
Porous Alpha-Tricalcium Phosphate with Immobilized Basic Fibroblast Growth Factor Enhances Bone Regeneration in a Canine Mandibular Bone Defect Model

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
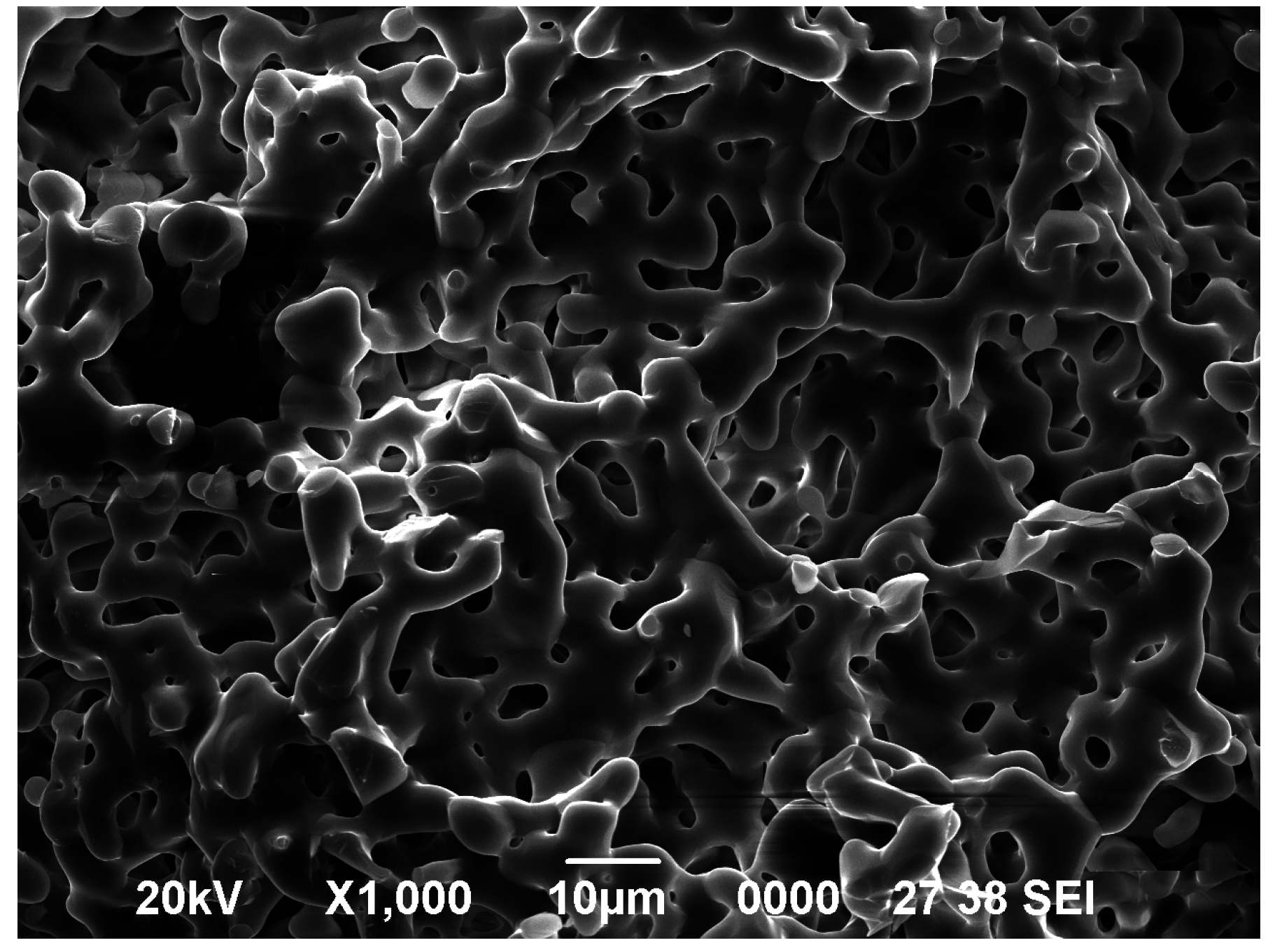
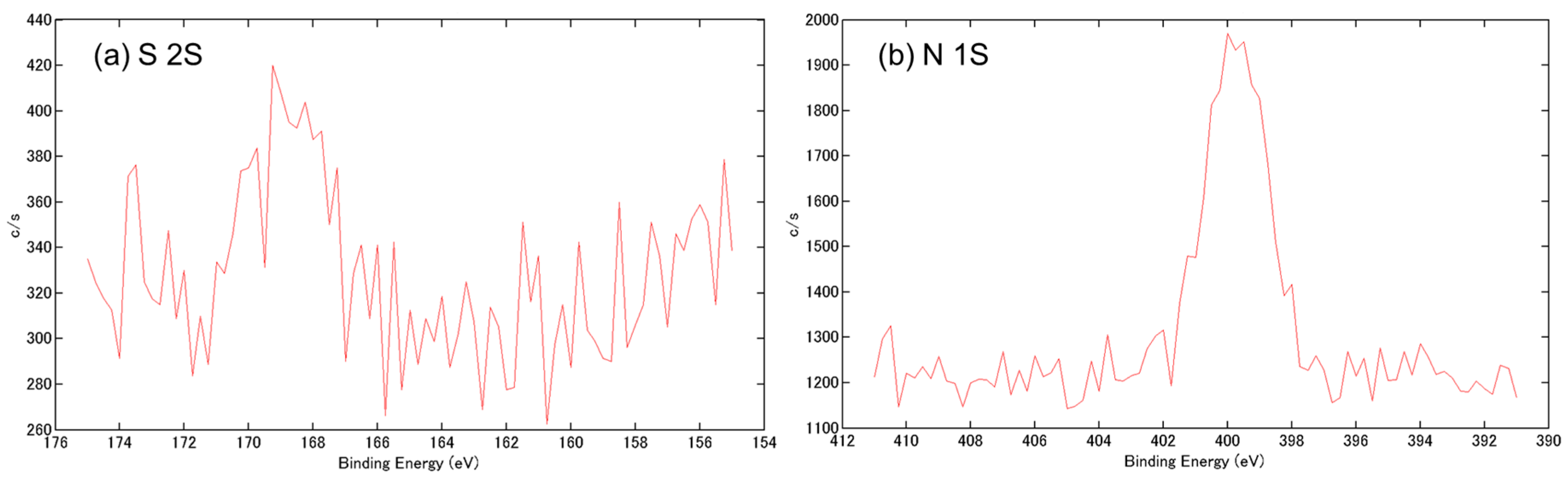
2.1. Analysis of Porous Alpha-Tricalcium Phosphate (α-TCP) Particles with Immobilized Basic Fibroblast Growth Factor (bFGF)
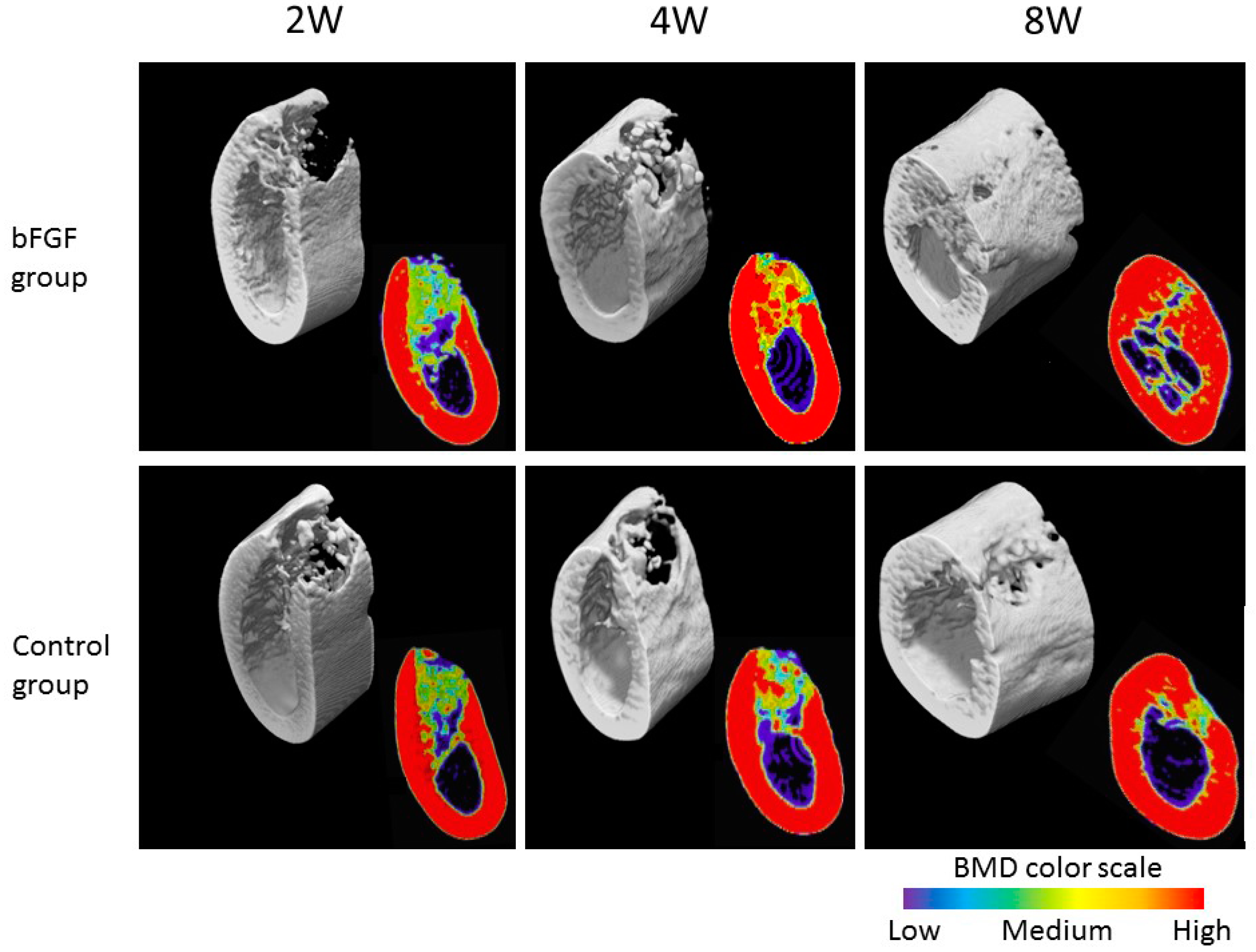
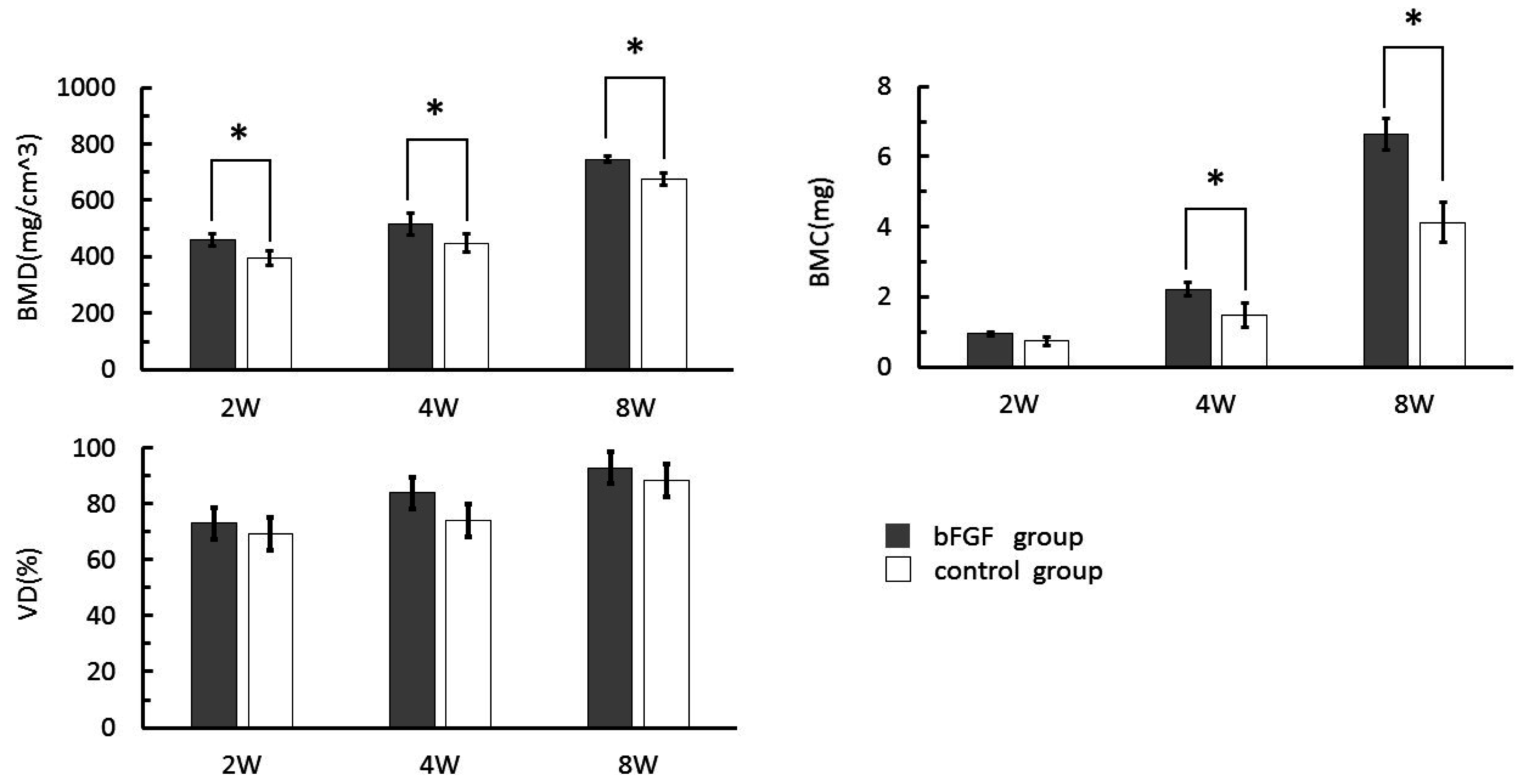
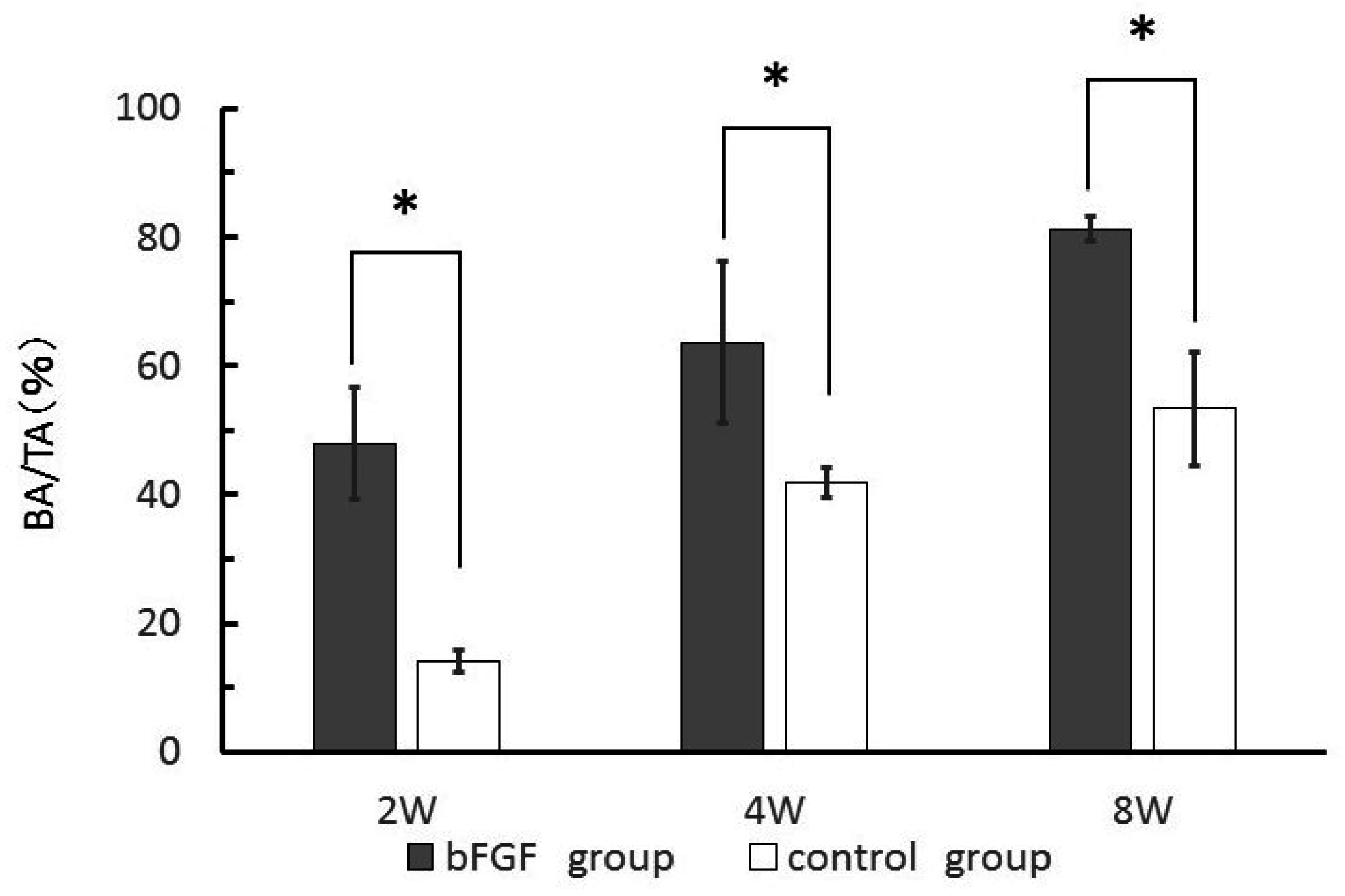
2.2. Three-Dimensional (3D) Microradiography and Bone Mineral Density (BMD) Analysis
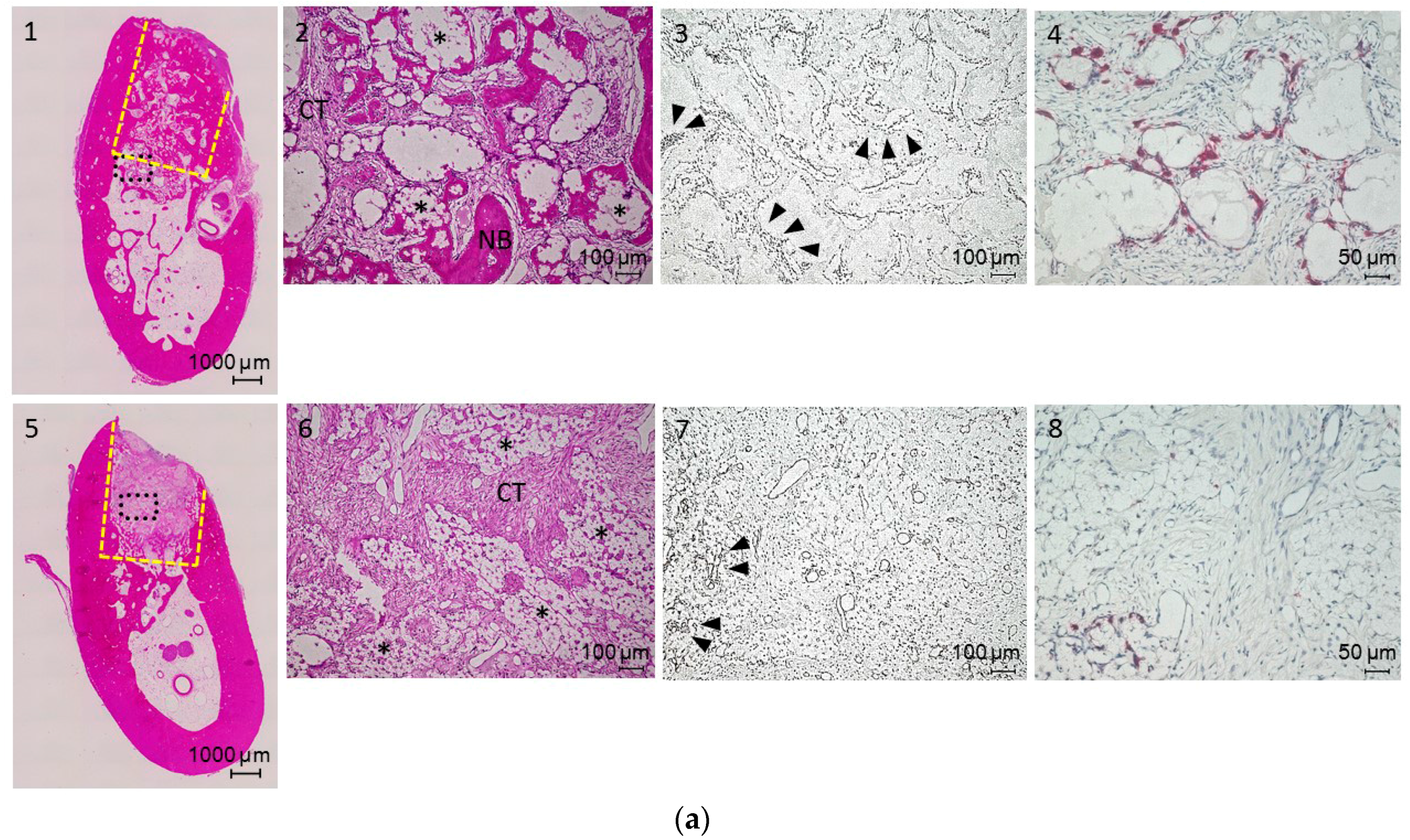
2.3. Histological Assessment
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Surface Modification of α-TCP Particles
4.3. Surface Analysis
4.4. Quantification of Immobilized bFGF
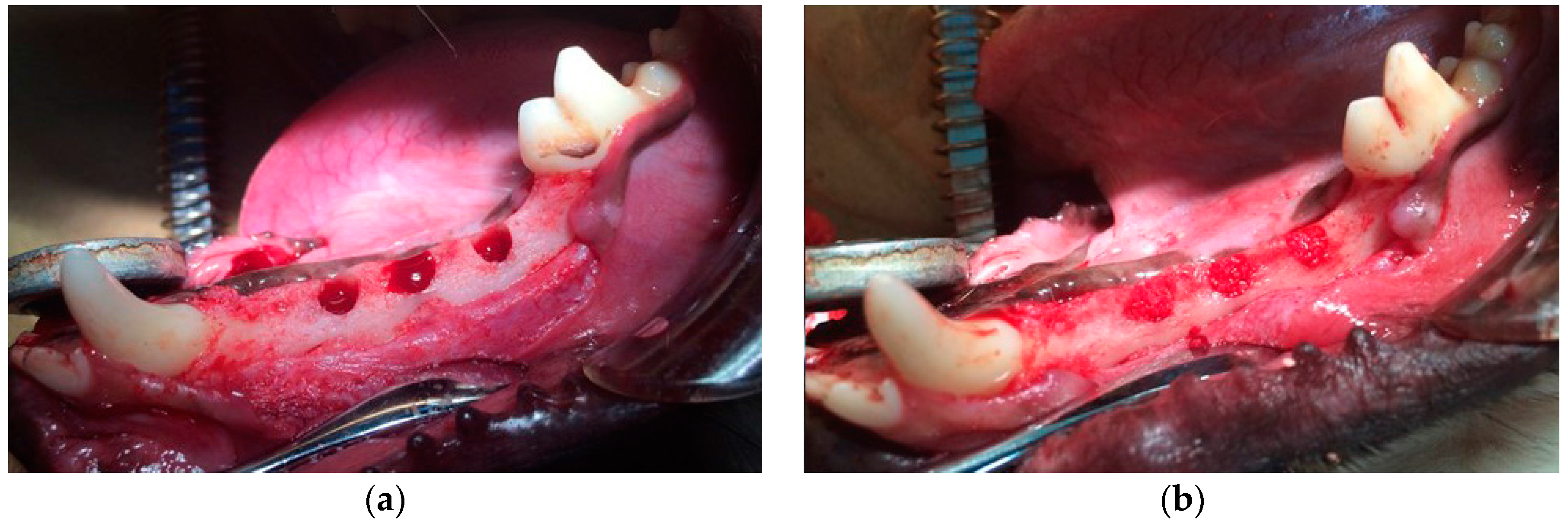
4.5. Canine Mandibular Defect Model
4.6. α-TCP Particle Transplantation
4.7. Radiographic Analysis
4.8. Histological Assessment
4.9. Statistical Analysis
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Matsuno, T.; Nakamura, T.; Kuremoto, K.; Notazawa, S.; Nakahara, T.; Hashimoto, Y.; Satoh, T.; Shimizu, Y. Development of β-tricalcium phosphate/collagen sponge composite for bone regeneration. Dent. Mater. J. 2006, 25, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Omata, K.; Matsuno, T.; Asano, K.; Hashimoto, Y.; Tabata, Y.; Satoh, T. Enhanced bone regeneration by gelatin-β-tricalcium phosphate composites enabling controlled release of bFGF. J. Tissue Eng. Regen. Med. 2014, 8, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Sakai, K.; Hashimoto, Y.; Baba, S.; Nishiura, A.; Matsumoto, N. Effects on bone regeneration when collagen model polypeptides are combined with various sizes of alpha-tricalcium phosphate particles. Dent. Mater. J. 2011, 30, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Weiland, A.J.; Phillips, T.W.; Randolph, M.A. Bone grafts: A radiologic, histologic, and biomechanical model comparing autografts, allografts, and free vascularized bone grafts. Plast. Reconstr. Surg. 1984, 74, 368–379. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, M.; Ohtsuki, C.; Iwasaki, H.; Ogata, S.I.; Tanihara, M.; Miyazaki, T. The controlled resorption of porous α-tricalcium phosphate using a hydroxypropylcellulose coating. J. Mater. Sci. Mater. Med. 2004, 15, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Hashimoto, Y.; Baba, S.; Iseki, T.; Morita, S. Bone regeneration with a collagen model polypeptides/α-tricalcium phosphate sponge in a canine tibia defect model. Implant. Dent. 2015, 24, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Hashimoto, Y.; Honda, Y.; Arima, Y.; Matsumoto, N. The effect of interferon-γ and zoledronate treatment on alpha-tricalcium phosphate/collagen sponge-mediated bone-tissue engineering. Int. J. Mol. Sci. 2015, 16, 25678–25690. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, J.; Anger, D.; Krummenauer, F.; Breitig, D.; Fickert, S.; Guenther, K.P. Biological activity of recombinant human growth factors released from biocompatible bone implants. J. Biomed. Mater. Res. A 2008, 86, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Bierie, B.; Moses, H.L. Tumour microenvironment—TGFB: The molecular jekyll and hyde of cancer. Nat. Rev. Cancer 2006, 6, 506–520. [Google Scholar] [CrossRef] [PubMed]
- Carragee, E.J.; Chu, G.; Rohatgi, R.; Hurwitz, E.L.; Weiner, B.K.; Yoon, S.T.; Comer, G.; Kopjar, B. Cancer risk after use of recombinant bone morphogenetic protein-2 for spinal arthrodesis. J. Bone Jt. Surg. 2013, 95, 1537–1545. [Google Scholar] [CrossRef] [PubMed]
- Tabata, Y.; Yamada, K.; Miyamoto, S.; Nagata, I.; Kikuchi, H.; Aoyama, I.; Tamura, M.; Ikada, Y. Bone regeneration by basic fibroblast growth factor complexed with biodegradable hydrogels. Biomaterials 1998, 19, 807–815. [Google Scholar] [CrossRef]
- Kakinoki, S.; Sakai, Y.; Fujisato, T.; Yamaoka, T. Accelerated tissue integration into porous materials by immobilizing basic fibroblast growth factor using a biologically safe three-step reaction. J. Biomed. Mater. Res. A 2015, 103, 3790–3797. [Google Scholar] [CrossRef] [PubMed]
- Young, C.; Ladd, P.; Browning, C.; Thompson, A.; Bonomo, J.; Shockley, K.; Hart, C. Release, biological potency, and biochemical integrity of recombinant human platelet-derived growth factor-BB (rhPDGF-BB) combined with augment™ bone graft or GEM 21S beta-tricalcium phosphate (β-TCP). J. Control. Release 2009, 140, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Pitaru, S.; Kotev-Emeth, S.; Noff, D.; Kaffuler, S.; Savion, N. Effect of basic fibroblast growth factor on the growth and differentiation of adult stromal bone marrow cells: Enhanced development of mineralized bone-like tissue in culture. J. Bone Miner. Res. 1993, 8, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.; Ladage, D.; Schinköthe, T.; Klausmann, U.; Ulrichs, C.; Klinz, F.J.; Brixius, K.; Arnhold, S.; Desai, B.; Mehlhorn, U.; et al. Basic fibroblast growth factor controls migration in human mesenchymal stem cells. Stem Cells 2006, 24, 1750–1758. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Hara, Y.; Tagawa, M.; Tamura, M.; Yuge, T.; Fukuda, H.; Nigi, H. Recombinant human basic fibroblast growth factor accelerates fracture healing by enhancing callus remodeling in experimental dog tibial fracture. J. Bone Miner. Res. 1998, 13, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Hosokawa, R.; Kikuzaki, K.; Kimoto, T.; Matsuura, T.; Chiba, D.; Wadamoto, M.; Sato, Y.; Maeda, M.; Sano, A.; Akagawa, Y. Controlled local application of basic fibroblast growth factor (FGF-2) accelerates the healing of GBR. Clin. Oral Implants Res. 2000, 11, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Lee, J.; Igawa, K.; Liu, I.-L.; Honnami, M.; Suzuki, S.; Nishimura, R.; Chung, U.-I.; Sasaki, N.; Mochizuki, M. Changes in bone regeneration by trehalose coating and basic fibroblast growth factor after implantation of tailor-made bone implants in dogs. J. Vet. Med. Sci. 2013, 75, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Curran, J.M.; Gallagher, J.A.; Hunt, J.A. The inflammatory potential of biphasic calcium phosphate granules in osteoblast/macrophage co-culture. Biomaterials 2005, 26, 5313–5320. [Google Scholar] [CrossRef] [PubMed]
- Wiltfang, J.; Merten, H.A.; Schlegel, K.A.; Schultze-Mosgau, S.; Kloss, F.R.; Rupprecht, S.; Kessler, P. Degradation characteristics of α and β tri-calcium-phosphate (TCP) in minipigs. J. Biomed. Mater. Res. 2002, 63, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Shiota, M.; Yamashita, Y.; Kasugai, S. Histological and histomorphometrical comparative study of the degradation and osteoconductive characteristics of α- and β-tricalcium phosphate in block grafts. J. Biomed. Mater. Res. B 2007, 82, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; De Bruijn, J.D.; Li, Y.; Feng, J.; Yang, Z.; De Groot, K.; Zhang, X. Bone formation induced by calcium phosphate ceramics in soft tissue of dogs: A comparative study between porous α-TCP and β-TCP. J. Mater. Sci. Mater Med. 2001, 12, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Pri-Chen, S.; Pitaru, S.; Lokiec, F.; Savion, N. Basic fibroblast growth factor enhances the growth and expression of the osteogenic phenotype of dexamethasone-treated human bone marrow-derived bone-like cells in culture. Bone 1998, 23, 111–117. [Google Scholar] [CrossRef]
- Shimizu, A.; Tajima, S.; Tobita, M.; Tanaka, R.; Tabata, Y.; Mizuno, H. Effect of control-released basic fibroblast growth factor incorporated in β-tricalcium phosphate for murine cranial model. Plast. Reconstr. Surg. 2014, 2, e126. [Google Scholar] [CrossRef] [PubMed]
- Carrel, J.P.; Wiskott, A.; Scherrer, S.; Durual, S. Large bone vertical augmentation using a three-dimensional printed TCP/HA bone graft: A pilot study in dog mandible. Clin. Implant Dent. Relat. Res. 2016. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.; Richards, R.; Milz, S.; Schneider, E.; Pearce, S. Animal models for implant biomaterial research in bone: A review. Eur. Cell Mater. 2007, 13, 1–10. [Google Scholar] [PubMed]
- Frost, H.M. Tetracycline-based histological analysis of bone remodeling. Calcif. Tissue Int. 1969, 3, 211–237. [Google Scholar] [CrossRef]
- Verstraete, F.J.; Lommer, M.J. Oral and Maxillofacial Surgery in Dogs and Cats; Saunders/Elsevier: Philadelphia, PA, USA, 2012. [Google Scholar]
- Hashimoto, Y.; Kaida, K.; Uemura, N.; Kimura, D.; Matuse, K.; Ueda, M.; Hirose, M.; Toda, I.; Komuro, A.; Kawaue, Y.; et al. Bone regeneration with a collagen model polypeptide/porous alpha-tricalcium phosphate sponge. J. Oral Tissue Eng. 2016, in press. [Google Scholar]








© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobayashi, N.; Hashimoto, Y.; Otaka, A.; Yamaoka, T.; Morita, S. Porous Alpha-Tricalcium Phosphate with Immobilized Basic Fibroblast Growth Factor Enhances Bone Regeneration in a Canine Mandibular Bone Defect Model. Materials 2016, 9, 853. https://doi.org/10.3390/ma9100853
Kobayashi N, Hashimoto Y, Otaka A, Yamaoka T, Morita S. Porous Alpha-Tricalcium Phosphate with Immobilized Basic Fibroblast Growth Factor Enhances Bone Regeneration in a Canine Mandibular Bone Defect Model. Materials. 2016; 9(10):853. https://doi.org/10.3390/ma9100853
Chicago/Turabian StyleKobayashi, Nobuhiro, Yoshiya Hashimoto, Akihisa Otaka, Tetsuji Yamaoka, and Shosuke Morita. 2016. "Porous Alpha-Tricalcium Phosphate with Immobilized Basic Fibroblast Growth Factor Enhances Bone Regeneration in a Canine Mandibular Bone Defect Model" Materials 9, no. 10: 853. https://doi.org/10.3390/ma9100853
APA StyleKobayashi, N., Hashimoto, Y., Otaka, A., Yamaoka, T., & Morita, S. (2016). Porous Alpha-Tricalcium Phosphate with Immobilized Basic Fibroblast Growth Factor Enhances Bone Regeneration in a Canine Mandibular Bone Defect Model. Materials, 9(10), 853. https://doi.org/10.3390/ma9100853