and Deformation on Surrounding Mandibular Bone During Insertion of an Implant: A Three-Dimensional Finite Element Study. Cureus 2020, 12, e9430. [Google Scholar] [CrossRef]
- Ryu, H.-S.; Namgung, C.; Lee, J.-H.; Lim, Y.-J. The Influence of Thread Geometry on Implant Osseointegration under Immediate Loading: A Literature Review. J. Adv. Prosthodont. 2014, 6, 547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herekar, M.G.; Patil, V.N.; Mulani, S.S.; Sethi, M.; Padhye, O. The Influence of Thread Geometry on Biomechanical Load Transfer to Bone: A Finite Element Analysis Comparing Two Implant Thread Designs. Dent. Res. J. 2014, 11, 489–494. [Google Scholar]
- Menaka, R.; Ramamurthy, K. A Novel Feature Extraction Scheme for Visualisation of 3D Anatomical Structures. Int. J. Biomed. Eng. Technol. 2016, 21, 49. [Google Scholar] [CrossRef]
- Paracchini, L.; Barbieri, C.; Redaelli, M.; Di Croce, D.; Vincenzi, C.; Guarnieri, R. Finite Element Analysis of a New Dental Implant Design Optimized for the Desirable Stress Distribution in the Surrounding Bone Region. Prosthesis 2020, 2, 225–236. [Google Scholar] [CrossRef]
- El–said, S.A. 3D Medical Image Segmentation Technique. Int. J. Biomed. Eng. Technol. 2015, 17, 232–251. [Google Scholar] [CrossRef]
- Cook, S.D.; Klawitter, J.J.; Weinstein, A.M. The Influence of Implant Geometry on the Stress Distribution around Dental Implants. J. Biomed. Mater. Res. 1982, 16, 369–379. [Google Scholar] [CrossRef]
- Di Stefano, D.A.; Perrotti, V.; Greco, G.B.; Cappucci, C.; Arosio, P.; Piattelli, A.; Iezzi, G. The Effect of Undersizing and Tapping on Bone to Implant Contact and Implant Primary Stability: A Histomorphometric Study on Bovine Ribs. J. Adv. Prosthodont. 2018, 10, 227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burger, E.H.; Klein-Nulend, J. Mechanotransduction in bone—Role of the lacunocanalicular network. FASEB J. 1999, 13, S101–S112. [Google Scholar]
- Burstein, A.H.; Reilly, D.T.; Martens, M. Aging of bone tissue: Mechanical properties. J. Bone Jt. Surg. Am. Vol. 1976, 58, 82–86. [Google Scholar]
- Cowin, S.C.; Moss-Salentijn, L.; Moss, M.L. Candidates for the Mechanosensory System in Bone. J. Biomech. Eng. 1991, 113, 191–197. [Google Scholar] [CrossRef]
- Tanaka, M.; Sawaki, Y.; Niimi, A.; Kaneda, T. Effects of Bone Tapping on Osseointegration of Screw Dental Implants. Int. J. Oral Maxillofac. Implant. 1994, 9, 541–547. [Google Scholar]
- Natali, A.N.; Carniel, E.L.; Pavan, P.G. Dental Implants Press Fit Phenomena: Biomechanical Analysis Considering Bone Inelastic Response. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2009, 25, 573–581. [Google Scholar] [CrossRef]
- Natali, A.N.; Carniel, E.L.; Pavan, P.G. Investigation of Viscoelastoplastic Response of Bone Tissue in Oral Implants Press Fit Process. J. Biomed. Mater. Res. Part B Appl. Biomater 2009, 91, 868–875. [Google Scholar] [CrossRef]
- Aslam, A.; Hassan, S.H.; Aslam, H.M.; Khan, D.A. Effect of Platform Switching on Peri-Implant Bone: A 3D Finite Element Analysis. J. Prosthet. Dent. 2019, 121, 935–940. [Google Scholar] [CrossRef]
- Niroomand, M.R.; Arabbeiki, M. Implant Stability in Different Implantation Stages: Analysis of Various Interface Conditions. Inform. Med. Unlocked 2020, 19, 100317. [Google Scholar] [CrossRef]
- Li, J.; Jansen, J.A.; Walboomers, X.F.; van den Beucken, J.J. Mechanical Aspects of Dental Implants and Osseointegration: A Narrative Review. J. Mech. Behav. Biomed. Mater. 2020, 103, 103574. [Google Scholar] [CrossRef] [PubMed]
- Steigenga, J.T.; Al-Shammari, K.F.; Nociti, F.H.; Misch, C.E.; Wang, H.-L. Dental Implant Design and Its Relationship to Long-Term Implant Success. Implant Dent. 2003, 12, 306–317. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Steignga, J.; Barboza, E.; Misch-Dietsh, F.; Cianciola, L.J.; Kazor, C. Short Dental Implants in Posterior Partial Edentulism: A Multicenter Retrospective 6-Year Case Series Study. J. Periodontol. 2006, 77, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Zhou, Y.; Zhou, J.; Xu, M.; Zheng, W.; Huang, W.; Zhou, W.; Shen, Y.; Zhao, K.; Wu, Y.; et al. Comparison of Intraoral Bone Regeneration with Iliac and Alveolar BMSCs. J. Dent. Res. 2018, 97, 1229–1235. [Google Scholar] [CrossRef]
- Gümrükçü, Z.; Korkmaz, Y.T.; Korkmaz, F.M. Biomechanical Evaluation of Implant-Supported Prosthesis with Various Tilting Implant Angles and Bone Types in Atrophic Maxilla: A Finite Element Study. Comput. Biol. Med. 2017, 86, 47–54. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Young’s Modulus (in GPa) | Poisson’s Ratio | Density (in g/cm3) | Tensile Yield Strength (in MPa) | Compressive Yield Strength (in MPa) | |
|---|---|---|---|---|---|
| Cortical bone | 15 | 0.35 | 1.5 | 115 | 182 |
| Cancellous bone | 6 | 0.30 | 0.67 | 32.4 | 51 |
| Titanium implant | 113 | 0.30 | 4.54 | 830 | 830 |
| Timepoint (Seconds) | B1 | B2 | B3 | Pair-Wise Comparisons | ||
|---|---|---|---|---|---|---|
| B1 vs. B2 | B1 vs. B3 | B2 vs. B3 | ||||
| 10 | 16.16 ±35.93 | 1.42 ± 3.98 | 2.55 ± 5.37 | 0.0001 * | 0.3080 | 0.0001 * |
| 30 | 26.19 ± 7.28 | 8.03 ± 7.77 | 23.82 ± 5.56 | 0.0001 * | 0.0700 | 0.0001 * |
| 57 | 22.73 ± 7.60 | 11.86 ± 3.55 | 22.73 ± 7.60 | 0.0001 * | 1.0000 | 0.0001 * |
| Time Interval (Seconds) | B1 | B2 | B3 | Pair-Wise Comparisons | ||
|---|---|---|---|---|---|---|
| B1 vs. B2 | B1 vs. B3 | B2 vs. B3 | ||||
| 10 to 15 | 3.10 ± 10.53 | 0.86 ± 3.44 | 2.44 ± 3.51 | 0.4300 | 0.0020 | 0.0001 * |
| 10 to 30 | 10.02 ± 33.81 | 6.61 ± 7.82 | 21.27 ± 6.81 | 0.0001 * | 0.8230 | 0.0001 * |
| 10 to 57 | 6.56 ± 33.28 | 10.44 ± 3.83 | 20.18 ± 7.82 | 0.0001 * | 0.1040 | 0.0001 * |
| Timepoint (Seconds) | B1 | B2 | B3 | Pair-Wise Comparisons | ||
|---|---|---|---|---|---|---|
| B1 vs. B2 | B1 vs. B3 | B2 vs. B3 | ||||
| 10 | 134.94 ± 20.68 | 90.14 ± 37.88 | 0.00 ± 0.00 | 0.0260 * | 0.0001 * | 0.0001 * |
| 30 | 105.99 ± 12.37 | 100.88 ± 10.39 | 67.94 ± 12.08 | 0.3680 | 0.0010 * | 0.0010 * |
| 57 | 125.03 ± 30.67 | 114.55 ± 28.63 | 73.16 ± 14.36 | 0.3680 | 0.0070 * | 0.0040 * |
| Time Interval (Seconds) | B1 | B2 | B3 | Pair-Wise Comparisons | ||
|---|---|---|---|---|---|---|
| B1 vs. B2 | B1 vs. B3 | B2 vs. B3 | ||||
| 5 to 10 | 17.89 ± 23.45 | 6.06 ± 31.61 | 11.39 ± 7.30 | 0.1010 | 0.0340 * | 0.9080 |
| 5 to 30 | 28.95 ± 18.55 | 10.74 ± 40.05 | 67.94 ± 12.08 | 0.0500 * | 0.0010 * | 0.0030 * |
| 5 to 57 | 9.90 ± 31.30 | 24.41 ± 45.88 | 73.16 ± 14.36 | 0.2660 | 0.0010 * | 0.0210 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahendra, J.; Chand, Y.B.; Mahendra, L.; Fageeh, H.N.; Fageeh, H.I.; Ibraheem, W.; Alzahrani, K.M.; Alqahtani, N.M.; Alahmari, N.M.; Almagbol, M.; et al. Evaluation of Stress Distribution during Insertion of Tapered Dental Implants in Various Osteotomy Techniques: Three-Dimensional Finite Element Study. Materials 2021, 14, 7547. https://doi.org/10.3390/ma14247547
Mahendra J, Chand YB, Mahendra L, Fageeh HN, Fageeh HI, Ibraheem W, Alzahrani KM, Alqahtani NM, Alahmari NM, Almagbol M, et al. Evaluation of Stress Distribution during Insertion of Tapered Dental Implants in Various Osteotomy Techniques: Three-Dimensional Finite Element Study. Materials. 2021; 14(24):7547. https://doi.org/10.3390/ma14247547
Chicago/Turabian StyleMahendra, Jaideep, Yemineni Bhavan Chand, Little Mahendra, Hytham N. Fageeh, Hammam Ibrahim Fageeh, Wael Ibraheem, Khaled M. Alzahrani, Nasser M. Alqahtani, Nasser Mesfer Alahmari, Mohammad Almagbol, and et al. 2021. "Evaluation of Stress Distribution during Insertion of Tapered Dental Implants in Various Osteotomy Techniques: Three-Dimensional Finite Element Study" Materials 14, no. 24: 7547. https://doi.org/10.3390/ma14247547
APA StyleMahendra, J., Chand, Y. B., Mahendra, L., Fageeh, H. N., Fageeh, H. I., Ibraheem, W., Alzahrani, K. M., Alqahtani, N. M., Alahmari, N. M., Almagbol, M., Robaian, A., Jigeesh, N., Varadarajan, S., Balaji, T. M., & Patil, S. (2021). Evaluation of Stress Distribution during Insertion of Tapered Dental Implants in Various Osteotomy Techniques: Three-Dimensional Finite Element Study. Materials, 14(24), 7547. https://doi.org/10.3390/ma14247547