
Clinical and Radiological Profiles of COVID-19 Patients with Neurological Symptomatology: A Comparative Study

 ,
,
Abstract
:1. Introduction
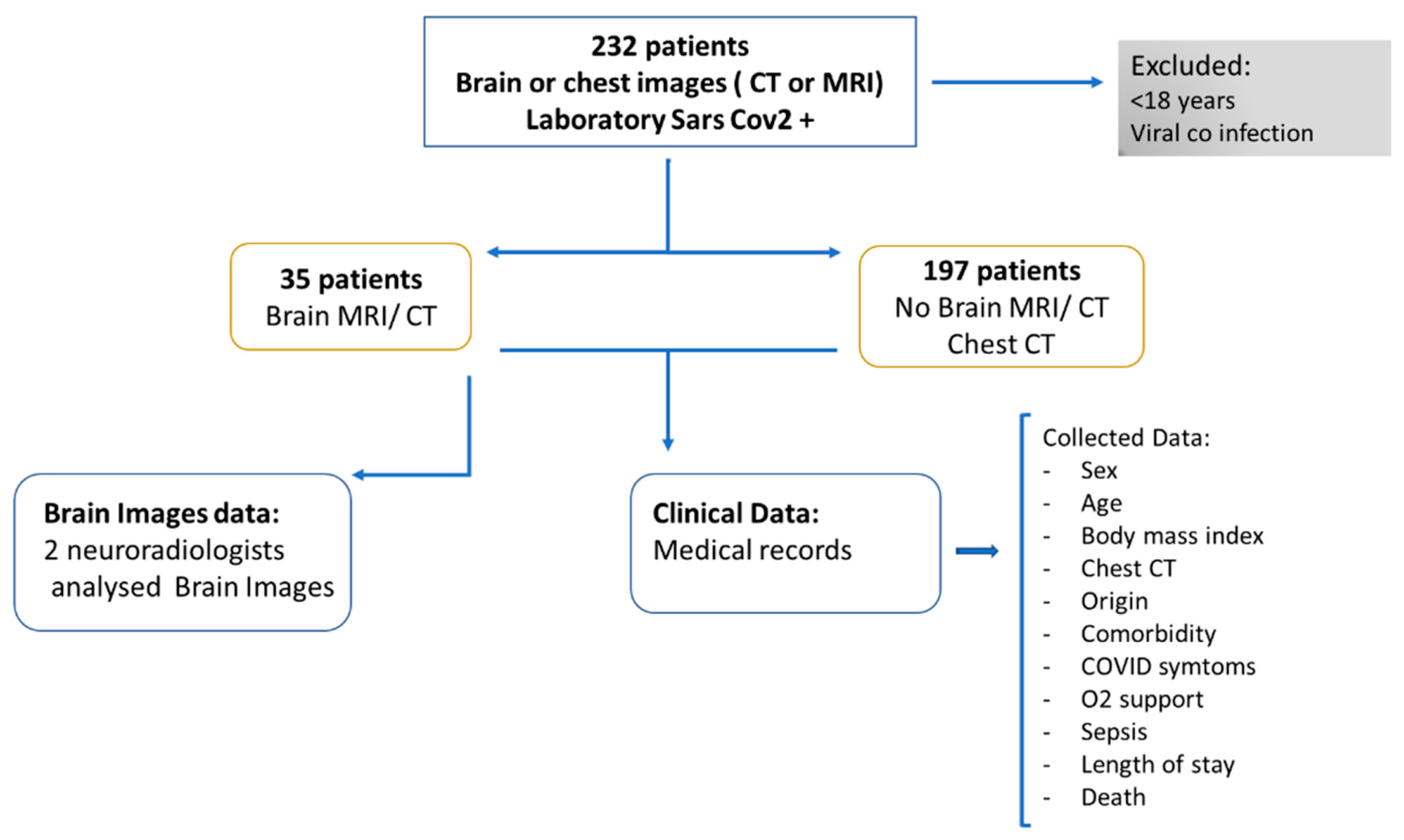
2. Method
Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mirzaee, S.M.M.; Gonçalves, F.G.; Mohammadifard, M.; Tavakoli, S.M.; Vossough, A. Focal Cerebral Arteriopathy in a COVID-19 Pediatric Patient. Radiology 2020, 297, E274–E275. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, M.; Wang, M.; Zhou, Y.; Chang, J.; Xian, Y.; Wang, D.; Mao, L.; Jin, H.; Hu, B. Acute cerebrovascular disease following COVID-19: A single center, retrospective, observational study. Stroke Vasc. Neurol. 2020, 5, 279–284. [Google Scholar] [CrossRef]
- Franceschi, A.; Ahmed, O.; Giliberto, L.; Castillo, M. Hemorrhagic Posterior Reversible Encephalopathy Syndrome as a Manifestation of COVID-19 Infection. Am. J. Neuroradiol. 2020, 41, 1173–1176. [Google Scholar] [CrossRef]
- Poyiadji, N.; Shahin, G.; Noujaim, D.; Stone, M.; Patel, S.; Griffith, B. COVID-19–associated acute hemorrhagic necrotizing encephalopathy: CT and MRI features. Radiology 2020, 296, E119–E120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francesco, G.; Francesca, D.G.; Eliseo, P.; Valerio, D.R.; Roberto, F. Venous cerebral thrombosis in COVID-19 patient. J. Neurol. Sci. 2020, 29, 105379. [Google Scholar] [CrossRef]
- Hughes, C.; Nichols, T.; Pike, M.; Subbe, C.; Elghenzai, S. Cerebral Venous Sinus Thrombosis as a Presentation of COVID-19. Eur. J. Case Rep. Intern. Med. 2020, 7, 001691. [Google Scholar] [CrossRef] [PubMed]
- Lang, M.; Buch, K.; Li, M.D.; Mehan, W.A., Jr.; Lang, A.L.; Leslie-Mazwi, T.M.; Rincon, S.P. Leukoencephalopathy Associated with Severe COVID-19 Infection: Sequela of Hypoxemia? Am. J. Neuroradiol. 2020, 41, 1641–1645. [Google Scholar] [CrossRef]
- Radmanesh, A.; Derman, A.; Lui, Y.W.; Raz, E.; Loh, J.P.; Hagiwara, M.; Borja, M.J.; Zan, E.; Fatterpekar, G.M. COVID-19-associated Diffuse Leukoencephalopathy and Microhemorrhages. Radiology 2020, 297, E223–E227. [Google Scholar] [CrossRef]
- Agarwal, S.; Jain, R.; Dogra, S.; Krieger, P.; Lewis, A.; Nguyen, V.; Melmed, K.; Galetta, S. Cerebral Microbleeds and Leukoencephalopathy in Critically Ill Patients with COVID-19. Stroke 2020, 51, 2649–2655. [Google Scholar] [CrossRef]
- Conte, G.; Avignone, S.; Carbonara, M.; Meneri, M.; Ortolano, F.; Cinnante, C.; Triulzi, F. COVID-19–Associated PRES–like Encephalopathy with Perivascular Gadolinium Enhancement. Am. J. Neuroradiol. 2020, 41, 2206–2208. [Google Scholar] [CrossRef]
- Rasmussen, C.; Niculescu, I.; Patel, S.; Krishnan, A. COVID-19 and Involvement of the Corpus Callosum: Potential Effect of the Cytokine Storm? Am. J. Neuroradiol. 2020, 41, 1625–1628. [Google Scholar] [CrossRef]
- Laurendon, T.; Radulesco, T.; Mugnier, J.; Gérault, M.; Chagnaud, C.; El Ahmadi, A.A.; Varoquaux, A. Bilateral transient olfactory bulb edema during COVID-19–related anosmia. Neurology 2020, 95, 224–225. [Google Scholar] [CrossRef]
- Chetrit, A.; Lechien, J.R.; Ammar, A.; Chekkoury-Idrissi, Y.; Distinguin, L.; Circiu, M.; Saussez, S.; Ballester, M.C.; Vasse, M.; Berradja, N.; et al. Magnetic resonance imaging of COVID-19 anosmic patients reveals abnormalities of the olfactory bulb: Preliminary prospective study. J. Infect. 2020, 81, 816–846. [Google Scholar] [CrossRef]
- Aragão, M.d.F.V.V.; Leal, M.D.C.; Filho, O.Q.C.; Fonseca, T.M.; Valença, M.M. Anosmia in COVID-19 associated with injury to the olfactory bulbs evident on MRI. Am. J. Neuroradiol. 2020, 41, 1703–1706. [Google Scholar] [CrossRef] [PubMed]
- Hutchins, K.L.; Jansen, J.H.; Comer, A.D.; Scheer, R.V.; Zahn, G.S.; Capps, A.E.; Weaver, L.M.; Koontz, N.A. COVID-19–Associated Bifacial Weakness with Paresthesia Subtype of Guillain-Barré Syndrome. Am. J. Neuroradiol. 2020, 41, 1707–1711. [Google Scholar] [CrossRef]
- Aragão, M.F.V.V.; Leal, M.C.; Fonseca, T.M.; Cartaxo Filho, O.Q.; Valença, M.M. Reply. Am. J. Neuroradiol. 2020. [Google Scholar] [CrossRef]
- Dixon, L.; McNamara, C.; Gaur, P.; Mallon, D.; O’Callaghan, C.; Tona, F.; Jan, W.; Wilson, M.; Jones, B. Cerebral microhaemorrhage in COVID-19: A critical illness related phenomenon? Stroke Vasc. Neurol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Klironomos, S.; Tzortzakakis, A.; Kits, A.; Öhberg, C.; Kollia, E.; Ahoromazdae, A.; Almqvist, H.; Aspelin, Å.; Martin, H.; Ouellette, R.; et al. Nervous system involvement in COVID-19: Results from a retrospective consecutive neuroimaging cohort. Radiology 2020, 297, E324–E334. [Google Scholar] [CrossRef]
- Kremer, S.; Lersy, F.; de Sèze, J.; Ferré, J.C.; Maamar, A.; Carsin-Nicol, B.; Collange, O.; Bonneville, F.; Adam, G.; Martin-Blondel, G.; et al. Brain MRI findings in severe COVID-19: A retrospective observational study. Radiology 2020, 297, E242–E251. [Google Scholar] [CrossRef]
- Sachs, J.R.; Gibbs, K.W.; Swor, D.E.; Sweeney, A.P.; Williams, D.W.; Burdette, J.H.; West, T.G.; Geer, C.P. COVID-19-Associated Leukoencephalopathy. Radiology 2020, 296, E184–E185. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Spiezia, L.; Boscolo, A.; Poletto, F.; Cerruti, L.; Tiberio, I.; Campello, E.; Navalesi, P.; Simioni, P. COVID-19-related severe hypercoagulability in patients admitted to intensive care unit for acute respiratory failure. Thromb. Haemost. 2020, 120, 998–1000. [Google Scholar] [CrossRef]
- Jaunmuktane, Z.; Mahadeva, U.; Green, A.; Sekhawat, V.; Barrett, N.A.; Childs, L.; Shankar-Hari, M.; Thom, M.; Jäger, H.R.; Brandner, S. Microvascular injury and hypoxic damage: Emerging neuropathological signatures in COVID-19. Acta Neuropathol. 2020, 140, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Toledano-Massiah, S.; Badat, N.; Leberre, A.; Bruel, C.; Ray, A.; Gerber, S.; Zins, M.; Hodel, J. Unusual Brain MRI Pattern in 2 Patients with COVID-19 Acute Respiratory Distress Syndrome. Am. J. Neuroradiol. 2020, 41, 2204–2205. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Lawson, E.; Verma, S.; Peterson, R.; Sidhu, R. Cytotoxic Lesion of the Corpus Callosum in an Adolescent with Multisystem Inflammatory Syndrome and SARS-CoV-2 Infection. Am. J. Neuroradiol. 2020, 41, 2017–2019. [Google Scholar] [CrossRef] [PubMed]
- Gaur, P.; Dixon, L.; Jones, B.; Lyall, H.; Jan, W. COVID-19-Associated Cytotoxic Lesions of the Corpus Callosum. Am. J. Neuroradiol. 2020, 41, 1905–1907. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C.; et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.Y.; Lee, H.K.; Park, J.H.; Cho, S.J.; Kwon, M.; Jo, C.; Koh, Y.H. Altered COVID-19 receptor ACE2 expression in a higher risk group for cerebrovascular disease and ischemic stroke. Biochem. Biophys. Res. Commun. 2020, 528, 413–419. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Zayet, S.; Kadiane-Oussou, N.J.; Lepiller, Q.; Zahra, H.; Royer, P.Y.; Toko, L.; Gendrin, V.; Klopfenstein, T. Clinical features of COVID-19 and influenza: A comparative study on Nord Franche-Comte cluster. Microbes Infect. 2020, 22, 481–488. [Google Scholar] [CrossRef]
- Yan, C.; Faraji, F.; Prajapati, D.; Boone, C.; De Conde, A. Association of chemosensory dysfunction and Covid-19 in patients presenting with influenza-like symptoms [published online 12 April 2020]. Int. Forum. Allergy Rhinol. 2020, 10, 806–813. [Google Scholar] [CrossRef] [Green Version]
- Kosugi, E.M.; Lavinsky, J.; Romano, F.R.; Fornazieri, M.A.; Luz-Matsumoto, G.R.; Lessa, M.M.; Piltcher, O.B.; Sant’Anna, G.D. Incomplete and late recovery of sudden olfactory dysfunction in COVID-19. Braz. J. Otorhinolaryngol. 2020, 86, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Vaira, L.A.; Deiana, G.; Fois, A.G.; Pirina, P.; Madeddu, G.; De Vito, A.; Babudieri, S.; Petrocelli, M.; Serra, A.; Bussu, F.; et al. Objective evaluation of anosmia and ageusia in COVID-19 patients: Single-center experience on 72 cases. Head Neck 2020, 42, 1252–1258. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli, A.; Pezzati, L.; Conti, F.; Bernacchia, D.; Siano, M.; Oreni, L.; Rusconi, S.; Gervasoni, C.; Ridolfo, A.L.; Rizzardini, G.; et al. Self-reported Olfactory and Taste Disorders in Patients With Severe Acute Respiratory Coronavirus 2 Infection: A Cross-sectional Study. Clin. Infect. Dis. 2020, 71, 889–890. [Google Scholar] [CrossRef] [Green Version]
- Pauline, V.; Lan, V.D.; L’Huillier Arnaud, G.; Manuel, S.; Laurent, K.; Frederique, J. Clinical features of covid-19. BMJ 2020, 369, m1470. [Google Scholar] [CrossRef] [Green Version]
- Fajnzylber, J.; Regan, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Worrall, D.; Giguel, F.; Piechocka-, A.; Atyeo, C.; et al. Massachusetts Consortium for Pathogen Readiness.SARS-CoV-2 viral load is associated with increased disease severity and mortality. Nat. Commun. 2020, 11, 5493. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Perl, D.P.; Nair, G.; Li, W.; Maric, D.; Murray, H.; Dodd, S.J.; Koretsky, A.P.; Watts, J.A.; Cheung, V.; et al. Microvascular Injury in the Brains of Patients with Covid-19. N. Engl. J. Med. 2021, 384, 481–483. [Google Scholar] [CrossRef]
- Aragao, M.F.V.V.; Oliveira, A.D.P.; Lima, A.R.M.C.; Leal, M.C.; Valenca, M.M. Virtual Biopsy: A Reality Thanks to Advances in Radiology. AJNR Am. J. Neuroradiol. 2021. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | CT and/or MRI of the Brain | p-Value | |
|---|---|---|---|
| Yes | No | ||
| n (%) | n (%) | ||
| Sex (Masculine) | 20/35 (57.1) | 115/197 (58.4) | 0.892 * |
| Chest CT (Extension of pulmonary involvement) | |||
| Normal | 3/31 (9.7) | 0/197 (0.0) | <0.001 ** |
| Typical (T) < 25% | 13/31 (41.9) | 121/197 (61.4) | |
| T beween 25–50% | 5/31 (16.1) | 61/197 (31.0) | |
| T > 50% | 9/31 (29.0) | 14/197 (7.1) | |
| Between 25–50% with pleural effusion | 0/31 (0.0) | 1/197 (0.5) | |
| >50% with pleural effusion | 1/31 (3.2) | 0/197 (0.0) | |
| Origin | |||
| Internal | 14/33 (42.4) | 103/197 (52.3) | <0.001 ** |
| Intensive care unit | 11/33 (33.3) | 5/197 (2.5) | |
| Urgency | 4/33 (12.1) | 64/197 (32.5) | |
| External | 4/33 (12.1) | 25/197 (12.7) | |
| Systemic arterial hypertension | 18/34 (52.9) | 67/186 (36.0) | 0.062 * |
| Diabetes melitus | 10/32 (31.3) | 44/184 (23.9) | 0.376 * |
| Dyslipidemia | 2/27 (7.4) | 17/185 (9.2) | 1.000 ** |
| Asthma/COPD | 2/29 (6.9) | 25/173 (14.5) | 0.382 ** |
| Chronic kidney failure | 4/30 (13.3) | 7/182 (3.8) | 0.053 ** |
| Fever | 24/29 (82.8) | 151/188 (80.3) | 0.757 * |
| Cough | 22/29 (75.9) | 159/189 (84.1) | 0.289 ** |
| Dyspnea | 18/30 (60.0) | 151/190 (79.5) | 0.019 * |
| O2 catheter | 14/29 (48.3) | 78/189 (41.3) | 0.477 * |
| Mechanic ventilatory assistance | 10/29 (34.5) | 19/190 (10.0) | 0.001 ** |
| Headache | 12/28 (42.9) | 78/188 (41.5) | 0.891 * |
| Anosmia | 7/11 (63.6) | 50/66 (75.8) | 0.462 ** |
| Disgeusia | 5/9 (55.6) | 32/43 (74.4) | 0.419 ** |
| Gastric symptoms | 7/26 (26.9) | 61/190 (32.1) | 0.594 * |
| Sepsis | 7/9 (24.1) | 12/189 (6.3) | 0.006 ** |
| Obesity (qualitative) | 5/29 (17.2) | 20/186 (10.8) | 0.347 ** |
| Death | 3/33 (9.1) | 10/192 (5.2) | 0.413 ** |
| Obesity (BMI ≥ 30) | 2/9 (22.2) | 35/78 (44.9) | 0.289 ** |
| Mean ± DP | Mean ± DP | ||
| Age (years) | 54.3 ± 18.1 | 49.6 ± 13.7 | 0.163 *** |
| Body mass index | 27.1 ± 6.3 | 29.6 ± 5.2 | 0.179 *** |
| Median (Q1; Q3) | Median (Q1; Q3) | ||
| Interval of symptom onset at admission | 6.0 (3.7; 7.7) | 7.0 (5.0; 8.0) | 0.497 ¥ |
| Length of stay | 8.5 (5.0; 23.5) | 8.0 (5.0; 14.0) | 0.630 ¥ |
| #. | Sex | Age | Anosmia | Other Neurological Symptoms | Fever | Cough | Dyspnea | Oxygen Support | Brain Imaging | Thorax ct | Type of Care | Death |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 31 | yes | seizure | yes | yes | yes | ventilator | normal (CT/MRI) | >50% | ICU | no |
| 2 | M | 54 | - | seizure | yes | yes | yes | O2 catheter | normal (CT) | <25% | urgency | no |
| 3 | F | 72 | no | headache | no | no | no | no | normal (CT) | <25% | urgency | no |
| 4 | M | 46 | - | headache | no | no | no | no | normal (CT) | <25% | internal | no |
| 5 | M | 29 | - | headache, seizure | yes | yes | no | no | cavernous sinus gaseous foci (CT) | <25% | urgency | no |
| 6 | M | 60 | - | dysesthesia, inferior limbs paresthesia | yes | yes | yes | ventilator | normal (CT) | >50% | internal | no |
| 7 | M | 73 | - | syncope | no | yes | no | no | hypodensity foci (CT) | 25–50% | internal | no |
| 8 | F | 84 | - | no | no | no | no | intraparanchymal temporoparietal hematoma (CT) | 25–50% | internal | yes | |
| 9 | F | 43 | yes | headache | yes | yes | yes | no | normal (MRI) | 25–50% | urgency | no |
| 10 | M | 67 | no | myopathy | yes | yes | yes | ventilator | normal (CT) | >50% | internal | no |
| 11 | F | 53 | - | headache | yes | yes | yes | no | normal (CT) | <25% | internal | No |
| 12 | F | 69 | - | seizure | yes | yes | yes | no | normal (CT) | <25% | internal | No |
| 13 | M | 55 | - | - | no | yes | no | no | normal (CT) | <25% | internal | no |
| 14 | M | 81 | - | alteration of consciousness | yes | yes | no | ventilator | normal (CT) | <25% | internal | yes |
| 15 | M | 26 | seizure, hemiparesis | no | no | no | no | temporo-occipital hypersignal on FLAIR, hemosiderosis (MRI) | >50% | ICU | no | |
| 16 | F | 34 | yes | headache | yes | yes | no | no | olfactory bulb injury (MRI) | <25% | internal | no |
| 17 | F | 43 | no | headache, dizziness | no | yes | yes | no | olfactory bulb injury (MRI) | - | internal | no |
| 18 | M | 40 | yes | headache, hemiparesthesia, visual field fog | yes | yes | no | no | corpus callosum restricted DWI lesion and olfactory bulb injuries (MRI) | - | internal | no |
| 19 | F | 35 | yes | headache | yes | yes | no | no | olfactory bulb injury (MRI) | normal | internal | no |
| 20 | F | 43 | - | seizure | no | no | no | no | normal | <25% | internal | no |
| 21 | M | 83 | - | lowering of level of consciousness | yes | yes | no | O2 catheter | signs of past frontal and cerebellar injuries (MRI) | 25–50% | ICU | no |
| 22 | M | 62 | - | severe depression, parkinsonism, coma | yes | no | yes | ventilator | olfactory bulb injury (MRI) | >50% | ICU | no |
| 23 | M | 66 | - | ischemic encephalopathy due to cardiac arrest | yes | yes | no | ventilator | normal (CT/MRI) | 25–50% | ICU | no |
| 24 | F | 25 | yes | headache | yes | no | no | no | olfactory bulb injury (MRI) | normal | external | no |
| 25 | F | 36 | - | headache | - | - | - | no | olfactory bulb injury (MRI) | normal | external | no |
| 26 | M | 71 | - | Neurologic sequel | - | - | - | no | parietal subcortical microbleeding (MRI) | >50% | ICU | no |
| 27 | F | 61 | - | headache | - | - | - | no | cortical/subcortical hematomas and pale globes microbleedings + olfactory bulb injury (MRI) | >50% | internal | no |
| 28 | M | 80 | - | seizure, recurrent syncope | yes | yes | yes | O2 catheter | frontal microbleeding and olfactory bulb injury (MRI) | <25% | ICU | no |
| 29 | M | 49 | yes | seizure | yes | yes | yes | O2 catheter | normal (MRI) | <25% | ICU | no |
| 30 | F | 70 | - | yes | yes | yes | ventilator | microbleedings in base ganglia, brainstem and cerebellum (MRI) | >50% | ICU | yes | |
| 31 | M | 62 | - | coma | yes | yes | yes | ventilator | cerebellum, corpus callosum and parietal white matterbleeding and restricted DWI small lesions (MRI) | >50% | ICU | no |
| 32 | M | 40 | left facial palsy | yes | No | no | no | geniculate ganglion injury and olfactory bulb injury (MRI) | - | external | no | |
| 33 | M | 41 | encephalitis | - | - | - | - | olfactory bulb injury (MRI) | - | ICU | no | |
| 34 | F | 34 | stroke and seizure | - | - | - | - | old ischemic lesion with restricted DWI areas/right middle cerebral artery stenosis/areas of hemorrhage and olfactory bulb injury (MRI) | <25% | external | no | |
| 35 | M | 82 | desorientation | - | - | - | - | Small right parietal cortical gliosis (MRI) | >50% | internal | no |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aragao, M.d.F.V.V.; Leal, M.d.C.; Andrade, P.H.P.; Cartaxo Filho, O.Q.; Aragao, L.V.; Fonseca, T.M.; Valenca, M.A.; Leao, M.R.V.C.; Aragao, J.P.V.; Soares, M.L.; et al. Clinical and Radiological Profiles of COVID-19 Patients with Neurological Symptomatology: A Comparative Study. Viruses 2021, 13, 845. https://doi.org/10.3390/v13050845
Aragao MdFVV, Leal MdC, Andrade PHP, Cartaxo Filho OQ, Aragao LV, Fonseca TM, Valenca MA, Leao MRVC, Aragao JPV, Soares ML, et al. Clinical and Radiological Profiles of COVID-19 Patients with Neurological Symptomatology: A Comparative Study. Viruses. 2021; 13(5):845. https://doi.org/10.3390/v13050845
Chicago/Turabian StyleAragao, Maria de Fatima Viana Vasco, Mariana de Carvalho Leal, Pedro Henrique Pereira Andrade, Ocelio Queiroga Cartaxo Filho, Lucas Vasco Aragao, Tatiana Moreira Fonseca, Marcelo Andrade Valenca, Maria Regina Vendas Carneiro Leao, Joao Pedro Vasco Aragao, Maria Lúcia Soares, and et al. 2021. "Clinical and Radiological Profiles of COVID-19 Patients with Neurological Symptomatology: A Comparative Study" Viruses 13, no. 5: 845. https://doi.org/10.3390/v13050845
APA StyleAragao, M. d. F. V. V., Leal, M. d. C., Andrade, P. H. P., Cartaxo Filho, O. Q., Aragao, L. V., Fonseca, T. M., Valenca, M. A., Leao, M. R. V. C., Aragao, J. P. V., Soares, M. L., Lima, M. P., Caldas, S. S., & Valenca, M. M. (2021). Clinical and Radiological Profiles of COVID-19 Patients with Neurological Symptomatology: A Comparative Study. Viruses, 13(5), 845. https://doi.org/10.3390/v13050845