
Monkeypox Goes North: Ongoing Worldwide Monkeypox Infections in Humans


{kind=link}
Abstract
:1. The Poxvirus Family
2. Monkeypox (MPX)
3. The 2022 MPXV Outbreak
4. Orthopoxvirus Physical Stability and Transmission
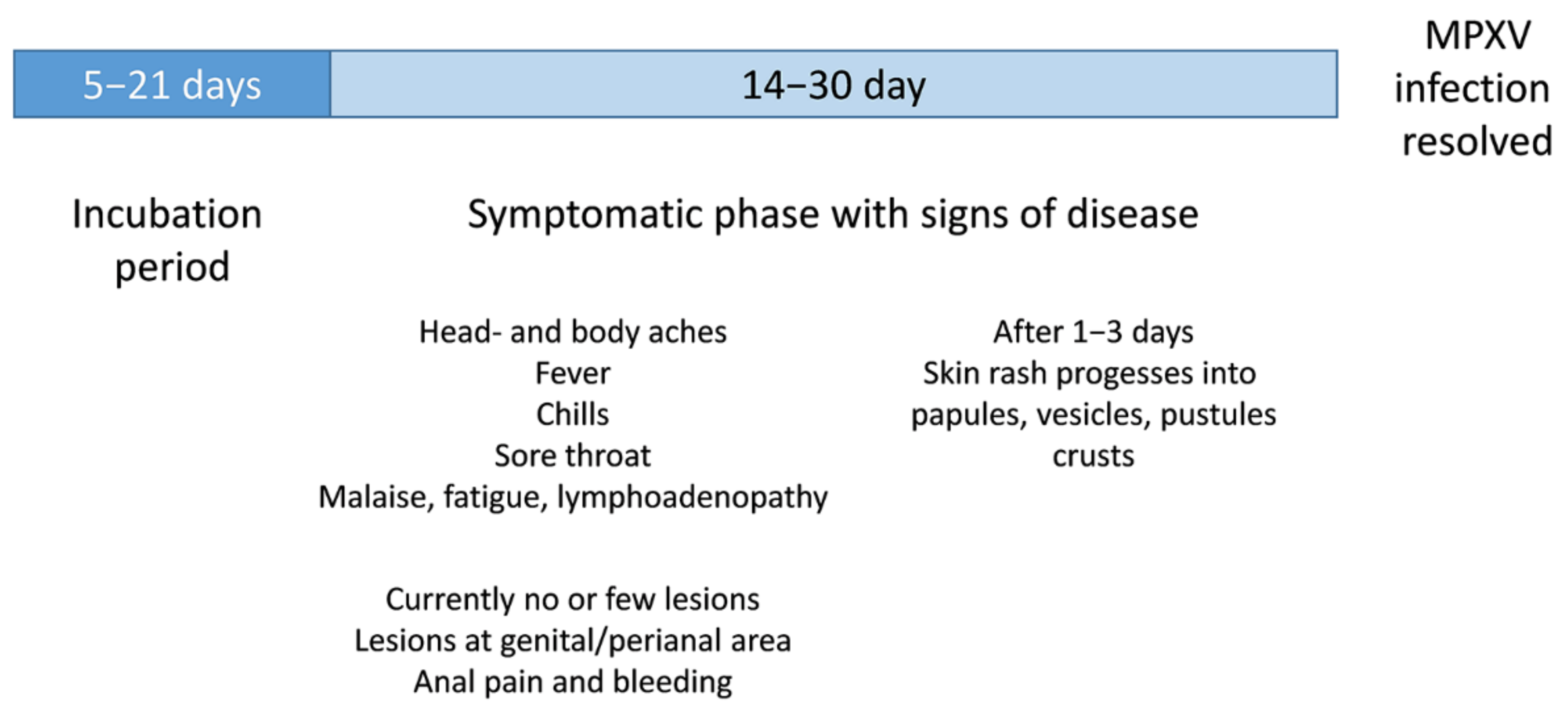
5. Clinical Disease Caused by MPXV Infections
6. Diagnostics
7. Treatment of MPXV Infections
8. Genomic Changes in the 2022 MPXV Genomes
9. Outlook
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- White, P.J.; Shackelford, P.G. Edward Jenner, MD, and the Scourge That Was. Am. J. Dis. Child. 1983, 137, 864–869. [Google Scholar] [CrossRef]
- Schmidt, F.I.; Bleck, C.K.E.; Mercer, J. Poxvirus host cell entry. Curr. Opin. Virol. 2012, 2, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Kilcher, S.; Schmidt, F.I.; Schneider, C.; Kopf, M.; Helenius, A.; Mercer, J. siRNA Screen of Early Poxvirus Genes Identifies the AAA+ ATPase D5 as the Virus Genome-Uncoating Factor. Cell Host Microbe 2014, 15, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Moss, B. Poxvirus entry and membrane fusion. Virology 2006, 344, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Moss, B. Vaccinia virus: A tool for research and vaccine development. Science 1991, 252, 1662–1667. [Google Scholar] [CrossRef]
- Payne, L.G. Significance of Extracellular Enveloped Virus in the in vitro and in vivo Dissemination of Vaccinia. J. Gen. Virol. 1980, 50, 89–100. [Google Scholar] [CrossRef]
- Von Magnus, P.; Andersen, E.K.; Petersen, K.B.; Birch-Andersen, A. A pox-Like disease in cynomolgus monkeys. Acta Pathol. Microbiol. Scand. 1959, 46, 156–176. [Google Scholar] [CrossRef]
- Ladnyj, I.D.; Ziegler, P.; Kima, E. A human infection caused by monkeypox virus in Basankusu Territory, Democratic Republic of the Congo. Bull. World Health Organ. 1972, 46, 593–597. [Google Scholar]
- Khodakevich, L.; Jezek, Z.; Messinger, D. Monkeypox virus: Ecology and public health significance. Bull. World Health Organ. 1988, 66, 747–752. [Google Scholar]
- Anderson, M.G.; Frenkel, L.D.; Homann, S.; Guffey, J. A case of severe monkeypox virus disease in an American child: Emerging infections and changing professional values. Pediatr. Infect. Dis. J. 2003, 22, 1093–1096. [Google Scholar] [CrossRef]
- Doty, J.B.; Malekani, J.M.; Kalemba, L.N.; Stanley, W.T.; Monroe, B.P.; Nakazawa, Y.U.; Mauldin, M.R.; Bakambana, T.L.; Liyandja, T.L.D.; Braden, Z.H.; et al. Assessing Monkeypox Virus Prevalence in Small Mammals at the Human-Animal Interface in the Democratic Republic of the Congo. Viruses 2017, 9, 283. [Google Scholar] [CrossRef]
- Di Giulio, D.B.; Eckburg, P.B. Human monkeypox: An emerging zoonosis. Lancet Infect. Dis. 2004, 4, 15–25. [Google Scholar] [CrossRef]
- Patrono, L.V.; Pléh, K.; Samuni, L.; Ulrich, M.; Röthemeier, C.; Sachse, A.; Muschter, S.; Nitsche, A.; Couacy-Hymann, E.; Boesch, C.; et al. Monkeypox virus emergence in wild chimpanzees reveals distinct clinical outcomes and viral diversity. Nat. Microbiol. 2020, 5, 955–965. [Google Scholar] [CrossRef]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox—A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef]
- Chen, N.; Li, G.; Liszewski, M.K.; Atkinson, J.P.; Jahrling, P.B.; Feng, Z.; Schriewer, J.; Buck, C.; Wang, C.; Lefkowitz, E.J.; et al. Virulence differences between monkeypox virus isolates from West Africa and the Congo basin. Virology 2005, 340, 46–63. [Google Scholar] [CrossRef]
- Available online: https://www.who.int/emergencies/emergency-events/item/2022-e000121 (accessed on 28 July 2022).
- Dixon, C.M. Smallpox; Little, Brown, and Company: Boston, MA, USA, 1962. [Google Scholar]
- Huq, F. Effect of temperature and relative humidity on variola virus in crusts. Bull. World Health Organ. 1976, 54, 710–712. [Google Scholar]
- Downie, A.; Dumbell, K.R. Survival of variola virus in dried exudate and crusts from smallpox patients. Lancet 1947, 249, 550–553. [Google Scholar] [CrossRef]
- Harper, G.J. Airborne micro-organisms: Survival tests with four viruses. J. Hyg. 1961, 59, 479–486. [Google Scholar] [CrossRef]
- Essbauer, S.; Meyer, H.; Porsch-Özcürümez, M.; Pfeffer, M. Long-Lasting Stability of Vaccinia Virus (Orthopoxvirus) in Food and Environmental Samples. Zoonoses Public Health 2007, 54, 118–124. [Google Scholar] [CrossRef]
- Wolff, H.L.; Croon, J.J. The survival of smallpox virus (variola minor) in natural circumstances. Bull. World Health Organ. 1968, 38, 492–493. [Google Scholar]
- World Health Organization Multi-Country Monkeypox Outbreak: Situation update. Retrieved 14 June 2022. 2022. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON393 (accessed on 28 July 2022).
- Orviz, E.; Negredo, A.; Ayerdi, O.; Vázquez, A.; Muñoz-Gomez, A.; Monzón, S.; Clavo, P.; Zaballos, A.; Vera, M.; Sánchez, P.; et al. Monkeypox outbreak in Madrid (Spain): Clinical and virological aspects. J. Infect. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Noe, S.; Zange, S.; Seilmaier, M.; Antwerpen, M.H.; Fenzl, T.; Schneider, J.; Spinner, C.D.; Bugert, J.J.; Wendtner, C.-M.; Wölfel, R. Clinical and virological features of first human monkeypox cases in Germany. Infection 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.cdc.gov/poxvirus/monkeypox/clinicians/smallpox-vaccine.html#anchor_1545415175541 (accessed on 20 August 2022).
- Gruber, M.F. Current status of monkeypox vaccines. NPJ Vaccines 2022, 7, 94. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, R.N.; Kennedy, J.S. ACAM2000: A newly licensed cell culture-based live vaccinia smallpox vaccine. Expert Opin. Investig. Drugs 2008, 17, 555–564. [Google Scholar] [CrossRef]
- Decker, M.D.; Garman, P.M.; Hughes, H.; Yacovone, M.A.; Collins, L.C.; Fegley, C.D.; Lin, G.; DiPietro, G.; Gordon, D.M. Enhanced safety surveillance study of ACAM2000 smallpox vaccine among US military service members. Vaccine 2021, 39, 5541–5547. [Google Scholar] [CrossRef]
- Brown, K.; Leggat, P.A. Human Monkeypox: Current State of Knowledge and Implications for the Future. Trop. Med. Infect. Dis. 2016, 1, 8. [Google Scholar] [CrossRef]
- Kenner, J.; Cameron, F.; Empig, C.; Jobes, D.V.; Gurwith, M. LC16m8: An attenuated smallpox vaccine. Vaccine 2006, 24, 7009–7022. [Google Scholar] [CrossRef]
- Iizuka, I.; Ami, Y.; Suzaki, Y.; Nagata, N.; Fukushi, S.; Ogata, M.; Morikawa, S.; Hasegawa, H.; Mizuguchi, M.; Kurane, I.; et al. A Single Vaccination of Nonhuman Primates with Highly Attenuated Smallpox Vaccine, LC16m8, Provides Long-term Protection against Monkeypox. Jpn. J. Infect. Dis. 2017, 70, 408–415. [Google Scholar] [CrossRef]
- Earl, P.L.; Americo, J.L.; Wyatt, L.S.; Eller, L.A.; Whitbeck, J.C.; Cohen, G.H.; Eisenberg, R.J.; Hartmann, C.J.; Jackson, D.L.; Kulesh, D.A.; et al. Immunogenicity of a highly attenuated MVA smallpox vaccine and protection against monkeypox. Nature 2004, 428, 182–185. [Google Scholar] [CrossRef]
- Overton, E.T.; Lawrence, S.J.; Stapleton, J.T.; Weidenthaler, H.; Schmidt, D.; Koenen, B.; Silbernagl, G.; Nopora, K.; Chaplin, P. A randomized phase II trial to compare safety and immunogenicity of the MVA-BN smallpox vaccine at various doses in adults with a history of AIDS. Vaccine 2020, 38, 2600–2607. [Google Scholar] [CrossRef]
- Xiao, Y.; Isaacs, S.N. Therapeutic Vaccines and Antibodies for Treatment of Orthopoxvirus Infections. Viruses 2010, 2, 2381–2403. [Google Scholar] [CrossRef]
- Adler, H.; Gould, S.; Hine, P.; Snell, L.B.; Wong, W.; Houlihan, C.F.; Osborne, J.C.; Rampling, T.; Beadsworth, M.B.; Duncan, C.J.; et al. Clinical features and management of human monkeypox: A retrospective observational study in the UK. Lancet Infect. Dis. 2022, 22, 1153–1162. [Google Scholar] [CrossRef]
- Smith, S.K.; Olson, V.A.; Karem, K.L.; Jordan, R.; Hruby, D.E.; Damon, I.K. In Vitro Efficacy of ST246 against Smallpox and Monkeypox. Antimicrob. Agents Chemother. 2009, 53, 1007–1012. [Google Scholar] [CrossRef]
- Chen, Y.; Honeychurch, K.M.; Yang, G.; Byrd, C.M.; Harver, C.; E Hruby, D.; Jordan, R. Vaccinia virus p37 interacts with host proteins associated with LE-derived transport vesicle biogenesis. Virol. J. 2009, 6, 44. [Google Scholar] [CrossRef] [Green Version]
- Lanier, R.; Trost, L.; Tippin, T.; Lampert, B.; Robertson, A.; Foster, S.; Rose, M.; Painter, W.; O’Mahony, R.; Almond, M.; et al. Development of CMX001 for the Treatment of Poxvirus Infections. Viruses 2010, 2, 2740–2762. [Google Scholar] [CrossRef]
- Isidro, J.; Borges, V.; Pinto, M.; Sobral, D.; Santos, J.D.; Nunes, A.; Mixão, V.; Ferreira, R.; Santos, D.; Duarte, S.; et al. Phylogenomic characterization and signs of microevolution in the 2022 multi-country outbreak of monkeypox virus. Nat. Med. 2022, 28, 1569–1572. [Google Scholar] [CrossRef]
- Gammon, D.B.; Gowrishankar, B.; Duraffour, S.; Andrei, G.; Upton, C.; Evans, D.H. Vaccinia Virus-Encoded Ribonucleotide Reductase Subunits Are Differentially Required for Replication and Pathogenesis. PLoS Pathog. 2010, 6, e1000984. [Google Scholar] [CrossRef]
- Wittek, R. Organization and expression of the poxvirus genome. Experientia 1982, 38, 285–297. [Google Scholar] [CrossRef]
- Roth, J.R.; Andersson, D. Poxvirus Use a “Gene Accordion” to Tune out Host Defenses. Cell 2012, 150, 671–672. [Google Scholar] [CrossRef]
- Alakunle, E.F.; Okeke, M.I. Monkeypox virus: A neglected zoonotic pathogen spreads globally. Nat. Rev. Genet. 2022, 20, 507–508. [Google Scholar] [CrossRef]
- Kremer, M.; Suezer, Y.; Martinez-Fernandez, Y.; Münk, C.; Sutter, G.; Schnierle, B.S. Vaccinia virus replication is not affected by APOBEC3 family members. Virol. J. 2006, 3, 86. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.C.; Schneider, J.; Muehlemann, B.; Veith, T.; Beheim-Schwarzbach, J.; Schmidt, M.L.; Walper, F.; Bleicker, T.; Caroline Isner, C.; Pfäfflin, F.; et al. Genetic variability, including gene du-plication and deletion, in early sequences from the 2022 European monkeypox outbreak. bioRxiv 2022. [Google Scholar] [CrossRef]
- Gigante, C.M.; Korber, B.; Seabolt, M.H.; Wilkins, K.; Davidson, W.; Rao, A.K.; Zhao, H.; Hughes, C.M.; Minhaj, F.; Waltenburg, M.A.; et al. Multiple lineages of Monkeypox virus detected in the United States, 2021–2022. bioRxiv 2022. [Google Scholar] [CrossRef]
- Benvenuto, D.; Vita, S.; Pascarella, S.; Bianchi, M.; Giovanetti, M.; Cauda, R.; Nicastri, E.; Cassone, A.; Ciccozzi, M. The evolution of Monkeypox virus: A genetic and structural analysis reveals mutations in proteins involved in host-pathogen interaction. bioRxiv 2022. [Google Scholar] [CrossRef]
- Abrahim, M.; Guterres, A.; Da Costa Neves, P.C.; Ano Bom, A.P.D. The emergence of new lineages of the Monkeypox virus could affect the 2022 outbreak. bioRxiv 2022. [Google Scholar] [CrossRef]
- Desingu, P.A.; Nagarajan, K. Genomic regions insertion and deletion in Monkeypox virus causing multi-country out-break-2022. bioRxiv 2022. [Google Scholar] [CrossRef]
- Giorgi, F.M.; Pozzobon, D.; Di Meglio, A.; Mercatelli, D. Genomic analysis of the recent monkeypox outbreak. bioRxiv 2022. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schnierle, B.S. Monkeypox Goes North: Ongoing Worldwide Monkeypox Infections in Humans. Viruses 2022, 14, 1874. https://doi.org/10.3390/v14091874
Schnierle BS. Monkeypox Goes North: Ongoing Worldwide Monkeypox Infections in Humans. Viruses. 2022; 14(9):1874. https://doi.org/10.3390/v14091874
Chicago/Turabian StyleSchnierle, Barbara S. 2022. "Monkeypox Goes North: Ongoing Worldwide Monkeypox Infections in Humans" Viruses 14, no. 9: 1874. https://doi.org/10.3390/v14091874
APA StyleSchnierle, B. S. (2022). Monkeypox Goes North: Ongoing Worldwide Monkeypox Infections in Humans. Viruses, 14(9), 1874. https://doi.org/10.3390/v14091874