Drug Repositioning: New Approaches and Future Prospects for Life-Debilitating Diseases and the COVID-19 Pandemic Outbreak


Abstract
:1. Introduction
2. Technological Advancements of Drug Repositioning—Current Methods in Research
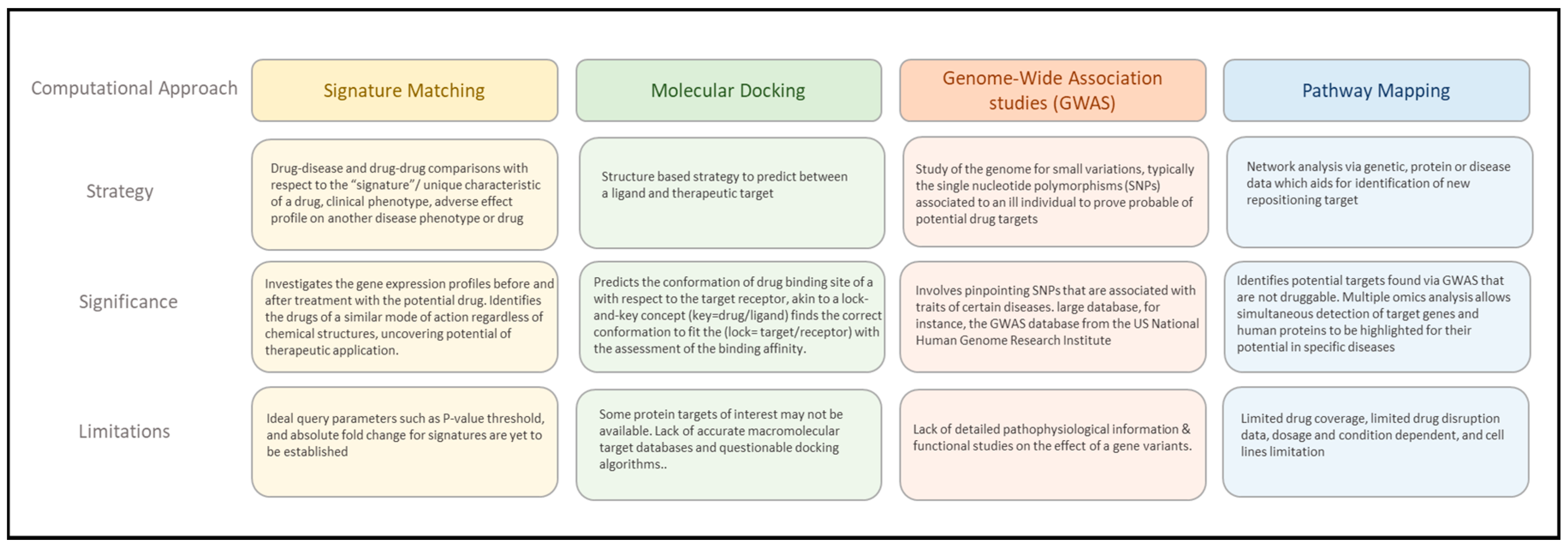
2.1. The Computational Approach to Drug Repositioning
2.1.1. Signature Matching
2.1.2. Molecular Docking
2.1.3. Genome-Wide Association Studies (GWAS)
2.1.4. Pathway Mapping
2.2. Potential Computational Construct to Drug Repositioning
2.3. Artificial Intelligence in Drug Repositioning
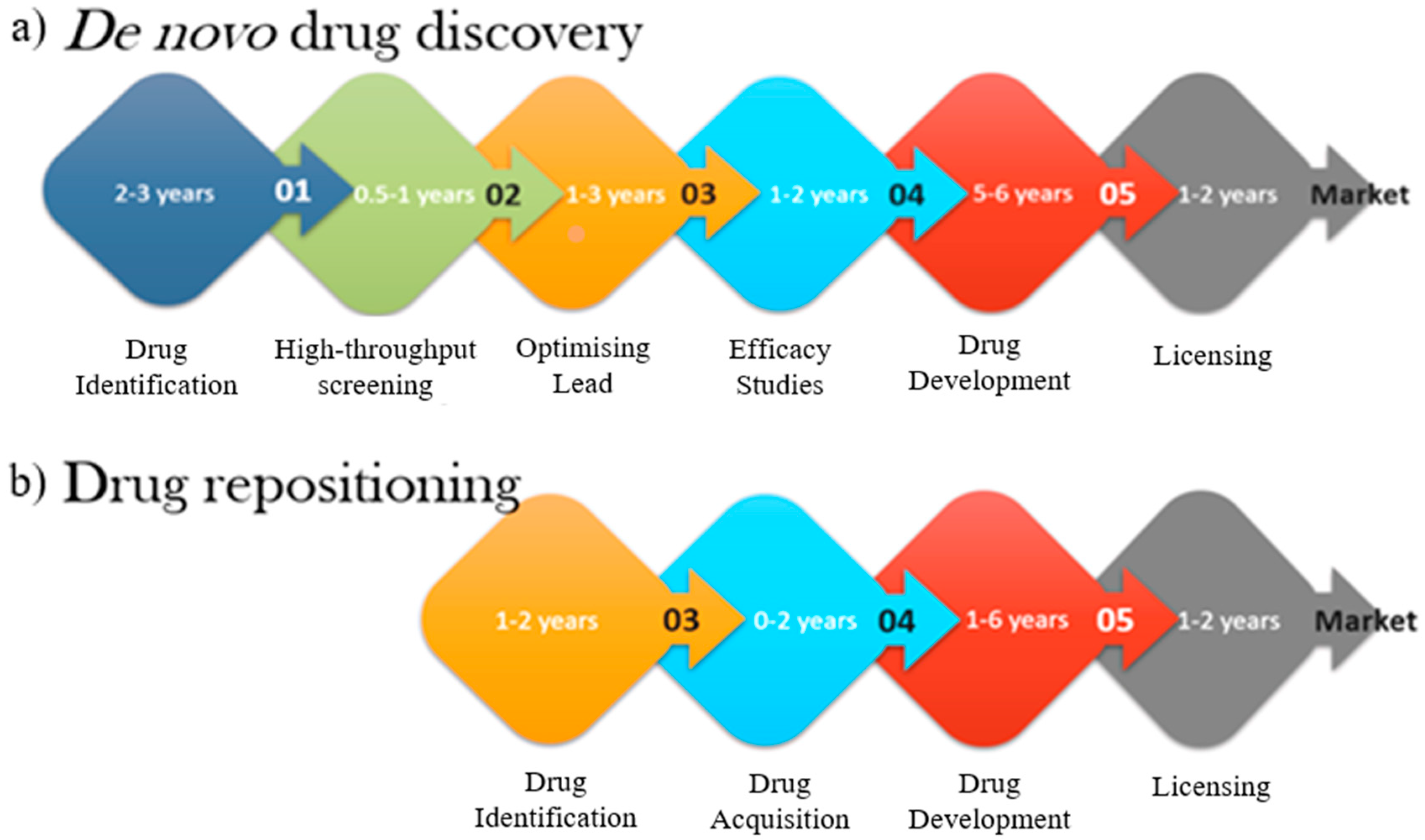
3. Advantages of Drug Repositioning
3.1. Cost and Time Saving
3.2. Accessible Bioinformatics Databases for Drug Candidates
4. Classic Examples of Repositioned Drugs
4.1. Minoxidil, Farewell to Hair Loss
4.2. Sildenafil, New Usage for Erectile Dysfunction
4.3. Duloxetine Repositioned for Stress Urinary Incontinence
4.4. New Hope for Orphan Disease Drug Development
4.4.1. Korlym’s Legacies on Orphan Disease
4.4.2. Everolimus on Rare Tuberous Sclerosis Complex
5. Promising Novel Uses in Drug Repositioning
5.1. Novel Uses of Zidovudine for Viral Diseases
5.2. New Life to almost Extinct Auranofin
6. Future Prospects of Drug Repositioning for COVID-19 Pandemic
Repurposing the Antimalarial Drug Chloroquine for SARS-CoV-2/COVID-19 Treatment
7. Future Prospects of Drug Repositioning
7.1. Path to Drug Personalisation
7.2. Challenges of Drug Repositioning
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Everett, J.R. Academic Drug Discovery: Current Status and Prospects. Expert Opin. Drug Discov. 2015, 10, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Aube, J. Drug Repurposing and the Medicinal Chemist. ACS Med. Chem. Lett. 2012, 3, 442–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, G.; Wong, S. Toward better drug repositioning: Prioritising and integrating existing methods into efficient pipelines. Drug Discov. Today 2014, 19, 637–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, H.; Li, J.; Xie, H.; Wang, Y. Review of drug repositioning approaches and resources. Int. J. Biol. Sci. 2018, 14, 1232–1244. [Google Scholar] [CrossRef] [Green Version]
- Ashburn, T.; Thor, K. Drug repositioning: Identifying and developing new uses for existing drugs. Nat. Rev. Drug Discov. 2004, 3, 673–683. [Google Scholar] [CrossRef]
- Uthman, B. Extended-release Antiepilepsy Drugs—Review of the Effects of Once-daily Dosing on Tolerability, Effectiveness, Adherence, Quality of Life, and Patient Preference. US Neurol. 2014, 10, 30. [Google Scholar] [CrossRef]
- Pelham, W.; Gnagy, E.; Burrows-Maclean, L.; Williams, A.; Fabiano, G.; Morrisey, S.; Chronis, A.; Forehand, G.; Nguyen, C.; Hoffman, M.; et al. Once-a-Day Concerta Methylphenidate Versus Three-Times-Daily Methylphenidate in Laboratory and Natural Settings. Pediatrics 2001, 107, e105. [Google Scholar] [CrossRef] [Green Version]
- Vora, P.; Somani, R.; Jain, M. Drug Repositioning: An Approach for Drug Discovery. Mini-Rev. Org. Chem. 2016, 13, 363–376. [Google Scholar] [CrossRef]
- Oprea, T.; Bauman, J.; Bologa, C.; Buranda, T.; Chigaev, A.; Edwards, B.; Jarvik, J.; Gresham, H.; Haynes, M.; Hjelle, B.; et al. Drug repurposing from an academic perspective. Drug Discov. Today: Ther. Strateg. 2011, 8, 61–69. [Google Scholar] [CrossRef] [Green Version]
- Chong, C.; Sullivan, D. New uses for old drugs. Nature 2007, 448, 645–646. [Google Scholar] [CrossRef]
- Pushpakom, S.; Iorio, F.; Eyers, P.; Escott, K.; Hopper, S.; Wells, A.; Doig, A.; Guilliams, T.; Latimer, J.; McNamee, C.; et al. Drug repurposing: Progress, challenges and recommendations. Nat. Rev. Drug Discov. 2018, 18, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Scialli, A. Thalidomide: The Tragedy of Birth Defects and the Effective Treatment of Disease. Toxicol. Sci. 2011, 122, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudley, J.; Deshpande, T.; Butte, A. Exploiting drug-disease relationships for computational drug repositioning. Brief. Bioinform. 2011, 12, 303–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gautret, P.; Lagier, J.; Parola, P.; Hoang, V.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomised clinical trial. Int. J. Antimicrob. Agents 2020, 105949. [Google Scholar] [CrossRef] [PubMed]
- Sleigh, S.; Barton, C. Repurposing Strategies for Therapeutics. Pharm. Med. 2010, 24, 151–159. [Google Scholar] [CrossRef]
- Keiser, M.; Setola, V.; Irwin, J.; Laggner, C.; Abbas, A.; Hufeisen, S.; Jensen, N.; Kuijer, M.; Matos, R.; Tran, T.; et al. Predicting new molecular targets for known drugs. Nature 2009, 462, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Le, B.; Iwatani, S.; Wong, R.; Stevenson, D.; Sirota, M. Computational discovery of therapeutic candidates for preventing preterm birth. JCI Insight 2020, 5. [Google Scholar] [CrossRef]
- Wei, G.; Twomey, D.; Lamb, J.; Schlis, K.; Agarwal, J.; Stam, R.; Opferman, J.; Sallan, S.; den Boer, M.; Pieters, R.; et al. Gene expression-based chemical genomics identifies Rapamycin as a modulator of MCL1 and glucocorticoid resistance. Cancer Cell 2006, 10, 331–342. [Google Scholar] [CrossRef] [Green Version]
- Brown, A.; Patel, C. MeSHDD: Literature-based drug-drug similarity for drug repositioning. J. Am. Med. Inform. Assoc. 2016, 24, 614–618. [Google Scholar] [CrossRef]
- Chan, J.; Wang, X.; Turner, J.; Baldwin, N.; Gu, J. Breaking the paradigm: Dr Insight empowers signature-free, enhanced drug repurposing. Bioinformatics 2019, 35, 2818–2826. [Google Scholar] [CrossRef] [Green Version]
- Meng, X.; Zhang, H.; Mezei, M.; Cui, M. Molecular Docking: A Powerful Approach for Structure-Based Drug Discovery. Curr. Comput. Aided-Drug Des. 2011, 7, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Dakshanamurthy, S.; Issa, N.; Assefnia, S.; Seshasayee, A.; Peters, O.; Madhavan, S.; Uren, A.; Brown, M.; Byers, S. Predicting New Indications for Approved Drugs Using a Proteochemometric Method. J. Med. Chem. 2012, 55, 6832–6848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, Y.; Tian, T.; Huang, S.; Wan, F.; Li, J.; Li, S.; Yang, H.; Hong, L.; Wu, N.; Yuan, E.; et al. A data-driven drug repositioning framework discovered a potential therapeutic agent targeting COVID-19. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Sanseau, P.; Agarwal, P.; Barnes, M.; Pastinen, T.; Richards, J.; Cardon, L.; Mooser, V. Use of genome-wide association studies for drug repositioning. Nat. Biotechnol. 2012, 30, 317–320. [Google Scholar] [CrossRef]
- Grover, M.; Ballouz, S.; Mohanasundaram, K.; George, R.; Goscinski, A.; Crowley, T.; Sherman, C.; Wouters, M. Novel therapeutics for coronary artery disease from genome-wide association study data. BMC Med. Genom. 2015, 8. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.; Dampier, W.; Tozeren, A.; Brown, J.; Magid-Slav, M. Identification of Common Biological Pathways and Drug Targets Across Multiple Respiratory Viruses Based on Human Host Gene Expression Analysis. PLoS ONE 2012, 7, e33174. [Google Scholar] [CrossRef]
- Amemiya, T.; Gromiha, M.; Horimoto, K.; Fukui, K. Drug repositioning for dengue haemorrhagic fever by integrating multiple omics analyses. Sci. Rep. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Wei, G.; Gao, L.; Tang, Z.; Lin, P.; Liang, L.; Zeng, J.; Chen, G.; Zhang, L. Drug repositioning in head and neck squamous cell carcinoma: An integrated pathway analysis based on connectivity map and differential gene expression. Pathol. Res. Pract. 2019, 215, 152378. [Google Scholar] [CrossRef]
- Samarpita, S.; Kim, J.; Rasool, M.; Kim, K. Investigation of toll-like receptor (TLR) 4 inhibitor TAK-242 as a new potential anti-rheumatoid arthritis drug. Arthritis Res. Ther. 2020, 22. [Google Scholar] [CrossRef] [Green Version]
- Qu, X.; Rajpal, D. Applications of Connectivity Map in drug discovery and development. Drug Discov. Today 2012, 17, 1289–1298. [Google Scholar] [CrossRef]
- Wang, R.; Li, S.; Cheng, L.; Wong, M.; Leung, K. Predicting associations among drugs, targets and diseases by tensor decomposition for drug repositioning. BMC Bioinform. 2019, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, Y.; Li, H.; Gao, L.; Lin, H.; Kung, H.; Lin, M.; Leung, K.; Wong, M.; Xiong, W.; Li, L. Old drug, new indication: Olsalazine sodium reduced serum uric acid levels in mice via inhibiting xanthine oxidoreductase activity. J. Pharmacol. Sci. 2017, 135, 114–120. [Google Scholar] [CrossRef]
- Wang, L.; Ding, J.; Pan, L.; Cao, D.; Jiang, H.; Ding, X. Artificial intelligence facilitates drug design in the big data era. Chemom. Intell. Lab. Syst. 2019, 194, 103850. [Google Scholar] [CrossRef]
- Napolitano, F.; Zhao, Y.; Moreira, V.; Tagliaferri, R.; Kere, J.; D’Amato, M.; Greco, D. Drug repositioning: A machine-learning approach through data integration. J. Cheminform. 2013, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanhaelen, Q.; Mamoshina, P.; Aliper, A.; Artemov, A.; Lezhnina, K.; Ozerov, I.; Labat, I.; Zhavoronkov, A. Design of efficient computational workflows for in silico drug repurposing. Drug Discov. Today 2017, 22, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Sheridan, R.; Liaw, A.; Dahl, G.; Svetnik, V. Deep Neural Nets as a Method for Quantitative Structure–Activity Relationships. J. Chem. Inf. Model. 2015, 55, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Spaulding, A.; Rutherford, G.; Siegfried, N. Stavudine or Zidovudine in three-drug combination therapy for initial treatment of HIV infection in antiretroviral-naïve individuals. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Wen, M.; Zhang, Z.; Niu, S.; Sha, H.; Yang, R.; Yun, Y.; Lu, H. Deep-Learning-Based Drug–Target Interaction Prediction. J. Proteome Res. 2017, 16, 1401–1409. [Google Scholar] [CrossRef]
- Richardson, P.; Griffin, I.; Tucker, C.; Smith, D.; Oechsle, O.; Phelan, A.; Stebbing, J. Baricitinib as potential treatment for 2019-nCoV acute respiratory disease. Lancet 2020, 395, e30–e31. [Google Scholar] [CrossRef] [Green Version]
- Velavan, T.; Meyer, C. The COVID-19 epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, Y.; Hara, H. Editorial: Drug Repositioning: Current Advances and Future Perspectives. Front. Pharmacol. 2018, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullard, A. 2013 FDA drug approvals. Nat. Rev. Drug Discov. 2014, 13, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Scannell, J.; Blanckley, A.; Boldon, H.; Warrington, B. Diagnosing the decline in pharmaceutical R&D efficiency. Nat. Rev. Drug Discov. 2012, 11, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V. Drug Repositioning: A Faster Path to Drug Discovery. Adv. Pharmacoepidemiol. Drug Saf. 2012, 01. [Google Scholar] [CrossRef] [Green Version]
- Strittmatter, S. Overcoming Drug Development Bottlenecks with Repurposing: Old drugs learn new tricks. Nat. Med. 2014, 20, 590–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ursu, O.; Holmes, J.; Knockel, J.; Bologa, C.; Yang, J.; Mathias, S.; Nelson, S.; Oprea, T. DrugCentral: Online drug compendium. Nucleic Acids Res. 2016, 45, D932–D939. [Google Scholar] [CrossRef]
- Bertolini, F.; Sukhatme, V.; Bouche, G. Drug repurposing in oncology—patient and health systems opportunities. Nat. Rev. Clin. Oncol. 2015, 12, 732–742. [Google Scholar] [CrossRef]
- Andronis, C.; Sharma, A.; Virvilis, V.; Deftereos, S.; Persidis, A. Literature mining, ontologies and information visualisation for drug repurposing. Brief. Bioinform. 2011, 12, 357–368. [Google Scholar] [CrossRef] [Green Version]
- Devine, B.; Fife, R.; Trust, P. Minoxidil for severe hypertension after failure of other hypotensive drugs. BMJ 1977, 2, 667–669. [Google Scholar] [CrossRef] [Green Version]
- Ishida, J.; Konishi, M.; Ebner, N.; Springer, J. Repurposing of approved cardiovascular drugs. J. Transl. Med. 2016, 14, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Camacho-Martínez, F. Hair Loss in Women. Semin. Cutan. Med. Surg. 2009, 28, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Epstein, E. Topical minoxidil therapy for androgenetic alopecia. Arch. Derm. 1988, 124, 322–323. [Google Scholar] [CrossRef]
- Messenger, A.; Rundegren, J. Minoxidil: Mechanisms of action on hair growth. Br. J. Dermatol. 2004, 150, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Rogers, N.; Avram, M. Medical treatments for male and female pattern hair loss. J. Am. Acad. Dermatol. 2008, 59, 547–566. [Google Scholar] [CrossRef] [PubMed]
- Renaud, R.; Xuereb, H. Erectile-dysfunction therapies. Nat. Rev. Drug Discov. 2002, 1, 663–664. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.; Lu, Y.; Detke, M.; Hudson, J.; Iyengar, S.; Demitrack, M. Effects of Duloxetine on Painful Physical Symptoms Associated With Depression. Psychosomatics 2004, 45, 17–28. [Google Scholar] [CrossRef]
- Doan, T.; Pollastri, M.; Walters, M.; Georg, G. The Future of Drug Repositioning. Annu. Rep. Med. Chem. 2011, 46, 385–401. [Google Scholar] [CrossRef]
- Smith, H.S.; Smith, E.J.; Smith, B.R. Duloxetine in the management of chronic musculoskeletal pain. Ther. Clin. Risk Manag. 2012, 8, 267. [Google Scholar] [CrossRef] [Green Version]
- Dunoyer, M. Accelerating access to treatments for rare diseases. Nat. Rev. Drug Discov. 2011, 10, 475–476. [Google Scholar] [CrossRef]
- Muthyala, R. Orphan/rare drug discovery through drug repositioning. Drug Discov. Today: Ther. Strateg. 2011, 8, 71–76. [Google Scholar] [CrossRef]
- Sardana, D.; Zhu, C.; Zhang, M.; Gudivada, R.; Yang, L.; Jegga, A. Drug repositioning for orphan diseases. Brief. Bioinform. 2011, 12, 346–356. [Google Scholar] [CrossRef] [Green Version]
- Wastfelt, M.; Fadeel, B.; Henter, J. A journey of hope: Lessons learned from studies on rare diseases and orphan drugs. J. Int. Med. 2006, 260, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Cote, T. Database identifies FDA-approved drugs with potential to be repurposed for treatment of orphan diseases. Brief. Bioinform. 2011, 12, 341–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, W.; Sanderson, P.; Zheng, W. Drug combination therapy increases successful drug repositioning. Drug Discov. Today 2016, 21, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, H.; Yamada, S. Cushing’s’s Disease. J. Clin. Med. 2019, 8, 1951. [Google Scholar] [CrossRef] [Green Version]
- Terzolo, M.; Iacuaniello, D.; Pia, A.; Adriano, P.; Moraitis, A.; Pivonello, R. SUN-463 Tumor Shrinkage with Preoperative Relacorilant Therapy in Two Patients with Cushing’s Disease Due to Pituitary Macroadenomas. J. Endocr. Soc. 2019, 3. [Google Scholar] [CrossRef]
- Mollica, V.; Di Nunno, V.; Cimadamore, A.; Lopez-Beltran, A.; Cheng, L.; Santoni, M.; Scarpelli, M.; Montironi, R.; Massari, F. Molecular Mechanisms Related to Hormone Inhibition Resistance in Prostate Cancer. Cells 2019, 8, 43. [Google Scholar] [CrossRef] [Green Version]
- Tejman-Yarden, N.; Miyamoto, Y.; Leitsch, D.; Santini, J.; Debnath, A.; Gut, J.; McKerrow, J.; Reed, S.; Eckmann, L. A Reprofiled Drug, Auranofin, Is Effective against Metronidazole-Resistant Giardia lamblia. Antimicrob. Agents Chemother. 2013, 57, 2029–2035. [Google Scholar] [CrossRef] [Green Version]
- Curatolo, P.; Bombardieri, R.; Jozwiak, S. Tuberous sclerosis. Lancet 2008, 372, 657–668. [Google Scholar] [CrossRef]
- Osborne, J.; Fryer, A.; Webb, D. Epidemiology of Tuberous Sclerosis. Ann. N. Y. Acad. Sci. 1991, 615, 125–127. [Google Scholar] [CrossRef]
- Bissler, J.; Kingswood, J.; Radzikowska, E.; Zonnenberg, B.; Belousova, E.; Frost, M.; Sauter, M.; Brakemeier, S.; de Vries, P.; Berkowitz, N.; et al. Everolimus long-term use in patients with tuberous sclerosis complex: Four-year update of the EXIST-2 study. PLoS ONE 2017, 12, e0180939. [Google Scholar] [CrossRef] [PubMed]
- Franz, D.; Capal, J. Profile of Everolimus in the treatment of tuberous sclerosis complex: An evidence-based review of its place in therapy. Neuropsychiatr. Dis. Treat. 2016, 12, 2165–2172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, J.; Liu, J. Recent Advances in Drug Repositioning for the Discovery of New Anticancer Drugs. Int. J. Biol. Sci. 2014, 10, 654–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arts, E.; Hazuda, D. HIV-1 Antiretroviral Drug Therapy. Cold Spring Harb. Perspect. Med. 2012, 2, a007161. [Google Scholar] [CrossRef] [PubMed]
- Clouser, C.; Patterson, S.; Mansky, L. Exploiting Drug Repositioning for Discovery of a Novel HIV Combination Therapy. J. Virol. 2010, 84, 9301–9309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostertag, W.; Roesler, G.; Krieg, C.; Kind, J.; Cole, T.; Crozier, T.; Gaedicke, G.; Steinheider, G.; Kluge, N.; Dube, S. Induction of Endogenous Virus and of Thymidine Kinase by Bromodeoxyuridine in Cell Cultures Transformed by Friend Virus. Proc. Natl. Acad. Sci. USA 1974, 71, 4980–4985. [Google Scholar] [CrossRef] [Green Version]
- Yamani, L.; Yano, Y.; Utsumi, T.; Wasityastuti, W.; Rinonce, H.; Widasari, D.; Juniastuti; Lusida, M.; Soetjipto; Hayashi, Y. Profile of Mutations in the Reverse Transcriptase and Overlapping Surface Genes of Hepatitis B Virus (HBV) in Treatment-Naïve Indonesian HBV Carriers. Jpn. J. Infect. Dis. 2017, 70, 647–655. [Google Scholar] [CrossRef] [Green Version]
- Yunusa, A.; Bello, S.; Chika, A.; Yakubu, A. An antiviral drug combinational studies against HIV-A computational drug repositioning approach. Asian J. Sci. Technol. 2019, 10, 9978–9984. [Google Scholar]
- Lewis, M.; DaFonseca, S.; Chomont, N.; Palamara, A.; Tardugno, M.; Mai, A.; Collins, M.; Wagner, W.; Yalley-Ogunro, J.; Greenhouse, J.; et al. Gold drug auranofin restricts the viral reservoir in the monkey AIDS model and induces containment of viral load following ART suspension. AIDS 2011, 25, 1347–1356. [Google Scholar] [CrossRef]
- Goenka, S.; Simon, S. Organogold drug Auranofin exhibits anti-melanogenic activity in B16F10 and MNT-1 melanoma cells. Arch. Dermatol. Res. 2019, 312, 213–221. [Google Scholar] [CrossRef]
- Shaw, A.; Yasothan, U.; Kirkpatrick, P. Crizotinib. Nat. Rev. Drug Discov. 2011, 10, 897–898. [Google Scholar] [CrossRef] [PubMed]
- Worldometers Coronavirus Update. Available online: https://www.worldometers.info/coronavirus/ (accessed on 1 August 2020).
- Wire, B. China’s Institute of Materia Medica Partners With Cyclica on Innovative Drug Repurposing for COVID-19. Available online: https://www.businesswire.com/news/home/20200305005764/en/China%E2%80%99s-Institute-Materia-Medica-Partners-Cyclica-Innovative (accessed on 20 March 2020).
- Khailany, R.; Safdar, M.; Ozaslan, M. Genomic characterisation of a novel SARS-CoV-2. Gene Rep. 2020, 19, 1–7. [Google Scholar] [CrossRef]
- Wang, H.; Li, X.; Li, T.; Zhang, S.; Wang, L.; Wu, X.; Liu, J. The genetic sequence, origin, and diagnosis of SARS-CoV-2. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 1, 1–7. [Google Scholar] [CrossRef]
- Times, N.S. Thailand Sees Apparent Success Treating Coronavirus with HIV Drug | New Straits Times. Available online: https://www.nst.com.my/world/world/2020/02/562079/thailand-sees-apparent-success-treating-coronavirus-hiv-drug (accessed on 6 March 2020).
- Liu, J.; Cao, R.; Xu, M.; Wang, X.; Zhang, H.; Hu, H.; Li, Y.; Hu, Z.; Zhong, W.; Wang, M. Hydroxychloroquine, a less toxic derivative of Chloroquine, is effective in inhibiting SARS-CoV-2 infection In Vitro. Cell Discov. 2020, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, C. Coronavirus puts drug repurposing on the fast track. Nat. Biotechnol. 2020, 38, 379–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Zhang, Y.; Huang, J.; Yin, P.; Cheng, Z.; Wu, J.; Chen, S.; Zhang, Y.; Chen, B.; Lu, M.; et al. Favipiravir versus Arbidol for COVID-19: A Randomised Clinical Trial. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Caly, L.; Druce, J.; Catton, M.; Jans, D.; Wagstaff, K. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 In Vitro. Antivir. Res. 2020, 178, 104787. [Google Scholar] [CrossRef]
- Wang, J. Fast Identification of Possible Drug Treatment of Coronavirus Disease-19 (COVID-19) through Computational Drug Repurposing Study. J. Chem. Inf. Model. 2020. [Google Scholar] [CrossRef]
- Wu, C.; Liu, Y.; Yang, Y.; Zhang, P.; Zhong, W.; Wang, Y.; Wang, Q.; Xu, Y.; Li, M.; Li, X.; et al. Analysis of therapeutic targets for SARS-CoV-2 and discovery of potential drugs by computational methods. Acta Pharm. Sin. B 2020. [Google Scholar] [CrossRef]
- Elfiky, A. Ribavirin, Remdesivir, Sofosbuvir, Galidesivir, and Tenofovir against SARS-CoV-2 RNA dependent RNA polymerase (RdRp): A molecular docking study. Life Sci. 2020, 253, 117592. [Google Scholar] [CrossRef]
- Biot, C.; Daher, W.; Chavain, N.; Fandeur, T.; Khalife, J.; Dive, D.; De Clercq, E. Design and Synthesis of Hydroxyferroquine Derivatives with Antimalarial and Antiviral Activities. J. Med. Chem. 2006, 49, 2845–2849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Yu, K.; Kim, Y.; Kim, S.; Kim, E.; Kim, S.; Kim, E.; Casel, M.; Rollon, R.; Jang, S.; et al. Antiviral Efficacies of FDA-Approved Drugs against SARS-CoV-2 Infection in Ferrets. mBio 2020, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Slater, A. Chloroquine: Mechanism of drug action and resistance in plasmodium falciparum. Pharmacol. Ther. 1993, 57, 203–235. [Google Scholar] [CrossRef]
- Sullivan, D.; Gluzman, I.; Russell, D.; Goldberg, D. On the molecular mechanism of Chloroquine’s antimalarial action. Proc. Natl. Acad. Sci. USA 1996, 93, 11865–11870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, M.; Bergeron, E.; Benjannet, S.; Erickson, B.; Rollin, P.; Ksiazek, T.; Seidah, N.; Nichol, S. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virol. J. 2005, 2, 69. [Google Scholar] [CrossRef] [Green Version]
- Helal, G.; Gad, M.; Abd-Ellah, M.; Eid, M. Hydroxychloroquine augments early virological response to pegylated interferon plus ribavirin in genotype-4 chronic hepatitis C patients. J. Med. Virol. 2016, 88, 2170–2178. [Google Scholar] [CrossRef]
- Yao, X.; Ye, F.; Zhang, M.; Cui, C.; Huang, B.; Niu, P.; Liu, X.; Zhao, L.; Dong, E.; Song, C.; et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Frie, K.; Gbinigie, K. Chloroquine and Hydroxychloroquine: Current Evidence for Their Effectiveness in Treating COVID-19. Available online: https://www.cebm.net/covid-19/chloroquine-and-hydroxychloroquine-current-evidence-for-their-effectiveness-in-treating-covid-19/ (accessed on 6 March 2020).
- Savarino, A.; Boelaert, J.; Cassone, A.; Majori, G.; Cauda, R. Effects of Chloroquine on viral infections: An old drug against today’s diseases. Lancet Infect. Dis. 2003, 3, 722–727. [Google Scholar] [CrossRef]
- Du, Y.; Chen, X. Favipiravir: Pharmacokinetics and Concerns about Clinical Trials for 2019-nCoV Infection. Clin. Pharmacol. Ther. 2020. [Google Scholar] [CrossRef] [Green Version]
- Momekov, G.; Momekova, D. Ivermectin as a potential COVID-19 treatment from the pharmacokinetic point of view. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Amirian, E.; Levy, J. Current knowledge about the antivirals remdesivir (GS-5734) and GS-441524 as therapeutic options for coronaviruses. One Health 2020, 9, 100128. [Google Scholar] [CrossRef] [PubMed]
- Eastman, R.; Roth, J.; Brimacombe, K.; Simeonov, A.; Shen, M.; Patnaik, S.; Hall, M. Remdesivir: A Review of Its Discovery and Development Leading to Emergency Use Authorization for Treatment of COVID-19. ACS Cent. Sci. 2020. [Google Scholar] [CrossRef]
- Ferner, R.; Aronson, J. Remdesivir in Covid-19. BMJ 2020, m1610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drugs. com. Baricitinib Side Effects: Common, Severe, Long Term—Drugs. com. Available online: https://www.drugs.com/sfx/baricitinib-side-effects.html#moreResources (accessed on 6 March 2020).
- Amir-Aslani, A.; Mangematin, V. The future of drug discovery and development: Shifting emphasis towards personalised medicine. Technol. Forecast. Soc. Chang. 2010, 77, 203–217. [Google Scholar] [CrossRef]
- Janku, F.; Stewart, D.; Kurzrock, R. Targeted therapy in non-small-cell lung cancer—Is it becoming a reality? Nat. Rev. Clin. Oncol. 2010, 7, 401–414. [Google Scholar] [CrossRef]
- Drilon, A.; Camidge, D.; Ou, S.; Clark, J.; Socinski, M.; Weiss, J.; Riely, G.; Winter, M.; Wang, S.; Monti, K.; et al. Efficacy and safety of crizotinib in patients (pts) with advanced MET exon 14-altered non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2016, 34, 108. [Google Scholar] [CrossRef]
- Novac, N. Challenges and opportunities of drug repositioning. Trends Pharmacol. Sci. 2013, 34, 267–272. [Google Scholar] [CrossRef]
- Sternitzke, C. Drug repurposing and the prior art patents of competitors. Drug Discov. Today 2014, 19, 1841–1847. [Google Scholar] [CrossRef]
- Stewart, A. How Thalidomide Works Against Cancer. Science 2014, 343, 256–257. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Oh, S. Novel Systemic Therapies for Advanced Gastric Cancer. J. Gastric Cancer 2018, 18, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Drug | Original Medication | Repositioned Medication | References |
|---|---|---|---|
| Auranofin | Rheumatoid arthritis | Metronidazole resistant Giardiasis | [68] |
| Crizotinib | Anaplastic large-cell lymphoma | Non-small-cell lung cancer (NSCLC) | [81] |
| Duloxetine | Major depressive disorder | Stress Urinary Incontinence (SUI) | [5] |
| Everolimus | Prevent solid organ transplant rejection, Augment anticancer treatment regimens, Prevent neovascularisation of artificial cardiac stents | Tuberous sclerosis complex [22] | [72] |
| Korlym | Abortion | Cushing’s Syndrome | [66] |
| Minoxidil | Hypertension | Androgenic alopecia (Hair loss) | [51] |
| Sildenafil | Angina, chest pain/discomfort | Erectile Dysfunction | [55] |
| Thalidomide | Morning sickness pregnant women | Multiple myelomas | [13] |
| Zidovudine | Anticancer agent | Antiretroviral agent-HIV | [75] |
| Drug | Initial Purpose | Side-Effects in COVID-19 Patients | Potential Therapeutic Mode of Action for SARS-CoV-2 | Clinical Trials for COVID-19 | Reference |
|---|---|---|---|---|---|
| Chloroquine/Hydroxychloroquine | Antimalarial medication |
| Impairs replication of virus by interfering with endosome-mediated viral entry or other pH-dependent viral replication steps | Currently ongoing | [101,102] |
| Favipiravir | Broad-spectrum inhibitor of viral RNA, i.e., Influenza |
| Inhibits viral RbRp in the genome replication process | currently ongoing | [23,89,103] |
| Ivermectin | Broad-spectrum anti-parasitic agent | Not reported for COVID-19. Predicted as:
| Nuclear transport inhibitory activity of viral proteins | In vitro studies | [90,104] |
| Remdesivir | Antiviral activity against RNA viruses, i.e., Ebola virus |
| Acts as RbRp inhibitor to target viral genome replication process | Currently ongoing | [105,106,107] |
| Baricitinib | An orally bioavailable inhibitor of Janus kinases 1 and 2 (JAK1/2), with potential anti-inflammatory, immunomodulating and antineoplastic activities. Typically used to treat autoimmune disorders such as rheumatoid arthritis. | Not reported for COVID-19. Previous original indication.
| A high-affinity NAK inhibitor, especially on AP2-associated protein kinase 1 (AAK1), a pivotal regulator of clathrin-mediated endocytosis involved in viral entry at the lungs | Currently ongoing | [39,108] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Low, Z.Y.; Farouk, I.A.; Lal, S.K. Drug Repositioning: New Approaches and Future Prospects for Life-Debilitating Diseases and the COVID-19 Pandemic Outbreak. Viruses 2020, 12, 1058. https://doi.org/10.3390/v12091058
Low ZY, Farouk IA, Lal SK. Drug Repositioning: New Approaches and Future Prospects for Life-Debilitating Diseases and the COVID-19 Pandemic Outbreak. Viruses. 2020; 12(9):1058. https://doi.org/10.3390/v12091058
Chicago/Turabian StyleLow, Zheng Yao, Isra Ahmad Farouk, and Sunil Kumar Lal. 2020. "Drug Repositioning: New Approaches and Future Prospects for Life-Debilitating Diseases and the COVID-19 Pandemic Outbreak" Viruses 12, no. 9: 1058. https://doi.org/10.3390/v12091058
APA StyleLow, Z. Y., Farouk, I. A., & Lal, S. K. (2020). Drug Repositioning: New Approaches and Future Prospects for Life-Debilitating Diseases and the COVID-19 Pandemic Outbreak. Viruses, 12(9), 1058. https://doi.org/10.3390/v12091058