
Effect of Different Surface Treatments on Repair Bond Strength of CAD/CAM Resin-Matrix Ceramics

Abstract
:1. Introduction
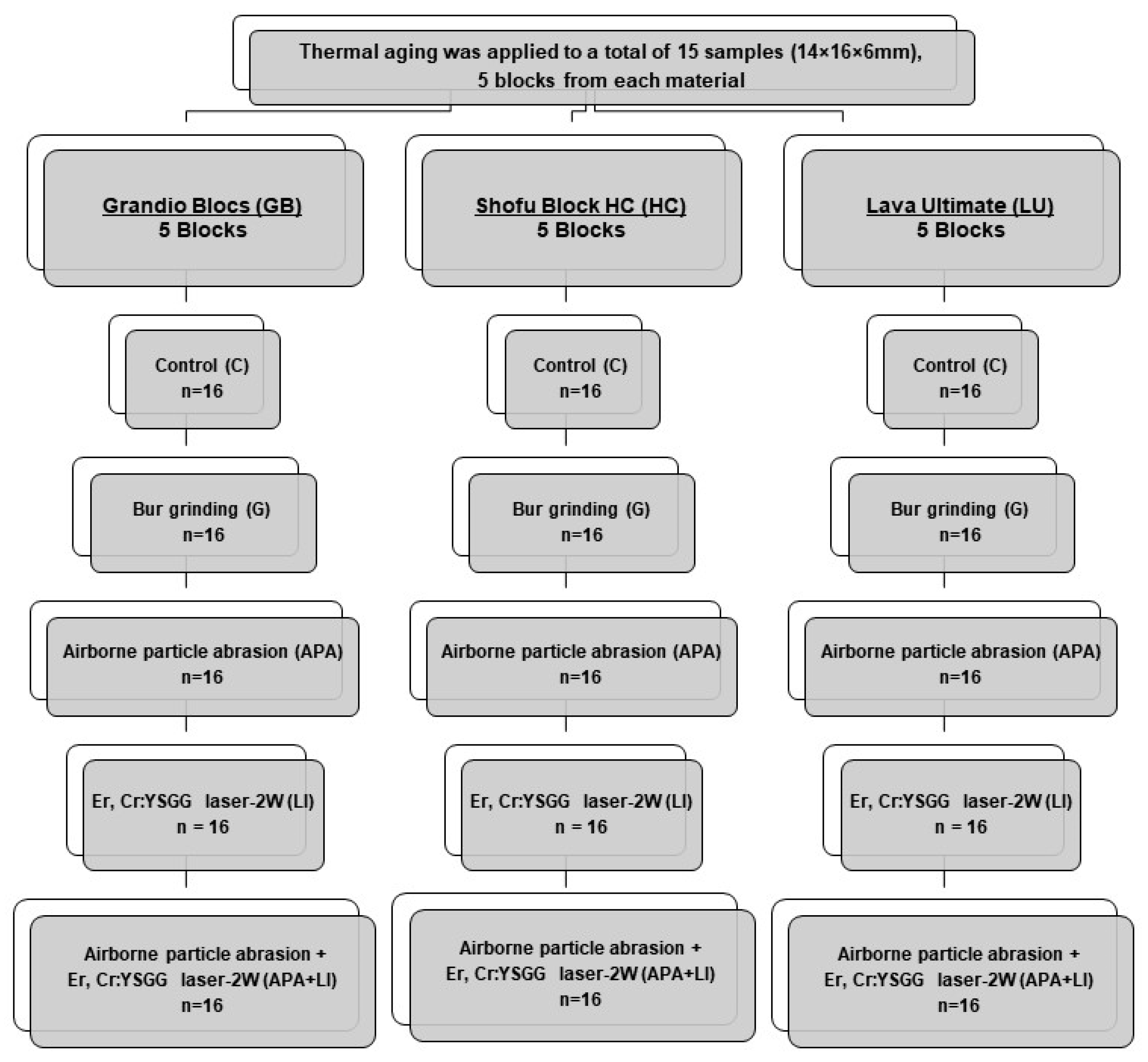
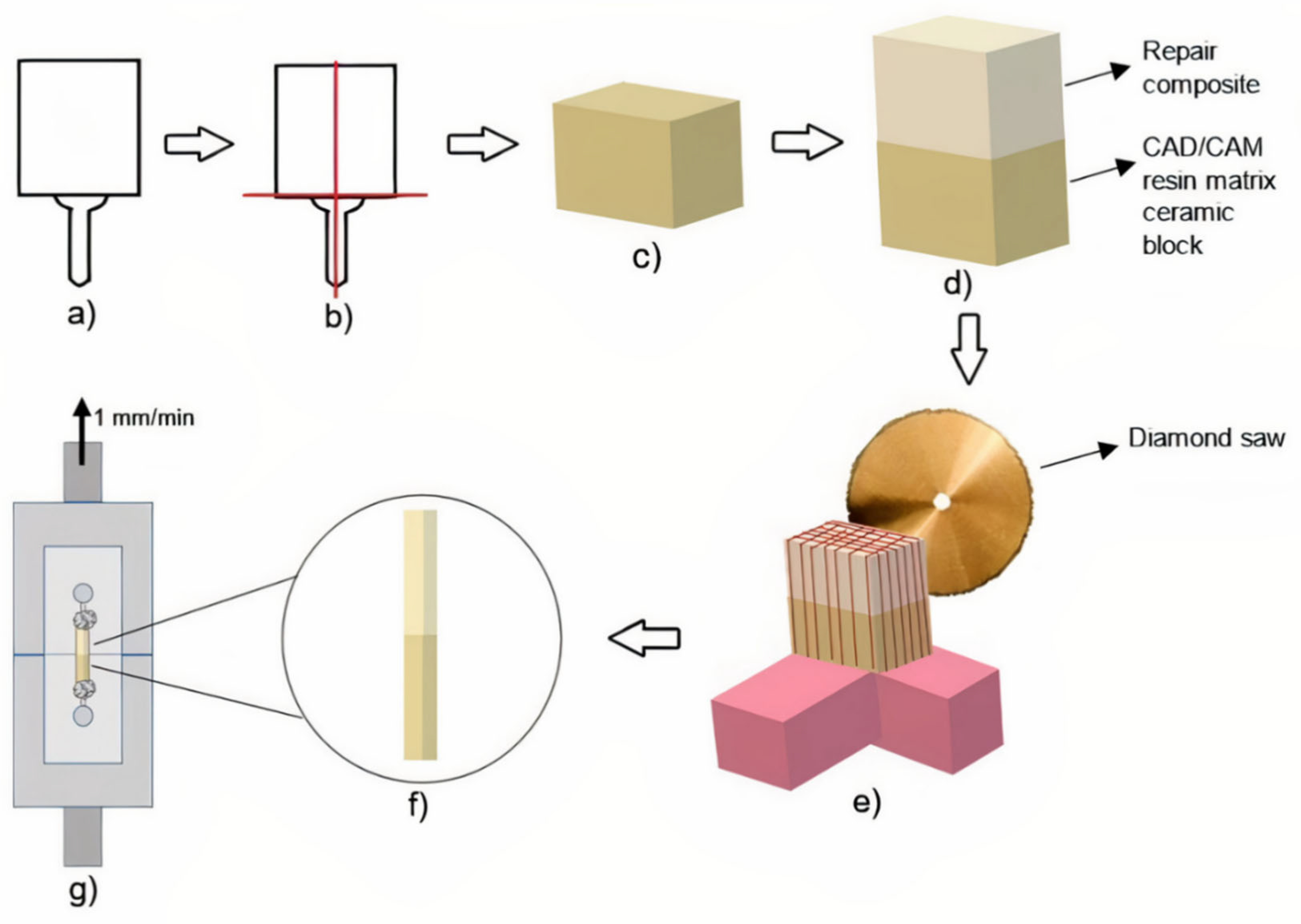
2. Materials and Methods
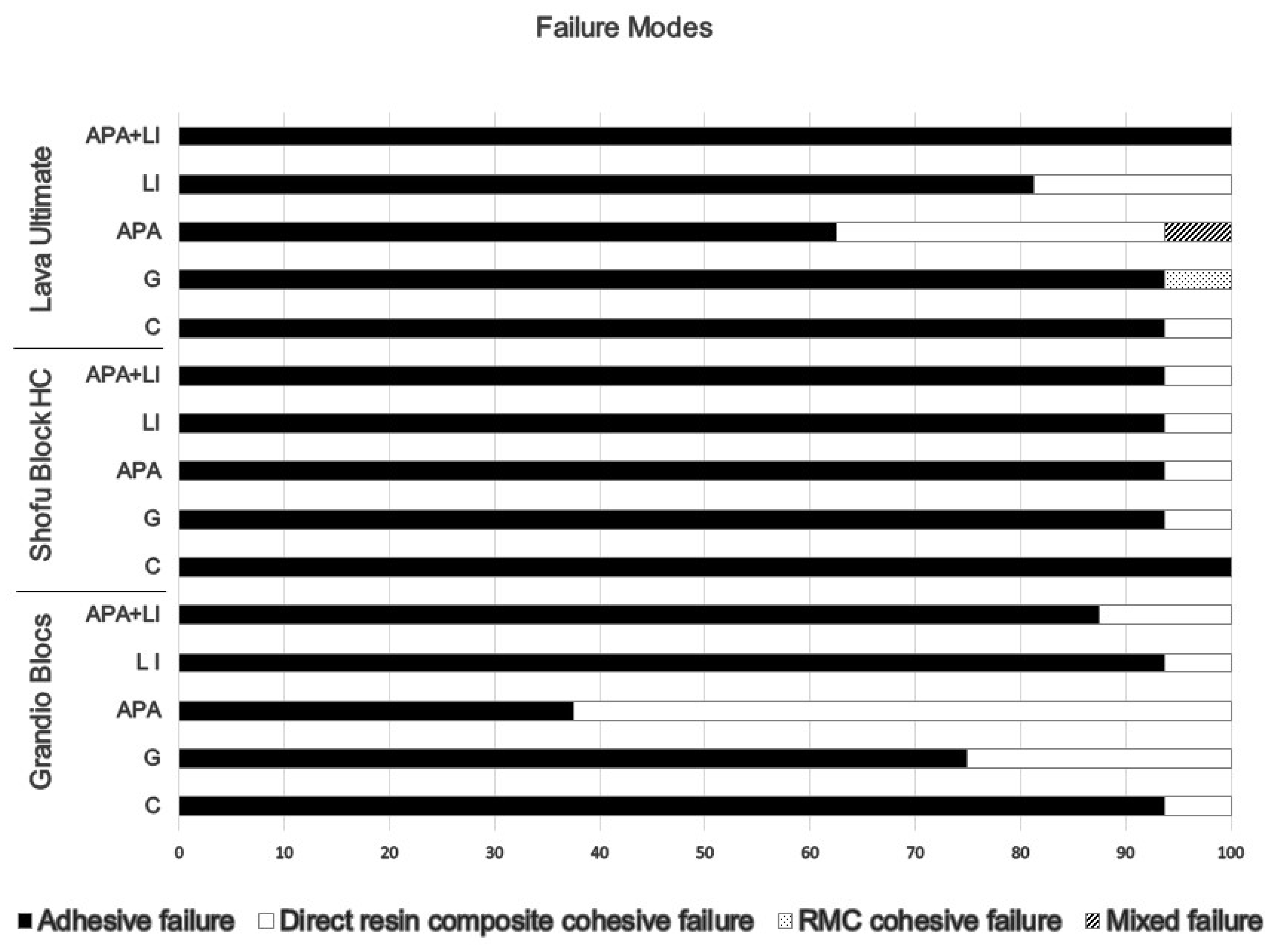
3. Results
4. Discussion
5. Conclusions
- Except for the Grandio Blocs control group (18.01 MPa), all surface treatments showed clinically acceptable (≥20 MPa) bond-strength values.
- Laser irradiation can be applied as an alternative route to bur grinding and airborne particle abrasion recommended for surface roughening in intraoral resin matrix ceramic repair.
- Considering the micro-tensile bond strength values obtained, it is recommended that airborne particle abrasion + laser irradiation and Single Bond Universal be used as surface treatments for the Grandio Blocs to be repaired, Single Bond Universal without any additional surface treatment for Shofu Block HC, and bur grinding and Single Bond Universal for Lava Ultimate.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Villarroel, M.; Fahl, N.; De Sousa, A.M.; De Oliveira, O.B., Jr. Direct Esthetic Restorations Based on Translucency and Opacity of Composite Resins. J. Esthet. Restor. Dent. 2011, 23, 73–87. [Google Scholar] [CrossRef]
- Peumans, M.; Valjakova, E.B.; De Munck, J.; Mishevska, C.B.; Van Meerbeek, B. Bonding effectiveness of luting composites to different CAD/CAM materials. J. Adhes. Dent. 2016, 18, 289–302. [Google Scholar] [CrossRef] [PubMed]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital dentistry: An overview of recent developments for CAD/CAM generated restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Li, R.W.; Chow, T.W.; Matinlinna, J.P. Ceramic dental biomaterials and CAD/CAM technology: State of the art. J. Prosthodont. Res. 2014, 58, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Lambert, H.; Durand, J.C.; Jacquot, B.; Fages, M. Dental biomaterials for chairside CAD/CAM: State of the art. J. Adv. Prosthodont. 2017, 9, 486–495. [Google Scholar] [CrossRef]
- Moura, D.; Dal Piva, A.; Januário, A.; Verissímo, A.H.; Bottino, M.A.; Özcan, M.; Souza, R. Repair Bond Strength of a CAD/CAM Nanoceramic Resin and Direct Composite Resin: Effect of Aging and Surface Conditioning Methods. J. Adhes. Dent. 2020, 22, 275–283. [Google Scholar] [CrossRef]
- Sismanoglu, S.; Yildirim-Bilmez, Z.; Erten-Taysi, A.; Ercal, P. Influence of different surface treatments and universal adhesives on the repair of CAD-CAM composite resins: An in vitro study. J. Prosthet. Dent. 2020, 124, 238.e1. [Google Scholar] [CrossRef]
- Rocha Gomes Torres, C.; Caroline Moreira Andrade, A.; Valente Pinho Mafetano, A.P.; Stabile de Abreu, F.; de Souza Andrade, D.; Cintra Mailart, M.; Aun de Barros Lima Rocha Campello de Souza, M.L.; Guimarães Alarça Nunes, L.; Ariel Rodrigues de Araújo, C.; Di Nicoló, R.; et al. Computer-aided design and computer-aided manufacturer indirect versus direct composite restorations: A randomized clinical trial. J. Esthet. Restor. Dent. 2022, 34, 776–788. [Google Scholar] [CrossRef]
- Ling, L.; Ma, Y.; Malyala, R. A novel CAD/CAM resin composite block with high mechanical properties. Dent. Mater. 2021, 37, 1150–1155. [Google Scholar] [CrossRef]
- El-Damanhoury, H.M.; AElsahn, N.; Sheela, S.; Gaintantzopoulou, M.D. Adhesive luting to hybrid ceramic and resin composite CAD/CAM Blocks:Er:YAG Laser versus chemical etching and micro-abrasion pretreatment. J. Prosthodont. Res. 2021, 65, 225–234. [Google Scholar] [CrossRef]
- Loomans, B.A.; Mesko, M.E.; Moraes, R.R.; Ruben, J.; Bronkhorst, E.M.; Pereira-Cenci, T.; Huysmans, M.C. Effect of different surface treatment techniques on the repair strength of indirect composites. J. Dent. 2017, 59, 18–25. [Google Scholar] [CrossRef]
- Goia, T.S.; Leite, F.P.; Valandro, L.F.; Ozcan, M.; Bottino, M.A. Repair bond strength of a resin composite to alumina-reinforced feldspathic ceramic. Int. J. Prosthodont. 2006, 19, 400–402. [Google Scholar]
- Bayraktar, Y.; Arslan, M.; Demirtag, Z. Repair bond strength and surface topography of resin-ceramic and ceramic restorative blocks treated by laser and conventional surface treatments. Microsc. Res. Tech. 2021, 84, 1145–1154. [Google Scholar] [CrossRef]
- Knobloch, L.A.; Kerby, R.E.; Seghi, R.; van Putten, M. Two-body wear resistance and degree of conversion of laboratory-processed composite materials. Int. J. Prosthodont. 1999, 12, 432–438. [Google Scholar]
- Bähr, N.; Keul, C.; Edelhoff, D.; Eichberger, M.; Roos, M.; Gernet, W.; Stawarczyk, B. Effect of different adhesives combined with two resin composite cements on shear bond strength to polymeric CAD/CAM materials. Dent. Mater. J. 2013, 32, 492–501. [Google Scholar] [CrossRef]
- Üstün, Ö.; Büyükhatipoğlu, I.K.; Seçilmiş, A. Shear Bond Strength of Repair Systems to New CAD/CAM Restorative Materials. J. Prosthodont. 2018, 27, 748–754. [Google Scholar] [CrossRef]
- Veríssimo, A.H.; Duarte Moura, D.M.; de Oliveira Dal Piva, A.M.; Bottino, M.A.; de Fátima Dantas de Almeida, L.; da Fonte Porto Carreiro, A.; de Assunção E Souza, R.O. Effect of different repair methods on the bond strength of resin composite to CAD/CAM materials and microorganisms adhesion: An in situ study. J. Dent. 2020, 93, 103266. [Google Scholar] [CrossRef]
- Arpa, C.; Ceballos, L.; Fuentes, M.V.; Perdigão, J. Repair bond strength and nanoleakage of artificially aged CAD-CAM composite resin. J. Prosthet. Dent. 2019, 121, 523–530. [Google Scholar] [CrossRef]
- Barutcigil, K.; Barutcigil, Ç.; Kul, E.; Özarslan, M.M.; Buyukkaplan, U.S. Effect of Different Surface Treatments on Bond Strength of Resin Cement to a CAD/CAM Restorative Material. J. Prosthodont. 2019, 28, 71–78. [Google Scholar] [CrossRef]
- Pameijer, C.H.; Louw, N.P.; Fischer, D. Repaırıng Fractured Porcelaın: How Surface Preparatıon Affects Shear Force Resıstance. J. Am. Dent. Assoc. 1996, 127, 203–209. [Google Scholar] [CrossRef]
- Silva, P.; Martinelli-Lobo, C.M.; Bottino, M.A.; Melo, R.M.; Valandro, L.F. Bond strength between a polymer-infiltrated ceramic network and a composite for repair: Effect of several ceramic surface treatments. Braz. Oral Res. 2018, 32, e28. [Google Scholar] [CrossRef]
- Elsaka, S.E. Repair bond strength of resin composite to a novel CAD/CAM hybrid ceramic using different repair systems. Dent. Mater. J. 2015, 34, 161–167. [Google Scholar] [CrossRef] [Green Version]
- Erdemir, U.; Sancakli, H.S.; Sancakli, E.; Eren, M.M.; Ozel, S.; Yucel, T.; Yildiz, E. Shear bond strength of a new self-adhering flowable composite resin for lithium disilicate-reinforced CAD/CAM ceramic material. J. Adv. Prosthodont. 2014, 6, 434. [Google Scholar] [CrossRef]
- Alex, G. Universal adhesives: The next evolution in adhesive dentistry? Compend. Contin. Educ. Dent. 2015, 36, 15–40. [Google Scholar]
- Nagayassu, M.P.; Shintome, L.K.; Uemura, E.S.; Araújo, J.E. Effect of surface treatment on the shear bond strength of a resin-based cement to porcelain. Braz. Dent. J. 2006, 17, 290–295. [Google Scholar] [CrossRef]
- Kasraei, S.; Rezaei-Soufi, L.; Heidari, B.; Vafaee, F. Bond strength of resin cement to CO2 and Er:YAG laser-treated zirconia ceramic. Restor. Dent. Endod. 2014, 39, 296–302. [Google Scholar] [CrossRef]
- Kirmali, O.; Barutcigil, Ç.; Ozarslan, M.M.; Barutcigil, K.; Harorlı, O.T. Repair bond strength of composite resin to sandblasted and laser irradiated Y-TZP ceramic surfaces. Scanning 2015, 37, 186–192. [Google Scholar] [CrossRef]
- Cengiz-Yanardag, E.; Kurtulmus Yilmaz, S.; Karakaya, I.; Ongun, S. Effect of Different Surface Treatment Methods on Micro-Shear Bond Strength of CAD-CAM Restorative Materials to Resin Cement. J. Adhes. Sci. Technol. 2019, 33, 110–123. [Google Scholar] [CrossRef]
- Güngör, M.B.; Nemli, S.K.; Bal, B.T.; Ünver, S.; Doğan, A. Effect of surface treatments on shear bond strength of resin composite bonded to CAD/CAM resin-ceramic hybrid materials. J. Adv. Prosthodont. 2016, 8, 259–266. [Google Scholar] [CrossRef]
- Xie, C.; Han, Y.; Zhao, X.Y.; Wang, Z.Y.; He, H.M. Microtensile bond strength of one- and two-step self-etching adhesives on sclerotic dentin: The effects of thermocycling. Oper. Dent. 2010, 35, 547–555. [Google Scholar] [CrossRef]
- Gale, M.S.; Darvell, B.W. Thermal cycling procedures for laboratory testing of dental restorations. J. Dent. 1999, 27, 89–99. [Google Scholar] [CrossRef]
- Gul, P.; Altınok-Uygun, L. Repair bond strength of resin composite to three aged CAD/CAM blocks using different repair systems. J. Adv. Prosthodont. 2020, 12, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Raposo, L.H.; Armstrong, S.R.; Maia, R.R.; Qian, F.; Geraldeli, S.; Soares, C.J. Effect of specimen gripping device, geometry and fixation method on microtensile bond strength, failure mode and stress distribution: Laboratory and finite element analyses. Dent. Mater. 2012, 28, e50–e62. [Google Scholar] [CrossRef] [PubMed]
- Valente, L.L.; Silva, M.F.; Fonseca, A.S.; Münchow, E.A.; Isolan, C.P.; Moraes, R.R. Effect of Diamond Bur Grit Size on Composite Repair. J. Adhes. Dent. 2015, 17, 257–263. [Google Scholar] [CrossRef]
- Costa, T.R.; Ferreira, S.Q.; Klein-Júnior, C.A.; Loguercio, A.D.; Reis, A. Durability of Surface Treatments and Intermediate Agents Used for Repair of a Polished Composite. Oper. Dent. 2010, 35, 231–237. [Google Scholar] [CrossRef]
- Oz, F.D.; Canatan, S.; Bolay, S. Effects of surface treatments on the bond strength of composite resin to hybrid computer-assisted design/manufacturing blocks. J. Adhes. Sci. Tech. 2019, 33, 986–1000. [Google Scholar] [CrossRef]
- Elsaka, S.E. Bond strength of novel CAD/CAM restorative materials to self-adhesive resin cement: The effect of surface treatments. J. Adhes Dent. 2014, 16, 531–540. [Google Scholar] [CrossRef]
- Ghorab, S.; Farahat, D. Influence of sandblasting parameters and luting materials on microshear bond strength to a CAD/CAM hybrid ceramic material. Egypt Dent. J. 2020, 66, 1637–1648. [Google Scholar] [CrossRef]
- Yoshihara, K.; Nagaoka, N.; Maruo, Y.; Nishigawa, G.; Irie, M.; Yoshida, Y.; Van Meerbeek, B. Sandblasting may damage the surface of composite CAD–CAM blocks. Dent. Mater. 2017, 33, e124–e135. [Google Scholar] [CrossRef]
- Curran, P.; Cattani-Lorente, M.; Anselm Wiskott, H.W.; Durual, S.; Scherrer, S.S. Grinding damage assessment for CAD-CAM restorative materials. Dent. Mater. 2017, 33, 294–308. [Google Scholar] [CrossRef]
- Kimyai, S.; Mohammadi, N.; Navimipour, E.J.; Rikhtegaran, S. Comparison of the Effect of Three Mechanical Surface Treatments on the Repair Bond Strength of a Laboratory Composite. Photomed. Laser Surg. 2010, 28, S-25–S-30. [Google Scholar] [CrossRef]
- Tzanakakis, E.G.; Tzoutzas, I.G.; Koidis, P.T. Is there a potential for durable adhesion to zirconia restorations? A systematic review. J. Prosthet. Dent. 2016, 115, 9–19. [Google Scholar] [CrossRef]
- Kurtulmus-Yilmaz, S.; Cengiz, E.; Ongun, S.; Karakaya, I. The Effect of Surface Treatments on the Mechanical and Optical Behaviors of CAD/CAM Restorative Materials. J. Prosthodont. 2019, 28, e496–e503. [Google Scholar] [CrossRef]
- Yavuz, T.; Dilber, E.; Kara, H.B.; Tuncdemir, A.R.; Ozturk, A.N. Effects of different surface treatments on shear bond strength in two different ceramic systems. Lasers Med. Sci. 2013, 28, 1233–1239. [Google Scholar] [CrossRef]
- Günal-Abduljalil, B.; Önöral, Ö.; Ongun, S. Micro-shear bond strengths of resin-matrix ceramics subjected to different surface conditioning strategies with or without coupling agent application. J. Adv. Prosthodont. 2021, 13, 180–190. [Google Scholar] [CrossRef]
- Colombo, M.; Poggio, C.; Lasagna, A.; Chiesa, M.; Scribante, A. Vickers Micro-Hardness of New Restorative CAD/CAM Dental Materials: Evaluation and Comparison after Exposure to Acidic Drink. Materials 2019, 12, 1246. [Google Scholar] [CrossRef]
- Sideridou, I.; Tserki, V.; Papanastasiou, G. Effect of chemical structure on degree of conversion in light-cured dimethacrylate-based dental resins. Biomaterials 2002, 23, 1819–1829. [Google Scholar] [CrossRef]
- Gajewski, V.E.; Pfeifer, C.S.; Fróes-Salgado, N.R.; Boaro, L.C.; Braga, R.R. Monomers used in resin composites: Degree of conversion, mechanical properties and water sorption/solubility. Braz. Dent. J. 2012, 23, 508–514. [Google Scholar] [CrossRef]
- Kallio, T.T.; Lastumäki, T.M.; Vallittu, P.K. Bonding of restorative and veneering composite resin to somepolymeric composites. Dent. Mater. 2001, 17, 80–86. [Google Scholar] [CrossRef]
- Michelotti, G.; Niedzwiecki, M.; Bidjan, D.; Dieckmann, P.; Deari, S.; Attin, T.; Tauböck, T.T. Silane Effect of Universal Adhesive on the Composite–Composite Repair Bond Strength after Different Surface Pretreatments. Polymers 2020, 12, 950. [Google Scholar] [CrossRef]
- Nagaoka, N.; Yoshihara, K.; Feitosa, V.P.; Tamada, Y.; Irie, M.; Yoshida, Y.; Van Meerbeek, B.; Hayakawa, S. Chemical interaction mechanism of 10-MDP with zirconia. Sci. Rep. 2017, 7, 45563. [Google Scholar] [CrossRef]
- El Zohairy, A.A.; De Gee, A.J.; Mohsen, M.M.; Feilzer, A.J. Microtensile bond strength testing of luting cements to prefabricated CAD/CAM ceramic and composite blocks. Dent. Mater. 2003, 19, 575–583. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; de Jager, N.; Kleverlaan, C.J.; Feilzer, A.J. Microtensile bond strength of different components of core veneered all-ceramic restorations. Dent. Mater. 2005, 21, 984–991. [Google Scholar] [CrossRef]
- Wang, H.; Cui, B.; Li, J.; Li, S.; Lin, Y.; Liu, D.; Li, M. Mechanical properties and biocompatibility of polymer infiltrated sodium aluminum silicate restorative composites. J. Adv. Ceram. 2017, 6, 73–79. [Google Scholar] [CrossRef]
- Van Noort, R.; Noroozi, S.; Howard, I.C.; Cardew, G. A critique of bond strength measurements. J. Dent. 1989, 17, 61–67. [Google Scholar] [CrossRef]
- Wiegand, A.; Stucki, L.; Hoffmann, R.; Attin, T.; Stawarczyk, B. Repairability of CAD/CAM high-density PMMA- and composite-based polymers. Clin. Oral Investig. 2015, 19, 2007–2013. [Google Scholar] [CrossRef]
- Makowka, S.R. Development of a Gripping Fixture for Micro-Tensile Testing of Bonded Ceramic Dumbbells. Ph.D. Thesis, State University of New York at Buffalo, Buffalo, NY, USA, 2018. [Google Scholar]
- Poitevin, A.; De Munck, J.; Van Landuyt, K.; Coutinho, E.; Peumans, M.; Lambrechts, P.; Van Meerbeek, B. Influence of three specimen fixation modes on the micro-tensile bond strength of adhesives to dentin. Dent. Mater. J. 2007, 26, 694–699. [Google Scholar] [CrossRef]
- Armstrong, S.R.; Boyer, D.B.; Keller, J.C. Microtensile bond strength testing and failure analysis of two dentin adhesives. Dent. Mater. 1998, 14, 44–50. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Manufacturer | Specification | Composition | Lot Number |
|---|---|---|---|---|
| Single Bond Universal | 3M ESPE, St. Paul, MN, USA | Universal Adhesive | HEMA, 10-MDP, dimethacrylate resins, Vitrebond copolymer, silane, filler, ethanol, water, initiators. pH: 2.7 | 01026A |
| Grandio SO | VOCO GmbH, Cuxhaven, Germany | Universal Nano-hybrid Composite | 89% w/w high filler content. 60% functionalized nanoparticles (20–40 nm) in the resin content and glass ceramic. | 2109672 |
| Grandio Blocs (GB) | VOCO GmbH, Cuxhaven, Germany | Nano-hybrid Composite | 86% w/w nano silica and barium glass fillers in a polymer matrix. 14% UDMA, DMA. | 2014063 |
| Shofu Block HC (HC) | Shofu Dental GmbH, Ratingen, Germany | Resin Nanoceramic | Silica powder, micro fumed silica, zirconium silicate fillers 61% by weight. UDMA, TEGDMA. | 071601 |
| Lava Ultimate (LU) | 3M ESPE, St. Paul, MN, USA | Resin Nanoceramic | 80% silica and zirconia nanoparticles and nanoclusters as filler content. 20% BisGMA, UDMA, BisEMA, TEGDMA. | NA57353 |
| Source | Type III Sum of Squares | df | Mean Square | F | Sig. |
|---|---|---|---|---|---|
| Material-Type (A) | 475.920 | 2 | 237.960 | 1.335 | 0.265 |
| Surface-Treatment (B) | 19352.476 | 4 | 4838.119 | 27.147 | 0.000 |
| A × B | 35023.972 | 8 | 4377.996 | 24.565 | 0.000 |
| Material | Surface Treatment | Group | Mean ± Standard Deviation |
|---|---|---|---|
| Grandio Blocs (GB) | Control (C) | GBC | 18.01 ± 7.88 A |
| Bur grinding (G) | GBG | 63.57 ± 11.22 EF | |
| Airborne particle abrasion (APA) | GBAPA | 61.88 ± 9.40 EF | |
| Laser irradiation (LI) | GBLI | 64.77 ± 5.26 EF | |
| Airborne particle abrasion + Laser irradiation (APA+LI) | GBAPA+LI | 70.94 ± 6.03 F | |
| Shofu Block HC (HC) | Control (C) | HCC | 64.35 ± 17.99 EF |
| Bur grinding (G) | HCG | 42.86 ± 17.18 BCD | |
| Airborne particle abrasion (APA) | HCAPA | 35.98 ± 7.20 BC | |
| Laser irradiation (LI) | HCLI | 60.50 ± 12.32 EF | |
| Airborne particle abrasion + Laser irradiation (APA+LI) | HCAPA+LI | 58.46 ± 16.87 DEF | |
| Lava Ultimate (LU) | Control (C) | LUC | 28.46 ± 4.92 AB |
| Bur grinding (G) | LUG | 66.09 ± 21.66 EF | |
| Airborne particle abrasion (APA) | LUAPA | 64.40 ± 21.62 EF | |
| Laser irradiation (LI) | LULI | 49.63 ± 10.54 CDE | |
| Airborne particle abrasion + Laser irradiation (APA+LI) | LUAPA+LI | 59,66 ± 12.34 EF |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arkoy, S.; Ulusoy, M. Effect of Different Surface Treatments on Repair Bond Strength of CAD/CAM Resin-Matrix Ceramics. Materials 2022, 15, 6314. https://doi.org/10.3390/ma15186314
Arkoy S, Ulusoy M. Effect of Different Surface Treatments on Repair Bond Strength of CAD/CAM Resin-Matrix Ceramics. Materials. 2022; 15(18):6314. https://doi.org/10.3390/ma15186314
Chicago/Turabian StyleArkoy, Semih, and Mutahhar Ulusoy. 2022. "Effect of Different Surface Treatments on Repair Bond Strength of CAD/CAM Resin-Matrix Ceramics" Materials 15, no. 18: 6314. https://doi.org/10.3390/ma15186314
APA StyleArkoy, S., & Ulusoy, M. (2022). Effect of Different Surface Treatments on Repair Bond Strength of CAD/CAM Resin-Matrix Ceramics. Materials, 15(18), 6314. https://doi.org/10.3390/ma15186314