
Deep Transfer Learning for Parkinson’s Disease Monitoring by Image-Based Representation of Resting-State EEG Using Directional Connectivity


Abstract
:1. Introduction
2. Materials and Methods
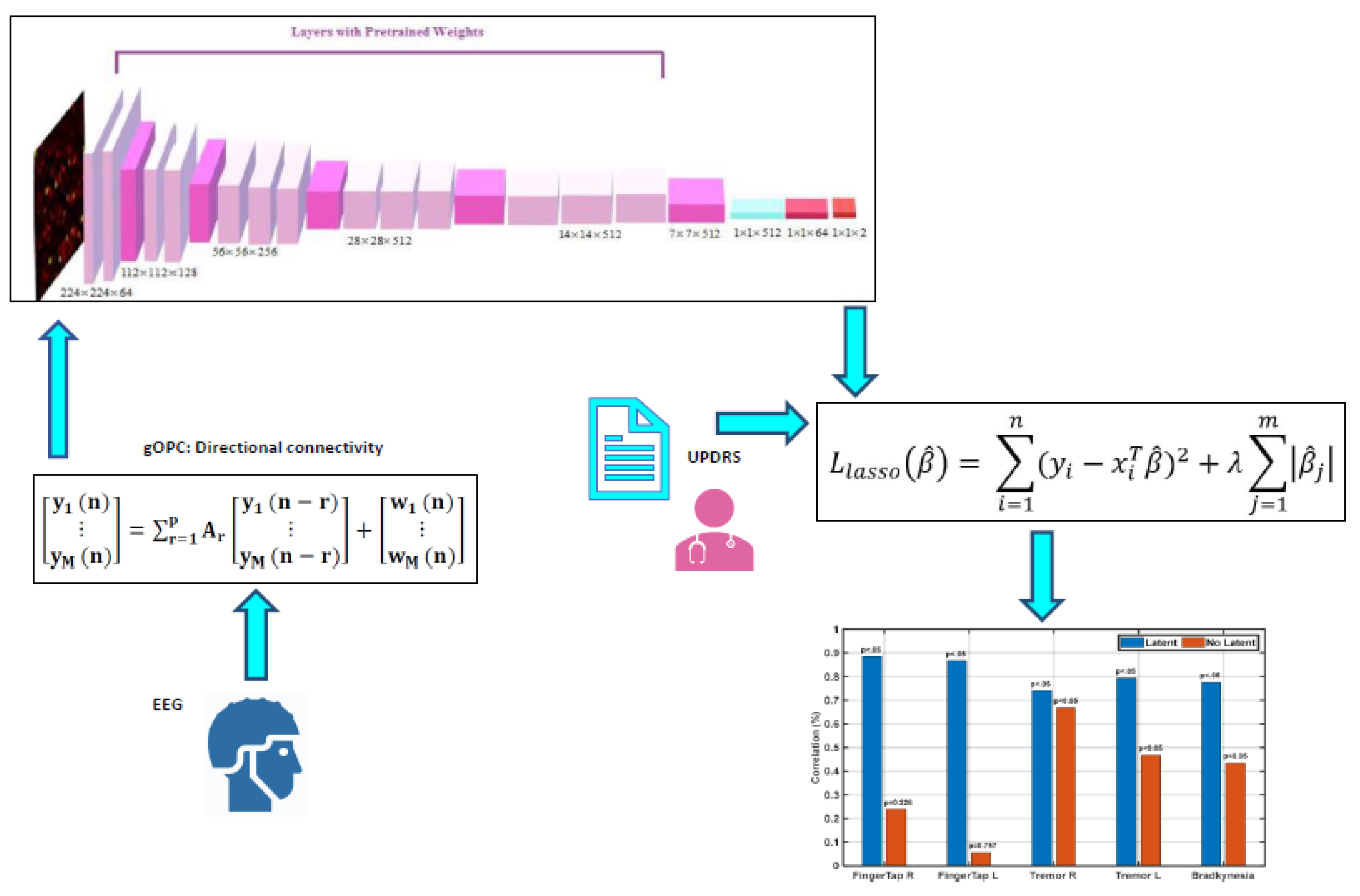
2.1. Overview
2.2. Participants
2.3. Study Protocols
2.4. Recording and Pre-Processing EEG Signals
2.5. Directional Connectivity
2.6. Image-Based Representation of DC
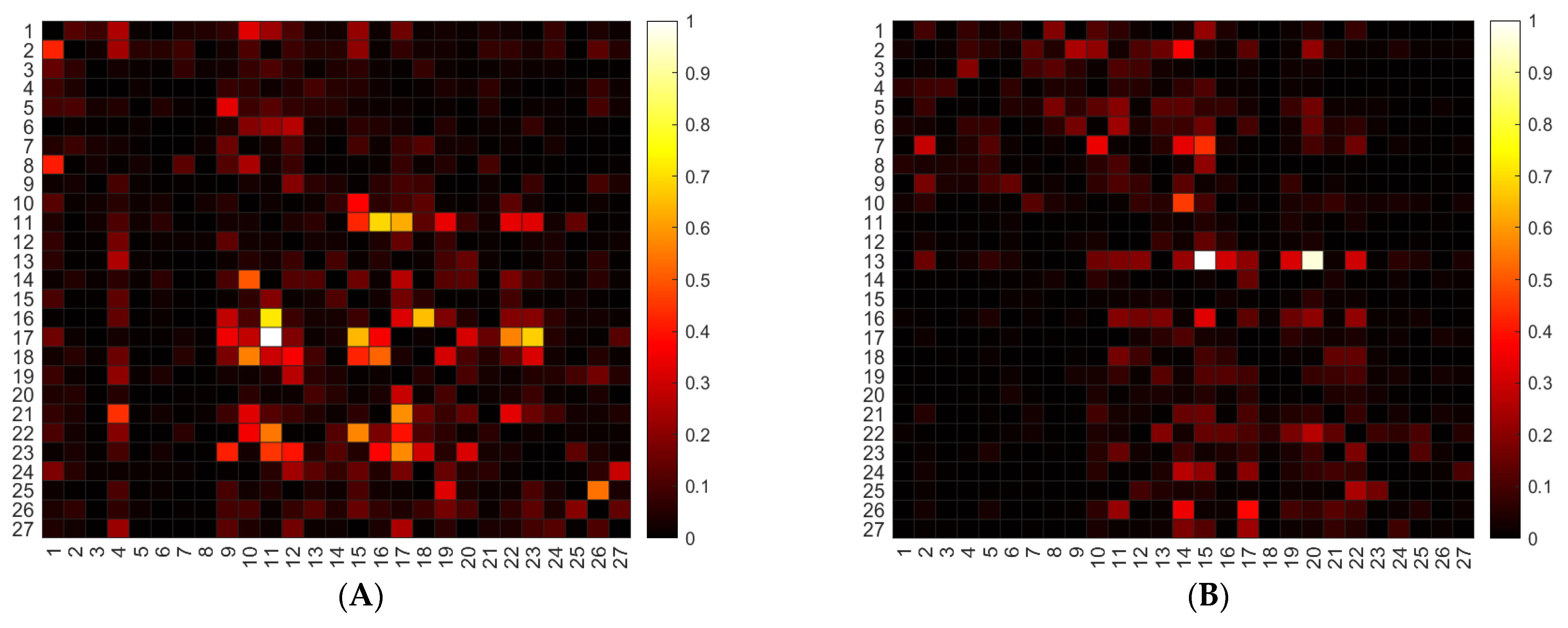
- In order to increase our sample size, for each of the 4 frequency bands, we created 2D matrices (27 × 27) as a heatmap since there were 27 channels, and there were 26 channels that can be directionally connected to each channel (connectivity of a channel with itself is ignored). In order to have a square matrix for sizing of the heatmap, we created a 27 x 27 matrix and set the main diagonal components of the matrix to zero.
- We normalized each matrix individually. In fact, we had normalized each matrix of DC (27 × 27) using the min/max approach.
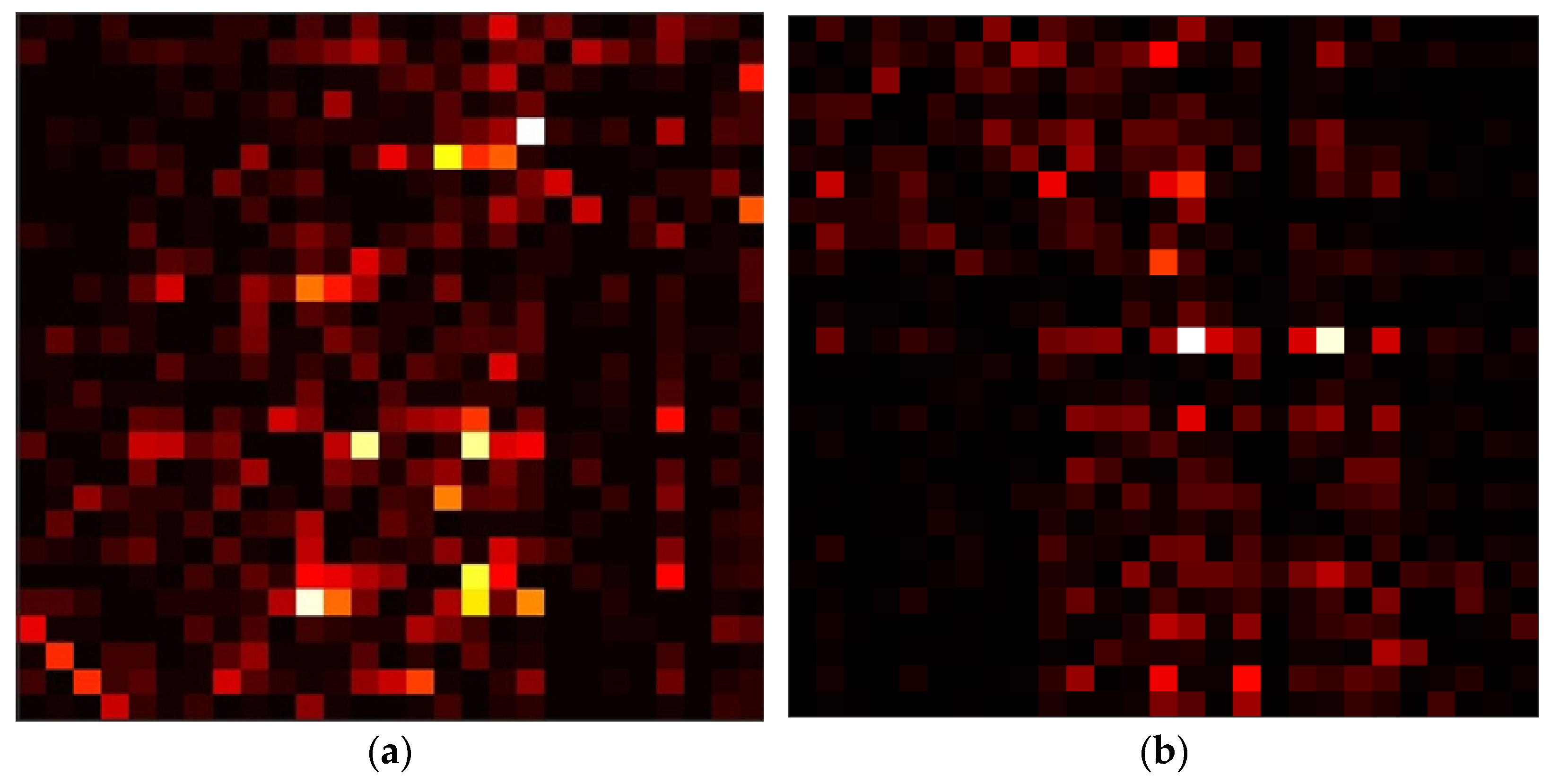
- We represented the results by computing heat maps, i.e., 2D representations of the values in a data matrix, in which colors represent their variability in intensity. Figure 2, as an example, shows two sample heat maps from two PD and HC cases. Larger values were represented by lighter pixels and smaller values by darker pixels.
- We resized the heatmap images to 224 × 224 in order to make them fit the architecture of the VGG-16 architecture.
2.7. Transfer Learning
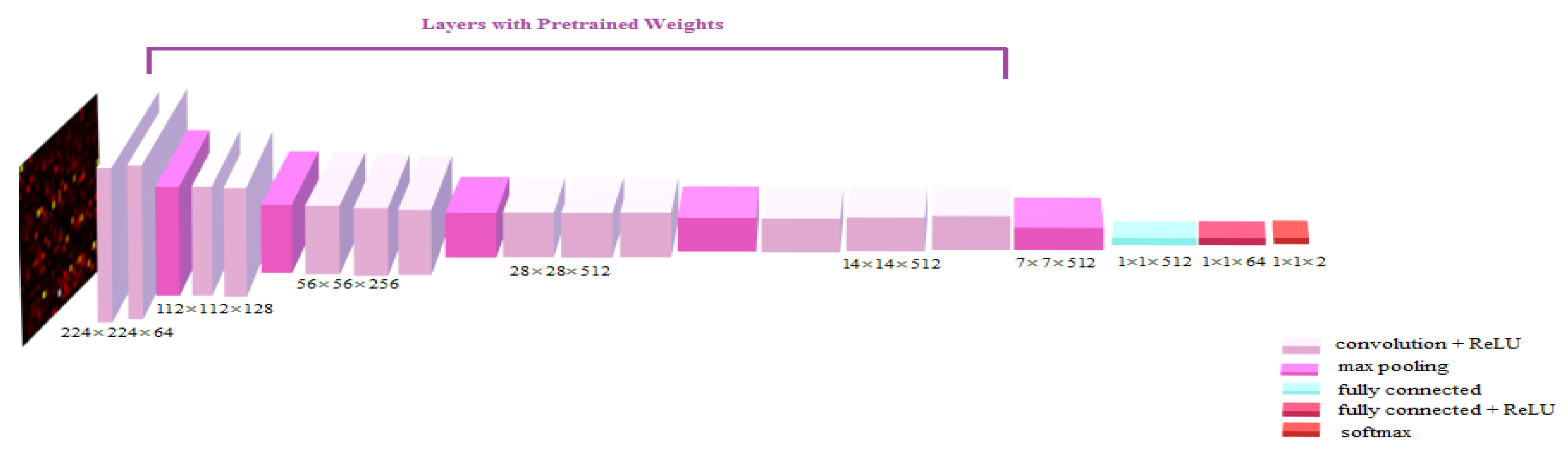
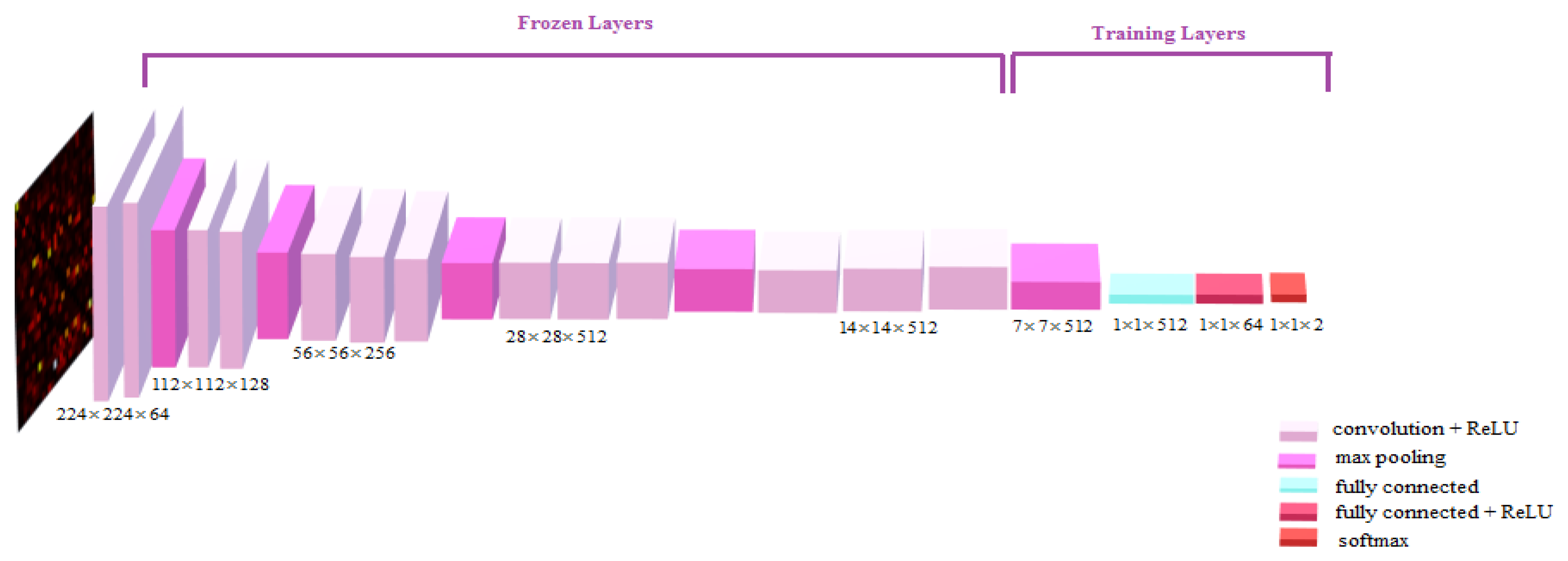
- We used the VGG-16 architecture [35] trained on the ImageNet dataset as our pre-trained model, and we used only weights of convolutional layers of the pre-trained model.
- To better fit our classification task, we modified the base model of VGG-16 in this order: (A) Implementing a fully connected layer (1 × 1 × 512) after the last max-pooling layer (7 × 7 × 512). (B) Developing a fully connected layer (1 × 1 × 64) with activation function of “Relu” to better map reduced features to the last layer. (C) Applying the fully connected layer (1 × 1 × 2) with the activation function of “Softmax” for the classification task consists of two categories, Parkinson’s disease and healthy controls.
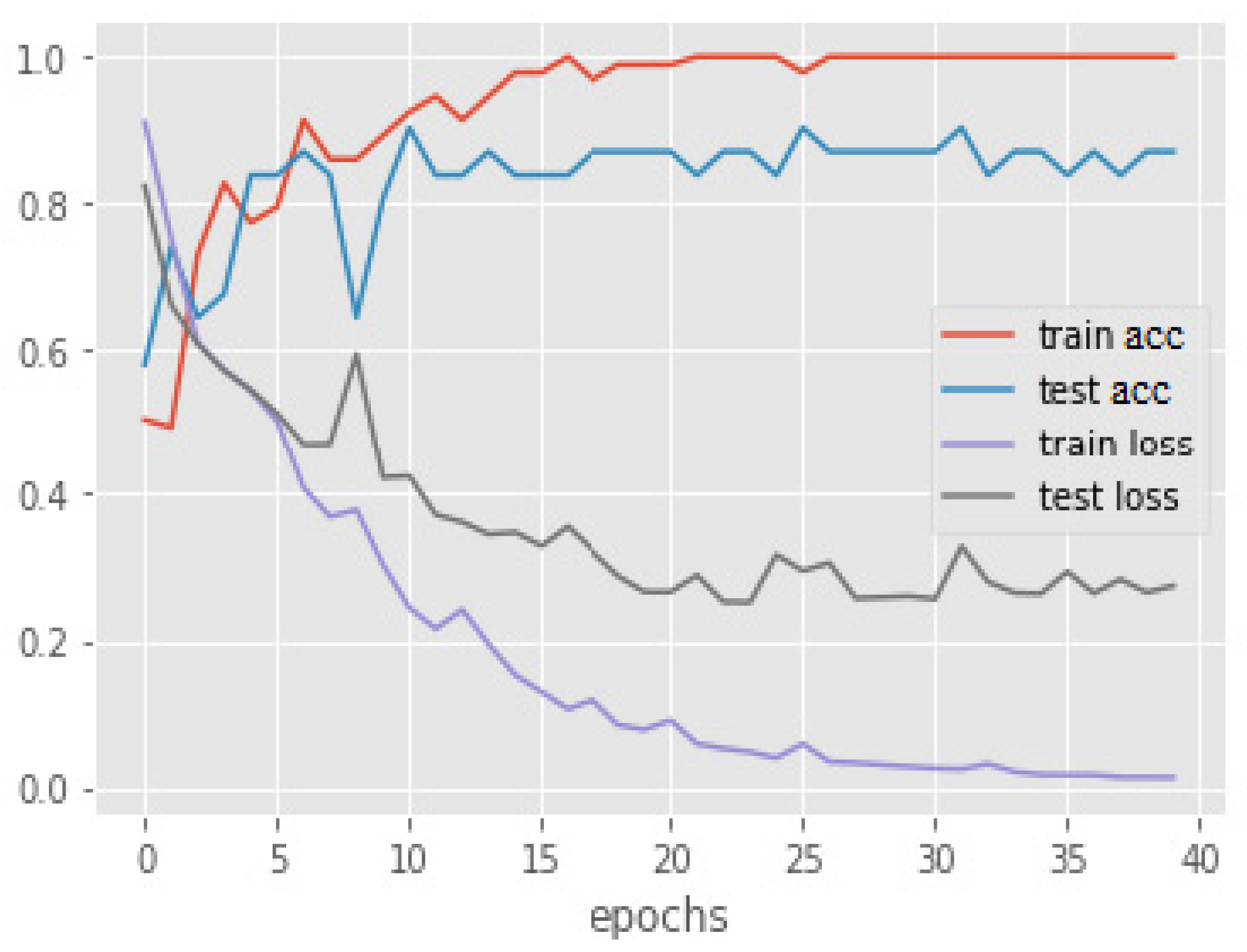
- We tried two techniques of fine-tuning: The network, which we call the Totally trained model, is represented in Figure 3, while the other alternative is represented in the Appendix A just for further information.
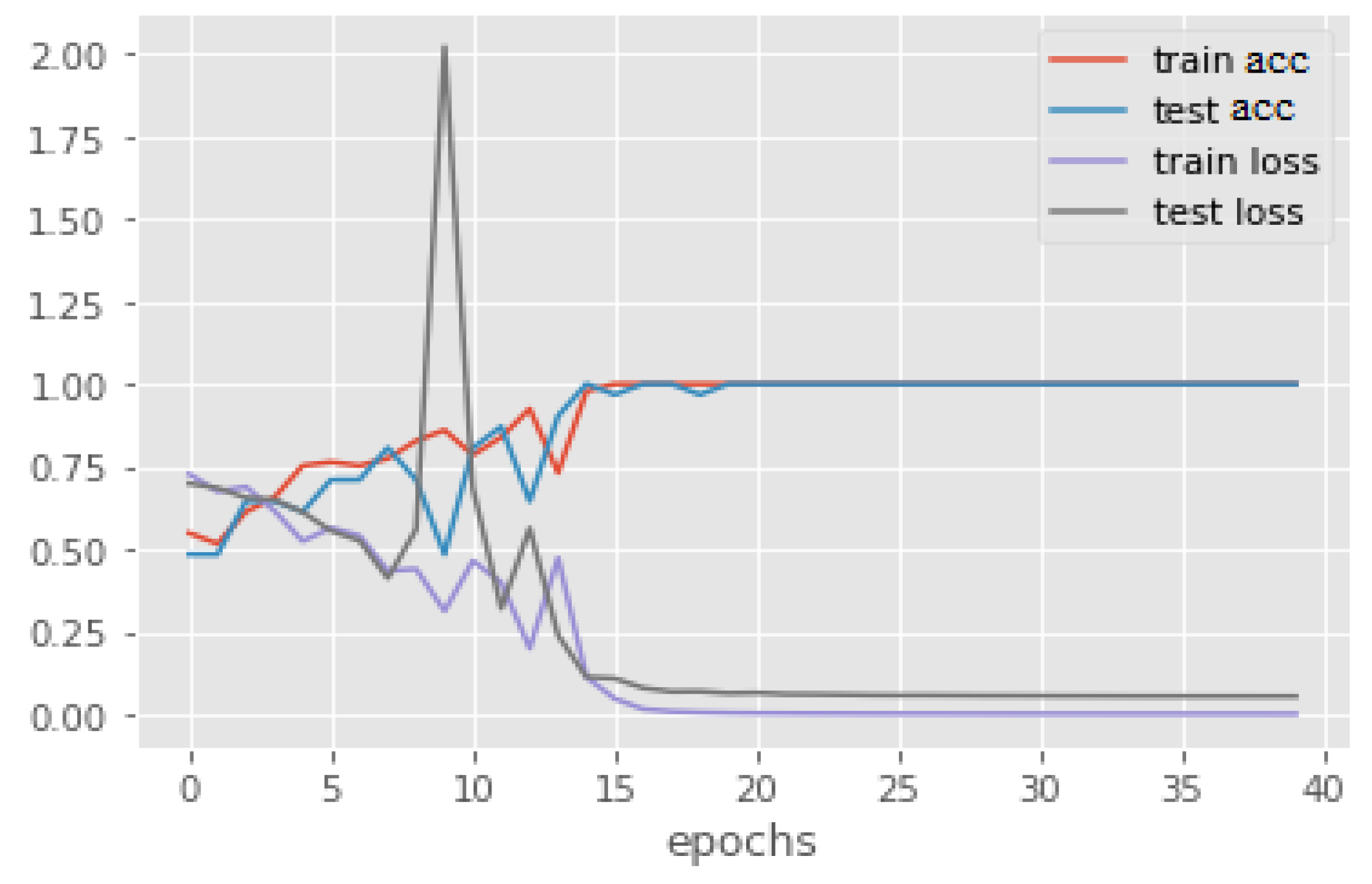
- To implement the first technique, we used weights of convolutional layers as initial weights and updated all layers’ weights with our data. The network architecture is shown in Figure 3. Table 2 and Table 3 represent the details of this network. In addition, Figure A1 shows the best performance of the proposed model over the epochs.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Model | |
|---|---|
| Optimizer | SGD |
| Learning rate | 0.01 |
| Decay | 0.001 |
| Batch size | 8 |
| Loss function | Binary cross entropy |
| Layer | Output Shape | Param |
|---|---|---|
| Functional VGG16 | (None, 7, 7, 512) | 14,714,688 |
| Max Pooling | (None, 1, 1, 512) | 0 |
| Flatten | (None, 512) | 0 |
| Dense | (None, 64) | 32,832 |
| Dense | (None, 2) | 130 |
| Total params: 14,747,650 Trainable params: 14,747,650 Non-trainable params: 0 |
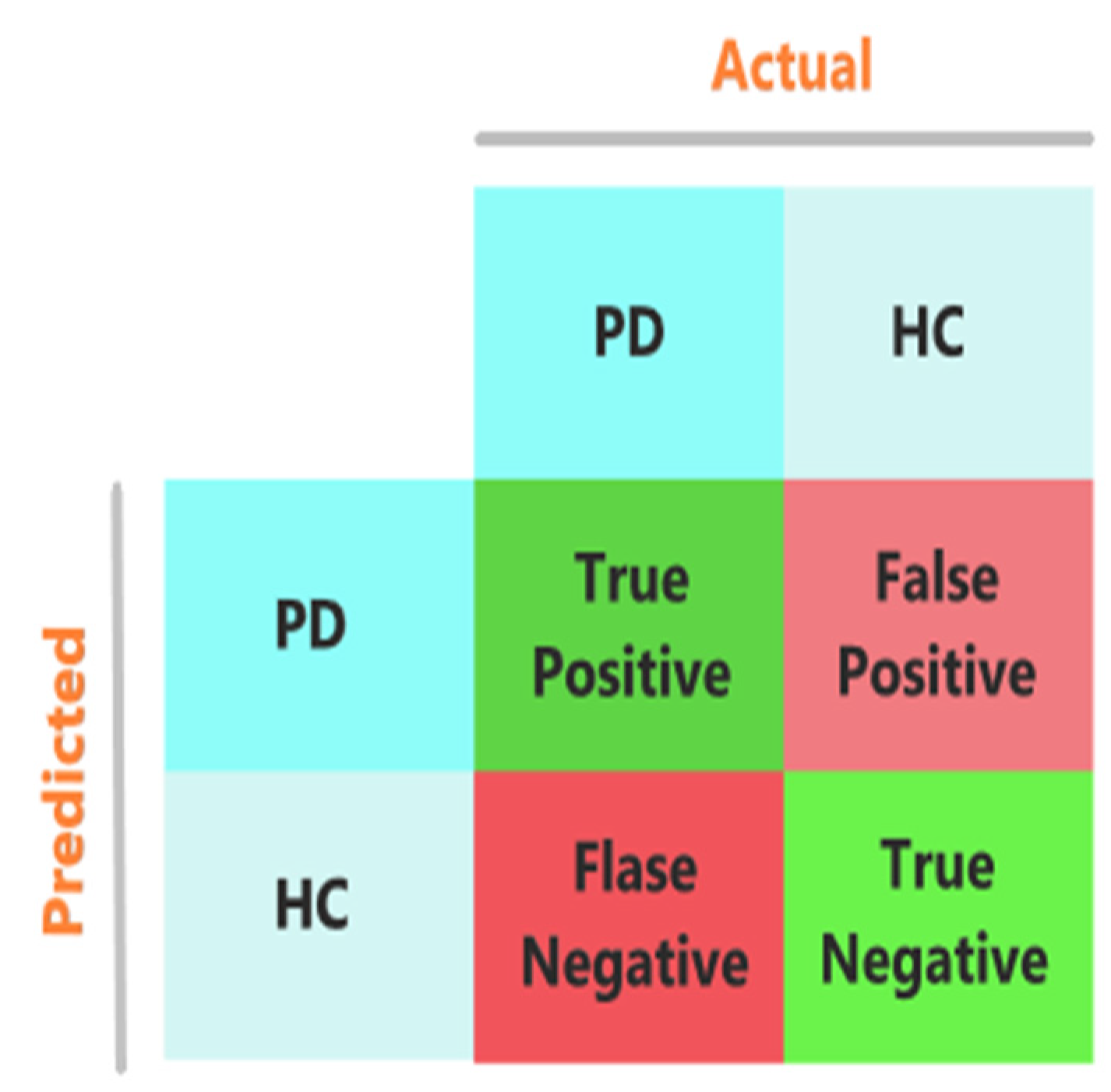
2.8. Performance Evaluation
2.9. Feature Extraction from the Network
3. Results
3.1. PD Classification Performance
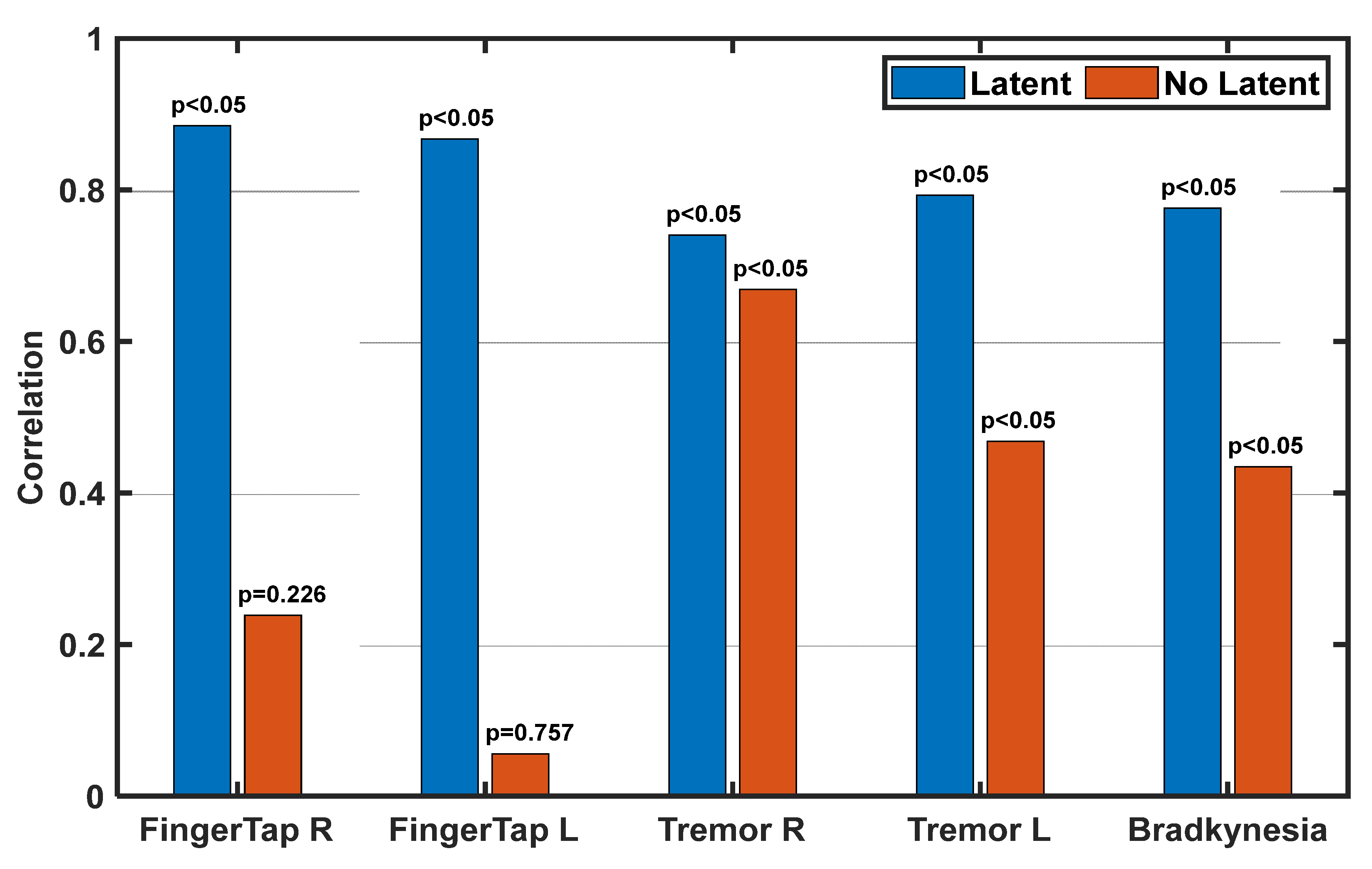
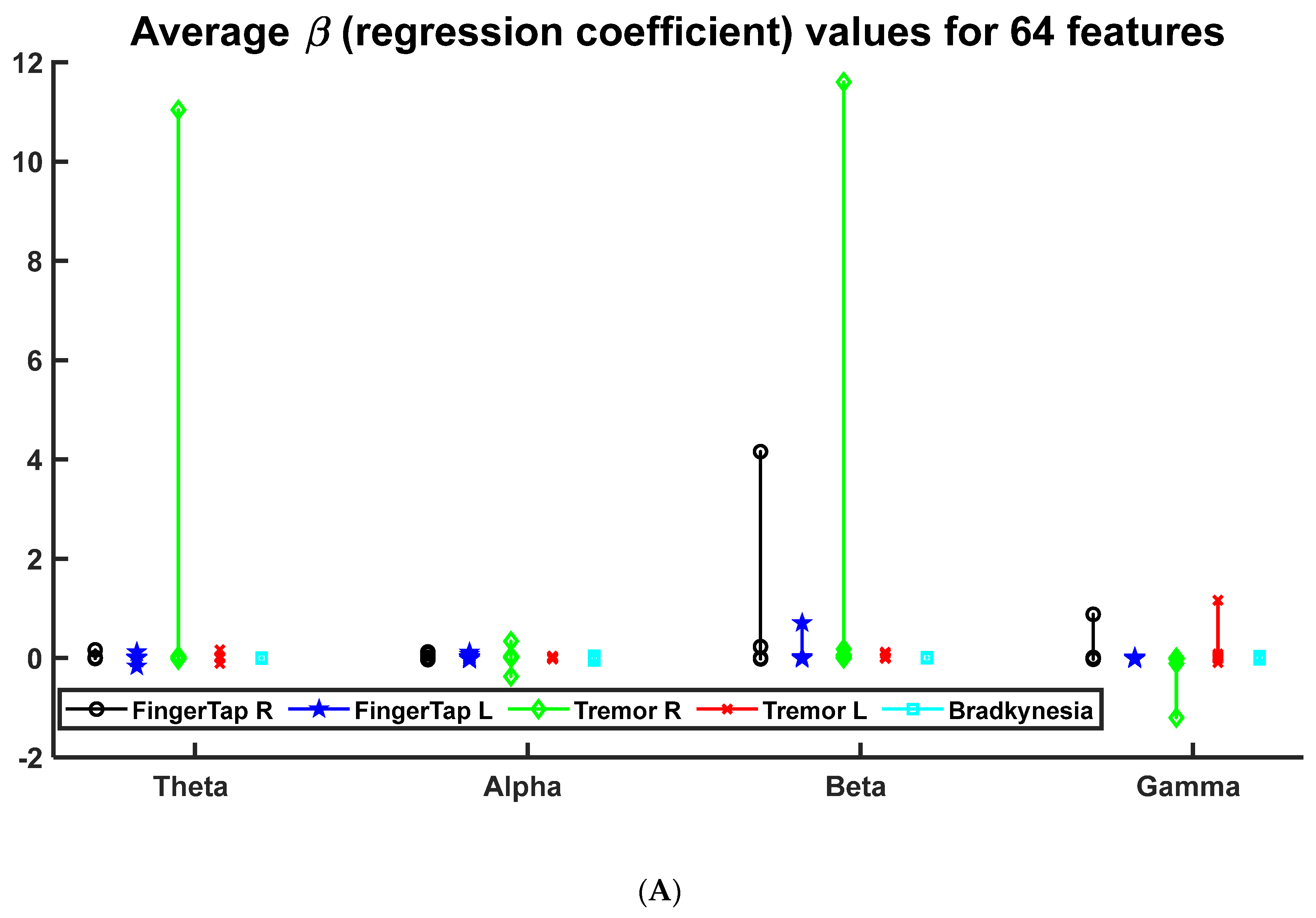
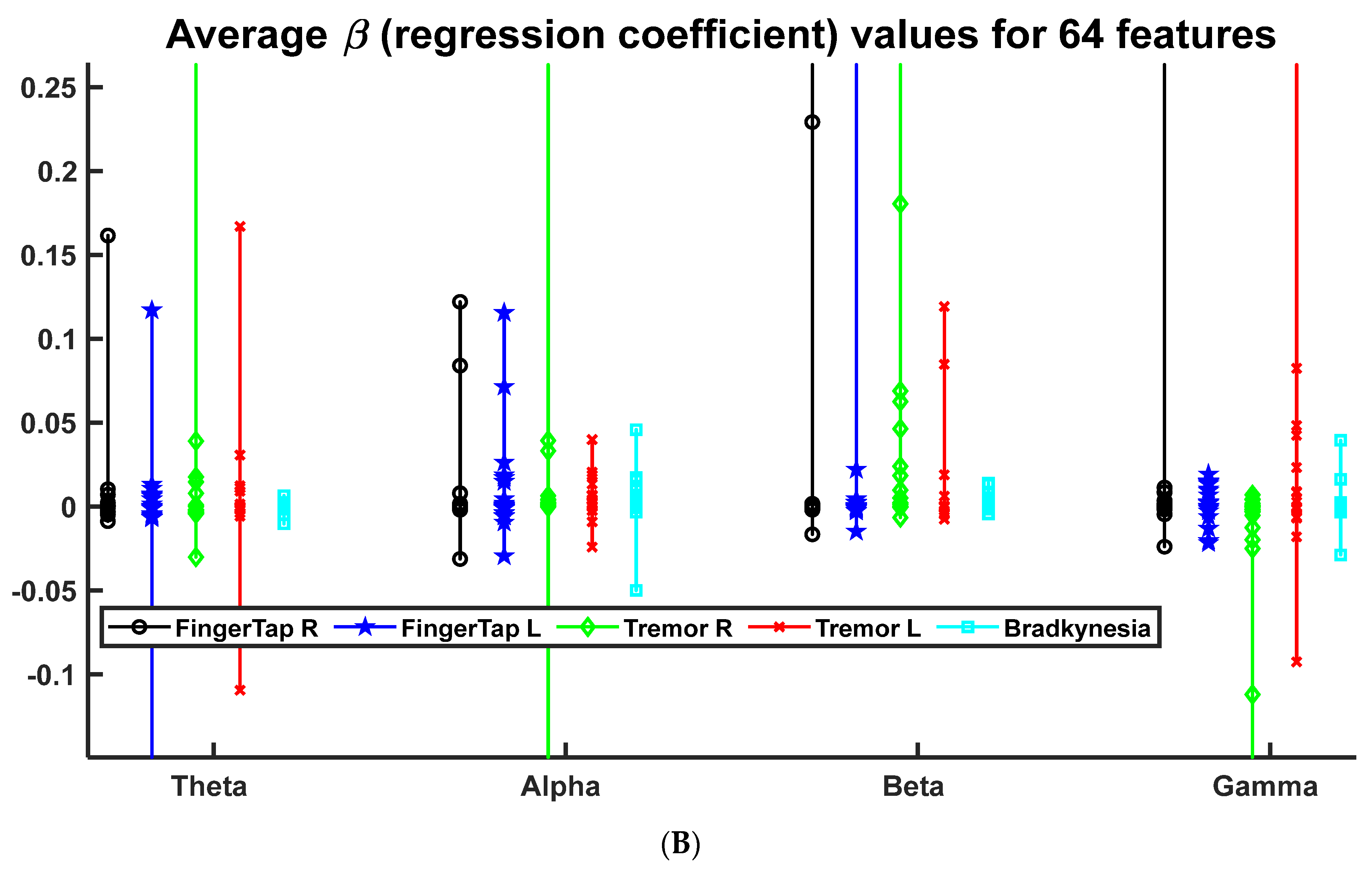
3.2. Clinical Relevance of Deep-Transfer-Learning-Based Classification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


| First Model | |
|---|---|
| Optimizer | Adam |
| Learning rate | 0.01 |
| Decay | 0.001 |
| Batch size | 8 |
| Loss function | Binary cross entropy |
| Layer | Output Shape | Param |
|---|---|---|
| Functional VGG16 | (None, 7, 7, 512) | 14,714,688 |
| Max Pooling | (None, 1, 1, 512) | 0 |
| Flatten | (None, 512) | 0 |
| Dense | (None, 64) | 32,832 |
| Dense | (None, 2) | 130 |
| Total params: 14,747,650 Trainable params: 32,962 Non-trainable params: 14,714,688 |




References
- Scandalis, T.A.; Bosak, A.; Berliner, J.C.; Helman, L.L.; Wells, M.R. Resistance training and gait function in patients with Parkinson’s disease. Am. J. Phys. Med. Rehabil. 2001, 80, 38–43. [Google Scholar] [CrossRef]
- Braak, H.; Del Tredici, K.; Rüb, U.; De Vos, R.A.; Steur, E.N.J.; Braak, E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Brooks, D.J.; Piccini, P. Imaging in Parkinson’s disease: The role of monoamines in behavior. Biol. Psychiatry 2006, 59, 908–918. [Google Scholar] [CrossRef] [PubMed]
- Rivlin-Etzion, M.; Marmor, O.; Heimer, G.; Raz, A.; Nini, A.; Bergman, H. Basal ganglia oscillations and pathophysiology of movement disorders. Curr. Opin. Neurobiol. 2006, 16, 629–637. [Google Scholar] [CrossRef]
- Helmich, R.C.; Derikx, L.C.; Bakker, M.; Scheeringa, R.; Bloem, B.R.; Toni, I. Spatial remapping of cortico-striatal connectivity in Parkinson’s disease. Cereb. Cortex 2010, 20, 1175–1186. [Google Scholar] [CrossRef] [Green Version]
- Seibert, T.M.; Murphy, E.A.; Kaestner, E.J.; Brewer, J.B. Interregional correlations in Parkinson disease and Parkinson-related dementia with resting functional MR imaging. Radiology 2012, 263, 226–234. [Google Scholar] [CrossRef] [Green Version]
- Han, C.-X.; Wang, J.; Yi, G.-S.; Che, Y.-Q. Investigation of EEG abnormalities in the early stage of Parkinson’s disease. Cogn. Neurodynamics 2013, 7, 351–359. [Google Scholar] [CrossRef]
- Lee, S.; Hussein, R.; Ward, R.; Wang, Z.J.; McKeown, M.J. A convolutional-recurrent neural network approach to resting-state EEG classification in Parkinson’s disease. J. Neurosci. Methods 2021, 361, 109282. [Google Scholar] [CrossRef] [PubMed]
- McBride, J.C.; Zhao, X.; Munro, N.B.; Smith, C.D.; Jicha, G.A.; Hively, L.; Broster, L.S.; Schmitt, F.A.; Kryscio, R.J.; Jiang, Y. Spectral and complexity analysis of scalp EEG characteristics for mild cognitive impairment and early Alzheimer’s disease. Comput. Methods Programs Biomed. 2014, 114, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.; Akrofi, K.; Schiffer, R.; O’Boyle, M.W. EEG patterns in mild cognitive impairment (MCI) patients. Open Neuroimag. J. 2008, 2, 52. [Google Scholar] [CrossRef]
- Vialatte, F.; Cichocki, A.; Dreyfus, G.; Musha, T.; Rutkowski, T.M.; Gervais, R. Blind source separation and sparse bump modelling of time frequency representation of EEG signals: New tools for early detection of Alzheimer’s disease. In Proceedings of the 2005 IEEE Workshop on Machine Learning for Signal Processing, Mystic, CT, USA, 28 September 2005. [Google Scholar]
- Khare, S.K.; Bajaj, V.; Acharya, U.R. PDCNNet: An automatic framework for the detection of Parkinson’s Disease using EEG signals. IEEE Sens. J. 2021, 21, 17017–17024. [Google Scholar] [CrossRef]
- Krishna, N.M.; Sekaran, K.; Vamsi, A.V.N.; Ghantasala, G.P.; Chandana, P.; Kadry, S.; Blažauskas, T.; Damaševičius, R. An efficient mixture model approach in brain-machine interface systems for extracting the psychological status of mentally impaired persons using EEG signals. IEEE Access 2019, 7, 77905–77914. [Google Scholar] [CrossRef]
- Akrofi, K.; Pal, R.; Baker, M.C.; Nutter, B.S.; Schiffer, R.W. Classification of Alzheimer’s disease and mild cognitive impairment by pattern recognition of EEG power and coherence. In Proceedings of the 2010 IEEE International Conference on Acoustics, Speech and Signal Processing, Dallas, TX, USA, 14–19 March 2010. [Google Scholar]
- Oh, S.L.; Hagiwara, Y.; Raghavendra, U.; Yuvaraj, R.; Arunkumar, N.; Murugappan, M.; Acharya, U.R. A deep learning approach for Parkinson’s disease diagnosis from EEG signals. Neural Comput. Appl. 2020, 32, 10927–10933. [Google Scholar] [CrossRef]
- Kwak, Y.; Kong, K.; Song, W.-J.; Min, B.-K.; Kim, S.-E. Multilevel feature fusion with 3d convolutional neural network for eeg-based workload estimation. IEEE Access 2020, 8, 16009–16021. [Google Scholar] [CrossRef]
- Wen, D.; Li, P.; Li, X.; Wei, Z.; Zhou, Y.; Pei, H.; Li, F.; Bian, Z.; Wang, L.; Yin, S. The feature extraction of resting-state EEG signal from amnestic mild cognitive impairment with type 2 diabetes mellitus based on feature-fusion multispectral image method. Neural Netw. 2020, 124, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Omidvarnia, A.H.; Azemi, G.; Boashash, B.; O’Toole, J.M.; Colditz, P.; Vanhatalo, S. Orthogonalized partial directed coherence for functional connectivity analysis of newborn EEG. In Proceedings of the International Conference on Neural Information Processing, Doha, Qatar, 12–15 November 2012; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Granger, C.W. Investigating causal relations by econometric models and cross-spectral methods. Econom. J. Econom. Soc. 1969, 37, 424–438. [Google Scholar] [CrossRef]
- Astolfi, L.; Cincotti, F.; Mattia, D.; Fallani, F.D.V.; Tocci, A.; Colosimo, A.; Salinari, S.; Marciani, M.G.; Hesse, W.; Witte, H. Tracking the time-varying cortical connectivity patterns by adaptive multivariate estimators. IEEE Trans. Biomed. Eng. 2008, 55, 902–913. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Liu, A.; Wang, Z.J.; McKeown, M.J. Abnormal phase coupling in Parkinson’s disease and normalization effects of subthreshold vestibular stimulation. Front. Hum. Neurosci. 2019, 13, 118. [Google Scholar] [CrossRef] [Green Version]
- Clemmensen, L.; Hastie, T.; Witten, D.; Ersbøll, B. Sparse discriminant analysis. Technometrics 2011, 53, 406–413. [Google Scholar] [CrossRef] [Green Version]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression and mortality. Neurology 2001, 57, S11–S26. [Google Scholar]
- Lee, S.; Liu, A.; McKeown, M.J. Current perspectives on galvanic vestibular stimulation in the treatment of Parkinson’s disease. Expert Rev. Neurother. 2021, 21, 405–418. [Google Scholar] [CrossRef]
- Baccala, L.A.; Sameshima, K.; Ballester, G.; do Valle, A.C.; Timo-Iaria, C. Studying the interaction between brain structures via directed coherence and Granger causality. Appl. Signal Process. 1998, 5, 40. [Google Scholar] [CrossRef]
- Tropini, G.; Chiang, J.; Wang, Z.J.; Ty, E.; McKeown, M.J. Altered directional connectivity in Parkinson’s disease during performance of a visually guided task. Neuroimage 2011, 56, 2144–2156. [Google Scholar] [CrossRef] [PubMed]
- Omidvarnia, A.; Azemi, G.; Boashash, B.; O’Toole, J.M.; Colditz, P.B.; Vanhatalo, S. Measuring time-varying information flow in scalp EEG signals: Orthogonalized partial directed coherence. IEEE Trans. Biomed. Eng. 2013, 61, 680–693. [Google Scholar] [CrossRef]
- Baccalá, L.A.; Sameshima, K. Partial directed coherence: A new concept in neural structure determination. Biol. Cybern. 2001, 84, 463–474. [Google Scholar] [CrossRef]
- Baccala, L.A.; Sameshima, K.; Takahashi, D.Y. Generalized partial directed coherence. In Proceedings of the 2007 15th International Conference on Digital Signal Processing, Cardiff, UK, 1–4 July 2007. [Google Scholar]
- Brunner, C.; Billinger, M.; Seeber, M.; Mullen, T.R.; Makeig, S. Volume conduction influences scalp-based connectivity estimates. Front. Comput. Neurosci. 2016, 10, 121. [Google Scholar] [CrossRef] [Green Version]
- Hipp, J.F.; Hawellek, D.J.; Corbetta, M.; Siegel, M.; Engel, A.K. Large-scale cortical correlation structure of spontaneous oscillatory activity. Nat. Neurosci. 2012, 15, 884–890. [Google Scholar] [CrossRef] [Green Version]
- Tan, C.; Sun, F.; Kong, T.; Zhang, W.; Yang, C.; Liu, C. A survey on deep transfer learning. In Proceedings of the International Conference on Artificial Neural Networks, Rhodes, Greece, 4–7 October 2018; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Donahue, J.; Jia, Y.; Vinyals, O.; Hoffman, J.; Zhang, N.; Tzeng, E.; Darrell, T. Decaf: A deep convolutional activation feature for generic visual recognition. In Proceedings of the International Conference on Machine Learning, Beijing, China, 21–26 June 2014. [Google Scholar]
- Zeiler, M.D.; Fergus, R. Stochastic pooling for regularization of deep convolutional neural networks. In Proceedings of the 1st International Conference on Learning Representations, Scottsdale, AZ, USA, 2–4 May 2013. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. In Proceedings of the The 3rd International Conference on Learning Representations, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Drysdale, A.T.; Grosenick, L.; Downar, J.; Dunlop, K.; Mansouri, F.; Meng, Y.; Fetcho, R.N.; Zebley, B.; Oathes, D.J.; Etkin, A. Resting-state connectivity biomarkers define neurophysiological subtypes of depression. Nat. Med. 2017, 23, 28–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacAskill, M.R.; Graham, C.F.; Pitcher, T.L.; Myall, D.J.; Livingston, L.; van Stockum, S.; Dalrymple-Alford, J.C.; Anderson, T.J. The influence of motor and cognitive impairment upon visually-guided saccades in Parkinson’s disease. Neuropsychologia 2012, 50, 3338–3347. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression shrinkage and selection via the lasso. J. R. Stat. Soc. Ser. B Methodol. 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Kazemi, A.; Mirian, M.; Lee, S.; McKeown, M. Galvanic Vestibular Stimulation Effects on EEG Biomarkers of Motor Vigor in Parkinson’s Disease. Front. Neurol. 2021, 12, 759149. [Google Scholar] [CrossRef] [PubMed]
- Li, J.Y.; Espay, A.J.; Gunraj, C.A.; Pal, P.K.; Cunic, D.I.; Lang, A.E.; Chen, R. Interhemispheric and ipsilateral connections in Parkinson’s disease: Relation to mirror movements. Mov. Disord. 2007, 22, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Hou, Y.; Hallett, M.; Zhang, J.; Chan, P. Lateralization of brain activity pattern during unilateral movement in Parkinson’s disease. Hum. Brain Mapp. 2015, 36, 1878–1891. [Google Scholar] [CrossRef]
- Little, S.; Brown, P. The functional role of beta oscillations in Parkinson’s disease. Parkinsonism Relat. Disord. 2014, 20, S44–S48. [Google Scholar] [CrossRef]
- DTL-GOPDC. Available online: https://github.com/DTL-GOPDC (accessed on 19 December 2021).








| PD (n = 15) | HC (n = 18) | |
|---|---|---|
| Age (year) | 67.3 ± 6.5 | 67.6 ± 8.9 |
| Sex (male/female) | 7/8 | 9/9 |
| Disease Duration (years), mean (std) | 7.4 (4.3) | - |
| UPDRS II, mean (std) | 14.8 (8.1) | - |
| UPDRS III, mean (std) | 23.3 (9.1) | - |
| Hoehn and Yahr scale, mean | 1.3 (1–2) | - |
| Totally-Trained Model | Limited-Trained Model | |
|---|---|---|
| Train accuracy | 1.00 | 1.00 |
| Test accuracy | 1.00 | 0.871 |
| Train loss | 0.0004 | 0.013 |
| Test loss | 0.053 | 0.274 |
| Proposed | CRNN [8] | SVM-RBF [8] | [15] | |
|---|---|---|---|---|
| Accuracy (%) | 99.6 | 99.2 | 95.4 | 95.4 |
| Precision (%) | 100 | 98.9 | 96.3 | 95.2 |
| Recall (%) | 99.17 | 99.4 | 94.3 | 95.5 |
| F1 score | 0.995 | 0.992 | 0.953 | 0.953 |
| AUC (area under the ROC curve) | 0.995 | 0.992 | 0.954 | 0.954 |
| Clinical Test | Right Finger Tap | Left Finger Tap | Right Tremor | Left Tremor | Bradykinesia |
|---|---|---|---|---|---|
| t-test | 6.0533 | 10.15 | 7.63 | 5.07 | 4.12 |
| p-value | <1 × 10−7 | <2 × 10−14 | <3 × 10−10 | <5 × 10−6 | <2 × 10−4 |
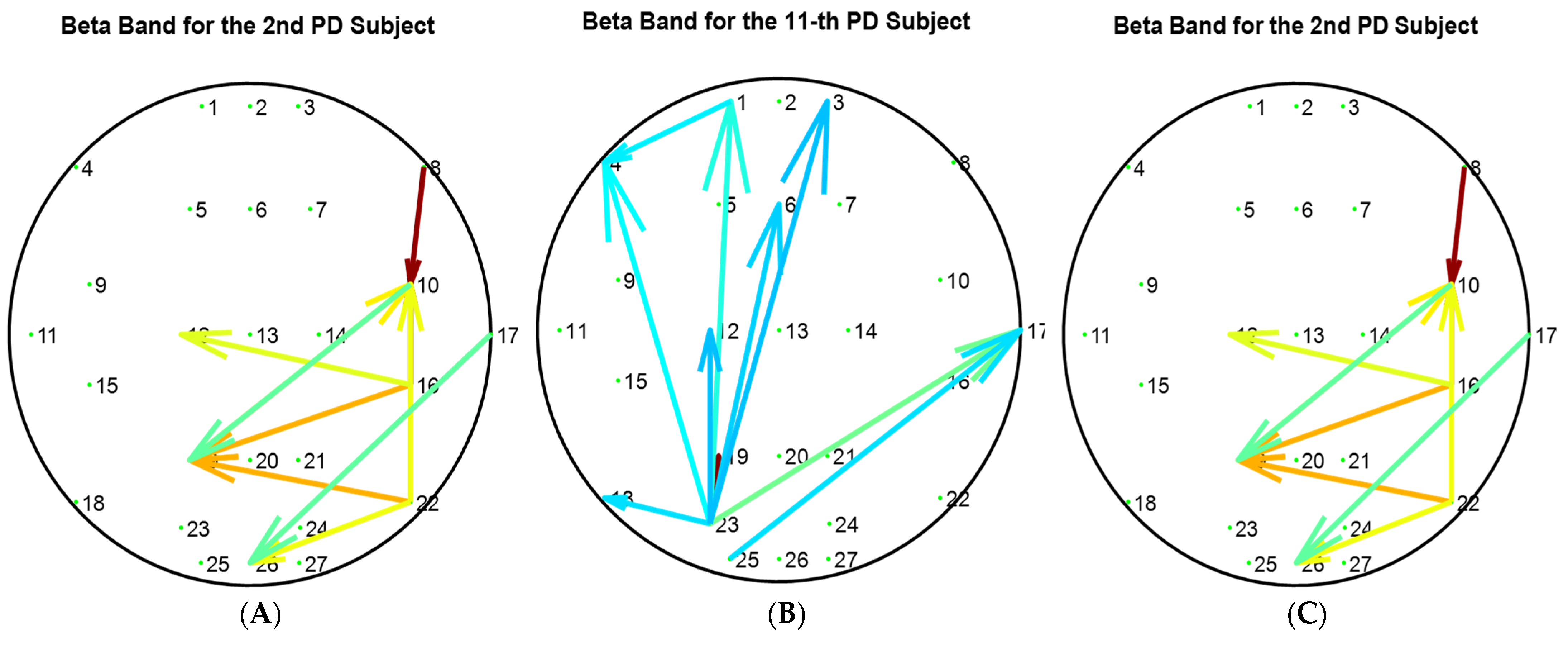
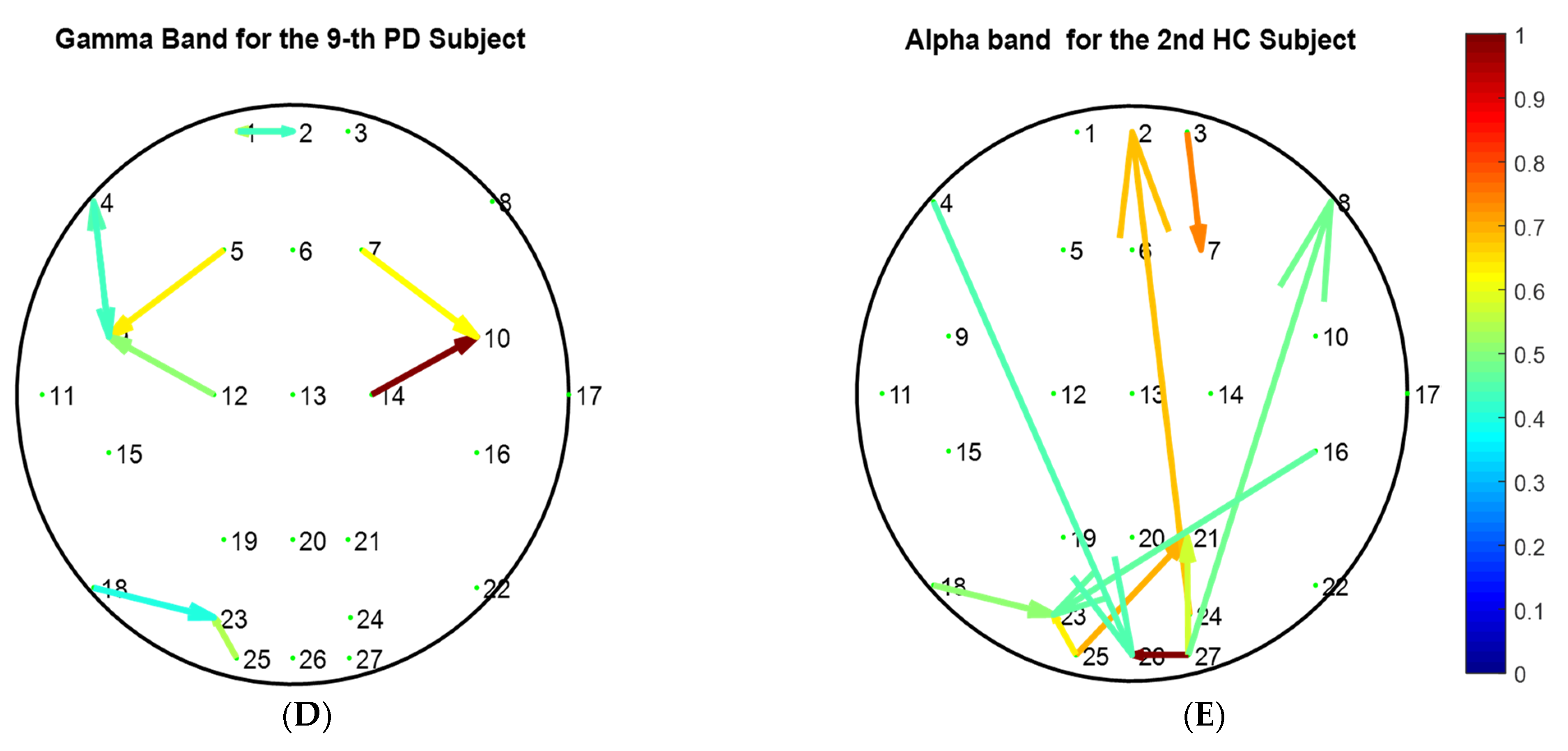
| Clinical Test | Right Finger Tap | Left Finger Tap | Right Tremor | Left Tremor | Bradykinesia |
|---|---|---|---|---|---|
| Subject | 2 | 11 | 2 | 9 | 2 |
| Health Status | PD | PD | PD | PD | HC |
| Frequency Sub-Band | Beta | Beta | Beta | Gamma | Alpha |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arasteh, E.; Mahdizadeh, A.; Mirian, M.S.; Lee, S.; McKeown, M.J. Deep Transfer Learning for Parkinson’s Disease Monitoring by Image-Based Representation of Resting-State EEG Using Directional Connectivity. Algorithms 2022, 15, 5. https://doi.org/10.3390/a15010005
Arasteh E, Mahdizadeh A, Mirian MS, Lee S, McKeown MJ. Deep Transfer Learning for Parkinson’s Disease Monitoring by Image-Based Representation of Resting-State EEG Using Directional Connectivity. Algorithms. 2022; 15(1):5. https://doi.org/10.3390/a15010005
Chicago/Turabian StyleArasteh, Emad, Ailar Mahdizadeh, Maryam S. Mirian, Soojin Lee, and Martin J. McKeown. 2022. "Deep Transfer Learning for Parkinson’s Disease Monitoring by Image-Based Representation of Resting-State EEG Using Directional Connectivity" Algorithms 15, no. 1: 5. https://doi.org/10.3390/a15010005
APA StyleArasteh, E., Mahdizadeh, A., Mirian, M. S., Lee, S., & McKeown, M. J. (2022). Deep Transfer Learning for Parkinson’s Disease Monitoring by Image-Based Representation of Resting-State EEG Using Directional Connectivity. Algorithms, 15(1), 5. https://doi.org/10.3390/a15010005