NS1 Antigenemia and Viraemia Load: Potential Markers of Progression to Dengue Fatal Outcome?

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Dengue and Fatal Dengue Cases
2.3. NS1 Antigenemia Quantification
2.4. Real Time RT-PCR (qRT-PCR) Assay for Viremia Quantification
2.5. Statistical Analysis
3. Results
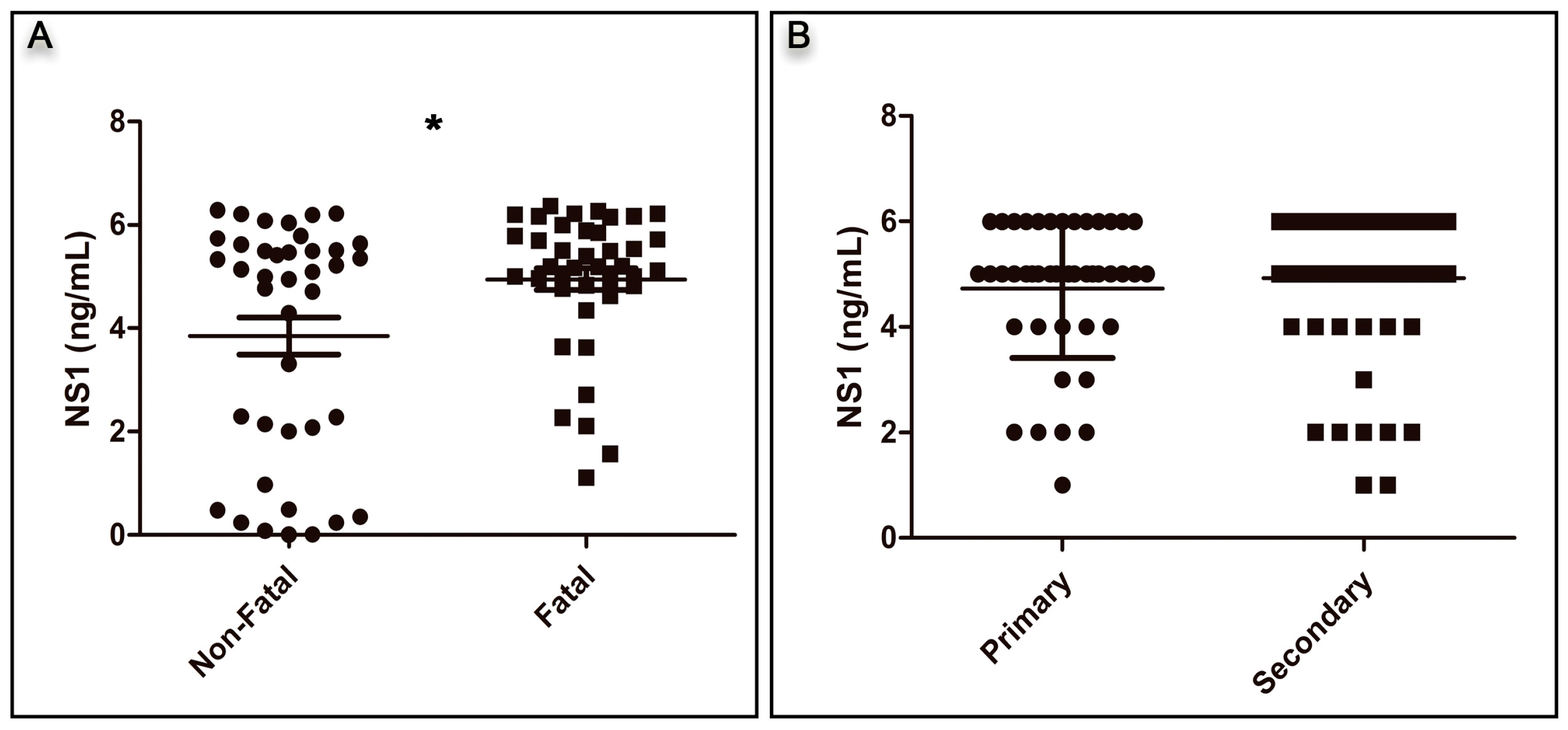
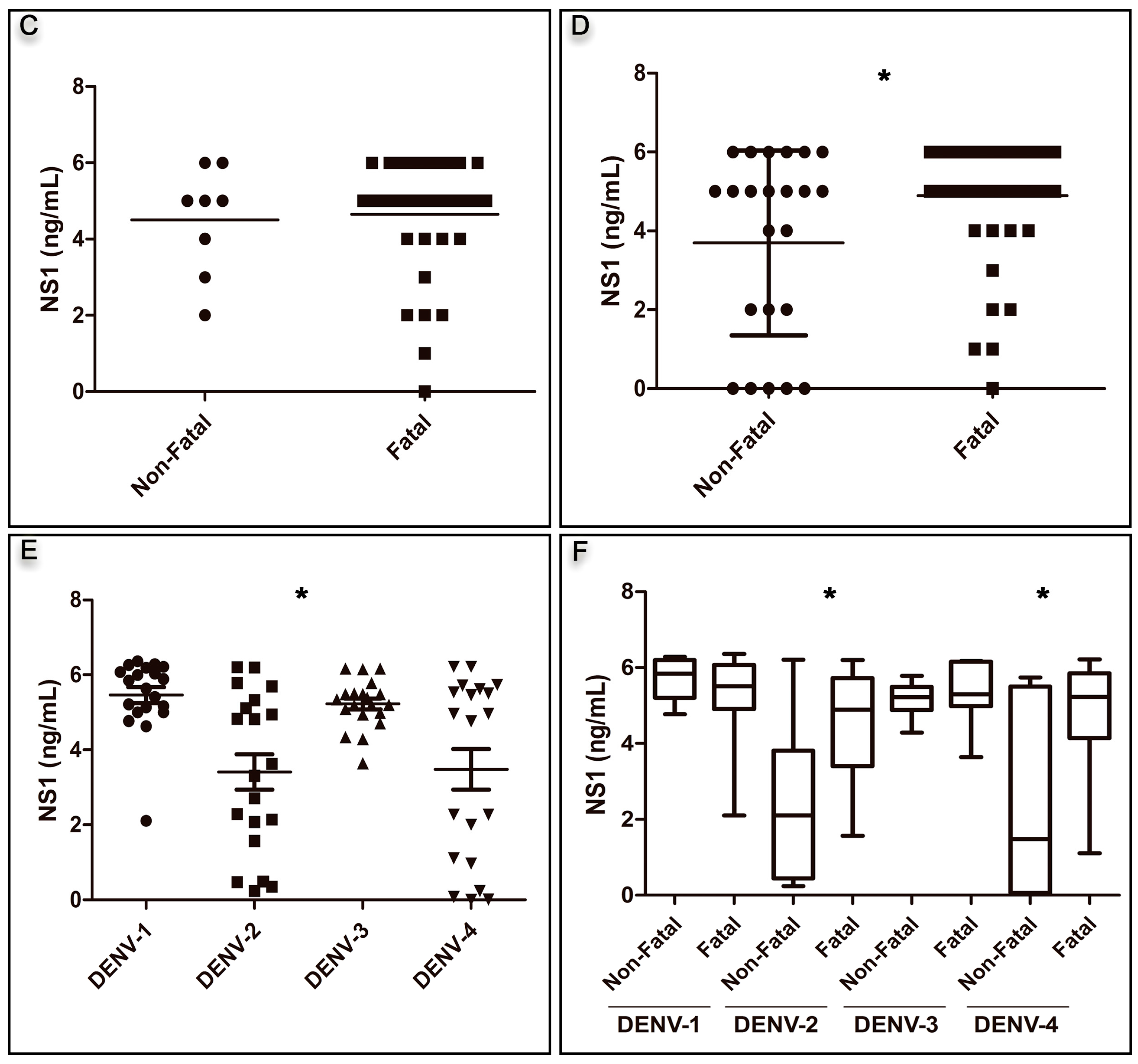
3.1. Analysis of NS1 Antigenemia
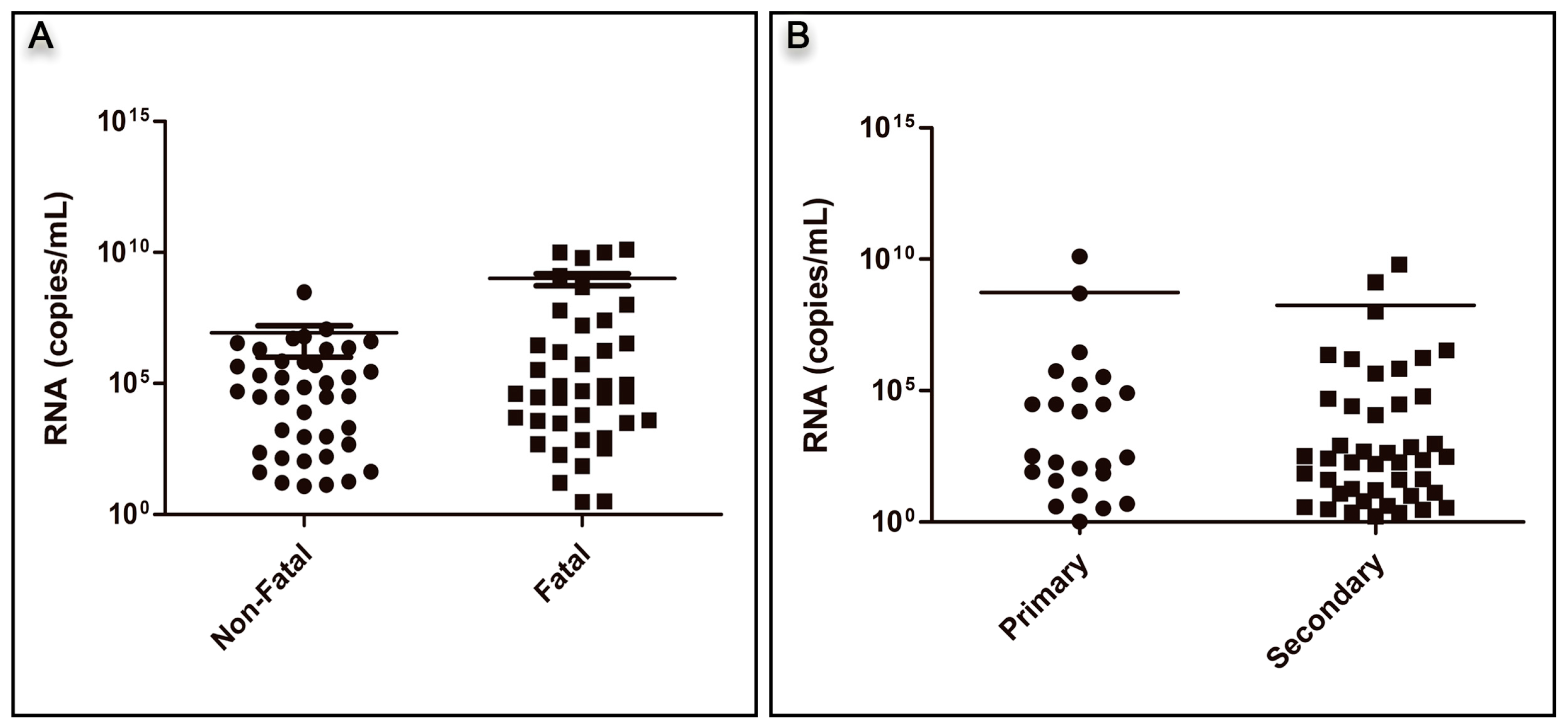
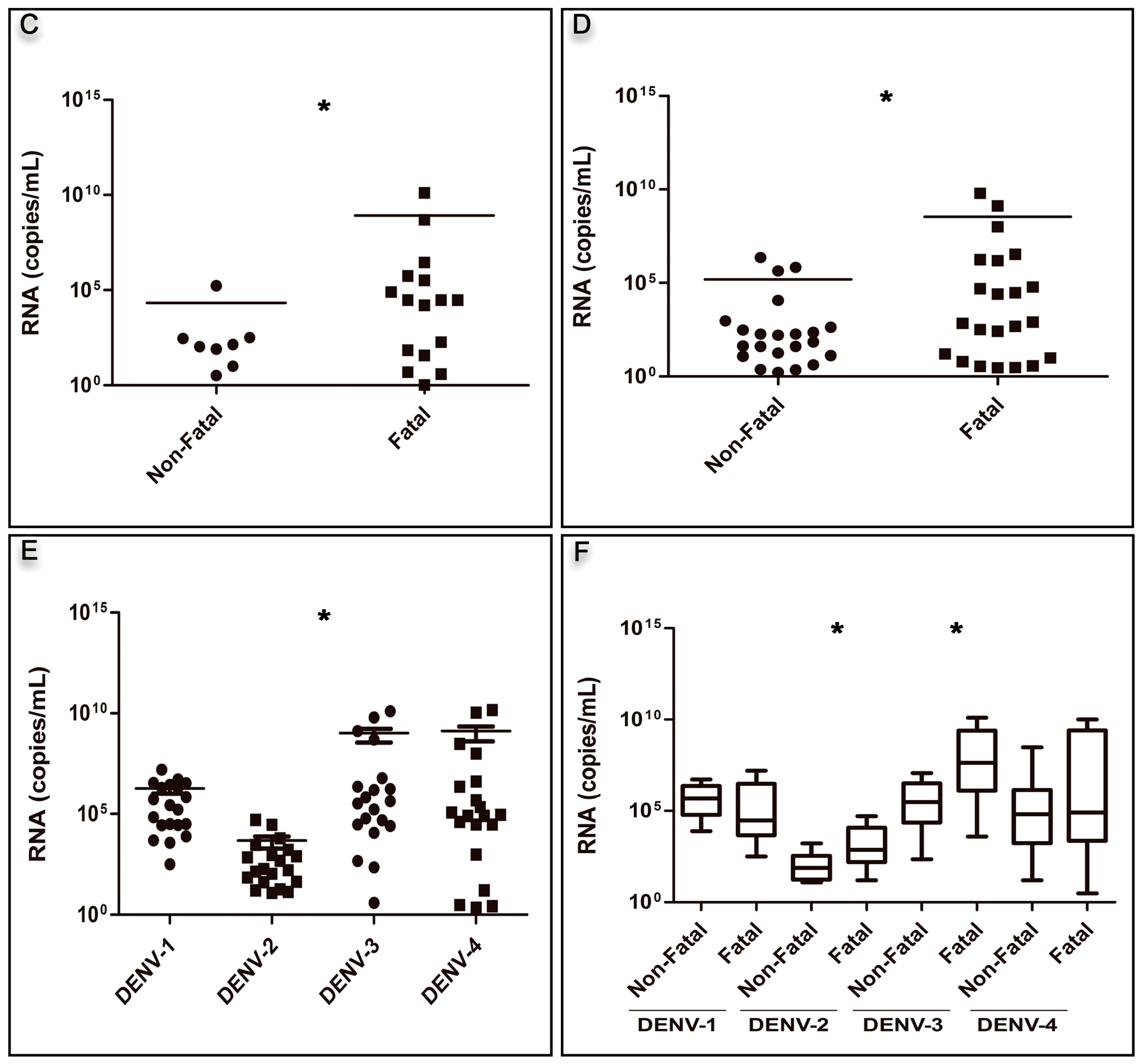
3.2. Analysis of Viral RNA Quantification
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization (WHO). Dengue and Severe Dengue: Fact Sheet No 117; World Health Organization (WHO): Geneva, Switzerland, 2016. [Google Scholar]
- Basu, A.; Chaturvedi, U.C. Vascular endothelium: The battlefield of dengue viruses. FEMS Immunol. Med. Microbiol. 2008, 53, 287–299. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Dengue Guidelines for Diagnosis, Treatment, Prevention and Control; World Health Organization (WHO): Geneva, Switzerland, 2009. [Google Scholar]
- Rigau-Pérez, J.G.; Ayala-López, A.; García-Rivera, E.J.; Hudson, S.M.; Vorndam, V.; Reiter, P.; Cano, M.P.; Clark, G.G. The reappearance of dengue-3 and a subsequent dengue-4 and dengue-1 epidemic in Puerto Rico in 1998. Am. J. Trop. Med. Hyg. 2002, 67, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Sam, S.-S.; Omar, S.F.S.; Teoh, B.-T.; Abd-Jamil, J.; AbuBakar, S. Review of Dengue hemorrhagic fever fatal cases seen among adults: A retrospective study. PLoS Negl. Trop. Dis. 2013, 7, e2194. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization (PAHO). Reported Cases of Dengue Fever in the Americas, by Country or Territory 1995–2017 (until October 2017); Pan American Health Organization (PAHO): Washington, DC, USA, 2017. [Google Scholar]
- Dos Santos, F.B.; Filippis, A.; Araújo, E.; Lima, M.; de Bruycker-Nogueira, F.; Faria, N.R.C.; Sampaio, S.; Nunes, P.C.G.; Heringer, M.; Lima, D.; et al. A Review on Dengue Diagnosis and Epidemiology by a Regional Reference Laboratory in 25 years, Rio de Janeiro, Brazil. Dengue Bull. 2013, 37, 61–76. [Google Scholar]
- Schatxmayr, H.G.; Nogueira, R.M.R.; Travassos da Rosa, A.P.A. An outbreak of dengue virus at Rio de Janeiro—1986. Memorias Do Institute Oswaldo Cruz 1986, 81, 245–246. [Google Scholar] [CrossRef]
- Pinheiro, F.P.; Corber, S.J. Global situation of dengue and dengue haemorrhagic fever, and its emergence in the Americas. World Health Stat. Q. Rapp. Trimest. Stat. Sanit. Mond. 1997, 50, 161–169. [Google Scholar]
- SES/SINAN Óbitos Por Dengue. Brasil, Grandes Regiões e Unidades Federadas, 1990 a 2016. Available online: http://portalarquivos.saude.gov.br/images/pdf/2017/fevereiro/10/obitos-ate-2016.pdf (accessed on 14 April 2017).
- SES/SINAN Casos Graves Confirmados, Segundo ano de Confirmação, Brasil, Grandes Regiões e Unidades Federadas, 1990 a 2016. Available online: http://portalarquivos.saude.gov.br/images/pdf/2017/fevereiro/10/Graves-ate-2016.pdf (accessed on 14 April 2017).
- Gubler, D.J. Dengue and dengue hemorrhagic fever. Clin. Microbiol. Rev. 1998, 11, 480–496. [Google Scholar] [PubMed]
- Villabona-Arenas, C.J.; de Oliveira, J.L.; de Capra, C.S.; Balarini, K.; Loureiro, M.; Fonseca, C.R.T.P.; Passos, S.D.; de Zanotto, P.M.A. Detection of Four Dengue Serotypes Suggests Rise in Hyperendemicity in Urban Centers of Brazil. PLoS Negl. Trop. Dis. 2014, 8, e2620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaturro, P.; Cortese, M.; Chatel-Chaix, L.; Fischl, W.; Bartenschlager, R. Dengue Virus Non-structural Protein 1 Modulates Infectious Particle Production via Interaction with the Structural Proteins. PLoS Pathog. 2015, 11, e1005277. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Di, B.; Pan, Y.; Qiu, L.; Wang, Y.; Hao, W.; He, L.; Yuen, K.; Che, X. Serotype 1-specific monoclonal antibody-based antigen capture immunoassay for detection of circulating nonstructural protein NS1: Implications for early diagnosis and serotyping of dengue virus infections. J. Clin. Microbiol. 2006, 44, 2872–2878. [Google Scholar] [CrossRef] [PubMed]
- Duong, V.; Ly, S.; Lorn Try, P.; Tuiskunen, A.; Ong, S.; Chroeung, N.; Lundkvist, A.; Leparc-Goffart, I.; Deubel, V.; Vong, S.; et al. Clinical and virological factors influencing the performance of a NS1 antigen-capture assay and potential use as a marker of dengue disease severity. PLoS Negl. Trop. Dis. 2011, 5, e1244. [Google Scholar] [CrossRef] [PubMed]
- Moi, M.L.; Omatsu, T.; Tajima, S.; Lim, C.-K.; Kotaki, A.; Ikeda, M.; Harada, F.; Ito, M.; Saijo, M.; Kurane, I.; et al. Detection of dengue virus nonstructural protein 1 (NS1) by using ELISA as a useful laboratory diagnostic method for dengue virus infection of international travelers. J. Travel Med. 2013, 20, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Libraty, D.H.; Endy, T.P.; Houng, H.-S.H.; Green, S.; Kalayanarooj, S.; Suntayakorn, S.; Chansiriwongs, W.; Vaughn, D.W.; Nisalak, A.; Ennis, F.A.; et al. Differing influences of virus burden and immune activation on disease severity in secondary dengue-3 virus infections. J. Infect. Dis. 2002, 185, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- Nunes, P.C.G.; Sampaio, S.A.F.; da Costa, N.R.; de Mendonça, M.C.L.; da Lima, M.R.Q.; Araujo, S.E.M.; dos Santos, F.B.; Simões, J.B.S.; de Gonçalves, B.S.; Nogueira, R.M.R.; et al. Dengue severity associated with age and a new lineage of dengue virus-type 2 during an outbreak in Rio De Janeiro, Brazil. J. Med. Virol. 2016, 88, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Tricou, V.; Minh, N.N.; Farrar, J.; Tran, H.T.; Simmons, C.P. Kinetics of viremia and NS1 antigenemia are shaped by immune status and virus serotype in adults with dengue. PLoS Negl. Trop. Dis. 2011, 5, e1309. [Google Scholar] [CrossRef] [PubMed]
- De Araújo, J.M.G.; Bello, G.; Schatzmayr, H.G.; dos Santos, F.B.; Nogueira, R.M.R. Dengue virus type 3 in Brazil: A phylogenetic perspective. Memorias Do Instituto Oswaldo Cruz 2009, 104, 526–529. [Google Scholar] [CrossRef]
- Allonso, D.; Meneses, M.D.F.; Fernandes, C.A.; Ferreira, D.F.; Mohana-Borges, R. Assessing positivity and circulating levels of NS1 in samples from a 2012 dengue outbreak in Rio de Janeiro, Brazil. PLoS ONE 2014, 9, e113634. [Google Scholar] [CrossRef] [PubMed]
- Avirutnan, P.; Punyadee, N.; Noisakran, S.; Komoltri, C.; Thiemmeca, S.; Auethavornanan, K.; Jairungsri, A.; Kanlaya, R.; Tangthawornchaikul, N.; Puttikhunt, C.; et al. Vascular leakage in severe dengue virus infections: A potential role for the nonstructural viral protein NS1 and complement. J. Infect. Dis. 2006, 193, 1078–1088. [Google Scholar] [CrossRef] [PubMed]
- Beatty, P.R.; Puerta-Guardo, H.; Killingbeck, S.S.; Glasner, D.R.; Hopkins, K.; Harris, E. Dengue virus NS1 triggers endothelial permeability and vascular leak that is prevented by NS1 vaccination. Sci. Transl. Med. 2015, 7, 304ra141. [Google Scholar] [CrossRef] [PubMed]
- Puerta-Guardo, H.; Glasner, D.R.; Harris, E. Dengue Virus NS1 Disrupts the Endothelial Glycocalyx, Leading to Hyperpermeability. PLoS Pathog. 2016, 12, e1005738. [Google Scholar] [CrossRef] [PubMed]
- Glasner, D.R.; Ratnasiri, K.; Puerta-Guardo, H.; Espinosa, D.A.; Beatty, P.R.; Harris, E. Dengue virus NS1 cytokine-independent vascular leak is dependent on endothelial glycocalyx components. PLoS Pathog. 2017, 13, e1006673. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, A. Isolation of a Singh’s Aedes albopictus cell clone sensitive to Dengue and Chikungunya viruses. J. Gen. Virol. 1978, 40, 531–544. [Google Scholar] [CrossRef] [PubMed]
- Gubler, D.J.; Kuno, G.; Sather, G.E.; Velez, M.; Oliver, A. Mosquito cell cultures and specific monoclonal antibodies in surveillance for dengue viruses. Am. J. Trop. Med. Hyg. 1984, 33, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, R.M.; Miagostovich, M.P.; Lampe, E.; Souza, R.W.; Zagne, S.M.; Schatzmayr, H.G. Dengue epidemic in the stage of Rio de Janeiro, Brazil, 1990-1: Co-circulation of dengue 1 and dengue 2 serotypes. Epidemiol. Infect. 1993, 111, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Miagostovich, M.P.; Nogueira, R.M.; dos Santos, F.B.; Schatzmayr, H.G.; Araújo, E.S.; Vorndam, V. Evaluation of an IgG enzyme-linked immunosorbent assay for dengue diagnosis. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 1999, 14, 183–189. [Google Scholar] [CrossRef]
- Lanciotti, R.S.; Calisher, C.H.; Gubler, D.J.; Chang, G.J.; Vorndam, A.V. Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase-polymerase chain reaction. J. Clin. Microbiol. 1992, 30, 545–551. [Google Scholar] [PubMed]
- Heringer, M.; Souza, T.M.A.; da Lima, M.R.Q.; Nunes, P.C.G.; da Faria, N.R.C.; de Bruycker-Nogueira, F.; Chouin-Carneiro, T.; Nogueira, R.M.R.; Dos Santos, F.B. Dengue type 4 in Rio de Janeiro, Brazil: Case characterization following its introduction in an endemic region. BMC Infect. Dis. 2017, 17, 410. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.W.; Russell, B.J.; Lanciotti, R.S. Serotype-specific detection of dengue viruses in a fourplex real-time reverse transcriptase PCR assay. J. Clin. Microbiol. 2005, 43, 4977–4983. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J. NS1: A corner piece in the dengue pathogenesis puzzle? Sci. Transl. Med. 2015, 7, 304fs37. [Google Scholar] [CrossRef] [PubMed]
- De La Cruz Hernández, S.I.; Flores-Aguilar, H.; González-Mateos, S.; López-Martínez, I.; Ortiz-Navarrete, V.; Ludert, J.E.; Del Angel, R.M. Viral load in patients infected with dengue is modulated by the presence of anti-dengue IgM antibodies. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2013, 58, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Paranavitane, S.A.; Gomes, L.; Kamaladasa, A.; Adikari, T.N.; Wickramasinghe, N.; Jeewandara, C.; Shyamali, N.L.A.; Ogg, G.S.; Malavige, G.N. Dengue NS1 antigen as a marker of severe clinical disease. BMC Infect. Dis. 2014, 14, 570. [Google Scholar] [CrossRef] [PubMed]
- Modhiran, N.; Watterson, D.; Muller, D.A.; Panetta, A.K.; Sester, D.P.; Liu, L.; Hume, D.A.; Stacey, K.J.; Young, P.R. Dengue virus NS1 protein activates cells via Toll-like receptor 4 and disrupts endothelial cell monolayer integrity. Sci. Transl. Med. 2015, 7, 304ra142. [Google Scholar] [CrossRef] [PubMed]
- Adikari, T.N.; Gomes, L.; Wickramasinghe, N.; Salimi, M.; Wijesiriwardana, N.; Kamaladasa, A.; Shyamali, N.L.A.; Ogg, G.S.; Malavige, G.N. Dengue NS1 antigen contributes to disease severity by inducing interleukin (IL)-10 by monocytes. Clin. Exp. Immunol. 2016, 184, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Malavige, G.N.; Ogg, G.S. Pathogenesis of vascular leak in dengue virus infection. Immunology 2017, 151, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erra, E.O.; Korhonen, E.M.; Voutilainen, L.; Huhtamo, E.; Vapalahti, O.; Kantele, A. Dengue in travelers: Kinetics of viremia and NS1 antigenemia and their associations with clinical parameters. PLoS ONE 2013, 8, e65900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perdomo-Celis, F.; Salgado, D.M.; Narváez, C.F. Magnitude of viremia, antigenemia and infection of circulating monocytes in children with mild and severe dengue. Acta Trop. 2017, 167, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bich Chau, T.N.; Anders, K.L.; Lien, L.B.; Hung, N.T.; Minh Hieu, L.T.; Tuan, N.M.; Thuy, T.T.; Phuong, L.T.; Hong Tham, N.T.; Lanh, M.N.; et al. Clinical and Virological Features of Dengue in Vietnamese Infants. PLoS Negl. Trop. Dis. 2010, 4. [Google Scholar] [CrossRef] [PubMed]
- Duyen, H.T.L.; Ngoc, T.V.; Ha, D.T.; Hang, V.T.T.; Kieu, N.T.T.; Young, P.R.; Farrar, J.J.; Simmons, C.P.; Wolbers, M.; Wills, B.A. Kinetics of Plasma Viremia and Soluble Nonstructural Protein 1 Concentrations in Dengue: Differential Effects According to Serotype and Immune Status. J. Infect. Dis. 2011, 203, 1292–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, A.; Hoa, L.N.M.; Simmons, C.P.; Wolbers, M.; Wertheim, H.F.L.; Khuong, P.T.; Ninh, T.T.H.; Lien, T.T.M.; Lien, N.T.; Trung, N.V.; et al. Immunological and Viral Determinants of Dengue Severity in Hospitalized Adults in Ha Noi, Viet Nam. PLoS Negl. Trop. Dis. 2011, 5. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, D.W.; Green, S.; Kalayanarooj, S.; Innis, B.L.; Nimmannitya, S.; Suntayakorn, S.; Endy, T.P.; Raengsakulrach, B.; Rothman, A.L.; Ennis, F.A.; et al. Dengue viremia titer, antibody response pattern, and virus serotype correlate with disease severity. J. Infect. Dis. 2000, 181, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Murgue, B.; Roche, C.; Chungue, E.; Deparis, X. Prospective study of the duration and magnitude of viraemia in children hospitalised during the 1996–1997 dengue-2 outbreak in French Polynesia. J. Med. Virol. 2000, 60, 432–438. [Google Scholar] [CrossRef]
- Wang, W.-K.; Chao, D.-Y.; Kao, C.-L.; Wu, H.-C.; Liu, Y.-C.; Li, C.-M.; Lin, S.-C.; Ho, S.-T.; Huang, J.-H.; King, C.-C. High levels of plasma dengue viral load during defervescence in patients with dengue hemorrhagic fever: Implications for pathogenesis. Virology 2003, 305, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.-F.; Liu, J.-W.; Yeh, W.-T.; Wang, L.; Chang, J.-C.; Yu, H.-R.; Cheng, J.-T.; Yang, K.D. Altered T helper 1 reaction but not increase of virus load in patients with dengue hemorrhagic fever. FEMS Immunol. Med. Microbiol. 2005, 44, 43–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singla, M.; Kar, M.; Sethi, T.; Kabra, S.K.; Lodha, R.; Chandele, A.; Medigeshi, G.R. Correction: Immune Response to Dengue Virus Infection in Pediatric Patients in New Delhi, India-Association of Viremia, Inflammatory Mediators and Monocytes with Disease Severity. PLoS Negl. Trop. Dis. 2016, 10, e0004642. [Google Scholar] [CrossRef] [PubMed]
- Sudiro, T.M.; Zivny, J.; Ishiko, H.; Green, S.; Vaughn, D.W.; Kalayanarooj, S.; Nisalak, A.; Norman, J.E.; Ennis, F.A.; Rothman, A.L. Analysis of plasma viral RNA levels during acute dengue virus infection using quantitative competitor reverse transcription-polymerase chain reaction. J. Med. Virol. 2001, 63, 29–34. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DENV Serotype | n | NS1 Antigenemia (Mean, ng/mL) | p | RNA Quantification (Mean, Copies RNA/mL) | p |
|---|---|---|---|---|---|
| Dengue 1 | 20 | 5.46 | <0.001 | 1.83 × 106 | =0.001 |
| Dengue 2 | 20 | 3.41 | 4.73 × 103 | ||
| Dengue 3 | 20 | 5.23 | 1.03 × 109 | ||
| Dengue 4 | 20 | 3.48 | 1.30 × 109 |
| Serotype | Disease Outcome | n | NS1 Antigenemia (mean, ng/mL) | p | RNA Quantification (mean, RNA Copies/mL) | p |
|---|---|---|---|---|---|---|
| Dengue 1 | Non-Fatal | 10 | 5.69 | =0.285 | 1.38 × 106 | =0.266 |
| Fatal | 10 | 5.27 | 2.29 × 106 | |||
| Dengue 2 | Non-Fatal | 10 | 2.92 | =0.013 | 3.13 × 101 | =0.018 |
| Fatal | 10 | 4.53 | 9.15 × 103 | |||
| Dengue 3 | Non-Fatal | 10 | 5.16 | =0.663 | 2.15 × 106 | =0.011 |
| Fatal | 10 | 5.29 | 2.06 × 109 | |||
| Dengue 4 | Non-Fatal | 10 | 2.24 | =0.016 | 3.04 × 107 | =0.731 |
| Fatal | 10 | 4.73 | 2.01 × 109 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nunes, P.C.G.; Nogueira, R.M.R.; Heringer, M.; Chouin-Carneiro, T.; Damasceno dos Santos Rodrigues, C.; De Filippis, A.M.B.; Lima, M.D.R.Q.; Dos Santos, F.B. NS1 Antigenemia and Viraemia Load: Potential Markers of Progression to Dengue Fatal Outcome? Viruses 2018, 10, 326. https://doi.org/10.3390/v10060326
Nunes PCG, Nogueira RMR, Heringer M, Chouin-Carneiro T, Damasceno dos Santos Rodrigues C, De Filippis AMB, Lima MDRQ, Dos Santos FB. NS1 Antigenemia and Viraemia Load: Potential Markers of Progression to Dengue Fatal Outcome? Viruses. 2018; 10(6):326. https://doi.org/10.3390/v10060326
Chicago/Turabian StyleNunes, Priscila Conrado Guerra, Rita Maria Ribeiro Nogueira, Manoela Heringer, Thaís Chouin-Carneiro, Cintia Damasceno dos Santos Rodrigues, Ana Maria Bispo De Filippis, Monique Da Rocha Queiroz Lima, and Flávia Barreto Dos Santos. 2018. "NS1 Antigenemia and Viraemia Load: Potential Markers of Progression to Dengue Fatal Outcome?" Viruses 10, no. 6: 326. https://doi.org/10.3390/v10060326
APA StyleNunes, P. C. G., Nogueira, R. M. R., Heringer, M., Chouin-Carneiro, T., Damasceno dos Santos Rodrigues, C., De Filippis, A. M. B., Lima, M. D. R. Q., & Dos Santos, F. B. (2018). NS1 Antigenemia and Viraemia Load: Potential Markers of Progression to Dengue Fatal Outcome? Viruses, 10(6), 326. https://doi.org/10.3390/v10060326