



Autonomous Self-Healing Methods as a Potential Technique for the Improvement of Concrete’s Durability

 ,
,  and
and
Abstract
:1. Introduction
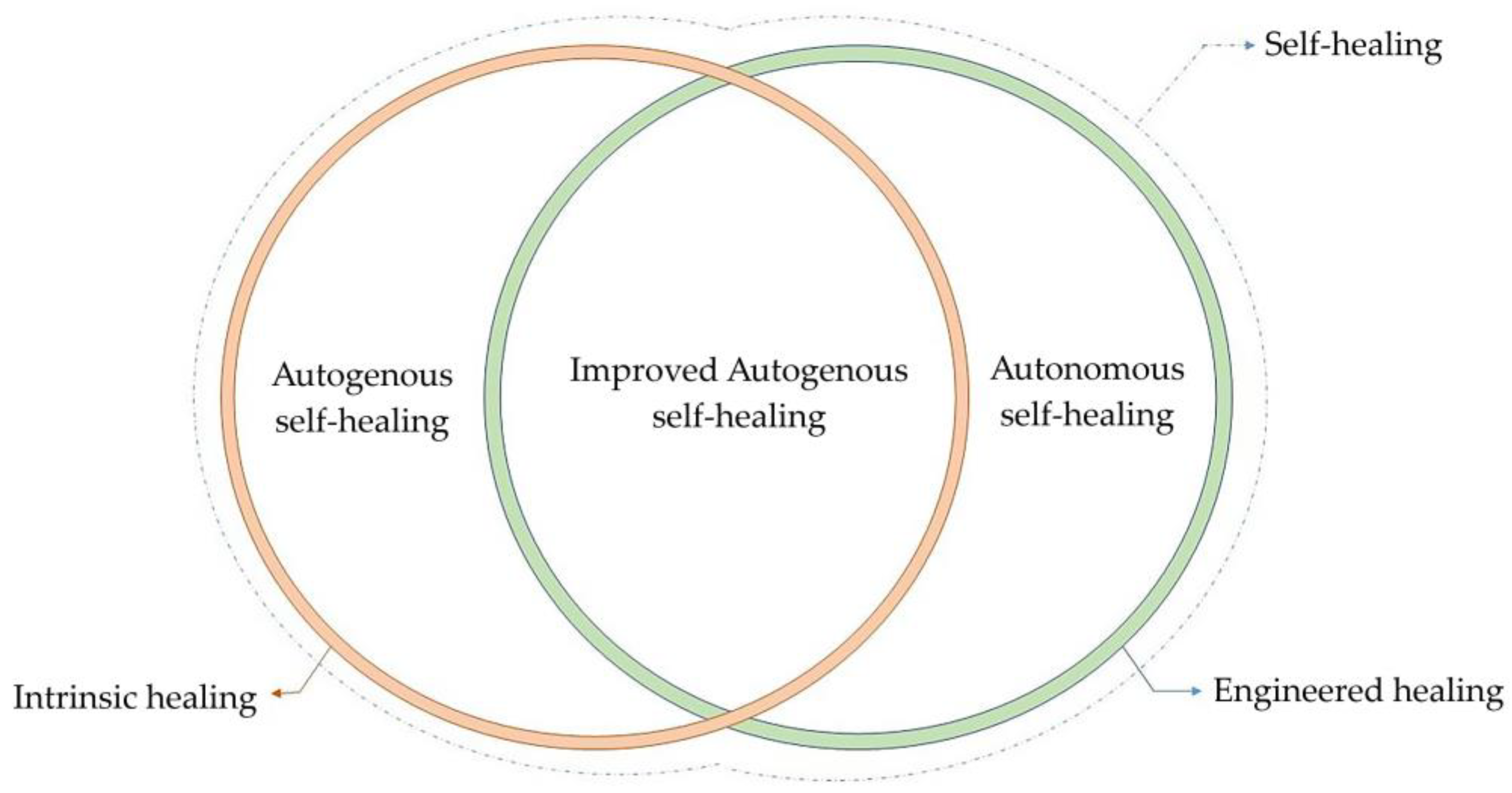
2. Autogenous and Improved Autogenous Self-Healing
2.1. Physical Process
2.2. Chemical Processes
2.3. Mechanical Processes
3. Autonomous or Engineered Self-Healing
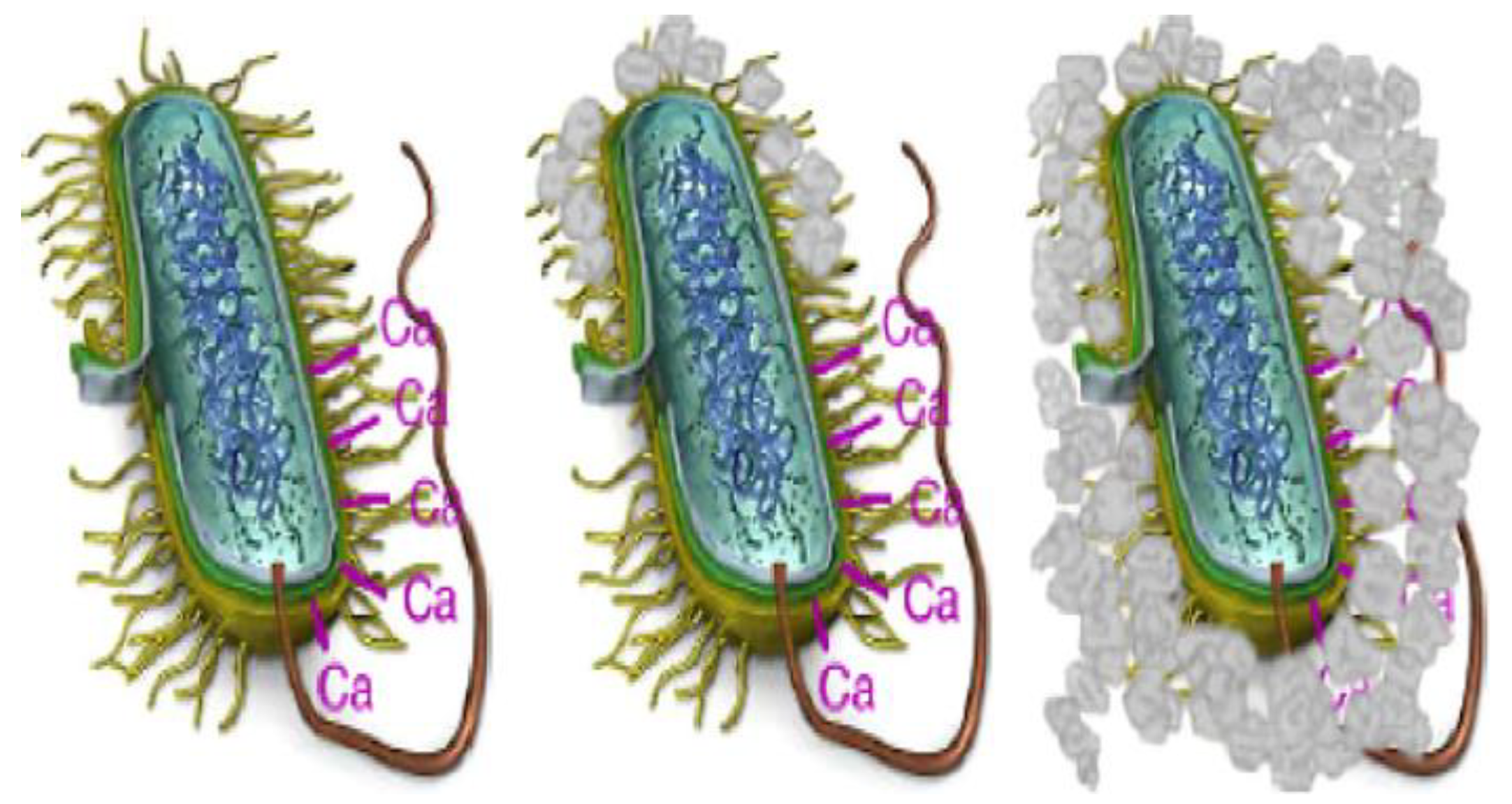
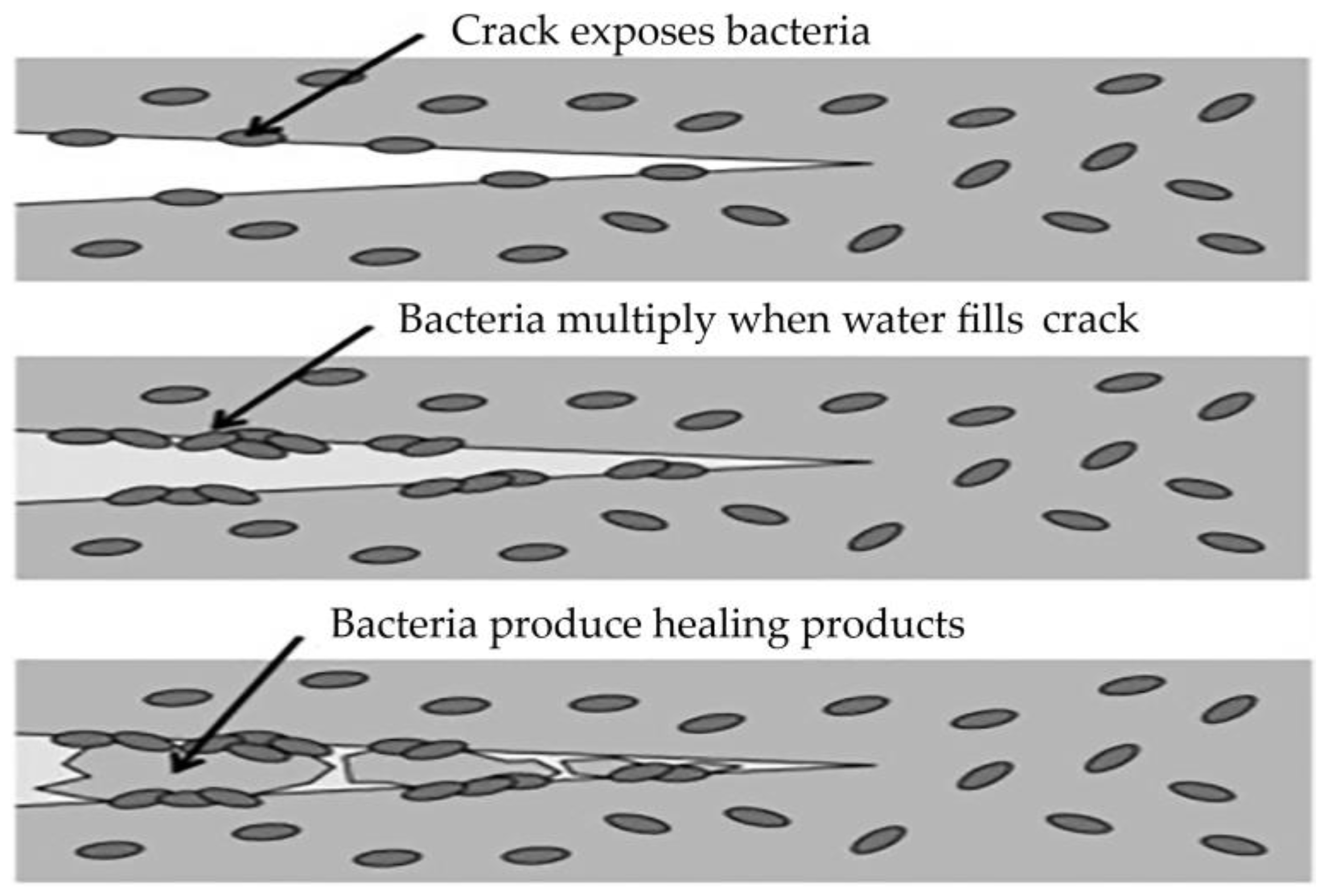
3.1. Self-Healing of Concrete Using Bacteria
3.2. Self-Healing of Concrete Using Crystalline Hydrophilic Admixtures
- Precipitation Reaction Mechanism—active chemicals penetrate the concrete with water and react with the free lime and oxides in the pores, forming crystalline materials that block pores and cracks. Water is a critical factor stimulating the crystal precipitation in the crack due to the reactive and hydrophilic nature of crystalline admixtures. The reaction between the active compound of the crystalline additive and tricalcium silicate in the presence of water forms a denser calcium silicate hydrate. The effect of the calcium additive can lead to pore clogging, creating a hydrophobic layer in the capillaries, or both. Crystalline additives block pores and, in doing so, deposit hydrates in the cracks to resist water ingress under pressure.
- Complexation Precipitation Reaction Mechanism—active chemicals bind with Ca2+ in concrete, forming an unstable complex that disperses in the pore solution. Complex ions are replaced with SiO32− on non-hydrated cement particles to form C–S–H gels and fill the pores. Active chemicals become free again and continue to diffuse in the solution. The primary identified products of hardened paste are ettringite and calcium silicate hydrate. The primary process for external crack healing is the formation of calcium carbonate, resulting from the action of calcium additives. The interaction of carbonate and bicarbonate ions leads to the precipitation of calcium carbonate, which is associated with increased material durability.
- Combined Mechanism of Precipitation and Complexation Reactions—part of the active chemicals participates in the capillary crystallization reaction, while another part catalyzes the hydration of non-hydrated cement particles. Limestone formations react with tricalcium aluminate and form different calcium carboaluminates, such as hemi-carbo aluminate, mono-carbo aluminate, and tri-carbo aluminate. Silicate formations (ground quartz) react with calcium hydrate. Limestone formations have a much higher moisture absorption capacity. The high affinity between limestone formation and calcium aluminate favors the crystallization of mono-carbo aluminate over mono-sulfate. This process results in reduced porosity and an increase in the volume of hydrated phases.
- Condensation Crystallization Mechanism of Active Chemicals—these substances form insoluble crystals through condensation polymerization to fill cracks and pores.
3.3. Self-Healing of Concrete through Capsule Application
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gardner, D.; Lark, R.; Jefferson, T.; Davies, R. A survey on problems encountered in current concrete construction and the potential benefits of self-healing cementitious materials. Case Stud. Constr. Mater. 2018, 8, 238–247. [Google Scholar] [CrossRef]
- Danish, A.; Mosaberpanah, M.A.; Salim, M.U. Past and present techniques of self-healing in cementitious materials: A critical review on efficiency of implemented treatments. J. Mater. Res. Technol. 2020, 9, 6883–6889. [Google Scholar] [CrossRef]
- Du, W.; Yu, J.; Gu, Y.; Li, Y.; Han, X.; Liu, Q. Preparation and application of microcapsules containing toluene diisocyanate for self-healing of concrete. Constr. Build. Mater. 2019, 202, 762–769. [Google Scholar] [CrossRef]
- Golewski, G.L. The Phenomenon of Cracking in Cement Concretes and Reinforced Concrete Structures: The Mechanism of Cracks Formation, Causes of Their Initiation, Types and Places of Occurrence, and Methods of Detection—A Review. Buildings 2023, 13, 765. [Google Scholar] [CrossRef]
- Koroth, S.R. Evaluation and Improvement of Frost Durability of Clay Bricks—A Thesis in The Centre for Building Studies. PhD. Dissertation, University of Concordia, Montreal, QC, Canada, 1997. [Google Scholar]
- Pilehvar, S.; Szczotok, A.M.; Rodríguez, J.F.; Valentini, L.; Lanzón, M.; Pamies, R.; Kjøniksen, A.L. Effect of freeze-thaw cycles on the mechanical behavior of geopolymer concrete and Portland cement concrete containing micro-encapsulated phase change materials. Constr. Build. Mater. 2019, 200, 94–103. [Google Scholar] [CrossRef]
- Richardson, M.G. Fundamentals of Durable Reinforced Concrete, 1st ed.; Spon Press: London, UK, 2002. [Google Scholar]
- De Maio, U.; Gaetano, D.; Greco, F.; Lonetti, P.; Blasi, P.N.; Pranno, A. The Reinforcing Effect of Nano-Modified Epoxy Resin on the Failure Behavior of FRP-Plated RC Structures. Buildings 2023, 13, 1139. [Google Scholar] [CrossRef]
- De Maio, U.; Gaetano, D.; Greco, F.; Lonetti, P.; Pranno, A. The damage effect on the dynamic characteristics of FRP-strengthened reinforced concrete structures. Compos. Struct. 2023, 309, 116731. [Google Scholar] [CrossRef]
- Qiu, Y.; Peng, H.; Zhao, H. Study on New Type of Concrete Air-Entraining Agent. In Proceedings of the International Conference on Artificial Intelligence and Electromechanical Automation (AIEA), Tianjin, China, 26–28 June 2020. [Google Scholar]
- Nicula, L.M.; Corbu, O.; Iliescu, M. Influence of Blast Furnace Slag on the Durability Characteristic of Road Concrete Such as Freeze-Thaw Resistance. Procedia Manuf. 2020, 46, 194–201. [Google Scholar] [CrossRef]
- Islam, M.M.; Alam, M.T.; Islam, M.S. Effect of fly ash on freeze–thaw durability of concrete in marine environment. Aust. J. Struct. Eng. 2018, 19, 1–16. [Google Scholar] [CrossRef]
- Zang, P.; Li, Q.F. Freezing–thawing durability of fly ash concrete composites containing silica fume and polypropylene fiber. Proc. Inst. Mech. Eng. Part L J. Mater. Des. Appl. 2013, 228, 241–246. [Google Scholar] [CrossRef]
- Zhang, J.; Fan, Y.; Li, N. Pore structure and freezing resistance of nanoclay modified cement based materials. Mater. Res. Innov. 2014, 18, 358–362. [Google Scholar] [CrossRef]
- Li, X.; Ling, T.C.; Mo, K.H. Functions and impacts of plastic/rubber wastes as eco-friendly aggregate in concrete—A review. Constr. Build. Mater. 2020, 240, 117869. [Google Scholar] [CrossRef]
- Kumar, R.; Dev, N. Effect of acids and freeze-thaw on durability of modified rubberized concrete with optimum rubber crumb content. J. Appl. Polym. Sci. 2022, 139, 52191. [Google Scholar] [CrossRef]
- He, Y.; Xu, F.; Wei, H. Effect of Particle Size on Properties of Concrete with Rubber Crumbs. Am. J. Civ. Eng. 2022, 10, 79–87. [Google Scholar]
- Pham, N.P.; Toumi, A.; Turatsinze, A. Effect of an enhanced rubber-cement matrix interface on freeze-thaw resistance of the cement-based composite. Constr. Build. Mater. 2019, 207, 528–534. [Google Scholar] [CrossRef]
- Ribeiro, M.S.C.; Juvandes, L.F.P.; Rodrigues, J.D.; Ferreira, A.; Marques, A.T. Behaviour of Cement and Polymer Mortar Materials to Rapid Freeze-Thaw Cycling. Mater. Sci. Forum 2010, 636–637, 1329–1335. [Google Scholar] [CrossRef]
- Khashayar, J.; Heidarnezhad, F.; Moammer, O.; Jarrah, M. Experimental investigation on freeze—Thaw durability of polymer concrete. Front. Struct. Civ. Eng. 2021, 15, 1038–1046. [Google Scholar] [CrossRef]
- Qu, Z.; Guo, S.; Sproncken, C.C.M.; Surís-Valls, R.; Yu, Q.; Voets, I.K. Enhancing the Freeze–Thaw Durability of Concrete through Ice Recrystallization Inhibition by Poly(vinyl alcohol). ACS Omega 2020, 5, 12825–12831. [Google Scholar] [CrossRef]
- Guo, Y.; Shen, A.; Sun, X. Exploring Polymer-Modified Concrete and Cementitious Coating with High-Durability for Roadside Structures in Xinjiang, China. Adv. Mater. Sci. Eng. 2017, 2017, 9425361. [Google Scholar] [CrossRef]
- Hammodat, W.W. Investigate road performance using polymer modified concrete. Mater. Today Proc. 2021, 42, 2089–2094. [Google Scholar] [CrossRef]
- Saeed, H. Properties of polymer impregnated concrete spacers. Case Stud. Constr. Mater. 2021, 15, e00772. [Google Scholar] [CrossRef]
- Caiyun, W.; Li, W.; Zhang, C.; Jinpeng, F. Effect of Protective Coatings on Frost Resistance of Concrete Structures in Northeast Coastal Areas. IOP Conf. Ser. Mater. Sci. Eng. 2019, 678, 012108. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, C.; Zhou, K.; Tian, Y. Freeze-thaw cycling damage evolution of additive cement mortar. Eur. J. Environ. Civ. Eng. 2021, 25, 2089–2110. [Google Scholar] [CrossRef]
- Setzer, M.J.; Fagerlund, G.; Janssen, D.J. CDF test—Test Method for the Freeze-Thaw Resistance of Concrete-Tests with Sodium Chloride Solution (CDF). Mater. Struct. 1996, 29, 523–528. [Google Scholar] [CrossRef]
- Matar, M.G.; Aday, A.N.; Srubar III, W.V. Surfactant properties of a biomimetic antifreeze polymer admixture for improved freeze-thaw durability of concrete. Constr. Build. Mater. 2021, 313, 125423. [Google Scholar] [CrossRef]
- Ji, Y.; Zou, Y.; Ma, Y.; Wang, H.; Li, W.; Xu, X. Frost Resistance Investigation of Fiber-Doped Cementitious Composites. Materials 2022, 15, 2226. [Google Scholar] [CrossRef]
- De Rooij, M.; Van Tittelboom, K.; De Belie, N.; Schlangen, E. (Eds.) Self-Healing Phenomena in Cement-Based Materials: State-of-the-Art Report of RILEM Technical Committee 221-SHC: Self-Healing Phenomena in Cement-Based Materials; Springer: Dordrecht, The Netherlands, 2013; Volume 11. [Google Scholar]
- Lahman, D.; Edvardsen, C.; Kessler, S. Autogenous self-healing of concrete: Experimental design and test methods—A review. Eng. Rep. 2023, 5, e12565. [Google Scholar] [CrossRef]
- Edvardsen, C. Water Permeability and Autogenous Healing of Cracks in Concrete. Ph.D. Dissertation, RWTH Aachen, Aachen, Germany, 1996. [Google Scholar]
- Rajczakowska, M.; Nilsson, L.; Habermehl-Cwirzen, K.; Hedlund, H.; Cwirzen, A. Does a High Amount of Unhydrated Portland Cement Ensure an Effective Autogenous Self-Healing of Mortar? Materials 2020, 12, 3298. [Google Scholar] [CrossRef]
- Yuan, L.; Chen, S.; Wang, S.; Huang, Y.; Yang, Q.; Liu, S.; Wang, J.; Du, P.; Cheng, X.; Zhou, Z. Research on the improvement of concrete autogenous self-healing based on the regulation of cement particle size distribution (PSD). Materials 2019, 12, 2818. [Google Scholar] [CrossRef]
- Meichsner, H.; Röhling, S. Die Selbstdichtung (Selbstheilung) von Trennrissen-einRisiko in der WU-Richtlinie. Der Bausachverständige 2015, 11, 9. [Google Scholar]
- Roig-Flores, M.; Serna, P. Concrete Early-Age Crack Closing by Autogenous Healing. Sustainability 2020, 12, 4476. [Google Scholar] [CrossRef]
- Hearn, N.; Morley, C.T. Self-sealing property of concrete—Experimental evidence. Mater. Struct. 1997, 30, 404–411. [Google Scholar] [CrossRef]
- Mahmoodi, S.; Sadeghian, P. Self-Healing Concrete: A Review of Recent Research Developments and Existing Research Gaps. In Proceedings of the CSCE Annual Conference, Laval (Greater Montreal), Montreal, QC, Canada, 12–15 June 2019. [Google Scholar]
- Suleiman, A.R.; Nehdi, M.L. Efect of autogenous crack self-healing on mechanical strength recovery of cement mortar under various environmental exposure. Sci. Rep. 2021, 11, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hong, G.; Song, C.; Choi, S. Autogenous Healing of Early-Age Cracks in Cementitious Materials by Superabsorbent Polymers. Materials 2020, 13, 690. [Google Scholar] [CrossRef] [PubMed]
- Snoeck, D.; De Belie, N. Autogenous Healing in Strain-Hardening Cementitious Materials With and Without Superabsorbent Polymers: An 8-Year Study. Front. Mater. 2019, 6, 48. [Google Scholar] [CrossRef]
- Zeng, Y.; Zuo, Q.; Jiang, S.; Guo, M.Z.; Wang, T.; Chu, H. Effect of CTAB on the healing of concrete cracks repaired by electrodeposition and the durability of repaired concrete. Constr. Build. Mater. 2022, 326, 126757. [Google Scholar] [CrossRef]
- Vijay, K.; Murmu, M.; Deo, S.V. Bacteria based self healing concrete—A review. Constr. Build. Mater. 2017, 152, 1008–1014. [Google Scholar] [CrossRef]
- Jogi, P.K.; Lakshmi, T.V.S.V. Selfhealing concrete based on different bacteria: A review. Mater. Today Proc. 2020, 43, 1246–1252. [Google Scholar] [CrossRef]
- Erşan, Y.C.; Verbruggen, H.; De Graeve, I.; Verstraete, W.; Boon, N. Nitrate reducing CaCO3 precipitating bacteria survive in mortar and inhibit steel corrosion. Cem. Constr. Res. 2016, 83, 19–30. [Google Scholar] [CrossRef]
- Wang, J.; Dewanckele, J.; Cnudde, V.; Van Vlierberghe, S.; Verstraete, W.; De Belie, N. X-ray computed tomography proof of bacterial-based self-healing in concrete. Cem. Constr. Compos. 2014, 53, 289–304. [Google Scholar] [CrossRef]
- Zhang, L.V.; Nehdi, M.L.; Suleiman, A.R.; Allaf, M.M.; Gan, M.; Marani, A.; Tuyan, M. Crack self-healing in bio-green concrete. Compos. Part B 2021, 227, 109397. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, Y.; Feng, T.; Zhou, M.; Zhao, L.; Zhou, A.; Li, Z. Immobilizing bacteria in expanded perlite for the crack self-healing in concrete. Constr. Build. Mater. 2017, 148, 610–617. [Google Scholar] [CrossRef]
- Erşan, Y.C.; Hernandez-Sanabria, E.; Boon, N.; De Belie, N. Enhanced crack closure performance of microbial mortar through nitrate reduction. Cem. Constr. Compos. 2016, 70, 159–170. [Google Scholar] [CrossRef]
- Algaifi, H.A.; Bakar, S.A.; Alyousef, R.; Sam, A.R.M.; Wan Ibrahim, M.H.; Shahidan, S.; Ibrahim, M.; Salami, B.A. Bio-inspired self-healing of concrete cracks using new B. pseudoycoides species. J. Mater. Res. Technol. 2021, 12, 967–981. [Google Scholar] [CrossRef]
- Safiuddin, M.; Ihtheshaam, S.; Kareem, R.A. Shalam A study on self-healing concrete. Mater. Today Proc. 2022, 52, 1175–1181. [Google Scholar] [CrossRef]
- Khaliq, W.; Ehsan, M.B. Crack healing in concrete using various bio influenced self-healing techniques. Constr. Build. Mater. 2016, 102, 349–357. [Google Scholar] [CrossRef]
- Pei, R.; Liu, J.; Wang, S.; Yang, M. Use of bacterial cell walls to improve the mechanical performance of concrete. Cem. Constr. Compos. 2013, 39, 122–130. [Google Scholar] [CrossRef]
- Jiang, L.; Jia, G.; Jiang, C.; Li, Z. Sugar-coated expanded perlite as a bacterial carrier for crack-healing concrete applications: Highlights. Constr. Build. Mater. 2020, 232, 117222. [Google Scholar] [CrossRef]
- Kanwal, M.; Khushnood, R.A.; Khaliq, W.; Watoo, A.G.; Shahid, T. Synthesis of pyrolytic carbonized bagasse to immobilize Bacillus subtilis; application in healing micro-cracks and fracture properties of concrete. Cem. Constr. Compos. 2022, 126, 104334. [Google Scholar] [CrossRef]
- Achal, V.; Mukerjee, A.; Reddy, M.S. Biogenic treatment improves the durability and remediates the cracks of concrete structures. Constr. Build. Mater. 2013, 48, 1–5. [Google Scholar] [CrossRef]
- García Calvo, J.L.; Sánchez Moreno, M.; Carballosa, P.; Pedrosa, F.; Tavares, F. Improvement of the Concrete Permeability by Using Hydrophilic Blended Additive. Materials 2019, 12, 2384. [Google Scholar] [CrossRef] [PubMed]
- EN 934-2:2009+A1:2012; Admixtures for Concrete, Mortar and Grout—Part 2: Concrete Admixtures—Definitions, Requirements, Conformity, Marking and Labelling. CEN: Brussels, Belgium, 2012.
- ACI Committee 212. American Report on Chemical Admixtures for Concrete—ACI 212.3R-16; American Concrete Institute, March 2016; ISBN: 978-1-942727-80-4. Available online: https://www.concrete.org/Portals/0/Files/PDF/Previews/212_3R-16_PREVIEW.pdf (accessed on 20 October 2023).
- Hu, X.; Xiao, J.; Zhang, Z.; Wang, C.; Long, C.; Dai, L. Effects of CCCW on properties of cement-based materials: A review. J. Build. Eng. 2022, 50, 104184. [Google Scholar] [CrossRef]
- Sisomphon, K.; Copuroglu, O.; Koenders, E. Self-healing of surface cracks in mortars with expansive additive and crystalline additive. Cem. Constr. Compos. 2012, 34, 566–574. [Google Scholar] [CrossRef]
- Park, B.; Choi, Y.C. Effect of healing products on the self-healing performance of cementitious materials with crystalline admixtures. Constr. Build. Mater. 2021, 270, 121389. [Google Scholar] [CrossRef]
- Roig-Flores, M.; Moscato, S.; Serna, P.; Ferrara, L. Self-healing capability of concrete with crystalline admixtures in different environments. Constr. Build. Mater. 2015, 86, 1–11. [Google Scholar] [CrossRef]
- Escoffres, P.; Desmettre, C.; Charron, J.P. Effect of a crystalline admixture on the self-healing capability of high-performance fiber reinforced concretes in service conditions. Constr. Build. Mater. 2018, 173, 763–774. [Google Scholar] [CrossRef]
- Li, G.; Huang, X.; Lin, J.; Jiang, X.; Zhang, X. Activated chemicals of cementitious capillary crystalline waterproofing materials and their self-healing behavior. Constr. Build. Mater. 2019, 200, 36–45. [Google Scholar] [CrossRef]
- Roig-Flores, M.; Piritano, F.; Serna, P.; Ferrara, L. Effect of crystalline admixtures on the self-healing capability of early-age concrete studied by means of permeability and crack closing tests. Constr. Build. Mater. 2016, 114, 447–457. [Google Scholar] [CrossRef]
- Elsalamawy, M.; Mohamed, A.R.; Abdel-latif, E.A. Performance of crystalline forming additive materials in concrete. Constr. Build. Mater. 2020, 230, 117056. [Google Scholar] [CrossRef]
- Lauch, K.S.; Desmettre, C.; Charron, J.P. Self-healing of concrete containing different admixtures under laboratory and long-term real outdoor expositions based on water permeability test. Constr. Build. Mater. 2022, 324, 126700. [Google Scholar] [CrossRef]
- Li, D.; Chen, B.; Chen, X.; Fu, B.; Wei, H.; Xiang, X. Synergetic effect of superabsorbent polymer (SAP) and crystalline admixture (CA) on mortar macro-crack healing. Constr. Build. Mater. 2020, 247, 118521. [Google Scholar] [CrossRef]
- Park, B.; Young, C.C. Investigating a new method to assess the self-healing performance of hardened cement pastes containing supplementary cementitious materials and crystalline admixtures. J. Mater. Res. Technol. 2019, 8, 6058–6073. [Google Scholar] [CrossRef]
- Oliveira, A.S.; Toledo Filho, R.D.; Rego Fairbairn, E.M.; Cappa de Oliveira, L.F.; Martins Gomes, O.F. Microstructural characterization of self-healing products in cementitious systems containing crystalline admixture in the short- and long-term. Cem. Constr. Compos. 2022, 126, 104369. [Google Scholar] [CrossRef]
- Reddy, T.C.S.; Ravitheja, A. Macro mechanical properties of self healing concrete with crystalline admixture under different environments. Ain Shams Eng. J. 2019, 10, 23–32. [Google Scholar] [CrossRef]
- Zhang, C.; Lu, R.; Li, Y.; Guan, X. Effect of crystalline admixtures on mechanical, self-healing and transport properties of engineered cementitious composite. Cem. Constr. Compos. 2021, 124, 104256. [Google Scholar] [CrossRef]
- Gojević, A.; Ducman, V.; Netinger Grubeša, I.; Baričević, A.; Banjad Pečur, I. The Effect of Crystalline Waterproofing Admixtures on the Self-Healing and Permeability of Concrete. Materials 2021, 14, 1860. [Google Scholar] [CrossRef] [PubMed]
- Azarsa, P.; Gupta, R.; Biparva, A. Assessment of self-healing and durability parameters of concretes incorporating crystalline admixtures and Portland Limestone Cement. Cem. Constr. Compos. 2019, 99, 17–31. [Google Scholar] [CrossRef]
- Souradeep, G.; Kua, H.W. Encapsulation Technology and Techniques in Self-Healing Concrete. J. Mater. Civ. Eng. 2016, 28, 12. [Google Scholar] [CrossRef]
- Souza, L.; Al-Tabbaa, A. Microfluidic fabrication of microcapsules tailored for self-healing in cementitious materials. Constr. Build. Mater. 2018, 184, 713–722. [Google Scholar] [CrossRef]
- Milla, J.; Hassan, M.M.; Rupnow, T.; Daly, W.H. Measuring the crack-repair efficiency of steel fiber reinforced concrete beams with microencapsulated calcium nitrate. Constr. Build. Mater. 2019, 201, 526–538. [Google Scholar] [CrossRef]
- Wu, M.; Hu, X.M.; Hu, Z.X.; Zhao, Y.; Cheng, W.M.; Lu, W. Two-component polyurethane healing system: Effect of different accelerators and capsules on the healing efficiency of dynamic concrete cracks. Constr. Build. Mater. 2019, 227, 116700. [Google Scholar] [CrossRef]
- Gilabert, F.A.; Van Tittelboom, K.; Van Stappen, J.; Cnudde, V.; De Belie, N.; Van Paepegem, W. Integral procedure to assess crack filling and mechanical contribution of polymer-based healing agent in encapsulation-based self-healing concrete. Cem. Constr. Compos. 2017, 77, 68–80. [Google Scholar] [CrossRef]
- Hu, Z.X.; Hu, X.M.; Cheng, W.M.; Zhao, Y.Y.; Wu, M.Y. Performance optimization of one-component polyurethane healing agent for self-healing concrete. Constr. Build. Mater. 2018, 179, 151–159. [Google Scholar] [CrossRef]
- Du, W.; Yu, J.; He, B.; He, Y.; He, P.; Li, Y.; Liu, Q. Preparation and characterization of nano-SiO2/paraffin/PE wax composite shell microcapsules containing TDI for self-healing of cementitious materials. Constr. Build. Mater. 2020, 231, 117060. [Google Scholar] [CrossRef]
- Du, W.; Yu, J.; Gu, S.; Wang, R.; Li, J.; Han, X.; Liu, Q. Effect of temperatures on self-healing capabilities of concrete with different shell composition microcapsules containing toluene-di-isocyanate. Constr. Build. Mater. 2020, 247, 118575. [Google Scholar] [CrossRef]
- Li, Y.; Yu, J.; Cao, Z.; He, P.; Liu, Q.; Han, X.; Wan, Y. Preparation and application of novel microcapsules ruptured by microwave for self-healing concrete. Constr. Build. Mater. 2021, 304, 124616. [Google Scholar] [CrossRef]
- Wang, X.; Chen, S.; Yang, Z.; Ren, J.; Zhang, X.; Xing, F. Self-healing concrete incorporating mineral additives and encapsulated lightweight aggregates: Preparation and application. Constr. Build. Mater. 2021, 301, 124119. [Google Scholar] [CrossRef]
- Wang, X.; Huang, Y.; Huang, Y.; Zhang, J.; Fang, C.; Yu, K.; Chen, Q.; Li, T.; Han, R.; Yang, Z.; et al. Laboratory and field study on the performance of microcapsule-based self-healing concrete in tunnel engineering. Constr. Build. Mater. 2019, 220, 90–101. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, J.; Han, R.; Han, N.; Xing, F. Evaluation of damage and repair rate of self-healing microcapsule-based cementitious materials using electrochemical impedance spectroscopy. J. Clean. Prod. 2019, 235, 966–976. [Google Scholar] [CrossRef]
- Feng, J.; Dong, H.; Wang, R.; Su, Y. A novel capsule by poly (ethylene glycol) granulation for self-healing concrete. Cem. Constr. Res. 2020, 133, 106053. [Google Scholar] [CrossRef]
- Oliveira, T.A.; Bragança, M.D.O.G.P.; Pinkoski, I.M.; Carrera, G. The effect of silica nanocapsules on self-healing concrete. Constr. Build. Mater. 2021, 300, 124010. [Google Scholar] [CrossRef]
- Papaioannou, S.; Amenta, M.; Kilikoglou, V.; Gournis, D.; Karatasios, I. Synthesis and integration of cement-based capsules modified with sodium silicate for developing self-healing cements. Constr. Build. Mater. 2022, 316, 125803. [Google Scholar] [CrossRef]
- Dong, B.; Fang, G.; Ding, W.; Liu, Y.; Zhang, J.; Han, N.; Xing, F. Self-healing features in cementitious material with urea–formaldehyde/epoxy microcapsules. Constr. Build. Mater. 2016, 106, 608–617. [Google Scholar] [CrossRef]
- Hilloulin, B.; Van Tittelboom, K.; Gruyaert, E.; De Belie, N.; Loukili, A. Design of polymeric capsules for self-healing concrete. Cem. Constr. Compos. 2015, 55, 298–307. [Google Scholar] [CrossRef]
- Van Tittelboom, K.; Wang, J.; Araújo, M.; Snoeck, D.; Gruyaert, E.; Debbaut, B.; Derluyn, H.; Cnudde, V.; Tsangouri, E.; Van Hemelrijck, D.; et al. Comparison of different approaches for self-healing concrete in a large-scale lab test. Constr. Build. Mater. 2016, 107, 125–137. [Google Scholar] [CrossRef]
- Al-Tabbaa, A.; Litina, C.; Giannaros, P.; Kanellopoulos, A.; Souza, L. First UK field application and performance of microcapsule-based self-healing concrete. Constr. Build. Mater. 2019, 208, 669–685. [Google Scholar] [CrossRef]
- Araújo, M.; Chatrabhuti, S.; Gurdebeke, S.; Alderete, N.; Van Tittelboom, K.; Raquez, J.M.; Cnudde, V.; Van Vlierberghe, S.; De Belie, N.; Gruyaert, E. Poly(methyl methacrylate) capsules as an alternative to the ‘’proof-of-concept’’ glass capsules used in self-healing concrete. Cem. Constr. Compos. 2018, 89, 260–271. [Google Scholar] [CrossRef]
- Seifan, M.; Samani, A.K.; Berenjian, A. Bioconcrete: Next generation of self-healing concrete. Appl. Microbiol. Biotechnol. 2016, 100, 2591–2602. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Type of Bacteria | Tested Properties | Results |
|---|---|---|---|
| Çağatay Erşan et al. [45] | Protected and unprotected Pseudomonas aeruginosa and Diaphorobacter nitroreducens; unprotected mixtures of microbiological cultures containing activated compact denitrification core (ACDC) | Survival in concrete | Unprotected mixture of microbiological cultures containing ACDC was superior; Pseudomonas aeruginosa and Diaphorobacter nitroreducens survival was better when protected |
| Wang et al. [46] | Bacillus sphaericus with nutrients; hydrogel; hydrogel encapsulated bacteria; no bacteria | Crack healing in different humidity conditions | Best healing during wet–dry cycles for specimens with hydrogel encapsulated bacteria |
| Zhang et al. [47] | Sporosarcina pasteurii on expanded glass granules; expanded glass granules | Crack healing in water and wet–dry conditions | Better healing during wet–dry cycles for specimens with bacteria on expanded glass granules |
| Zhang et al. [48] | Bacillus cohnii directly added; Bacillus cohnii added on a carrier made of either expanded perlite or expanded clay; no bacteria | Crack healing in water | Best healing for specimens with bacteria on expanded perlite |
| Çağatay Erşan et al. [49] | Pseudomonas aeruginosa and Diaphorobacter nitroreducens added on a carrier of either expanded clay or granular activated carbon | Crack healing in water | Both types of bacteria were equally effective on both carriers |
| Algaifi et al. [50] | Bacillus pseudomycoides; no bacteria | Crack healing in water; compressive strength | Healing was better and compressive strength was higher for concrete with bacteria |
| Safiuddin et al. [51] | Bacillus subtilis and Escherichia coli each separately and combined | Crack healing by sprinkling water; compressive strength; splitting tensile strength | Bacillus subtilis positively influenced healing; each bacteria separately had a positive effect on compressive and splitting tensile strength but a negative effect when combined |
| Khaliq and Ehsan [52] | Bacillus subtilis added either directly or on a carrier of lightweight aggregate/graphite nanoparticles; no bacteria | Crack healing in water; compressive strength | Graphite nanoparticles were a more efficient carrier; bacteria improved compressive strength regardless of whether it is applied |
| Pei et al. [53] | Living and dead Bacillus subtilis bacteria and cell walls of living Bacillus subtilis | Compressive strength | Dead and live Bacillus subtilis cells had a negative effect on compressive strength; Bacillus subtilis walls increased compressive strength |
| Jiang et al. [54] | Bacillus cohnii added on a carrier made of expanded perlite non-coated or coated with geopolymers, Portland cement, acid sulfoaluminate cement, potassium magnesium phosphate cement, and hemihydrate gypsum; no bacteria | Crack healing in water | Geopolymer and Portland cement coatings significantly improved healing |
| Kanwal et al. [55] | Bacillus subtilis with or without coal; no bacteria | Crack healing in water; compressive strength; water absorption | Best healing for bacteria with coal; bacteria with or without coal improved compressive strength and reduced water absorption |
| Achal et al. [56] | Bacillus subtilis; no bacteria | Crack healing in contact with water; compressive strength; porosity; chloride penetration | Bacteria improved healing, increased compressive strength, reduced porosity, and reduced chloride penetration |
| Authors | Type of Crystalline Hydrophilic Admixture (CA) | Tested Properties | Results |
|---|---|---|---|
| Park and Choi [62] | Na2SO4 or Al2(SO4)3, with or without expanding agent (CSA); no CA | Crack-healing in contact with water | CA promotes healing, especially when combined with CSA |
| Roig-Flores et al. [63] | Unnamed CA; no CA | Crack healing in different humidity conditions | CA promotes healing, especially when specimens are in contact with water |
| Escoffres et al. [64] | Sika WT-250; no CA | Mechanical recovery in terms of bending strength of specimens cured in water and in air | CA slightly improved recovery when specimens were in water |
| Li et al. [65] | CA coatings based on sodium carbonate, sodium silicate, sodium aluminate, tetrasodium EDTA, and glycerin | Crack healing in contact with water | Coating based on sodium silicate had the best healing ability |
| Roig-Flores et al. [66] | Unnamed CA; no CA | Crack healing in different humidity conditions | CA promotes healing, especially when specimens are cured in water at 30 °C |
| Elsalamawy et al. [67] | Three different commercially available CAs; no CA | Initial water absorption | CA significantly reduces initial water absorption |
| Lauch et al. [68] | Penetron admix alone or combined with expansive agent (CSA)/superabsorbent polymer (SAP); no admixture | Crack healing in different humidity conditions | CA promotes healing, especially in wet/dry cycles, which is further enhanced when CA is combined with CSA |
| Li et al. [69] | Citric acid, silica, sodium silicate, sodium carbonate, and a commercial product from the manufacturer Harbin, all combined with SAP | Crack healing in contact with water | Citric acid achieved the best synergistic effects with SAP in terms of crack healing |
| Park and Choi [70] | Various sulfate-based and carbonate-based CAs; no CA | Heat of hydration | Sulfate-based CA promoted healing at an early age, while carbonate-based CA promoted healing at a later age |
| Oliveira et al. [71] | Unnamed CA; no CA | Heat of hydration | CA slows down the setting process of the cement paste |
| Reddy and Ravitheja [72] | Unnamed CA | Mechanical recovery in terms of compressive strength and split tensile strength of specimens cured in different humidity conditions | Water immersion of specimens best promotes healing |
| Zhang et al. [73] | CA made of ion chelator, calcium formate, silica sol, and ethylene–vinyl acetate; no CA | Crack healing in contact with water; compressive strength | CA positively impacted healing and compressive strength |
| Gojević et al. [74] | Penetron admix; no CA | Crack healing in water; compressive strength; water penetration depth | CA improved healing, had no effect on compressive strength, and reduced water penetration depth |
| Azarsaa et al. [75] | Unnamed CA; no CA | Crack healing in contact with water; water penetration depth; electrical resistivity; resistance to chloride penetration | CA improved healing, reduced water penetration depth, had no effect on electrical resistivity, and improved resistance to chloride penetration |
| Authors | Capsule Types | Tested Properties | Results |
|---|---|---|---|
| Milla et al. [78] | Microcapsules made of calcium nitrate as a healing agent and urea–formaldehyde as a shell material, with and without emulsifiers added; no microcapsules | Crack healing in water | Microcapsules improved healing; the ones without emulsifiers were more effective in healing |
| Wu et al. [79] | Glass capsules with a dual-component healing system for encapsulating polyurethane and different accelerators | Crack healing in air | Polyurethane is a very effective healing agent |
| Gilabert et al. [80] | Capsules made of borosilicate glass filled with either polyurethane resin or a combination of polyurethane resin and accelerator | Crack healing in air | Polyurethane resin acted more like an adhesive than a healing agent |
| Hu et al. [81] | Capsules made of quartz glass filled with polyurethane as a healing agent diluted with acetone | Crack healing in air | Acetone increased the dispersion area of the healing agent |
| Du et al. [3] | Microcapsules made of toluene di-isocyanate as a core and paraffin as a shell; no microcapsules | Crack healing in air; mechanical recovery in terms of compressive strength | Microcapsules promoted healing and mechanical recovery |
| Du et al. [82] | Microcapsules made of toluene di-isocyanate as a core and paraffin/paraffin with wax/paraffin with wax and nano SiO2 as a shell; no microcapsules | Crack healing in air | Microcapsules with a shell made of paraffin with wax and nano SiO2 showed the most successful healing |
| Du et al. [83] | Microcapsules made of toluene di-isocyanate as a core and paraffin/paraffin with wax/paraffin with wax and nano SiO2 as a shell; no microcapsules | Mechanical recovery in terms of compressive strength at different temperatures; recovery rate of chloride diffusion coefficient | Higher temperatures favored crack healing |
| Li et al. [84] | Microcapsules made from toluene di-isocyanate as a core, with graphite, paraffin, and polyethene wax as a shell; no microcapsules | Crack healing in two curing regimes: room temperature and 10 min of microwave treatment followed by five days at room temperature; compressive strength; chloride diffusion coefficient | Ten min of microwave treatment followed by five days at room temperature ensured better healing than room temperature curing; 5% of microcapsules improved compressive strength and reduced chloride diffusion coefficient |
| Wang et al. [85] | Lightweight aggregate (LWA) as a Na2CO3 carrier in concrete mixes (coated and non-coated); lightweight aggregate (LWA) | Crack healing in water and in a solution saturated with Ca(OH)2; compressive and tensile strength; chloride penetration coefficient | Healing was better in a solution saturated with Ca(OH)2; coated LWA ensured the best healing and the highest compressive and tensile strength; non-coated LWA ensured the lowest chloride penetration coefficient |
| Wang et al. [86] | Microcapsules synthesized using urea–formaldehyde resin as a shell and epoxy resin as a healing agent; no microcapsules | Crack healing at room temperature; recovery in terms of compressive strength and chloride penetration coefficient | Microcapsules improved healing and had a positive effect on recovery in terms of compressive strength and chloride penetration coefficient |
| Wang et al. [87] | Microcapsules synthesized using urea–formaldehyde resin as a shell and epoxy resin as a healing agent; no microcapsules | Crack healing at room temperature of single-cracked specimens and multiple-cracked specimens | Samples with multiple cracks are more prone to healing than samples with one crack |
| Feng et al. [88] | Capsules made of cement and polyethylene glycol (PEG) or cement, superabsorbent polymer (SAP), and polyethylene glycol (PEG); no capsules | Crack healing in water; recovery in terms of compressive and flexural strength as well as water permeability | Capsules improved healing and recovery in terms of compressive and flexural strength as well as water permeability; capsules with SAP were more efficient |
| Apolinário de Oliveira et al. [89] | Nanocapsules made of silica; no nanocapsules | Crack healing at room temperature and in high-humidity chamber; compressive and tensile strength; electrical resistance | Healing was better in high humidity chamber; microcapsules improved healing efficiency and decreased compressive and tensile strength but increased electrical resistance |
| Papaioannou et al. [90] | Capsules made of Portland cement prepared by pelletizing in a drum as a core and Na2SiO3 solution as a shell; no capsules | Healing in contact with water; flexural and compressive strength; modulus of elasticity | Capsules improved healing, compressive strength, and modulus of elasticity but reduced flexural strength |
| Dong et al. [91] | Microcapsules from urea–formaldehyde resin as a shell and epoxy resin as a healing agent; no microcapsules | Recovery in terms of compressive strength, water permeability, and chloride penetration depth | Microcapsules positively influenced recovery of compressive strength, water permeability, and chloride penetration depth |
| Hilloulin et al. [92] | Extruded capsules from different polymers | Survival in concrete | Capsules exhibited brittle behavior during concrete mixing |
| Van Tittelboom [93] | Capsules with polyurethane core and glass shell (PU); no capsules | Healing through water spraying | Capsules were most effective for the most expansive cracks |
| Al-Tabbaa et al. [94] | Microcapsules with a shell made of gelatin/gum Arabic and sodium silicate as a core; no microcapsules | Healing in contact with water; strength recovery | Microcapsules improved healing and strength recovery |
| Araújo et al. [95] | Capsules made of water-repellent agent as a core and polymeric cylindrical capsules (PMMA) or glass capsules as a shell; no capsules | Healing in contact with water | PMMA and glass capsules improved healing process |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gojević, A.; Netinger Grubeša, I.; Marković, B.; Juradin, S.; Crnoja, A. Autonomous Self-Healing Methods as a Potential Technique for the Improvement of Concrete’s Durability. Materials 2023, 16, 7391. https://doi.org/10.3390/ma16237391
Gojević A, Netinger Grubeša I, Marković B, Juradin S, Crnoja A. Autonomous Self-Healing Methods as a Potential Technique for the Improvement of Concrete’s Durability. Materials. 2023; 16(23):7391. https://doi.org/10.3390/ma16237391
Chicago/Turabian StyleGojević, Anita, Ivanka Netinger Grubeša, Berislav Marković, Sandra Juradin, and Anđelko Crnoja. 2023. "Autonomous Self-Healing Methods as a Potential Technique for the Improvement of Concrete’s Durability" Materials 16, no. 23: 7391. https://doi.org/10.3390/ma16237391
APA StyleGojević, A., Netinger Grubeša, I., Marković, B., Juradin, S., & Crnoja, A. (2023). Autonomous Self-Healing Methods as a Potential Technique for the Improvement of Concrete’s Durability. Materials, 16(23), 7391. https://doi.org/10.3390/ma16237391