CD4 and CD8 Lymphocyte Counts as Surrogate Early Markers for Progression in SARS-CoV-2 Pneumonia: A Prospective Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Assessments
2.2. Lymphocyte Subsets Determination
2.3. Statistical Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.-E.; Katsaounou, P.; et al. Complex Immune Dysregulation in COVID-19 Patients with Severe Respiratory Failure. Cell Host Microbe 2020, 27, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef] [PubMed]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; Macary, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Li, T.; Qiu, Z.; Zhang, L.; Han, Y.; He, W.; Liu, Z.-Y.; Ma, X.; Fan, H.; Lu, W.; Xie, J.; et al. Significant Changes of Peripheral T Lymphocyte Subsets in Patients with Severe Acute Respiratory Syndrome. J. Infect. Dis. 2004, 189, 648–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Janice, O.H.L.; Ken-En Gan, S.; Bertoletti, A.; Tan, Y.J. Understanding the T cell immune response in SARS coronavirus infection. Emerg. Microbes Infect. 2012, 1, e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Wu, Z.; Li, J.-W.; Zhao, H.; Wang, G.-Q. Cytokine release syndrome in severe COVID-19: Interleukin-6 receptor antagonist tocilizumab may be the key to reduce mortality. Int. J. Antimicrob. Agents 2020, 55, 105954. [Google Scholar] [CrossRef]
- Martínez-Sanz, J.; Muriel, A.; Ron, R.; Herrera, S.; Pérez-Molina, J.A.; Moreno, S.; Serrano-Villar, S. Effects of Tocilizumab on Mortality in Hospitalized Patients with COVID-19: A Multicenter Cohort Study. Clin. Microbiol. Infect. 2020. [CrossRef]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.V.A.O.; et al. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients With Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA 2020, 324, 1307. [Google Scholar] [CrossRef]
- Cecconi, M.; Piovani, D.; Brunetta, E.; Aghemo, A.; Greco, M.; Ciccarelli, M.; Angelini, C.; Voza, A.; Omodei, P.; Vespa, E.; et al. Early Predictors of Clinical Deterioration in a Cohort of 239 Patients Hospitalized for Covid-19 Infection in Lombardy, Italy. J. Clin. Med. 2020, 9, 1548. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.; Su, W.; Tang, H.; Le, W.; Zhang, X.; Zheng, Y.; Ding, W.; Xie, L.; Li, J.; Ye, J.; et al. Immune cell profiling of COVID-19 patients in the recovery stage by single-cell sequencing. Cell Discov. 2020, 6, 31. [Google Scholar] [CrossRef]
- Whitmire, J.K. Induction and function of virus-specific CD4+ T cell responses. Virology 2011, 411, 216–228. [Google Scholar] [CrossRef] [Green Version]
- Channappanavar, R.; Zhao, J.; Perlman, S. T cell-mediated immune response to respiratory coronaviruses. Immunol. Res. 2014, 59, 118–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, D.-W.; Zhang, D.; Tian, R.-H.; Li, Y.; Wang, Y.-S.; Cao, J.; Tang, Y.; Zhang, N.; Zan, T.; Gao, L.; et al. The underlying changes and predicting role of peripheral blood inflammatory cells in severe COVID-19 patients: A sentinel? Clin. Chim. Acta 2020, 508, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Nie, J.; Wang, H.; Zhao, Q.; Xiong, Y.; Deng, L.; Song, S.; Ma, Z.; Mo, P.; Zhang, Y. Characteristics of Peripheral Lymphocyte Subset Alteration in COVID-19 Pneumonia. J. Infect. Dis. 2020, 221, 1762–1769. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Zhao, J.; Perlman, S. T cell responses are required for protection from clinical disease and for virus clearance in severe acute respiratory syndrome coronavirus-infected mice. J. Virol. 2010, 84, 9318–9325. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Lau, Y.F.; Lamirande, E.W.; Paddock, C.D.; Bartlett, J.H.; Zaki, S.R.; Subbarao, K. Cellular immune responses to severe acute respiratory syndrome coronavirus (SARS-CoV) infection in senescent BALB/c mice: CD4+ T cells are important in control of SARS-CoV infection. J. Virol. 2010, 84, 1289–1301. [Google Scholar] [CrossRef] [Green Version]
- Jiang, M.; Guo, Y.; Luo, Q.; Huang, Z.; Zhao, R.; Liu, S.; Le, A.; Li, J.; Wan, L. T cell subset counts in peripheral blood can be used as discriminatory biomarkers for diagnosis and severity prediction of COVID-19. J. Infect. Dis. 2020, 222, 198–202. [Google Scholar] [CrossRef]
- Urra, J.; Cabrera, C.; Porras, L.; Ródenas, I. Selective CD8 cell reduction by SARS-CoV-2 is associated with a worse prognosis and systemic inflammation in COVID-19 patients. Clin. Immunol. 2020, 217, 108486. [Google Scholar] [CrossRef]
- Sun, Y.; Dong, Y.; Wang, L.; Xie, H.; Li, B.; Chang, C.; Wang, F.-S. Characteristics and prognostic factors of disease severity in patients with COVID-19: The Beijing experience. J. Autoimmun. 2020, 112, 102473. [Google Scholar] [CrossRef]
- Zheng, H.-Y.; Zhang, M.; Yang, C.-X.; Zhang, N.; Wang, X.-C.; Yang, X.-P.; Dong, X.-Q.; Zheng, Y.-T. Elevated exhaustion levels and reduced functional diversity of T cells in peripheral blood may predict severe progression in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 541–543. [Google Scholar] [CrossRef]
- Hengeveld, P.J.; Khader, A.O.; De Bruin, L.H.A.; Geelen, I.G.P.; Van Baalen, E.A.; Jansen, E.; Bouwer, N.I.; Balak, Ö.; Riedl, J.A.; Langerak, A.W.; et al. Blood cell counts and lymphocyte subsets of patients admitted during the COVID-19 pandemic: A prospective cohort study. Br. J. Haematol. 2020, 190. [Google Scholar] [CrossRef]
- Hoffmann, H.-H.; Schneider, W.M.; Sánchez-Rivera, F.J.; Luna, J.M.; Ashbrook, A.W.; Soto-Feliciano, Y.M.; Leal, A.A.; Le Pen, J.; Ricardo-Lax, I.; Michailidis, E.; et al. Functional interrogation of a SARS-CoV-2 host protein interactome identifies unique and shared coronavirus host factors. bioRxiv 2020. [CrossRef]
- Ganji, A.; Farahani, I.; Khansarinejad, B.; Ghazavi, A.; Mosayebi, G. Increased expression of CD8 marker on T-cells in COVID-19 patients. Blood Cells Mol. Dis. 2020, 83, 102437. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Jurado, A.; Martin, M.C.; Abad-Molina, C.; Orduna, A.; Martinez, A.; Ocana, E.; Yarce, O.; Navas, A.M.; Trujillo, A.; Fernandez-Pereira, L.; et al. COVID-19: Age, Interleukin-6, C-Reactive Protein and lymphocytes as key clues from a multicentre retrospective study in Spain. medRxiv 2020. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Shang, W.; Dong, J.; Ren, Y.; Tian, M.; Li, W.; Hu, J.; Li, Y. The value of clinical parameters in predicting the severity of COVID-19. J. Med. Virol. 2020, 92, 2188–2192. [Google Scholar] [CrossRef] [PubMed]
- Du, R.-H.; Liang, L.-R.; Yang, C.-Q.; Wang, W.; Cao, T.-Z.; Li, M.; Guo, G.-Y.; Du, J.; Zheng, C.-L.; Zhu, Q.; et al. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: A prospective cohort study. Eur. Respir. J. 2020, 55, 2000524. [Google Scholar] [CrossRef] [Green Version]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Friedman, J.H.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2008, 33, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Efron, B. Annals of Statistics. Bootstrap Methods: Another Look at the Jackknife. Ann. Stat. 1979, 7, 1–26. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Re, S.L.; Lison, D.; Huaux, F. CD4+ T lymphocytes in lung fibrosis: Diverse subsets, diverse functions. J. Leukoc. Biol. 2013, 93, 499–510. [Google Scholar]
- Sun, Q.; Li, L.; Ji, S.; Chen, J.; Yin, G.; Tang, Z.; Liu, Z. Variation of CD4+ and CD8+ T lymphocytes as predictor of outcome in renal allograft recipients who developed acute respiratory distress syndrome caused by cytomegalovirus pneumonia. Transplant. Proc. 2005, 37, 2118–2121. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics and Blood Measurements | All (n = 30) | Non-Critical (n = 17) | Critical (n = 13) | p-Value |
|---|---|---|---|---|
| Age | 60.6 (6.1, 63.3) | 60.1 (51.7, 74.9) | 61.1 (55.2, 64.5) | 0.9833 |
| Gender (Male) | 20 (66.7%) | 12 (70.6%) | 8 (61.5%) | 0.6030 |
| Days of symptoms onset | 7.000 (6.000, 10.000) | 7.000 (4.000, 11.000) | 6.000 (5.000, 10.000) | 0.6439 |
| Days to hospital discharge | 8.000 (5.000, 14.000) | 5.000 (4.000, 6.000) | 15.500 (12.000, 22.000) | <0.001 |
| HT | 6 (20.0%) | 3 (17.6%) | 3 (23.1%) | 0.7134 |
| DM | 1 (3.3%) | 1 (5.9%) | 0 (0.0%) | 0.2810 |
| DLP | 5 (16.7%) | 2 (11.8%) | 3 (23.1%) | 0.4119 |
| OBESITY | 1 (3.3%) | 0 (0.0%) | 1 (7.7%) | 0.1900 |
| Leucocyte count (cells × 109/L) | 6310 (5310, 8860) | 6550 (5310, 9440) | 5970 (5120, 11370) | 0.4512 |
| Neutrophyl count (cells × 109/L) | 4440 (3920, 6650) | 4570 (3950, 7030) | 4200 (2900, 9370) | 0.4388 |
| Lymphocyte count (cells × 109/L) | 1215 (1040, 1310) | 1260 (1040, 1440) | 1180 (920, 1840) | 0.5030 |
| Ratio N/L | 4.26 (3.05, 5.08) | 4.19 (2.90, 5.08) | 4.33 (1.58, 7.95) | 0.8835 |
| Ferritin (ng/mL) | 711.7 (382.6, 1136.2) | 639.7 (270.6, 1136.2) | 783.7 (354.5, 2390) | 0.2330 |
| CRP (mg/dL) | 8.80 (5.07, 11.25) | 8.54 (4.74, 11.25) | 9.50 (5.00, 15.64) | 0.3909 |
| D-Dimer (mg/mL) | 691 (443, 860) | 703 (443, 860) | 679 (269, 1722) | 0.7695 |
| LDH (U/L) | 282 (244, 365) | 267 (238, 387) | 356 (243, 446) | 0.1713 |
| T lymphocyte count | 714 (497, 823) | 725 (497, 1119) | 647 (375, 1113) | 0.4025 |
| CD3+CD4+ count | 467 (303, 574) | 545 (445, 767) | 278 (178, 663) | 0.0180 |
| CD3+CD8+ count | 245 (171, 319) | 253 (145, 319) | 237 (87, 586) | 0.7064 |
| CD3+CD4+CD8+ count | 13 (8, 21) | 16 (9, 24) | 11 (4, 35) | 0.295 |
| CD3+CD4−CD8− count | 18.000 (12.000, 23.000) | 19 (12, 27) | 12 (5, 23) | 0.2249 |
| B Lymphocyte count | 112 (78, 162) | 121 (86, 185) | 79 (46, 197) | 0.3254 |
| Natural Killer count | 196 (154, 253) | 192 (140, 278) | 234 (128, 327) | 0.8017 |
| Ratio CD4+/CD8+ | 1.91 (1.58, 3.12) | 3.12 (1.58, 3.99) | 1.72 (0.78, 2.52) | 0.0135 |
| CD4+ MFI | 24861 (22770, 26259) | 26259 (24683, 27939) | 21820 (20666, 25157) | 0.0013 |
| CD8+ MFI | 25856 (23819, 27476) | 25948 (23819, 27607) | 25337 (22878, 32176) | 0.7855 |
| Blood Determinations | Adjusted Means (95% CI) | F-Test | |
|---|---|---|---|
| Non-Critical | Critical | p-Value | |
| Leucocyte count (cells × 109/L) | 7292.5 (5851.2, 9088.9) | 6789.8 (5275.6, 8738.5) | 0.6665 |
| Neutrophyl count (cells × 109/L) | 5167.1 (3921.5, 6808.3) | 4871.5 (3551.3, 6682.3) | 0.7764 |
| Lymphocyte count (cells × 109/L) | 1281.7 (1081.5, 1519.0) | 1209.2 (995.3, 1468.9) | 0.6487 |
| Ratio N/L | 4.03 (2.89, 5.62) | 4.03 (2.75, 5.91) | 0.9980 |
| Ferritin (ng/mL) | 485.2 (290.9, 809.1) | 981.9 (546.5, 1764.2) | 0.0757 |
| CRP (mg/dL) | 7.37 (4.56, 10.84) | 8.93 (5.41, 13.33) | 0.5285 |
| D-Dimer (mg/mL) | 573.9 (426.2, 814.4) | 588.6 (418.3, 888.8) | 0.9175 |
| LDH (U/L) | 268.5 (229.0, 319.2) | 341.4 (280.2, 425.1) | 0.0776 |
| T lymphocyte count | 829.3 (606.8, 1086.5) | 683.3 (456.6, 955.6) | 0.3991 |
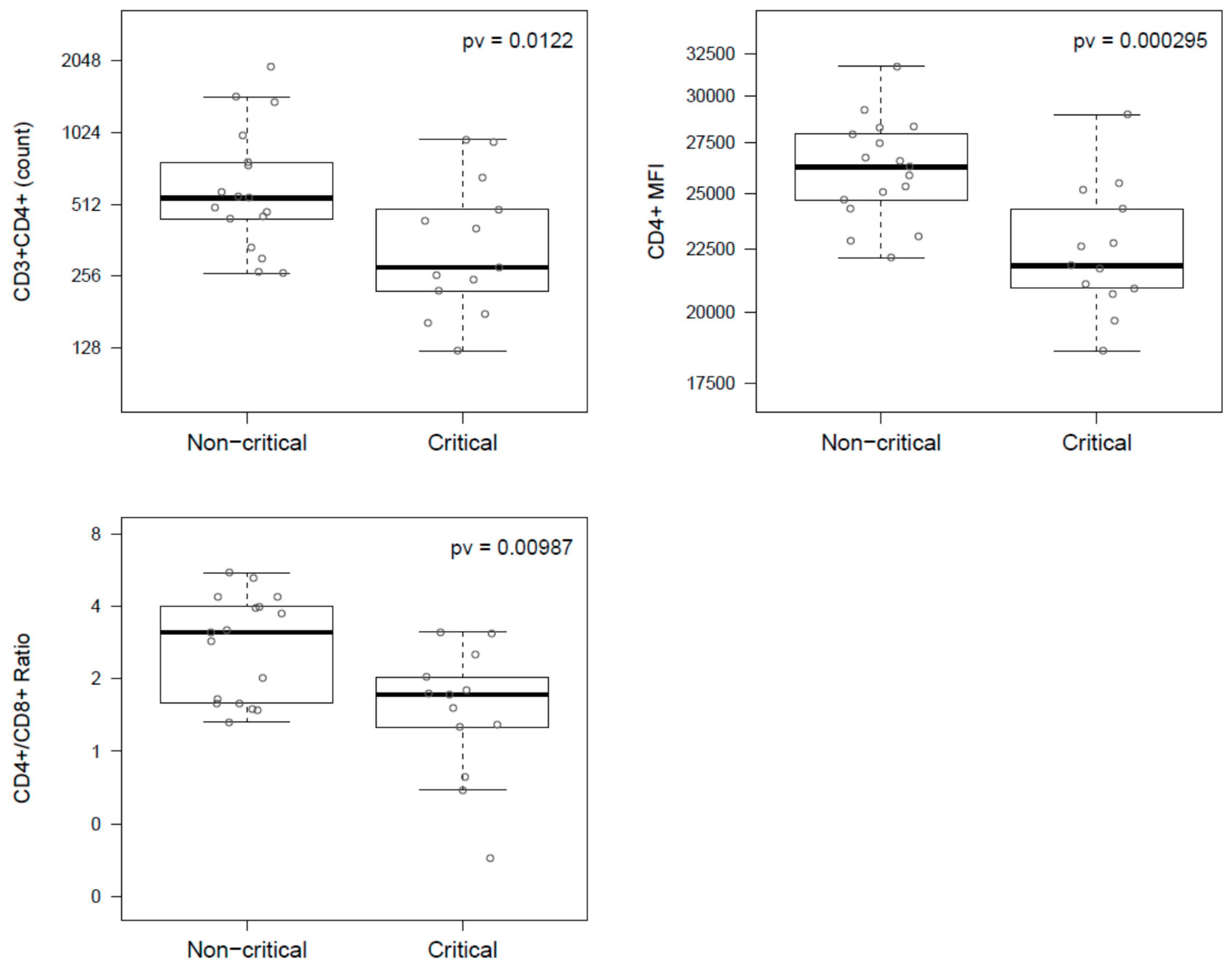
| CD3+CD4+ count | 597.8 (445.8, 801.6) | 331.5 (236.9, 464.0) | 0.0122 |
| CD3+CD8+ count | 214.8 (153.1, 301.5) | 217.2 (147.3, 320.3) | 0.9659 |
| CD3+CD4+CD8+ count | 15.4 (9.8, 24.3) | 11.5 (6.8, 19.5) | 0.4027 |
| CD3+CD4−CD8− count | 19.3 (12.4, 30.1) | 10.7 (6.4, 17.7) | 0.0840 |
| B Lymphocyte count | 129.7 (92.5, 173.3) | 101.9 (65.0, 147.0) | 0.3356 |
| Natural Killer count | 198.0 (148.9, 254.1) | 199.4 (143.5, 264.4) | 0.9725 |
| Ratio CD4+/CD8+ | 2.65 (2.01, 3.50) | 1.49 (1.08, 2.05) | 0.0010 |
| CD4+ MFI | 26128 (24878, 27441) | 22416 (21192, 23712) | 0.0003 |
| CD8+ MFI | 26076 (23953, 28386) | 25863 (23465, 28506) | 0.8980 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvet, J.; Gratacós, J.; Amengual, M.J.; Llop, M.; Navarro, M.; Moreno, A.; Berenguer-Llergo, A.; Serrano, A.; Orellana, C.; Cervantes, M. CD4 and CD8 Lymphocyte Counts as Surrogate Early Markers for Progression in SARS-CoV-2 Pneumonia: A Prospective Study. Viruses 2020, 12, 1277. https://doi.org/10.3390/v12111277
Calvet J, Gratacós J, Amengual MJ, Llop M, Navarro M, Moreno A, Berenguer-Llergo A, Serrano A, Orellana C, Cervantes M. CD4 and CD8 Lymphocyte Counts as Surrogate Early Markers for Progression in SARS-CoV-2 Pneumonia: A Prospective Study. Viruses. 2020; 12(11):1277. https://doi.org/10.3390/v12111277
Chicago/Turabian StyleCalvet, Joan, Jordi Gratacós, María José Amengual, Maria Llop, Marta Navarro, Amàlia Moreno, Antoni Berenguer-Llergo, Alejandra Serrano, Cristóbal Orellana, and Manel Cervantes. 2020. "CD4 and CD8 Lymphocyte Counts as Surrogate Early Markers for Progression in SARS-CoV-2 Pneumonia: A Prospective Study" Viruses 12, no. 11: 1277. https://doi.org/10.3390/v12111277
APA StyleCalvet, J., Gratacós, J., Amengual, M. J., Llop, M., Navarro, M., Moreno, A., Berenguer-Llergo, A., Serrano, A., Orellana, C., & Cervantes, M. (2020). CD4 and CD8 Lymphocyte Counts as Surrogate Early Markers for Progression in SARS-CoV-2 Pneumonia: A Prospective Study. Viruses, 12(11), 1277. https://doi.org/10.3390/v12111277