Rift Valley Fever Virus Exposure amongst Farmers, Farm Workers, and Veterinary Professionals in Central South Africa


 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Design and Data Collection
2.3. Sample Collection and Laboratory Procedures
2.4. Statistical Analyses
3. Results
3.1. Study Population
3.2. Seroprevalence and Factors Associated with Human Exposure
3.3. Estimation of RVF Cases in Farm Population
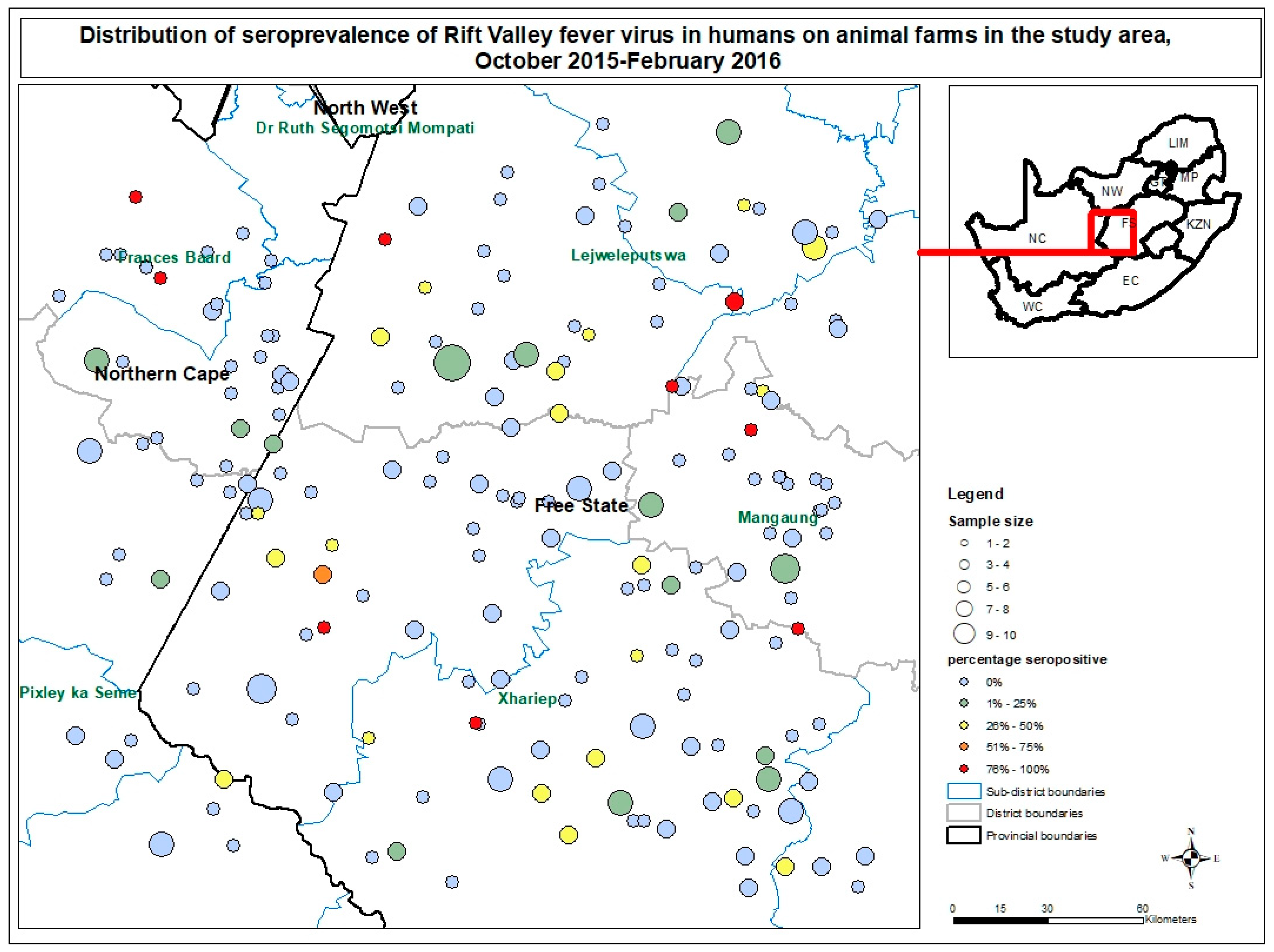
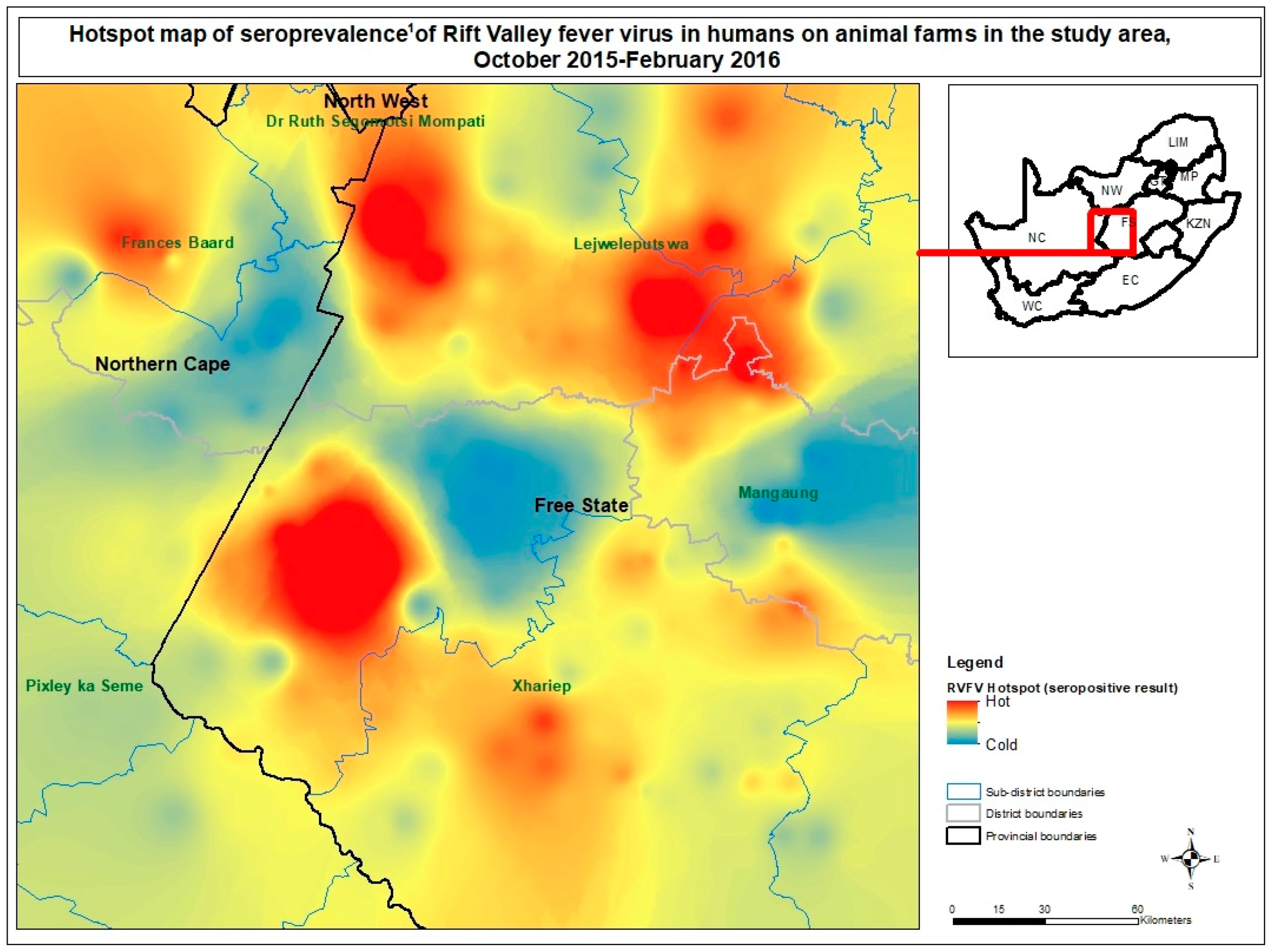
3.4. Spatial Distribution of RVFV Farm Seroprevalence
4. Discussion
4.1. Seroprevalence
4.2. Risk Factors
4.3. Case Estimates
4.4. Spatial Analysis
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Linthicum, K.J.; Britch, S.C.; Anyamba, A. Rift Valley Fever: An Emerging Mosquito-Borne Disease. Annu. Rev. Entomol. 2016, 61, 395–415. [Google Scholar] [CrossRef] [PubMed]
- Erasmus, B.J.; Coetzer, J. Symptomatology and pathology of Rift Valley fever in domestic animals. Proc. Rift Val. Fever Workshop 1981. [Google Scholar]
- Lefkowitz, E.J.; Dempsey, D.M.; Hendrickson, R.C.; Orton, R.J.; Siddell, S.G.; Smith, D.B. Virus taxonomy: The database of the International Committee on Taxonomy of Viruses (ICTV). Nucleic Acids Res. 2018, 46, D708–D717. [Google Scholar] [CrossRef] [PubMed]
- Blumberg, L.; Enria, D.; Bausch, D.G. 16–Viral Haemorrhagic Fevers. In Manson’s Tropical Infectious Diseases, 23rd ed.; Farrar, J., Hotez, P.J., Junghanss, T., Kang, G., Lalloo, D., White, N.J., Eds.; W.B. Saunders: London, UK, 2014; pp. 171–194.e2. ISBN 978-0-7020-5101-2. [Google Scholar]
- Al-Hazmi, M.; Ayoola, E.A.; Abdurahman, M.; Banzal, S.; Ashraf, J.; El-Bushra, A.; Hazmi, A.; Abdullah, M.; Abbo, H.; Elamin, A.; et al. Epidemic Rift Valley fever in Saudi Arabia: A clinical study of severe illness in humans. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2003, 36, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Deutman, A.F.; Klomp, H.J. Rift Valley Fever Retinitis. Am. J. Ophthalmol. 1981, 92, 38–42. [Google Scholar] [CrossRef]
- WHO | Rift Valley fever. Available online: http://www.who.int/emergencies/diseases/rift-valley-fever/en/ (accessed on 25 June 2018).
- Rift Valley Fever Fact Sheet. Available online: https://www.cdc.gov/vhf/rvf/RVF-FactSheet.pdf (accessed on 25 June 2018).
- Archer, B.N.; Weyer, J.; Paweska, J.; Nkosi, D.; Leman, P.; Tint, K.S.; Blumberg, L. Outbreak of Rift Valley fever affecting veterinarians and farmers in South Africa, 2008. S. Afr. Med. J. 2011, 101, 263–266. [Google Scholar] [CrossRef]
- Rostal, M.K.; Liang, J.E.; Zimmermann, D.; Bengis, R.; Paweska, J.; Karesh, W.B. Rift Valley Fever: Does Wildlife Play a Role? ILAR J. 2017, 58, 359–370. [Google Scholar] [CrossRef]
- Hassan, O.A.; Ahlm, C.; Sang, R.; Evander, M. The 2007 Rift Valley Fever Outbreak in Sudan. PLoS Negl. Trop. Dis. 2011, 5, e1229. [Google Scholar] [CrossRef]
- Smithburn, K.C.; Mahaffy, A.F. Rift Valley fever; accidental infections among laboratory workers. J. Immunol. 1949, 62, 213–227. [Google Scholar]
- Stern, L. Rift Valley Fever in Rhodesia Report of a Case in a Laboratory Worker. Cent. J. Afr. Med. 1956, 1, 281–283. [Google Scholar]
- Gear, J.; De Meillon, B.; Measroch, V.; Davis, D.; Harwin, H. Rift valley fever in South Africa. 2. The occurrence of human cases in the Orange Free State, the North-Western Cape Province, the Western and Southern Transvaal. B. Field and laboratory investigation. Afr. Med. J. 1951, 8, 908–912. [Google Scholar]
- Mundel, G.; Gear, J. Rift Valley fever. I. The occurrence of human cases in Johannesburg. Afr. Med. J. 1951, 25, 797–800. [Google Scholar]
- McIntosh, B.M.; Russell, D.; Dos Santos, I.; Gear, J.H. Rift Valley fever in humans in South Africa. Afr. Med. J. 1980, 15, 803–806. [Google Scholar]
- Archer, B.N.; Thomas, J.; Weyer, J.; Cengimbo, A.; Landoh, D.E.; Jacobs, C.; Ntuli, S.; Modise, M.; Mathonsi, M.; Mashishi, M.S.; et al. Epidemiologic Investigations into Outbreaks of Rift Valley Fever in Humans, South Africa, 2008–2011. Emerg. Infect. Dis. 2013, 19. [Google Scholar] [CrossRef] [PubMed]
- Jansen van Vuren, P.; Kgaladi, J.; Patharoo, V.; Ohaebosim, P.; Msimang, V.; Nyokong, B.; Paweska, J.T. Human Cases of Rift Valley Fever in South Africa, 2018. Vector-Borne Zoonotic Dis. 2018, 18, 713–715. [Google Scholar] [CrossRef] [PubMed]
- OIE Rift Valley Fever South Africa. RVF_2018_001, Letsemeng, Free State. Available online: https://www.oie.int/wahis_2/public/wahid.php/Reviewreport/Review?page_refer = MapFullEventReport&reportid=26639 (accessed on 26 June 2018).
- Pienaar, N.J.; Thompson, P.N. Temporal and spatial history of Rift Valley fever in South Africa: 1950 to 2011. Onderstepoort J. Vet. Res. 2013, 80, 13. [Google Scholar] [CrossRef] [PubMed]
- Parry, K.; Statistics South Africa, Sandringham, South Africa. Personal communication, 2014.
- Hartung, C.; Lerer, A.; Anokwa, Y.; Tseng, C.; Brunette, W.; Borriello, G. Open Data Kit: Tools to Build Information Services for Developing Regions. In Proceedings of the 4th ACM/IEEE International Conference on Information and Communication Technologies and Development, London, UK, 13–16 December 2010; ACM: New York, NY, USA, 2010; pp. 18:1–18:12. [Google Scholar]
- Paweska, J.T.; Jansen van Vuren, P.; Swanepoel, R. Validation of an indirect ELISA based on a recombinant nucleocapsid protein of Rift Valley fever virus for the detection of IgG antibody in humans. J. Virol. Methods 2007, 146, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Paweska, J.T.; Mortimer, E.; Leman, P.A.; Swanepoel, R. An inhibition enzyme-linked immunosorbent assay for the detection of antibody to Rift Valley fever virus in humans, domestic and wild ruminants. J. Virol. Methods 2005, 127, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Wolter, K. Introduction to Variance Estimation; Statistics for Social and Behavioral Sciences; Springer: New York, NY, USA, 2007; ISBN 978-0-387-32917-8. [Google Scholar]
- Rogan, W.; Gladen, B. Estimating Prevalence From Results of A Screening-test. Am. J. Epidemiol. 1978, 107, 71–76. [Google Scholar] [CrossRef]
- Blaker, H. Confidence curves and improved exact confidence intervals for discrete distributions. Can. J. Stat. 2000, 28, 783–798. [Google Scholar] [CrossRef]
- Moran, P.A.P. Notes on Continuous Stochastic Phenomena. Biometrika 1950, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Ord, J.K.; Getis, A. Local Spatial Autocorrelation Statistics: Distributional Issues and an Application. Geogr. Anal. 1995, 27, 286–306. [Google Scholar] [CrossRef]
- Mapaco, L.P.; Coetzer, J.A.W.; Paweska, J.T.; Venter, E.H. An investigation into an outbreak of Rift Valley fever on a cattle farm in Bela-Bela, South Africa, in 2008. J. S. Afr. Vet. Assoc. 2012, 83, 132. [Google Scholar] [CrossRef] [PubMed]
- Smithburn, K.C.; Kokernot, R.H.; Heymann, C.S.; Weinbren, M.P.; Zentkowsky, D. Neutralizing antibodies for certain viruses in the sera of human beings residing in Northern Natal. S. Afr. Med. J. 1959, 33, 555–561. [Google Scholar]
- Msimang, V.; Weyer, J.; Kemp, A.; Jansen van Vuren, P.; le Roux, C.; Frean, J.; Paweska, J.T. Arboviral and bacterial zoonoses amongst human population in the Kruger national game park, 2013–2014. In Proceedings of the Virology Africa 2015, Cape Town, South Africa, 19–20 April 2015. [Google Scholar]
- Simpson, G.J.G.; Quan, V.; Frean, J.; Knobel, D.L.; Rossouw, J.; Weyer, J.; Marcotty, T.; Godfroid, J.; Blumberg, L.H. Prevalence of Selected Zoonotic Diseases and Risk Factors at a Human-Wildlife-Livestock Interface in Mpumalanga Province, South Africa. Vector Borne Zoonotic Dis. Larchmt. N 2018, 18, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Beechler, B.R.; Bengis, R.; Swanepoel, R.; Paweska, J.T.; Kemp, A.; van Vuren, P.J.; Joubert, J.; Ezenwa, V.O.; Jolles, A.E. Rift valley Fever in Kruger national park: Do buffalo play a role in the inter-epidemic circulation of virus? Transbound. Emerg. Dis. 2015, 62, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Sindato, C.; Karimuribo, E.D.; Pfeiffer, D.U.; Mboera, L.E.G.; Kivaria, F.; Dautu, G.; Bernard, B.; Paweska, J.T. Spatial and Temporal Pattern of Rift Valley Fever Outbreaks in Tanzania; 1930 to 2007. PLoS ONE 2014, 9, e88897. [Google Scholar] [CrossRef] [PubMed]
- Pourrut, X.; Nkoghé, D.; Souris, M.; Paupy, C.; Paweska, J.; Padilla, C.; Moussavou, G.; Leroy, E.M. Rift Valley Fever Virus Seroprevalence in Human Rural Populations of Gabon. PLoS Negl. Trop. Dis. 2010, 4, e763. [Google Scholar] [CrossRef]
- LaBeaud, A.D.; Muiruri, S.; Sutherland, L.J.; Dahir, S.; Gildengorin, G.; Morrill, J.; Muchiri, E.M.; Peters, C.J.; King, C.H. Postepidemic Analysis of Rift Valley Fever Virus Transmission in Northeastern Kenya: A Village Cohort Study. PLoS Negl. Trop. Dis. 2011, 5, e1265. [Google Scholar] [CrossRef]
- Lernout, T.; Cardinale, E.; Jego, M.; Desprès, P.; Collet, L.; Zumbo, B.; Tillard, E.; Girard, S.; Filleul, L. Rift Valley Fever in Humans and Animals in Mayotte, an Endemic Situation? PLoS ONE 2013, 8, e74192. [Google Scholar] [CrossRef]
- Nicholas, D.E.; Jacobsen, K.H.; Waters, N.M. Risk factors associated with human Rift Valley fever infection: Systematic review and meta-analysis. Trop. Med. Int. Health 2014, 19, 1420–1429. [Google Scholar] [CrossRef] [PubMed]
- Velebit, B.; Radin, D.; Teodorovic, V. Transmission of Common Foodborne Viruses by Meat Products. Procedia Food Sci. 2015, 5, 304–307. [Google Scholar] [CrossRef]
- Meegan, J.M. The Rift Valley fever epizootic in Egypt 1977–78. 1. Description of the epizootic and virological studies. Trans. R. Soc. Trop. Med. Hyg. 1979, 73, 618–623. [Google Scholar] [CrossRef]
- Woods, C.W.; Karpati, A.M.; Grein, T.; McCarthy, N.; Gaturuku, P.; Muchiri, E.; Dunster, L.; Henderson, A.; Khan, A.S.; Swanepoel, R.; et al. An Outbreak of Rift Valley Fever in Northeastern Kenya, 1997–98. Emerg. Infect. Dis. 2002, 8, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, M.; Mosha, F.; Mghamba, J.; Zaki, S.R.; Shieh, W.-J.; Paweska, J.; Omulo, S.; Gikundi, S.; Mmbuji, P.; Bloland, P.; et al. Epidemiologic and clinical aspects of a Rift Valley fever outbreak in humans in Tanzania, 2007. Am. J. Trop. Med. Hyg. 2010, 83, 22–27. [Google Scholar] [CrossRef] [PubMed]
- LaBeaud, A.D.; Muchiri, E.M.; Ndzovu, M.; Mwanje, M.T.; Muiruri, S.; Peters, C.J.; King, C.H. Interepidemic Rift Valley Fever Virus Seropositivity, Northeastern Kenya. Emerg. Infect. Dis. 2008, 14, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- LaBeaud, A.D.; Ochiai, Y.; Peters, C.J.; Muchiri, E.M.; King, C.H. Spectrum of Rift Valley Fever Virus Transmission in Kenya: Insights from three Distinct Regions. Am. J. Trop. Med. Hyg. 2007, 76, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Daubney, R.; Hudson, J.R.; Garnham, P.C. Enzootic hepatitis or rift valley fever. An undescribed virus disease of sheep cattle and man from east africa. J. Pathol. Bacteriol. 1931, 34, 545–579. [Google Scholar] [CrossRef]
- Davies, F.G. The Historical and Recent Impact of Rift Valley Fever in Africa. Am. J. Trop. Med. Hyg. 2010, 83, 73–74. [Google Scholar] [CrossRef] [PubMed]
- Baba, M.; Masiga, D.K.; Sang, R.; Villinger, J. Has Rift Valley fever virus evolved with increasing severity in human populations in East Africa? Emerg. Microbes Infect. 2016, 5, e58. [Google Scholar] [CrossRef] [PubMed]
- Sall, A.A.; de A. Zanotto, P.M.; Sene, O.K.; Zeller, H.G.; Digoutte, J.P.; Thiongane, Y.; Bouloy, M. Genetic Reassortment of Rift Valley Fever Virus in Nature. J. Virol. 1999, 73, 8196. [Google Scholar] [PubMed]
- Siam, A.L.; Meegan, J.M.; Gharbawi, K.F. Rift Valley fever ocular manifestations: Observations during the 1977 epidemic in Egypt. Br. J. Ophthalmol. 1980, 64, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazmi, A.; Al-Rajhi, A.A.; Abboud, E.B.; Ayoola, E.A.; Al-Hazmi, M.; Saadi, R.; Ahmed, N. Ocular complications of Rift Valley fever outbreak in Saudi Arabia. Ophthalmology 2005, 112, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Schrire, L. Macular changes in Rift Valley fever. S. Afr. Med. J. 1951, 25, 926–930. [Google Scholar] [PubMed]
- Freed, I. Rift Valley fever in man: Complicated by retinal changes and loss of vision. S. Afr. Med. J. 1951, 25, 930–932. [Google Scholar] [PubMed]
- van Velden, D.J.; Meyer, J.D.; Olivier, J.; Gear, J.H.; McIntosh, B. Rift valley fever affecting humans in South Africa—A clinicopathological study. S. Afr. Med. J. 1977, 51, 867–871. [Google Scholar] [PubMed]
- Faburay, B.; LaBeaud, A.D.; McVey, D.S.; Wilson, W.C.; Richt, J.A. Current Status of Rift Valley Fever Vaccine Development. Vaccines 2017, 5, 29. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables 1 | RVFV Seropositive n/N (%) | Univariable Analysis | Multivariable Analysis 2 | ||
|---|---|---|---|---|---|
| Odds Ratio (CI95%) | p-Value (<0.2) | Odds Ratio (CI95%) | p-Value (<0.05) | ||
| Demographic characteristics | |||||
| Age (years) | |||||
| 16–29 | 5/196 (2.6%) | 1 (base) | - | 1 (base) | - |
| 30–39 | 12/196 (6.1%) | 2.7 (0.8–8.7) | 0.100 | 2.64 (0.76–9.18) | 0.126 |
| 40–49 | 13/114 (11.4%) | 5.9 (1.9–18.2) | 0.002 | 6.91 (2.15–22.2) | 0.001 |
| 50–63 | 20/106 (18.9%) | 12.6 (4.3–37.0) | <0.001 | 12.9 (4.15–40.0) | <0.001 |
| ≥64 | 7/40 (17.5%) | 16.9 (4.3–66.0) | <0.001 | 25.6 (5.50–119) | <0.001 |
| Working on farm (years) | Eliminated | ||||
| ≤5 | 16/299 (5.4%) | 1 (base) | - | ||
| 6–10 | 11/108 (10.2%) | 2.1 (1.0–4.5) | 0.53 | ||
| 11–20 | 14/128 (10.9%) | 2.5 (1.2–5.3) | 0.019 | ||
| 21–30 | 8/64 (12.5%) | 3.1 (1.2–7.9) | 0.016 | ||
| 31–40 | 5/37 (13.5%) | 4.0 (1.4–11.8) | 0.012 | ||
| >40 | 8/48 (16.7%) | 5.3 (2.0–13.6) | 0.001 | ||
| Working with animals (years) | Eliminated | ||||
| ≤5 | 10/240 (4.2%) | 1 (base) | - | ||
| 6–10 | 8/110 (7.3%) | 1.9 (0.8–4.7) | 0.166 | ||
| 11–20 | 15/145 (10.3%) | 3.0 (1.3–7.3) | 0.014 | ||
| 21–30 | 15/85 (17.6%) | 6.1 (2.5–15.2) | <0.001 | ||
| 31–40 | 6/51 (11.8%) | 4.5 (1.4–14.8) | 0.014 | ||
| >40 | 7/48 (14.6%) | 6.3 (2.1–18.6) | 0.001 | ||
| Job | |||||
| Farm worker/herdsman | 46/487 (9.5%) | 1 (base) | - | 1 (base) | - |
| Farm/livestock owner/manager | 15/173 (8.7%) | 0.9 (0.5–1.7) | 0.758 | 1.26 (0.42–3.80) | 0.678 |
| Family, domestic worker, driver | 1/24 (4.2%) | 0.4 (0.05–3.3) | 0.403 | 0.65 (0.06–6.72) | 0.718 |
| Activities in past | |||||
| Cleaning equipment | Eliminated | ||||
| Yes | 53/547 (9.7%) | 1.5 (0.8–2.9) | 0.176 | ||
| No | 9/137 (6.6%) | 1 (base) | - | ||
| Injection and collection of samples from animals | |||||
| Yes | 53/500 (10.6%) | 2.4 (1.2–4.7) | 0.014 | 2.33 (1.03–5.30) | 0.043 |
| No | 9/184 (4.9%) | 1 (base) | - | 1 (base) | - |
| Assisting with birth of animal | Eliminated | ||||
| Yes | 57/577 (9.9%) | 2.1 (0.7–6.3) | 0.172 | ||
| No | 5/107 (4.7%) | 1 (base) | - | ||
| Assisting with surgery | |||||
| Yes | 8/136 (6.0%) | 0.5 (0.3–1.1) | 0.097 | 0.38 (0.15–0.98) | 0.046 |
| No | 54/548 (9.9%) | 1 (base) | - | 1 (base) | - |
| Slaughtering of animals | |||||
| Yes | 58/563 (10.3%) | 3.3 (1.3–8.7) | 0.014 | 3.93 (1.20–12.88) | 0.024 |
| No | 4/121 (3.3%) | 1 (base) | - | 1 (base) | - |
| Burying dead animals | Eliminated | ||||
| Yes | 45/422 (10.7%) | 1.7 (0.9–3.0) | 0.079 | ||
| No | 17/262 (6.5%) | 1 (base) | - | ||
| Eating hooved animal found dead | |||||
| Yes | 42/342 (12.3%) | 3.4 (1.8–6.7) | <0.001 | 3.14 (1.49–6.61) | 0.003 |
| No | 20/342 (5.8%) | 1 (base) | - | 1 (base) | - |
| Measures against mosquito bites | |||||
| Yes | 22/305 (7.2%) | 0.7 (0.4–1.1) | 0.114 | 0.52 (0.29–0.90) | 0.021 |
| No | 40/379 (10.6%) | 1 (base) | - | 1 (base) | - |
| Working on farm with primarily domestic or wild animals | Eliminated | ||||
| Wild | 3/16 (18.8%) | 2.3 (1.2–4.4) | 0.011 | ||
| Domestic | 59/669 (8.8%) | 1 (base) | - | ||
| Working on farm with private or communal land use 3 | |||||
| Communal | 3/44 (6.8%) | 0.8 (0.3–2.4) | 0.656 | 0.75 (0.09–5.93) | 0.784 |
| Private | 59/641 (9.2%) | 1 (base) | - | 1 (base) | - |
| Working on farm that kept cattle | |||||
| Yes | 47/581 (8.1%) | 0.5 (0.2–1.0) | 0.059 | 0.35 (0.14–0.88) | 0.025 |
| No | 15/104 (14.4%) | 1 (base) | - | 1 (base) | - |
| Manmade dam(s) on farm | |||||
| Yes | 54/532 (10.2%) | 2.5 (1.1–5.7) | 0.032 | 2.68 (1.04–6.89) | 0.041 |
| No | 6/139 (4.3%) | 1 (base) | - | 1 (base) | - |
| New animals are quarantined | Eliminated | ||||
| Yes | 7/142 (4.9%) | 0.4 (0.2–1.1) | 0.069 | ||
| No | 55/543 (10.1%) | 1 (base) | - | ||
| Main purpose of farming 3 | |||||
| Meat | 40/367 (10.9%) | 1 (base) | - | 1 (base) | - |
| Dairy | 1/24 (4.2%) | 0.3 (0.03–3.6) | 0.373 | 1.00 (0.13–7.56) | 0.999 |
| Meat-wool | 15/194 (7.7%) | 0.7 (0.4–1.2) | 0.186 | 0.67 (0.34–1.29) | 0.225 |
| Other (milk, bartering, wealth, ceremonial, resale, tourism) | 6/100 (6.0%) | 0.5 (0.2–1.3) | 0.169 | 0.17 (0.03–0.93) | 0.041 |
| Animals are slaughtered on farm | Eliminated | ||||
| Yes | 47/443 (10.6%) | 1.8 (0.8–4.2) | 0.158 | ||
| No | 12/198 (6.1%) | 1 (base) | - | ||
| Animals vaccinated against RVFV in the past | Eliminated | ||||
| Yes | 41/357 (11.5%) | 1.9 (1.1–3.3) | 0.027 | ||
| No | 19/300 (6.3%) | 1 (base) | - | ||
| RVF on farm in past incl. participants working there 4 years or more only | Not included | ||||
| Yes | 19/149 (12.8%) | 1.3 (0.6–2.7) | 0.498 | Checked for confounding | |
| No | 28/272 (10.3%) | 1 (base) | - | ||
| Drinking milk | Not included | ||||
| Pasteurised/boiled | 19/233 (8.2%) | 1 (base) | |||
| On occasion raw | 5/56 (8.9%) | 1.2 (0.4–3.6) | 0.762 | ||
| Raw | 27/292 (9.2%) | 1.1 (0.5–2.2) | 0.817 | ||
| Variables 1 | RVFV Seropositive n/N (%) | Univariable Analysis | Multivariable Analysis 2 | ||
|---|---|---|---|---|---|
| Odds Ratio (CI95%) | p-Value (<0.2) | Odds Ratio (CI95%) | p-Value (<0.05) | ||
| Demographic characteristics | |||||
| Age (years) | |||||
| 16–49 | 1/98 (1.0%) | 1 (base) | - | 1 (base) | - |
| 50–63 | 6/22 (27.3%) | 92.5 (7.2–1196) | 0.001 | 92.5 (7.16–1196) | 0.001 |
| ≥64 | 2/7 (28.6%) | 166 (7.2–3916) | 0.002 | 167 (7.08–3916) | 0.002 |
| Working as AHCW (years) | Eliminated | ||||
| ≤40 | 1/85 (1.2%) | 1 (base) | - | ||
| 41–50 | 5/22 (22.7%) | 62.4 (2.07–1886) | 0.018 | ||
| ≥51 | 4/15 (26.7%) | 65.4 (3.9–1110) | 0.004 | ||
| Job description | |||||
| Animal health tech | 2/37 (5.4%) | 1 (base) | - | 1 (base) | - |
| Veterinarian | 6/66 (9.1%) | 1.75 (0.40–7.57) | 0.450 | 0.11 (0.01–1.72) | 0.116 |
| Other (incl. vet nurse, researcher, wildlife capturers) 3 | 2/19 (10.5%) | 2.06 (0.28–15.03) | 0.473 | 0.74 (0.05–11.01) | 0.825 |
| Activities in past | |||||
| Cleaning waste | Eliminated | ||||
| Yes | 9/83 (10.8%) | 3.4 (0.7–16.6) | 0.137 | ||
| No | 2/55 (3.6%) | 1 (base) | - | ||
| Working with hoofed animals | Eliminated | ||||
| <1 h | 3/67 (4.5%) | 1 (base) | - | ||
| Half day | 3/37 (8.1%) | 1.7 (0.3–9.7) | 0.548 | ||
| Whole day | 5/34 (14.7%) | 3.6 (0.7–17.3) | 0.110 | ||
| Contact with RVF positive animals in the past | Eliminated | ||||
| Yes | 9/82 (11.0%) | 5.1 (0.7–38.6) | 0.112 | ||
| No | 1/40 (2.5%) | 1 (base) | - | ||
| Taking measures against mosquito bites | Eliminated | ||||
| Yes | 4/84 (4.8%) | 0.4 (0.1–1.6) | 0.193 | ||
| No | 7/54 (13.0%) | 1 (base) | - | ||
| Drinking milk | Eliminated | ||||
| Yes | 8/125 (6.4%) | 0.18 (0.03–0.98) | 0.047 | ||
| No | 3/13 (23.1%) | 1 (base) | - | ||
| Conditions | |||||
| On chronic medication | Eliminated | ||||
| Yes | 5/43 (11.6%) | 2.6 (0.7–9.8) | 0.170 | ||
| No | 6/95 (6.3%) | 1 (base) | |||
| Chronic liver disease | Eliminated | ||||
| Yes | 1/2 (50%) | 11.8 (0.6–229) | 0.102 | ||
| No | 10/136 (7.4%) | 1 (base) | - | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Msimang, V.; Thompson, P.N.; Jansen van Vuren, P.; Tempia, S.; Cordel, C.; Kgaladi, J.; Khosa, J.; Burt, F.J.; Liang, J.; Rostal, M.K.; et al. Rift Valley Fever Virus Exposure amongst Farmers, Farm Workers, and Veterinary Professionals in Central South Africa. Viruses 2019, 11, 140. https://doi.org/10.3390/v11020140
Msimang V, Thompson PN, Jansen van Vuren P, Tempia S, Cordel C, Kgaladi J, Khosa J, Burt FJ, Liang J, Rostal MK, et al. Rift Valley Fever Virus Exposure amongst Farmers, Farm Workers, and Veterinary Professionals in Central South Africa. Viruses. 2019; 11(2):140. https://doi.org/10.3390/v11020140
Chicago/Turabian StyleMsimang, Veerle, Peter N. Thompson, Petrus Jansen van Vuren, Stefano Tempia, Claudia Cordel, Joe Kgaladi, Jimmy Khosa, Felicity J. Burt, Janice Liang, Melinda K. Rostal, and et al. 2019. "Rift Valley Fever Virus Exposure amongst Farmers, Farm Workers, and Veterinary Professionals in Central South Africa" Viruses 11, no. 2: 140. https://doi.org/10.3390/v11020140
APA StyleMsimang, V., Thompson, P. N., Jansen van Vuren, P., Tempia, S., Cordel, C., Kgaladi, J., Khosa, J., Burt, F. J., Liang, J., Rostal, M. K., Karesh, W. B., & Paweska, J. T. (2019). Rift Valley Fever Virus Exposure amongst Farmers, Farm Workers, and Veterinary Professionals in Central South Africa. Viruses, 11(2), 140. https://doi.org/10.3390/v11020140