
Measles in Vaccinated People: Epidemiology and Challenges in Surveillance and Diagnosis in the Post-Elimination Phase. Spain, 2014–2020

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Definition
2.2. Variables
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO-Europe. In Proceedings of the Eighth Meeting of The European Regional Verification Commission for Measles and Rubella Elimination (RVC), Warsaw, Poland, 12–14 June 2019. Available online: https://www.euro.who.int/__data/assets/pdf_file/0019/413236/8th-RVC-Report.pdf (accessed on 25 June 2021).
- Centro Nacional de Epidemiología. Instituto de Salud Carlos III y Red Nacional de Vigilancia Epidemiológica. Plan de Eliminación del Sarampión y de la Rubéola en España. Resultados de La Vigilancia. Informes Anual 2019. 2020. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/archivos%20A-Z/Sarampi%C3%B3n/Informe_anual_SAR_RUB_2019_VF_Rev.pdf (accessed on 25 June 2021).
- Masa-Calles, J.; López-Perea, N.; Godoy, P. Perfil epidemiológico del sarampión en España: Casos en adultos, secundarios a la importación y asociados con la asistencia sanitaria. Med. Fam. Semer. 2020, 46, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Arima, Y.; Oishi, K. Letter to the editor: Measles cases among fully vaccinated persons. Eurosurveillance 2018, 23, 1800449. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, M.; Brown, K. The public health implications of secondary measles vaccine failure. J. Prim. Health Care 2013, 5, 92. [Google Scholar] [CrossRef] [PubMed]
- Cheng, V.C.C.; MNurs, S.-C.W.; Chen, J.H.K.; Yip, C.C.Y.; Tsang, O.T.Y. Measles outbreak from Hong Kong International Airport to the hospital due to secondary vaccine failure in healthcare workers. Infect. Control Hosp. Epidemiol. 2019, 40, 1407–1415. [Google Scholar] [CrossRef] [PubMed]
- Cherry, J.D.; Zahn, M. Clinical Characteristics of Measles in Previously Vaccinated and Unvaccinated Patients in California. Clin. Infect. Dis. 2018, 67, 1315–1319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hickman, C.J.; Hyde, T.B.; Sowers, S.B.; Mercader, S.; McGrew, M.; Williams, N.J.; Beeler, J.A.; Audet, S.; Kiehl, B.; Nandy, R.; et al. Laboratory characterization of measles virus infection in previously vaccinated and unvaccinated individuals. J. Infect. Dis. 2011, 204 (Suppl. 1), S549–S558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masa-Calles, J. ¿Vuelve el sarampión? Med. Clín. 2019, 152, 350–352. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention (CDC). Frequently Asked Questions about measles in the US Atalanta: CDC. National Center fo Inmunizaion and Respiratory Diseases, Division of Viral diseases. Available online: https://www.cdc.gov/measles/about/faqs.html (accessed on 28 June 2021).
- Risco-Risco, C.; Masa-Calles, J.; López-Perea, N.; Echevarría, J.E.; Rodríguez-Caravaca, G. Epidemiology of measles in vaccinated people, Spain 2003–2014. Enferm. Infecc. Microbiol. Clin. (Engl. Ed.) 2017, 35, 569–573. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Manual for the Laboratory-based Surveillance of Measles, Rubella, and Congenital Rubella Syndrome. Published online 2018. Available online: https://cdn.who.int/media/docs/default-source/immunization/vpd_surveillance/lab_networks/measles_rubella/manual/chapter-8.pdf?sfvrsn=207dc784_2&download=true (accessed on 28 June 2021).
- Paunio, M.; Peltola, H.; Valle, M.; Davidkin, I.; Virtanen, M.; Heinonen, O.P. Explosive school-based measles outbreak: Intense exposure may have resulted in high risk, even among revaccinees. Am. J. Epidemiol. 1998, 148, 1103–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, R.S.; Duque, M.P.; Almeida, S.; Cruz1, I.; Sottomayor, A.; Almeida, I.; Oliveira, J.R.; Antunes, D. Measles outbreak in a tertiary level hospital, Porto, Portugal, 2018: Challenges in the post-elimination era. EuroSurveillance 2018, 23, 18–00224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torner, N.; Ferràs, J.; Curto, L.; Rebull, J.; Sold, J.; Costae, J.; Mosquera, M.M.; Izquierdo, C.; Martínez, A.; Jané, M. Measles outbreak related to healthcare transmission. Vacunas 2021, 22, 20–27. [Google Scholar] [CrossRef]
- Augusto, G.F.; Cruz, D.; Silva, A.; Pereira, N.; Aguiar, B.; Leça, A.; Serrada, E.; Valente, P.; Fernandes, T.; Guerra, F.; et al. Challenging measles case definition: Three measles outbreaks in three Health Regions of Portugal, February to April 2018. EuroSurveillance 2018, 23, 1800328. [Google Scholar] [CrossRef] [Green Version]
- Hahné, S.J.M.; Nic Lochlainn, L.M.; van Burgel, N.D.; Kerkhof, J.; Sane, S.; Bing Yap, K.; van Binnendijk, R.S. Measles Outbreak Among Previously Immunized Healthcare Workers, the Netherlands, 2014. J. Infect. Dis. 2016, 214, 1980–1986. [Google Scholar] [CrossRef] [PubMed]
- Rosen, J.B.; Rota, J.S.; Hickman, C.J.; Sowers, S.B.; Mercader, S.; Rota, P.A.; Bellini, W.J.; Huang, A.J.; Doll, M.K.; Zucker, J.R.; et al. Outbreak of Measles Among Persons with Prior Evidence of Immunity, New York City, 2011. Clin. Infect. Dis. 2014, 58, 1205–1210. [Google Scholar] [CrossRef] [PubMed]
- Komabayashi, K.; Seto, J.; Tanaka, S.; Suzuki, Y.; Ikeda, T.; Onuki, N.; Yamada, K.; Ahiko, T.; Ishikawa, H.; Mizuta, K.; et al. The Largest Measles Outbreak, Including 38 Modified Measles and 22 Typical Measles Cases in Its Elimination Era in Yamagata, Japan, 2017. Jpn. J. Infect. Dis. 2018, 71, 413–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centro Nacional de Epidemiología. Instituto de Salud Carlos III. Red Nacional de Vigilancia Epidemiológica. Protocolos de Enfermedades de Declaración Obligatoria. 2013. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/PROTOCOLOS/PROTOCOLOS%20EN%20BLOQUE/PROTOCOLOS_RENAVE-ciber.pdf (accessed on 29 June 2021).
- INEbase (Internet). Población Residente por Fecha, Sexo y Edad; Instituto Nacional de Estadística: Madrid; Available online: https://www.ine.es/jaxiT3/Tabla.htm?t=9681&L=0 (accessed on 31 May 2021).
- Limia Sánchez, A.; Olmedo Lucerón, C. 2nd Seroprevalence Study in Spain, 2017–2018. Rev. Esp. Salud Publica 2021, 95, e202103059. (In English). Available online: https://www.mscbs.gob.es/biblioPublic/publicaciones/recursos_propios/resp/revista_cdrom/VOL95/C_ESPECIALES/RS95C_202103059.pdf (accessed on 1 July 2021). [PubMed]
- Grupo de Trabajo de la Ponencia de Programa y Registro de Vacunaciones. Vacunación en Trabajadores Sanitarios. Comisión de Salud Pública del Consejo Interterritorial del Sistema Nacional de Salud. Ministerio de Sanidad, Servicios Sociales e Igualdad. 2017. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/vacunas/docs/Vacunacion_sanitarios.pdf (accessed on 5 July 2021).
- Centro Nacional de Epidemiología. ISCIII. Vigilancia en Salud Pública. RENAVE. A-Z Enfermedades. Sarampión. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Paginas/Enfermedades-A-Z.aspx (accessed on 3 July 2021).
- Centro Nacional de Epidemiología. Instituto de Salud Carlos III. Plan de Eliminación del Sarampión en España. Madrid, 2000. Available online: http://www.isciii.es/ISCIII/es/contenidos/fd-servicios-cientifico-tecnicos/fd-vigilancias-alertas/fd-enfermedades/fd-enfermedades-prevenibles-vacunacion/PLANSARAMPION.pdf (accessed on 30 June 2021).
- CDC. Interim Infection Prevention and Control Recommendations for Measles in Healthcare Settings. 2019. Available online: https://www.cdc.gov/infectioncontrol/pdf/guidelines/Measles-Interim-IC-Recs-H.pdf (accessed on 2 July 2021).
- Zhang, Z.; Chen, M.; Ma, R.; Pan, J.; Suo, L.; Lu, L. Outbreak of measles among persons with secondary vaccine failure, China, 2018. Hum. Vaccines Immunother. 2020, 16, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Moss, W. Measles in Vaccinated Individuals and the Future of Measles Elimination. Clin. Infect. Dis. 2018, 67, 1320–1321. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Vaccination Status | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age Group | IR ** | Unvaccinated | 1 Dose | ≥ 2 Doses | Total | ||||
| n | % | n | % | n | % | n | % | ||
| <1 year | 33.0 | 93 | 0.1% | 1 | 1.1% | - | - | 94 | 10.9% |
| 1–4 years | 6.7 | 61 | 0.1% | 20 | 24.7% | - | - | 81 | 9.4% |
| 5–19 years | 2.6 | 91 | 0.1% | 7 | 6.0% | 18 | 13.8% | 116 | 13.4% |
| ≥20 years | 2.6 | 416 | 0.6% | 53 | 9.3% | 103 | 15.1% | 572 | 66.3% |
| Total | 3.0 | 661 | 75.6% | 81 | 9.4% | 121 | 14.0% | 863 | 100% |
| No. of Vaccine Doses | No. of Cases | No. of Cases with Dates for Vaccination | Time (Years) from Vaccine to Rash | ||
|---|---|---|---|---|---|
| Mean * | Median * | Range | |||
| ≥2 doses | 121 | 102 | 18.0 | 18.8 | 1.0–31.5 |
| 1 dose | 81 | 63 | 16.2 | 18.2 | 1.0–43.2 |
| Unvaccinated | 1 MCV Doses | ≥2 MCV Doses | Total | p Value * | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | 0 vs. 1 Doses | 0 vs. 2 Doses | 1 vs. 2 Doses | |||
| Clinical presentation | |||||||||||
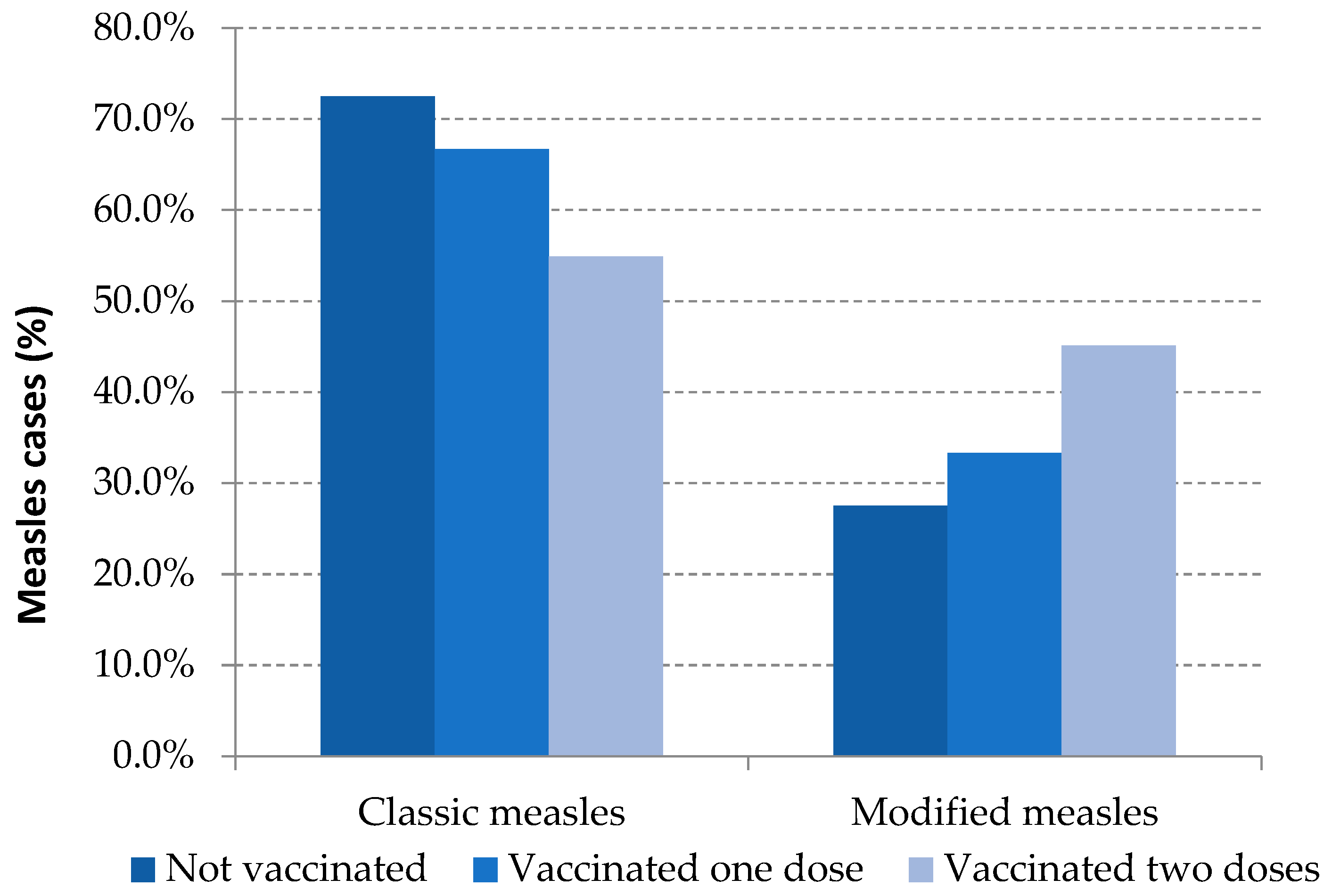
| Classic measles | 479 | 72.5% | 54 | 66.7% | 61 | 50.4% | 594 | 68.8% | 0.295 | 0.000 | 0.029 |
| Modified measles | 182 | 27.5% | 27 | 33.3% | 60 | 49.6% | 269 | 31.2% | |||
| Hospitalization | |||||||||||
| Yes | 253 | 38.3% | 20 | 24.7% | 12 | 9.9% | 285 | 33.0% | 0.020 | 0.000 | 0.006 |
| No | 408 | 61.7% | 61 | 75.3% | 109 | 90.1% | 578 | 67.0% | |||
| Healthcare working environment | |||||||||||
| Yes | 40 | 6.1% | 8 | 9.9% | 33 | 27.3% | 81 | 9.4% | 0.226 | 0.000 | 0.002 |
| No | 621 | 93.9% | 73 | 90.1% | 88 | 72.7% | 782 | 90.6% | |||
| Healthcare Workers (HCW) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | Unvaccinated (n, %) | 1 MCV Doses (n, %) | ≥2 MCV Doses (n, %) | |||||
| Nursing | Registered nurses | 19 | 26.8% | 6 | 20.7% | 1 | 14.3% | 11 | 34.4% |
| Auxiliary nurses | 8 | 11.3% | 3 | 10.3% | 3 | 42.9% | 2 | 6.3% | |
| Medicine | Medical officers | 6 | 8.5% | 2 | 6.9% | - | - | 3 | 9.4% |
| Resident doctors | 12 | 16.9% | 3 | 10.3% | 1 | 14.3% | 8 | 25.0% | |
| Health Science student | 5 | 7.0% | 3 | 10.3% | - | - | 2 | 6.3% | |
| Orderly | 8 | 11.3% | 5 | 17.2% | 1 | 14.3% | 2 | 6.3% | |
| Other HCW * | 13 | 18.3% | 7 | 24.1% | 1 | 14.3% | 4 | 12.5% | |
| Total | 71 | 100% | 29 | 40.8% | 7 | 9.9% | 32 | 45.1% | |
| No Healthcare Workers (HCW) | |||||||||
| n | % | Unvaccinated (n, %) | 1 MCV doses (n, %) | ≥2 MCV doses (n, %) | |||||
| Administrative staff | 7 | 53.8% | 7 | 63.6% | - | - | - | - | |
| Other workers in healthcare settings | 6 | 46.2% | 4 | 36.4% | 1 | 100% | 1 | 100% | |
| Total | 13 | 100% | 11 | 84.6% | 1 | 7.7% | 1 | 7.7% | |
| Sample | Global | Unvaccinated | 1 Dose | ≥2 Doses | p Value * | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | 0 vs. 1 Doses | 0 vs. 2 Doses | 1 vs. 2 Doses | |
| TS **/Urine + Serology | 536 | 57.9% | 344 | 55.5% | 50 | 65.8% | 62 | 55.9% | 0.098 | 0.844 | 0.245 |
| TS/Urine (only) | 260 | 28.1% | 191 | 30.8% | 19 | 25.0% | 36 | 32.4% | 0.159 | 0.514 | 0.529 |
| Serology (only) | 129 | 13.9% | 85 | 13.7% | 7 | 9.2% | 13 | 11.7% | 0.740 | 0.355 | 0.328 |
| Total | 925 | 100% | 620 | 100% | 76 | 100% | 111 | 100% | |||
| Global | Unvaccinated | 1 Dose | >2 Doses | p Value * | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % ** | n | % | n | % | n | % | 0 vs. 1 Doses | 0 vs. 2 Doses | 1 vs. 2 Doses | |
| IgM + | 436 | 81.3% | 302 | 87.8% | 38 | 76.0% | 27 | 43.5% | 0.027 | 0.000 | 0.001 |
| PCR+ | 466 | 86.9% | 314 | 91.3% | 39 | 78.0% | 53 | 85.5% | 0.010 | 0.162 | 0.331 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Perea, N.; Fernández-García, A.; Echevarría, J.E.; de Ory, F.; Pérez-Olmeda, M.; Masa-Calles, J. Measles in Vaccinated People: Epidemiology and Challenges in Surveillance and Diagnosis in the Post-Elimination Phase. Spain, 2014–2020. Viruses 2021, 13, 1982. https://doi.org/10.3390/v13101982
López-Perea N, Fernández-García A, Echevarría JE, de Ory F, Pérez-Olmeda M, Masa-Calles J. Measles in Vaccinated People: Epidemiology and Challenges in Surveillance and Diagnosis in the Post-Elimination Phase. Spain, 2014–2020. Viruses. 2021; 13(10):1982. https://doi.org/10.3390/v13101982
Chicago/Turabian StyleLópez-Perea, Noemí, Aurora Fernández-García, Juan Emilio Echevarría, Fernando de Ory, Mayte Pérez-Olmeda, and Josefa Masa-Calles. 2021. "Measles in Vaccinated People: Epidemiology and Challenges in Surveillance and Diagnosis in the Post-Elimination Phase. Spain, 2014–2020" Viruses 13, no. 10: 1982. https://doi.org/10.3390/v13101982
APA StyleLópez-Perea, N., Fernández-García, A., Echevarría, J. E., de Ory, F., Pérez-Olmeda, M., & Masa-Calles, J. (2021). Measles in Vaccinated People: Epidemiology and Challenges in Surveillance and Diagnosis in the Post-Elimination Phase. Spain, 2014–2020. Viruses, 13(10), 1982. https://doi.org/10.3390/v13101982