
Plasma Total Antioxidant Capacity and Carbonylated Proteins Are Increased in Pregnant Women with Severe COVID-19

 ,
,  , ,
, ,  ,
,  , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection and Plasma Measurement of OS, Angiogenic, and RAS Markers
2.3. Exposure
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Association between OS, Angiogenic, and RAS Markers with the Primary and Secondary Outcomes
4. Discussion
4.1. Clinical Interpretation
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Portilla, R.J.; Sotiriadis, A.; Chatzakis, C.; Torres-Torres, J.; Espino Y Sosa, S.; Sandoval-Mandujano, K.; Castro-Bernabe, D.A.; Medina-Jimenez, V.; Monarrez-Martin, J.C.; Figueras, F.; et al. Pregnant women with SARS-CoV-2 infection are at higher risk of death and pneumonia: Propensity score matched analysis of a nationwide prospective cohort (COV19Mx). Ultrasound Obs. Gynecol. 2021, 57, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Suhail, S.; Zajac, J.; Fossum, C.; Lowater, H.; McCracken, C.; Severson, N.; Laatsch, B.; Narkiewicz-Jodko, A.; Johnson, B.; Liebau, J.; et al. Role of Oxidative Stress on SARS-CoV (SARS) and SARS-CoV-2 (COVID-19) Infection: A Review. Protein J. 2020, 39, 644–656. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Roche, L.; Mesta, F. Oxidative Stress as Key Player in Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) Infection. Arch. Med. Res. 2020, 51, 384–387. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Gillies, C.L.; Singh, R.; Singh, A.; Chudasama, Y.; Coles, B.; Seidu, S.; Zaccardi, F.; Davies, M.J.; Khunti, K. Prevalence of co-morbidities and their association with mortality in patients with COVID-19: A systematic review and meta-analysis. Diabetes Obes. Metab. 2020, 22, 1915–1924. [Google Scholar] [CrossRef]
- Stefan, N.; Birkenfeld, A.L.; Schulze, M.B. Global pandemics interconnected—Obesity, impaired metabolic health and COVID-19. Nat. Rev. Endocrinol. 2021, 17, 135–149. [Google Scholar] [CrossRef]
- Saleh, J.; Peyssonnaux, C.; Singh, K.K.; Edeas, M. Mitochondria and microbiota dysfunction in COVID-19 pathogenesis. Mitochondrion 2020, 54, 1–7. [Google Scholar] [CrossRef]
- Verma, S.; Joshi, C.S.; Silverstein, R.B.; He, M.; Carter, E.B.; Mysorekar, I.U. SARS-CoV-2 colonization of maternal and fetal cells of the human placenta promotes alteration of local renin-angiotensin system. Med 2021, 2, 575–590. [Google Scholar] [CrossRef]
- Dupont, V.; Kanagaratnam, L.; Goury, A.; Poitevin, G.; Bard, M.; Julien, G.; Bonnivard, M.; Champenois, V.; Noel, V.; Mourvillier, B.; et al. Excess Soluble fms-like Tyrosine Kinase 1 Correlates With Endothelial Dysfunction and Organ Failure in Critically Ill Coronavirus Disease 2019 Patients. Clin. Infect. Dis. 2021, 72, 1834–1837. [Google Scholar] [CrossRef]
- Giardini, V.; Ornaghi, S.; Acampora, E.; Vasarri, M.V.; Arienti, F.; Gambacorti-Passerini, C.; Casati, M.; Carrer, A.; Vergani, P. Letter to the Editor: SFlt-1 and PlGF Levels in Pregnancies Complicated by SARS-CoV-2 Infection. Viruses 2021, 13, 2377. [Google Scholar] [CrossRef]
- Espino-Y-Sosa, S.; Martinez-Portilla, R.J.; Torres-Torres, J.; Solis-Paredes, J.M.; Estrada-Gutierrez, G.; Hernandez-Pacheco, J.A.; Espejel-Nuñez, A.; Mateu-Rogell, P.; Juarez-Reyes, A.; Lopez-Ceh, F.E.; et al. Novel Ratio Soluble Fms-like Tyrosine Kinase-1/Angiotensin-II (sFlt-1/ANG-II) in Pregnant Women Is Associated with Critical Illness in COVID-19. Viruses 2021, 13, 1906. [Google Scholar] [CrossRef] [PubMed]
- Torres-Torres, J.; Espino-Y-Sosa, S.; Poon, L.C.; Solis-Paredes, J.M.; Estrada-Gutierrez, G.; Espejel-Nuñez, A.; Alfonso-Guillen, Y.; Aguilar-Andrade, L.; Hernández-Pacheco, J.A. Increased levels of soluble fms-like tyrosine kinase-1 are associated with adverse outcomes in pregnant women with COVID-19. Ultrasound Obs. Gynecol. 2022, 59, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Gérard-Monnier, D.; Erdelmeier, I.; Régnard, K.; Moze-Henry, N.; Yadan, J.C.; Chaudière, J. Reactions of 1-methyl-2-phenylindole with malondialdehyde and 4-hydroxyalkenals. Analytical applications to a colorimetric assay of lipid peroxidation. Chem. Res. Toxicol. 1998, 11, 1176–1183. [Google Scholar] [CrossRef] [PubMed]
- Dalle-Donne, I.; Rossi, R.; Giustarini, D.; Milzani, A.; Colombo, R. Protein carbonyl groups as biomarkers of oxidative stress. Clin. Chim. Acta. 2003, 329, 23–38. [Google Scholar] [CrossRef]
- Apak, R.; Güçlü, K.; Ozyürek, M.; Karademir, S.E.; Altun, M. Total antioxidant capacity assay of human serum using copper(II)-neocuproine as chromogenic oxidant: The CUPRAC method. Free Radic. Res. 2005, 39, 949–961. [Google Scholar] [CrossRef]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef]
- Poon, L.C.; Yang, H.; Kapur, A.; Melamed, N.; Dao, B.; Divakar, H.; McIntyre, H.D.; Kihara, A.B.; Ayres-de-Campos, D.; Ferrazzi, E.M.; et al. Global interim guidance on coronavirus disease 2019 (COVID-19) during pregnancy and puerperium from FIGO and allied partners: Information for healthcare professionals. Int. J. Gynaecol. Obstet. 2020, 149, 273–286. [Google Scholar] [CrossRef]
- Alwazeer, D.; Liu, F.F.C.; Wu, X.Y.; LeBaron, T.W. Combating Oxidative Stress and Inflammation in COVID-19 by Molecular Hydrogen Therapy: Mechanisms and Perspectives. Oxid. Med. Cell. Longev. 2021, 2021, 5513868. [Google Scholar] [CrossRef]
- Mohiuddin, M.; Kasahara, K. The emerging role of oxidative stress in complications of COVID-19 and potential therapeutic approach to diminish oxidative stress. Respir. Med. 2021, 187, 106605. [Google Scholar] [CrossRef]
- Thomas, T.; Stefanoni, D.; Dzieciatkowska, M.; Issaian, A.; Nemkov, T.; Hill, R.C.; Francis, R.O.; Hudson, K.E.; Buehler, P.W.; Zimring, J.C.; et al. Evidence of Structural Protein Damage and Membrane Lipid Remodeling in Red Blood Cells from COVID-19 Patients. J. Proteome Res. 2020, 19, 4455–4469. [Google Scholar] [CrossRef]
- Halliwell, B.; Gutteridge, J.M.C. Free Radicals in Biology and Medicine; Oxford University Press: Oxford, UK, 2015; p. 896. [Google Scholar]
- Karkhanei, B.; Talebi Ghane, E.; Mehri, F. Evaluation of oxidative stress level: Total antioxidant capacity, total oxidant status and glutathione activity in patients with COVID-19. New Microbes New Infect. 2021, 42, 100897. [Google Scholar] [CrossRef] [PubMed]
- Ntyonga-Pono, M.P. COVID-19 infection and oxidative stress: An under-explored approach for prevention and treatment? Pan. Afr. Med. J. 2020, 35, 1–2. [Google Scholar] [CrossRef]
- Aykac, K.; Ozsurekci, Y.; Yayla, B.C.C.; Gurlevik, S.L.; Oygar, P.D.; Bolu, N.B.; Tasar, M.A.; Erdinc, F.S.; Ertem, G.T.; Neselioglu, S.; et al. Oxidant and antioxidant balance in patients with COVID-19. Pediatr Pulmonol. 2021, 56, 2803–2810. [Google Scholar] [CrossRef] [PubMed]
- Le Bras, M.; Clément, M.V.; Pervaiz, S.; Brenner, C. Reactive oxygen species and the mitochondrial signaling pathway of cell death. Histol. Histopathol. 2005, 20, 205–219. [Google Scholar]
- Camini, F.C.; da Silva Caetano, C.C.; Almeida, L.T.; de Brito Magalhães, C.L. Implications of oxidative stress on viral pathogenesis. Arch. Virol. 2017, 162, 907–917. [Google Scholar] [CrossRef]
- Kohen, R.; Nyska, A. Oxidation of biological systems: Oxidative stress phenomena, antioxidants, redox reactions, and methods for their quantification. Toxicol. Pathol. 2002, 30, 620–650. [Google Scholar] [CrossRef] [Green Version]
- Scibior, D.; Skrzycki, M.; Podsiad, M.; Czeczot, H. Glutathione level and glutathione-dependent enzyme activities in blood serum of patients with gastrointestinal tract tumors. Clin. Biochem. 2008, 41, 852–858. [Google Scholar] [CrossRef]
- Willcox, J.K.; Ash, S.L.; Catignani, G.L. Antioxidants and prevention of chronic disease. Crit. Rev. Food Sci. Nutr. 2004, 44, 275–295. [Google Scholar] [CrossRef]
- Otifi, H.M.; Adiga, B.K. Endothelial Dysfunction in Covid-19. Am. J. Med. Sci. 2022, 1–7. [Google Scholar] [CrossRef]
- Seitz, A.; Ong, P. Endothelial dysfunction in COVID-19: A potential predictor of long-COVID? Int. J. Cardiol. 2022, 349, 155–156. [Google Scholar] [CrossRef]
- Hokama, L.T.; Veiga, A.D.M.; Menezes, M.C.S.; Sardinha Pinto, A.A.; de Lima, T.M.; Ariga, S.K.K.; Barbeiro, H.V.; Barbeiro, D.F.; de Lucena Moreira, C.; Stanzani, G.; et al. Endothelial injury in COVID-19 and septic patients. Microvasc. Res. 2022, 140, 104303. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, M.W.; Castillo, J., Jr.; Ibrahim, T.; Cornelius, D.C.; Campbell, N.; Amaral, L.; Vaka, V.R.; Usry, N.; Williams, J.M.; LaMarca, B. AT1-AA (Angiotensin II Type 1 Receptor Agonistic Autoantibody) Blockade Prevents Preeclamptic Symptoms in Placental Ischemic Rats. Hypertension 2018, 71, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Forrester, S.J.; O’Brien, S.; Baggett, A.; Rizzo, V.; Eguchi, S. AT1 receptor signaling pathways in the cardiovascular system. Pharm. Res. 2017, 125, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Li, X.C.; Zhou, X.; Zhuo, J.L. Evidence for a Physiological Mitochondrial Angiotensin II System in the Kidney Proximal Tubules: Novel Roles of Mitochondrial Ang II/AT(1a)/O(2)(-) and Ang II/AT(2)/NO Signaling. Hypertension 2020, 76, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Ramin, S.M.; Kellems, R.E. Potential roles of angiotensin receptor-activating autoantibody in the pathophysiology of preeclampsia. Hypertension 2007, 50, 269–275. [Google Scholar] [CrossRef]
- Deer, E.; Jones, J.; Cornelius, D.C.; Comley, K.; Herrock, O.; Campbell, N.; Fitzgerald, S.; Ibrahim, T.; LaMarca, B.; Amaral, L.M. Progesterone Induced Blocking Factor Reduces Hypertension and Placental Mitochondrial Dysfunction in Response to sFlt-1 during Pregnancy. Cells 2021, 10, 2817. [Google Scholar] [CrossRef]
- Foidart, J.M.; Schaaps, J.P.; Chantraine, F.; Munaut, C.; Lorquet, S. Dysregulation of anti-angiogenic agents (sFlt-1, PLGF, and sEndoglin) in preeclampsia—A step forward but not the definitive answer. J. Reprod. Immunol. 2009, 82, 106–111. [Google Scholar] [CrossRef]
- Sánchez-Aranguren, L.C.; Espinosa-González, C.T.; González-Ortiz, L.M.; Sanabria-Barrera, S.M.; Riaño-Medina, C.E.; Nuñez, A.F.; Ahmed, A.; Vasquez-Vivar, J.; López, M. Soluble Fms-Like Tyrosine Kinase-1 Alters Cellular Metabolism and Mitochondrial Bioenergetics in Preeclampsia. Front. Physiol. 2018, 9, 83. [Google Scholar] [CrossRef] [Green Version]
- Gadotti, A.C.; Lipinski, A.L.; Vasconcellos, F.T.F.; Marqueze, L.F.; Cunha, E.B.B.; Campos, A.C.; Oliveira, C.F.; Amaral, A.N.; Baena, C.P.; Telles, J.P.; et al. Susceptibility of the patients infected with Sars-Cov2 to oxidative stress and possible interplay with severity of the disease. Free Radic. Biol. Med. 2021, 165, 184–190. [Google Scholar] [CrossRef]
- Cheng, S.B.; Liu, H.T.; Chen, S.Y.; Lin, P.T.; Lai, C.Y.; Huang, Y.C. Changes of Oxidative Stress, Glutathione, and Its Dependent Antioxidant Enzyme Activities in Patients with Hepatocellular Carcinoma before and after Tumor Resection. PLoS ONE 2017, 12, e0170016. [Google Scholar] [CrossRef]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid peroxidation: Production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid. Med. Cell. Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Non-Severe COVID-19 n = 40 | Severe COVID-19 n = 17 | p-Value |
|---|---|---|---|
| Maternal age (years) | 30.50 (26.1–33.7) | 31.5 (27.3–35.2) | 0.458 |
| Gestational age at diagnosis (weeks) | 34.6 (31.0–38.6) | 30.3 (27.1–33.6) | 0.02 |
| pBMI (kg/m2) | 28.9 (24.9–31.2) | 28.5 (23.3–31.6) | 0.827 |
| SpO2% | 95.6 (93.0–96.0) | 92.5 (79.6–96.0) | 0.095 |
| Smoking | 0 | 1 (5.90%) | 0.122 |
| Chronic hypertension | 1 (2.50%) | 1 (5.90%) | 0.495 |
| Pre-gestational diabetes | 2 (5.00%) | 0 | 0.348 |
| Chronic renal disease | 1 (2.50%) | 0 | 0.511 |
| Gestational age at delivery (weeks) | 38.1 (36.7–39.0) | 35.0 (31.5–37.5) | 0.002 |
| Apgar 1 min | 8 (7–8) | 2 (2–8) | 0.076 |
| Apgar 5 min | 9 (9–9) | 9 (7–9) | 0.126 |
| Fetal growth restriction | 3 (7.70%) | 4 (25.0%) | 0.08 |
| Stillbirth | 1 (2.60%) | 1 (6.30%) | 0.507 |
| Neonatal death | 2 (7.70%) | 2 (16.7%) | 0.402 |
| ICU admission | 4 (10.5%) | 5 (29.4%) | 0.08 |
| Viral sepsis | 7 (26.9%) | 5 (41.7%) | 0.363 |
| Maternal death | 0 | 3 (17.6%) | 0.006 |
| Characteristic | Non-Severe COVID-19 | Severe COVID-19 | p-Value |
|---|---|---|---|
| n = 40 | n = 17 | ||
| Leukocytes (×10/L) | 8.65 (7.25–11.9) | 8.40 (7.15–12.2) | 0.884 |
| Neutrophils (×10/L) | 6.75 (5.25–9.60) | 7.30 (4.95–10.6) | 0.548 |
| Lymphocytes (×10/L) | 1.20 (0.90–1.63) | 1.00 (0.85–1.20) | 0.168 |
| Hemoglobin (g/dL) | 12.1 (11.3–13.0) | 12.7 (11.2–14.2) | 0.348 |
| Hematocrit% | 36.5 (33.9–39.3) | 37.8 (34.7–42.0) | 0.229 |
| Platelets (×103/L) | 230 (200–275) | 196 (174–238) | 0.063 |
| Glucose (mg/dL) | 80.0 (73.0–86.5) | 85.0 (75.5–102) | 0.222 |
| Triglycerides (mg/dL) | 265 (204–320) | 295 (214–345) | 0.449 |
| Total cholesterol (mg/dL) | 197 (172–235) | 143 (123–207) | 0.015 |
| Creatinine (mg/dl) | 0.56 (0.56–0.68) | 0.64 (0.53–0.75) | 0.206 |
| Uric acid (mg/dL) | 4.30 (3.58–5.80) | 4.40 (3.50–6.30) | 0.951 |
| D-Dimer (ng/mL) | 2037 (1268–3598) | 1434 (1276–2917) | 0.58 |
| Fibrinogen (mg/dL) | 492 (446–603) | 570 (456–615) | 0.445 |
| PTT (seconds) | 27.0 (24.4–29.1) | 26.2 (24.7–27.9) | 0.774 |
| PT (seconds) | 11.0 (10.6–11.5) | 10.2 (9.65–11.4) | 0.011 |
| C-RP (mg/L) | 27.6 (9.64–106) | 24.9 (9.86–129) | 0.773 |
| Procalcitonin (ng/mL) | 0.07 (0.03–0.20) | 0.25 (0.05–0.77) | 0.038 |
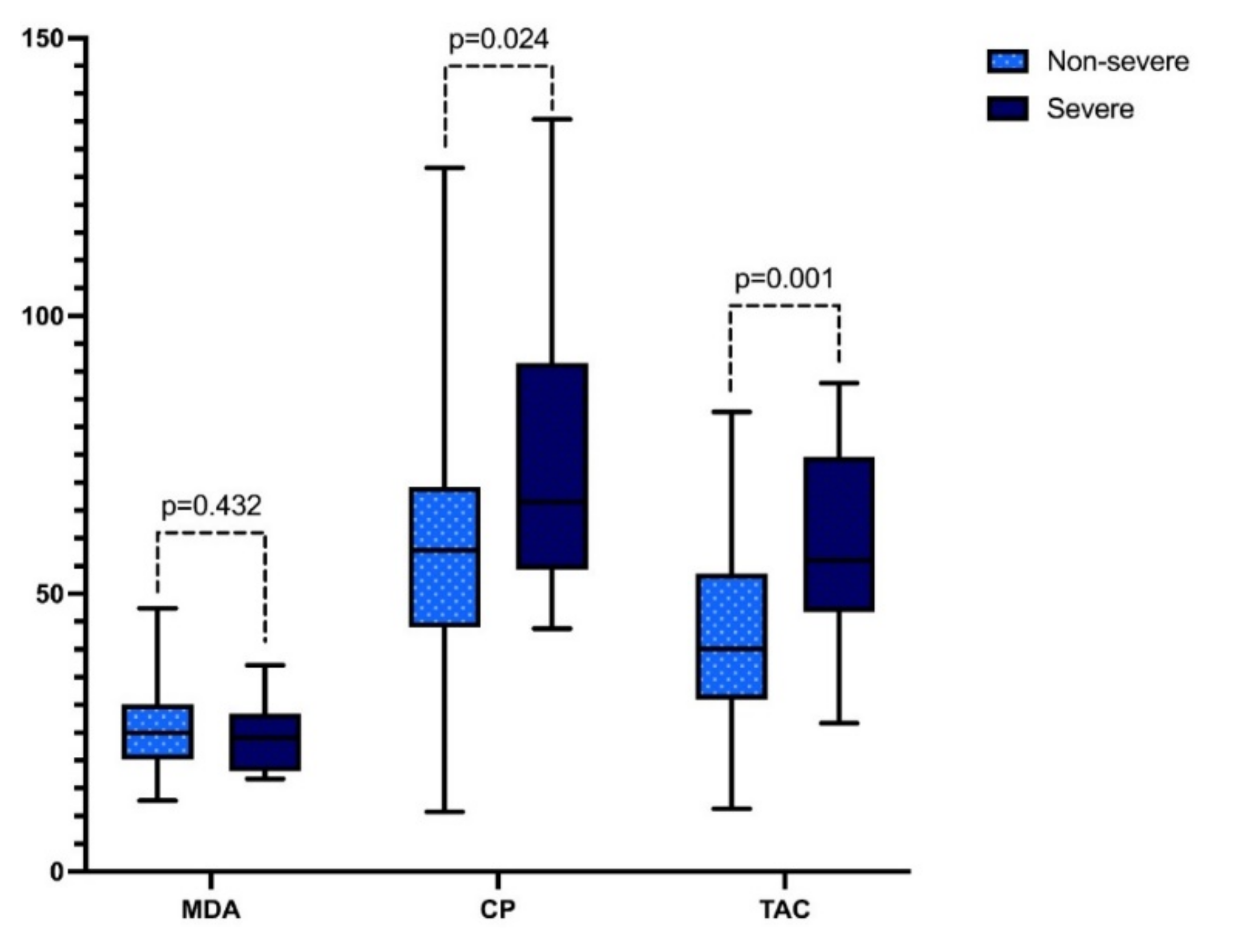
| MDA (pmol MDA/mg dry weight) | 25.0 (20.1–30.1) | 24.1 (18.0–28.5) | 0.432 |
| CP (pmol CP/mg of protein) | 5782 (4393–6919) | 6651 (5437–9154) | 0.024 |
| TAC (pmol of Trolox equivalent/mg of protein) | 40.1 (31.0–53.6) | 56.1 (46.8–74.7) | 0.001 |
| PlGF (pg/mL) | 135 (48.7–195) | 143 (52.4–281) | 0.48 |
| sFlt-1 (pg/mL) | 1477 (1096–3275) | 3607 (1936–8435) | 0.033 |
| sFlt1/PlGF ratio | 18.0 (5.95–58.8) | 30.3 (9.95–124) | 0.383 |
| ACE-2 (pg/mL) | 7904 (6032–16400) | 9480 (5621–28025) | 0.789 |
| ANG-II (pg/mL) | 917 (595–2381) | 549 (203–1073) | 0.061 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solis-Paredes, J.M.; Montoya-Estrada, A.; Cruz-Rico, A.; Reyes-Muñoz, E.; Perez-Duran, J.; Espino y Sosa, S.; Garcia-Salgado, V.R.; Sevilla-Montoya, R.; Martinez-Portilla, R.J.; Estrada-Gutierrez, G.; et al. Plasma Total Antioxidant Capacity and Carbonylated Proteins Are Increased in Pregnant Women with Severe COVID-19. Viruses 2022, 14, 723. https://doi.org/10.3390/v14040723
Solis-Paredes JM, Montoya-Estrada A, Cruz-Rico A, Reyes-Muñoz E, Perez-Duran J, Espino y Sosa S, Garcia-Salgado VR, Sevilla-Montoya R, Martinez-Portilla RJ, Estrada-Gutierrez G, et al. Plasma Total Antioxidant Capacity and Carbonylated Proteins Are Increased in Pregnant Women with Severe COVID-19. Viruses. 2022; 14(4):723. https://doi.org/10.3390/v14040723
Chicago/Turabian StyleSolis-Paredes, Juan Mario, Araceli Montoya-Estrada, Adriana Cruz-Rico, Enrique Reyes-Muñoz, Javier Perez-Duran, Salvador Espino y Sosa, Victor Ranferi Garcia-Salgado, Rosalba Sevilla-Montoya, Raigam Jafet Martinez-Portilla, Guadalupe Estrada-Gutierrez, and et al. 2022. "Plasma Total Antioxidant Capacity and Carbonylated Proteins Are Increased in Pregnant Women with Severe COVID-19" Viruses 14, no. 4: 723. https://doi.org/10.3390/v14040723
APA StyleSolis-Paredes, J. M., Montoya-Estrada, A., Cruz-Rico, A., Reyes-Muñoz, E., Perez-Duran, J., Espino y Sosa, S., Garcia-Salgado, V. R., Sevilla-Montoya, R., Martinez-Portilla, R. J., Estrada-Gutierrez, G., Gomez-Ruiz, J. A., Mateu-Rogell, P., Villafan-Bernal, J. R., Rojas-Zepeda, L., del Carmen Perez-Garcia, M., & Torres-Torres, J. (2022). Plasma Total Antioxidant Capacity and Carbonylated Proteins Are Increased in Pregnant Women with Severe COVID-19. Viruses, 14(4), 723. https://doi.org/10.3390/v14040723