Feline Parvovirus Seroprevalence Is High in Domestic Cats from Disease Outbreak and Non-Outbreak Regions in Australia

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
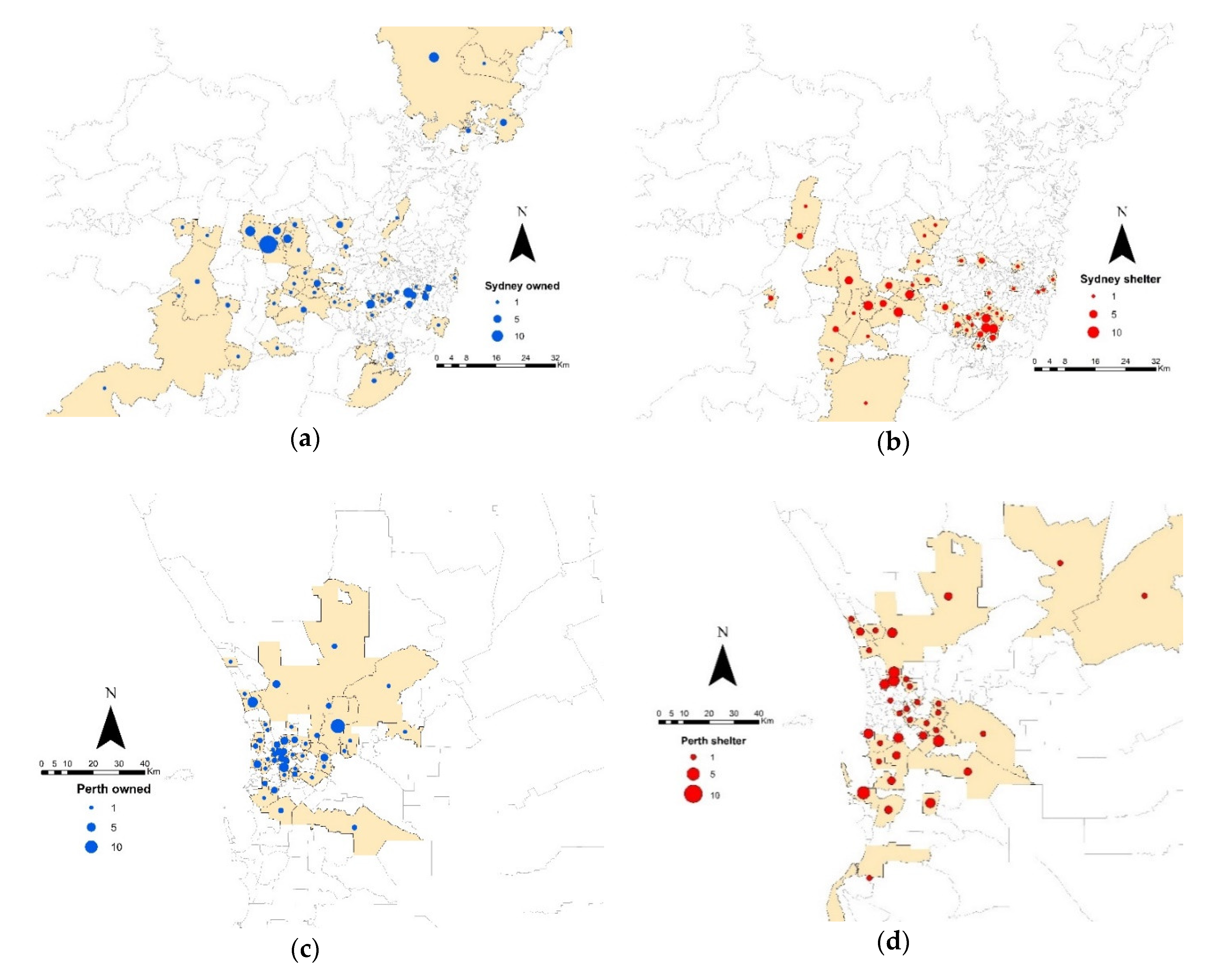
2.1. Study Populations
2.2. Sampling and Data Collection
2.3. Haemagglutination Inhibition (HI) Serology
2.4. Statistical Analysis
3. Results
3.1. Animals
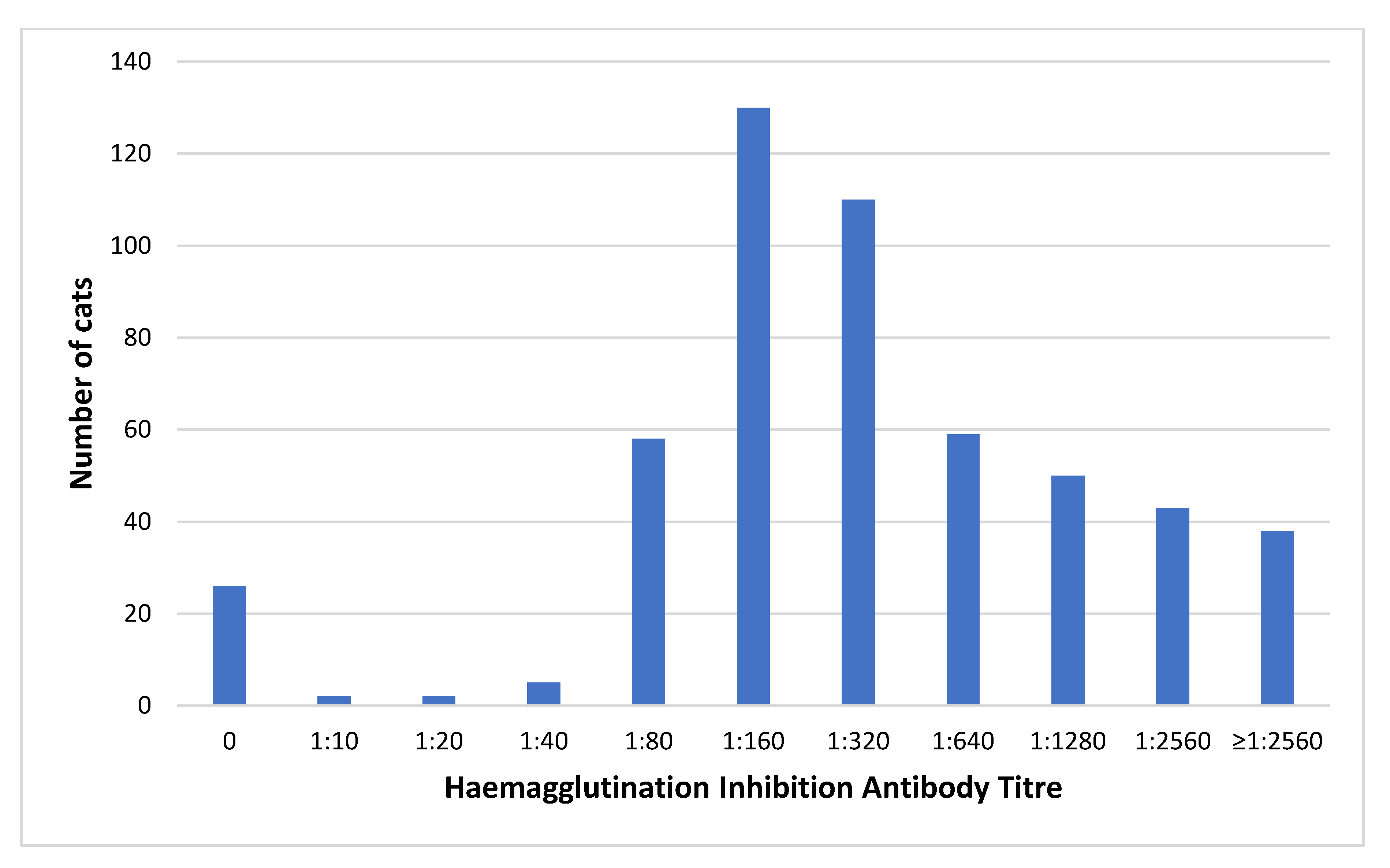
3.2. Seroprevalence and Variables Associated with a Protective FPV Titre
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barrs, V.R. Feline Panleukopenia: A Re-emergent Disease. Vet. Clin. Small Anim. Pract. 2019, 49, 651–670. [Google Scholar] [CrossRef] [PubMed]
- Van Brussel, K.; Carrai, M.; Lin, C.; Kelman, M.; Setyo, L.; Aberdein, D.; Brailey, J.; Lawler, M.; Maher, S.; Plaganyi, I.; et al. Distinct Lineages of Feline Parvovirus Associated with Epizootic Outbreaks in Australia, New Zealand and the United Arab Emirates. Viruses 2019, 11, 1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lappin, M.R.; Andrews, J.; Simpson, D.; Jensen, W.A. Use of serologic tests to predict resistance to feline herpesvirus 1, feline calicivirus, and feline parvovirus infection in cats. J. Am. Vet. Med. Assoc. 2002, 220, 38–42. [Google Scholar] [CrossRef]
- Scott, F.W.; Geissinger, C.M. Long-term immunity in cats vaccinated with an inactivated trivalent vaccine. Am. J. Vet. Res. 1999, 60, 652–658. [Google Scholar]
- Jakel, V.; Cussler, K.; Hanschmann, K.M.; Truyen, U.; Konig, M.; Kamphuis, E.; Duchow, K. Vaccination against Feline Panleukopenia: Implications from a field study in kittens. BMC Vet. Res. 2012, 8, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mende, K.; Stuetzer, B.; Truyen, U.; Hartmann, K. Evaluation of an in-house dot enzyme-linked immunosorbent assay to detect antibodies against feline panleukopenia virus. J. Feline Med. Surg. 2014, 16, 805–811. [Google Scholar] [CrossRef]
- Mouzin, D.E.; Lorenzen, M.J.; Haworth, J.D.; King, V.L. Duration of serologic response to three viral antigens in cats. J. Am. Vet. Med. Assoc. 2004, 224, 61–66. [Google Scholar] [CrossRef]
- Mende, K.; Stuetzer, B.; Sauter-Louis, C.; Homeier, T.; Truyen, U.; Hartmann, K. Prevalence of antibodies against feline panleukopenia virus in client-owned cats in Southern Germany. Vet. J. 2014, 199, 419–423. [Google Scholar] [CrossRef]
- DiGangi, B.A.; Levy, J.K.; Griffin, B.; McGorray, S.P.; Dubovi, E.J.; Dingman, P.A.; Tucker, S.J. Prevalence of serum antibody titers against feline panleukopenia virus, feline herpesvirus 1, and feline calicivirus in cats entering a Florida animal shelter. J. Am. Vet. Med. Assoc. 2012, 241, 1320–1325. [Google Scholar] [CrossRef]
- Coman, B.J.; Jones, E.H.; Westbury, H.A. Protozoan and viral infections of feral cats. Aust. Vet. J. 1981, 57, 319–323. [Google Scholar] [CrossRef]
- Day, M.J.; Horzinek, M.C.; Schultz, R.D.; Squires, R.A. WSAVA Guidelines for the vaccination of dogs and cats. J. Small Anim. Pract. 2010, 51, e1–e32. [Google Scholar] [CrossRef] [Green Version]
- Hellard, E.; Fouchet, D.; Santin-Janin, H.; Tarin, B.; Badol, V.; Coupier, C.; Leblanc, G.; Poulet, H.; Pontier, D. When cats’ ways of life interact with their viruses: A study in 15 natural populations of owned and unowned cats (Felis silvestris catus). Prev. Vet. Med. 2011, 101, 250–264. [Google Scholar] [CrossRef]
- Dall’Ara, P.; Labriola, C.; Sala, E.; Spada, E.; Magistrelli, S.; Lauzi, S. Prevalence of serum antibody titres against feline panleukopenia, herpesvirus and calicivirus infections in stray cats of Milan, Italy. Prev. Vet. Med. 2019, 167, 32–38. [Google Scholar] [CrossRef]
- Dhand, N.K.; Khakar, M.S. Statulator: An online statistical calculator. Sample Size Calculator for Comparing Two Independent Proportions. Available online: http://statulator.com/SampleSize/ss2P.html (accessed on 5 January 2020).
- Select Statistical Services Odds Ratio—Sample Size. Available online: https://select-statistics.co.uk/calculators/sample-size-calculator-odds-ratio/ (accessed on 16 March 2020).
- Cavalli, A.; Desario, C.; Marinaro, M.; Losurdo, M.; Camero, M.; Decaro, N.; Catella, C.; Lanave, G.; Buonavoglia, C. Oral administration of modified live canine parvovirus type 2b induces systemic immune response. Vaccine 2020, 38, 115–118. [Google Scholar] [CrossRef]
- Johnson, R.H. Serologic procedures for the study of feline panleukopenia. J. Am. Vet. Med. Assoc. 1971, 158, 876. [Google Scholar]
- Duijvestijn, M.; Mughini-Gras, L.; Schuurman, N.; Schijf, W.; Wagenaar, J.A.; Egberink, H. Enteropathogen infections in canine puppies: (Co-)occurrence, clinical relevance and risk factors. Vet. Microbiol. 2016, 195, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. Postal Area, SA1 Distributions, SEIFA 2011; Australian Bureau of Statistics: Canberra, Australia, 2013. [Google Scholar]
- Haselberger, A.; Tichy, A.; Mostl, K. Evaluation of antibody titres against feline Panleukopenia Virus, feline Herpesvirus-1 and feline Calicivirus in cats in eastern Austria. Wien. Tierarztl. Mon. 2016, 103, 149–161. [Google Scholar]
- Yamaguchi, N.; Macdonald, D.W.; Passanisi, W.C.; Harbour, D.A.; Hopper, C.D. Parasite prevalence in free-ranging farm cats, Felis silvestris catus. Epidemiol. Infect. 1996, 116, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Miyazawa, T.; Ikeda, Y.; Nakamura, K.; Naito, R.; Mochizuki, M.; Tohya, Y.; Vu, D.; Mikami, T.; Takahashi, E. Isolation of feline parvovirus from peripheral blood mononuclear cells of cats in northern Vietnam. Microbiol. Immunol. 1999, 43, 609–612. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, K.; Ikeda, Y.; Miyazawa, T.; Nguyen, N.T.P.; Duong, D.D.; Le, K.H.; Vo, S.D.; Phan, L.V.; Mikami, T.; Takahashi, E. Comparison of prevalence of feline herpesvirus type 1, calicivirus and parvovirus infections in domestic and leopard cats in Vietnam. J. Vet. Med Sci. 1999, 61, 1313–1315. [Google Scholar] [CrossRef] [Green Version]
- Ostrowski, S.; Van Vuuren, M.; Lenain, D.M.; Durand, A. A serologic survey of wild felids from central west Saudi Arabia. J. Wildl. Dis. 2003, 39, 696–701. [Google Scholar] [CrossRef] [Green Version]
- Levy, J.; Crawford, P.; Lappin, M.; Dubovi, E.; Levy, M.; Alleman, R.; Tucker, S.; Clifford, E. Infectious diseases of dogs and cats on Isabela Island, Galapagos. J. Vet. Intern. Med. 2008, 22, 60–65. [Google Scholar] [CrossRef]
- Fischer, S.M.; Quest, C.M.; Dubovi, E.J.; Davis, R.D.; Tucker, S.J.; Friary, J.A.; Crawford, P.C.; Ricke, T.A.; Levy, J.K. Response of feral cats to vaccination at the time of neutering. J. Am. Vet. Med. Assoc. 2007, 230, 52–58. [Google Scholar] [CrossRef]
- Pavlova, E.V.; Kirilyuk, V.E.; Naidenko, S.V. Patterns of seroprevalence of feline viruses among domestic cats (Felis catus) and Pallas’ cats (Otocolobus manul) in Daursky Reserve, Russia. Can. J. Zool. 2015, 93, 849–855. [Google Scholar] [CrossRef]
- Blanco, K.; Prendas, J.; Cortes, R.; Jimenez, C.; Dolz, G. Seroprevalence of Viral Infections in Domestic Cats in Costa Rica. J. Vet. Med Sci. 2009, 71, 661–663. [Google Scholar] [CrossRef] [Green Version]
- Lickey, A.L.A.; Kennedy, M.; Patton, S.; Ramsay, E.C. Serologic survey of domestic felids in the Peten region of Guatemala. J. Zool. Wildl. Med. 2005, 36, 121–123. [Google Scholar] [CrossRef]
- Johnson, R.H. Feline panleucopaenia. Vet. Rec. 1969, 84, 338–340. [Google Scholar] [CrossRef]
- Johnson, R.H. Feline panleucopaenia virus. 3. Some properties compared to a feline herpes virus. Res. Vet. Sci. 1966, 7, 112–115. [Google Scholar] [CrossRef]
- Bergmann, M.; Schwertler, S.; Speck, S.; Truyen, U.; Reese, S.; Hartmann, K. Faecal shedding of parvovirus deoxyribonucleic acid following modified live feline panleucopenia virus vaccination in healthy cats. Vet. Rec. 2019, 185, 83. [Google Scholar] [CrossRef]
- Hoelzer, K.; Parrish, C.R. The emergence of parvoviruses of carnivores. Vet. Res. 2010, 41, 39. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, K.; Ikeda, Y.; Miyazawa, T.; Tohya, Y.; Takahashi, E.; Mochizuki, M. Characterisation of cross-reactivity of virus neutralising antibodies induced by feline panleukopenia virus and canine parvoviruses. Res. Vet. Sci. 2001, 71, 219–222. [Google Scholar] [CrossRef]
- Truyen, U.; Parrish, C.R. Feline panleukopenia virus: Its interesting evolution and current problems in immunoprophylaxis against a serious pathogen. Vet. Microbiol. 2013, 165, 29–32. [Google Scholar] [CrossRef]
- Jack, S.C.; Sutton, D.; Bhogle, A.; Spibey, N.; Francis, M. FPL-vaccinated cats are protected from CPV2c and CPV2b challenge. Vet. Rec. 2014, 174, 146. [Google Scholar] [CrossRef]
- Balboni, A.; Bassi, F.; De Arcangeli, S.; Zobba, R.; Dedola, C.; Alberti, A.; Battilani, M. Molecular analysis of carnivore Protoparvovirus detected in white blood cells of naturally infected cats. BMC Vet. Res. 2018, 14, 41. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, Y.; Mochizuki, M.; Naito, R.; Nakamura, K.; Miyazawa, T.; Mikami, T.; Takahashi, E. Predominance of canine parvovirus (CPV) in unvaccinated cat populations and emergence of new antigenic types of CPVs in cats. Virology 2000, 278, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Marenzoni, M.L.; Antognoni, M.T.; Baldelli, F.; Miglio, A.; Stefanetti, V.; Desario, C.; Di Summa, A.; Buonavoglia, C.; Decaro, N. Detection of parvovirus and herpesvirus DNA in the blood of feline and canine blood donors. Vet. Microbiol. 2018, 224, 66–69. [Google Scholar] [CrossRef]
- Stuetzer, B.; Hartmann, K. Feline parvovirus infection and associated diseases. Vet. J. 2014, 201, 150–155. [Google Scholar] [CrossRef]
- Piewbang, C.; Kasantikul, T.; Pringproa, K.; Techangamsuwan, S. Feline bocavirus-1 associated with outbreaks of hemorrhagic enteritis in household cats: Potential first evidence of a pathological role, viral tropism and natural genetic recombination. Nat. Sci. Rep. 2019, 9, 16367. [Google Scholar] [CrossRef] [Green Version]
- Foley, J.E.; Orgad, U.; Hirsh, D.C.; Poland, A.; Pedersen, N.C. Outbreak of fatal salmonellosis in cats following use of a high-titer modified-live panleukopenia virus vaccine. J. Am. Vet. Med. Assoc. 1999, 214, 67–70. [Google Scholar]
- Ossent, P. Systemic aspergillosis and mucormycosis in 23 cats. Vet. Rec. 1987, 120, 330–333. [Google Scholar] [CrossRef]
- Metcalf, C.J.E.; Ferrari, M.; Graham, A.L.; Grenfell, B.T. Understanding Herd Immunity. Trends Immunol. 2015, 36, 753–755. [Google Scholar] [CrossRef] [Green Version]
- Guerra, F.M.; Bolotin, S.; Lim, G.; Heffernan, J.; Deeks, S.L.; Li, Y.; Crowcroft, N.S. The basic reproduction number (R0) of measles: A systematic review. Lancet Infect. Dis. 2017, 17, e420–e428. [Google Scholar] [CrossRef]
- Bergmann, M.; Schwertler, S.; Reese, S.; Speck, S.; Truyen, U.; Hartmann, K. Antibody response to feline panleukopenia virus vaccination in healthy adult cats. J. Feline Med. Surg. 2018, 20, 1087–1093. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Category | Total No. | Protective FPV Titre | 95% CI | Χ2-Value | p-Value 1 | |
|---|---|---|---|---|---|---|---|
| No. | % | ||||||
| Group | Perth owned | 117 | 112 | 95.7 | 90.4–96.8 | 11.733 | 0.008 |
| Perth shelter | 124 | 115 | 92.7 | 86.7–96.6 | |||
| Sydney owned | 172 | 156 | 90.7 | 90.9–96.7 | |||
| Sydney shelter | 110 | 110 | 100 | 96.7–100 | |||
| Shelter vs. Owned | Shelter | 234 | 225 | 96. | 92.8–98.2 | 2.798 | 0.094 |
| Owned | 289 | 268 | 92.7 | 89.1–95.5 | |||
| Location | Perth | 241 | 227 | 94.2 | 90.4–96.8 | 0.004 | 0.947 |
| Sydney | 282 | 266 | 94.3 | 90.9–96.7 | |||
| Age | <1 year | 205 | 188 | 91.7 | 87.05–95.1 | 4.154 | 0.125 |
| 1–8 years | 232 | 222 | 95.7 | 92.2–97.9 | |||
| >8 years | 86 | 83 | 96.5 | 90.1–99.3 | |||
| Sex | Male | 241 | 224 | 93 | 89–95.8 | 2.202 | 0.138 |
| Female | 250 | 240 | 96 | 92.8–98.1 | |||
| Desexing Status | Desexed | 275 | 263 | 95.6 | 92.5–97.7 | 0.755 | 0.686 |
| Intact | 195 | 183 | 93.9 | 89.5–96.8 | |||
| Unknown | 19 | 18 | 94.7 | 74.0–99.9 | |||
| Breed | Domestic | 418 | 403 | 96.4 | 94.2–98.0 | 0.087 | 0.087 |
| Non-domestic | 53 | 50 | 94.3 | 84.4–98.9 | |||
| Outdoor Access | Indoors only | 99 | 91 | 91.9 | 84.7–96.5 | 0.788 | 0.375 |
| Outdoor access | 253 | 239 | 94.5 | 90.9–96.9 | |||
| Dogs in the House | No | 97 | 96 | 99.0 | 94.4–100 | 0.519 | 0.471 |
| Yes | 50 | 50 | 100 | 92.9–100 | |||
| Source | Breeder/Pet shop | 51 | 48 | 94.1 | 83.8–98.8 | 4.435 | 0.109 |
| Shelter/Stray | 275 | 259 | 94.2 | 90.7–96.6 | |||
| Other | 108 | 107 | 99.1 | 95.0–100 | |||
| Health Status | Healthy | 417 | 396 | 95.0 | 92.4–96.9 | 0.085 | 0.770 |
| Sick/Injured | 71 | 68 | 95.8 | 88.1–99.1 | |||
| Vaccination Status | Vaccinated | 218 | 217 | 99.5 | 97.5–100 | 17.617 | <0.001 |
| Unvaccinated or Unknown | 305 | 276 | 90.5 | 86.6–93.5 | |||
| Vaccination Type | MLV only | 114 | 113 | 99.1 | 95.2–100 | 0.336 | 0.846 |
| Inactivated only | 18 | 18 | 100 | 81.5–100 | |||
| Both | 20 | 20 | 100 | 83.2–100 | |||
| Time Since Last Vaccination | <6 months | 22 | 21 | 95.5 | 77.16–99.9 | 1.651 | 0.199 |
| 6–12 months | 126 | 126 | 100 | 97.1–100 | |||
| 1–3 years | 38 | 38 | 100 | 90.8–100 | |||
| >3 years | 22 | 22 | 100 | 84.6–100 | |||
| Unknown | 10 | 10 | 100 | ||||
| Medications | No | 446 | 419 | 94.0 | 91.3–96.0 | 0.565 | 0.452 |
| Yes | 77 | 74 | 96.1 | 89.0–99.2 | |||
| FeLV Antigen Status | Negative | 82 | 82 | 100 | 95.6–100 | n/a | n/a |
| Positive | 0 | 0 | |||||
| FIV Antibody Status | Negative | 105 | 104 | 99.1 | 94.8–100 | 0.23 | 0.631 |
| Positive | 24 | 24 | 100 | 85.8–100 | |||
| B | SE | Wald | df | p-Value | OR | 95% CI | |
|---|---|---|---|---|---|---|---|
| Vaccinated | 3.293 | 1.024 | 10.346 | 1 | 0.001 | 29.94 | 3.62–200.4 |
| Shelter-Housed | 0.988 | 0.416 | 5.635 | 1 | 0.018 | 2.685 | 1.19–6.07 |
| Constant | 1.140 | 0.407 | 7.843 | 1 | <0.001 | 3.128 | – |
| B | SE | Wald | df | p-Value | OR | 95% CI | |
|---|---|---|---|---|---|---|---|
| IRSD | 1.780 | 0.629 | 7.995 | 1 | 0.005 | 5.928 | 1.73–20.35 |
| Constant | 2.369 | 0.240 | 97.486 | 1 | 0.000 | 10.684 | – |
| Year of Sampling | Country | No. Cats | Origin of Cats | Proportion Known to Be Vaccinated (%) | FPV Seroprevalence (%) | Reference |
|---|---|---|---|---|---|---|
| 1981 | Australia | 92 | stray/feral | 0 | 79 | [10] |
| 1989 | UK | 45 | free-ranging farm cats | 0 | 96 | [20] |
| 1997 | Vietnam (North) | 69 | unowned | 0 | 54 | [21] |
| 1998 | Vietnam (South) | 50 | unowned | 0 | 44 | [22] |
| 1998–2000 | Saudi Arabia | 13 | feral | 0 | 8 | [23] |
| 2004 | Ecuador | 52 | owned/feral | 0 | 67 | [24] |
| 2005 | USA (Florida) | 61 | feral | 0 | 33 | [25] |
| 2007 | France | 469 | owned/stray | 0 | 25 | [12] |
| 2010 | USA (Florida) | 347 | shelter | 0 | 40 | [9] |
| 2013 | Russia | 60 | owned | 0 | 45 | [26] |
| 2017–2018 | Italy | 151 | stray | 0 | 46 | [13] |
| 1998–2001 | Costa Rica | 97 | owned | 17 | 93 | [27] |
| 2001 | USA (Colorado) | 276 | owned | U | 69 | [3] |
| 2001 | Guatemala | 30 | owned | 27 | 50 | [28] |
| 2003 | USA and Canada | 272 | owned | 100 | 98 | [7] |
| 2011–2012 | Germany | 350 | owned | 81 | 71 | [8] |
| 2012–2014 | Germany | 112 | owned | 64 | 64 | [29] |
| 2016 | Austria | 92 | owned | 100 | 97 | [19] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jenkins, E.; Davis, C.; Carrai, M.; Ward, M.P.; O’Keeffe, S.; van Boeijen, M.; Beveridge, L.; Desario, C.; Buonavoglia, C.; Beatty, J.A.; et al. Feline Parvovirus Seroprevalence Is High in Domestic Cats from Disease Outbreak and Non-Outbreak Regions in Australia. Viruses 2020, 12, 320. https://doi.org/10.3390/v12030320
Jenkins E, Davis C, Carrai M, Ward MP, O’Keeffe S, van Boeijen M, Beveridge L, Desario C, Buonavoglia C, Beatty JA, et al. Feline Parvovirus Seroprevalence Is High in Domestic Cats from Disease Outbreak and Non-Outbreak Regions in Australia. Viruses. 2020; 12(3):320. https://doi.org/10.3390/v12030320
Chicago/Turabian StyleJenkins, Elizabeth, Conor Davis, Maura Carrai, Michael P. Ward, Susan O’Keeffe, Martine van Boeijen, Louise Beveridge, Costantina Desario, Canio Buonavoglia, Julia A. Beatty, and et al. 2020. "Feline Parvovirus Seroprevalence Is High in Domestic Cats from Disease Outbreak and Non-Outbreak Regions in Australia" Viruses 12, no. 3: 320. https://doi.org/10.3390/v12030320
APA StyleJenkins, E., Davis, C., Carrai, M., Ward, M. P., O’Keeffe, S., van Boeijen, M., Beveridge, L., Desario, C., Buonavoglia, C., Beatty, J. A., Decaro, N., & Barrs, V. R. (2020). Feline Parvovirus Seroprevalence Is High in Domestic Cats from Disease Outbreak and Non-Outbreak Regions in Australia. Viruses, 12(3), 320. https://doi.org/10.3390/v12030320