
Hantavirus in Panama: Twenty Years of Epidemiological Surveillance Experience

 ,
,  ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Definition
2.2. Data Collection
2.3. Spatial Distribution
2.4. Statistical Analyses
3. Results
3.1. Geographical Distribution
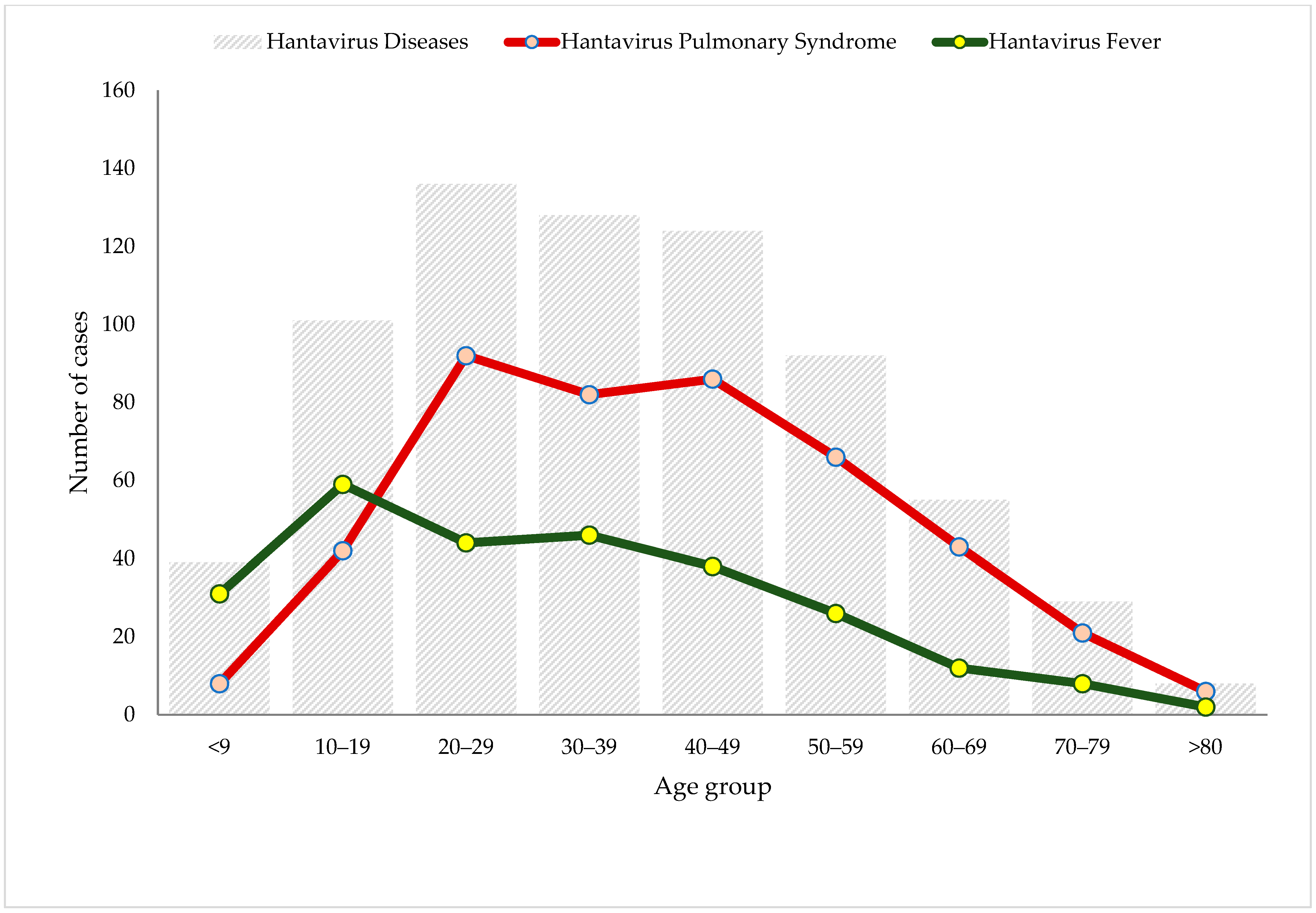
3.2. Demographic Characteristics and Disease Spectrum
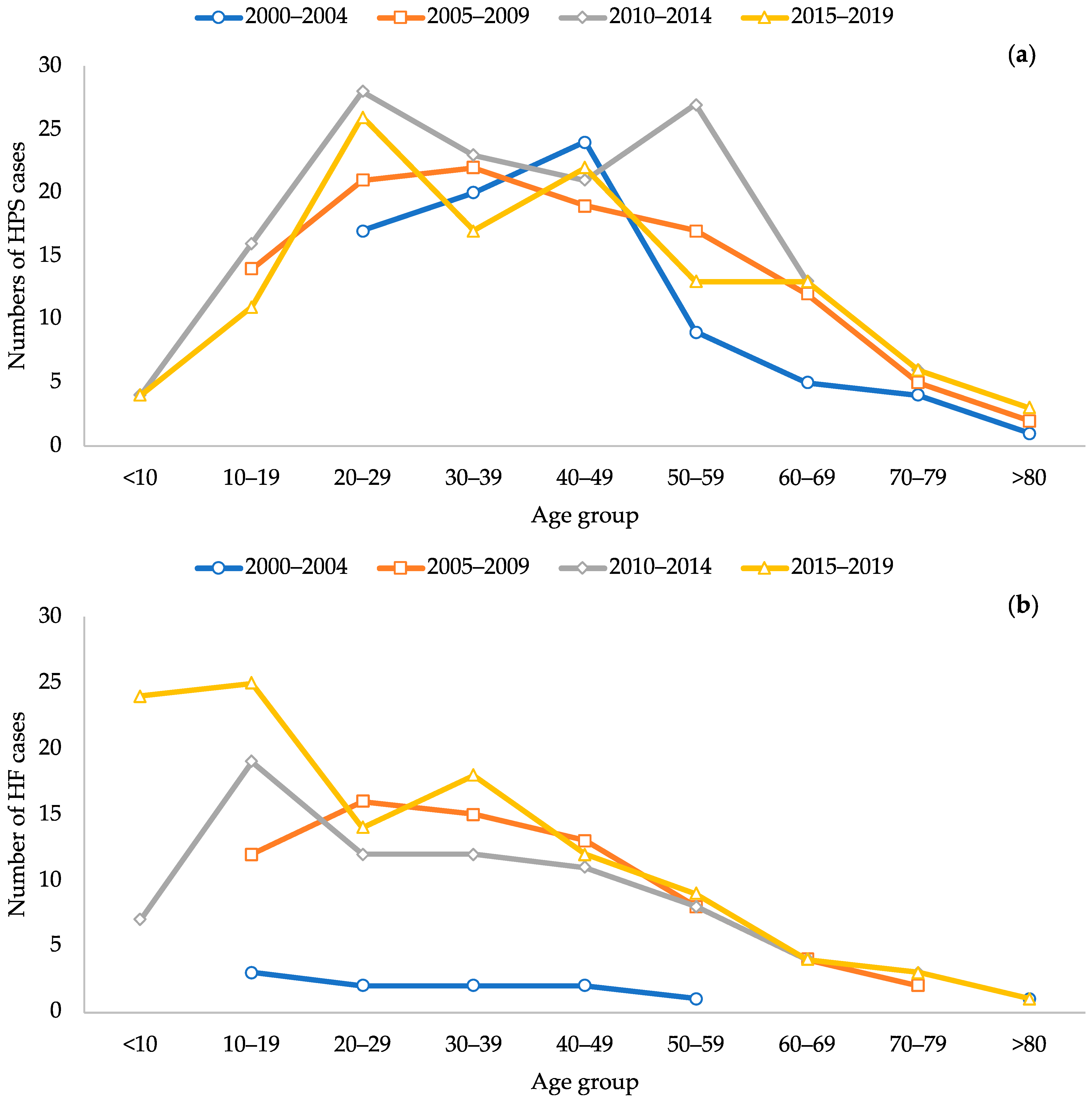
3.3. Temporal Distribution and Rates of Incidence, Case-Fatality Rate and Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nichol, S.T.; Spiropoulou, C.F.; Morzunov, S.; Rollin, P.E.; Ksiazek, T.G.; Feldmann, H.; Sanchez, A.; Childs, J.; Zaki, S.; Peters, C.J. Genetic Identification of a Hantavirus Associated with an Outbreak of Acute Respiratory Illness. Science (1979) 1993, 262, 914–917. [Google Scholar] [CrossRef]
- Childs, J.E.; Ksiazek, T.G.; Spiropoulou, C.F.; Krebs, J.W.; Morzunov, S.; Maupin, G.O.; Gage, K.L.; Rollin, P.E.; Sarisky, J.; Enscore, R.E.; et al. Serologic and Genetic Identification of Peromyscus maniculatus as the Primary Rodent Reservoir for a New Hantavirus in the Southwestern United States. J. Infect. Dis. 1994, 169, 1271–1280. [Google Scholar] [CrossRef] [Green Version]
- Milholland, M.T.; Castro-Arellano, I.; Suzán, G.; Garcia-Peña, G.E.; Lee, T.E.; Rohde, R.E.; Alonso Aguirre, A.; Mills, J.N. Global Diversity and Distribution of Hantaviruses and Their Hosts. Ecohealth 2018, 15, 163–208. [Google Scholar] [CrossRef]
- Yanagihara, R.; Gu, S.H.; Arai, S.; Kang, H.J.; Song, J.W. Hantaviruses: Rediscovery and New Beginnings. Virus Res. 2014, 187, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Martinez, V.P.; Bellomo, C.; San Juan, J.; Pinna, D.; Forlenza, R.; Elder, M.; Padula, P.J. Person-to-Person Transmission of Andes Virus. Emerg. Infect. Dis. 2005, 11, 1848–1853. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Valdebenito, C.; Calvo, M.; Vial, C.; Mansilla, R.; Marco, C.; Palma, R.E.; Vial, P.A.; Valdivieso, F.; Mertz, G.; Ferrés, M. Person-to-Person Household and Nosocomial Transmission of Andes Hantavirus, Southern Chile, 2011. Emerg. Infect. Dis. 2014, 20, 1629–1636. [Google Scholar] [CrossRef] [PubMed]
- Ferrés, M.; Vial, P.; Marco, C.; Yañez, L.; Godoy, P.; Castillo, C.; Hjelle, B.; Delgado, I.; Lee, S.J.; Mertz, G.J. Prospective Evaluation of Household Contacts of Persons with Hantavirus Cardiopulmonary Syndrome in Chile. J. Infect. Dis. 2007, 195, 1563–1571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso, D.O.; Pérez-Sautu, U.; Bellomo, C.M.; Prieto, K.; Iglesias, A.; Coelho, R.; Periolo, N.; Domenech, I.; Talmon, G.; Hansen, R.; et al. Person-to-Person Transmission of Andes Virus in Hantavirus Pulmonary Syndrome, Argentina, 2014. Emerg. Infect. Dis. 2020, 26, 756–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padula, P.J.; Edelstein, A.; Miguel, S.D.L.; Lo  Pez, N.M.; Rossi, C.M.; Rabinovich, R.D. Hantavirus Pulmonary Syndrome Outbreak in Argentina: Molecular Evidence for Person-to-Person Transmission of Andes Virus. Virology 1998, 241, 323–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toledo, J.; Haby, M.M.; Reveiz, L.; Sosa Leon, L.; Angerami, R.; Aldighieri, S. Evidence for Human-to-Human Transmission of Hantavirus: A Systematic Review. J. Infect. Dis. 2022, 226, 1362–1371. [Google Scholar] [CrossRef]
- Tian, H.; Stenseth, N.C. The Ecological Dynamics of Hantavirus Diseases: From Environmental Variability to Disease Prevention Largely Based on Data from China. PLoS Negl. Trop. Dis. 2019, 13, e0006901. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, J.H.; Bradfute, S.B.; Calisher, C.H.; Klempa, B.; Klingström, J.; Laenen, L.; Palacios, G.; Schmaljohn, C.S.; Tischler, N.D.; Maes, P. Pending Reorganization of Hantaviridae to Include Only Completely Sequenced Viruses: A Call to Action. Viruses 2023, 15, 660. [Google Scholar] [CrossRef]
- Bayard, V.; Kitsutani, P.; Barria, E.; Ruedas, L.; Tinnin, D.; Muñoz, C.; Mosca, I.; Guerrero, G.; Kant, R.; Garcia, A.; et al. Outbreak of Hantavirus Pulmonary Syndrome, Los Santos, Panama, 1999–2000. Emerg. Infect. Dis. 2004, 10, 1635–1642. [Google Scholar] [CrossRef]
- Vincent, M.J.; Quiroz, E.; Gracia, F.; Sanchez, A.J.; Ksiazek, T.G.; Kitsutani, P.T.; Ruedas, L.A.; Tinnin, D.S.; Caceres, L.; Garcia, A.; et al. Hantavirus Pulmonary Syndrome in Panama: Identification of Novel Hantaviruses and Their Likely Reservoirs. Virology 2000, 277, 14–19. [Google Scholar] [CrossRef] [Green Version]
- Ruedas, L.; Salazar-Bravo, J.; Tinnin, D.; Armien, B.; Caceres, L.; Garcia, A.; Diaz, M.A.; Gracia, F.; Suzan, G.; Peters, C.; et al. Community Ecology of Small Mammal Populations in Panama Following an Outbreak of Hantavirus Pulmonary Syndrome. J. Vector Ecol. 2004, 29, 177–191. [Google Scholar] [PubMed]
- Hanson, J.D.; Utrera, A.; Fulhorst, C.F. The Delicate Pygmy Rice Rat (Oligoryzomys delicatus) Is the Principal Host of Maporal Virus (Family Bunyaviridae, Genus Hantavirus). Vector-Borne Zoonotic Dis. 2011, 11, 691–695. [Google Scholar] [CrossRef] [Green Version]
- Armién, A.G.; Armién, B.; Koster, F.; Pascale, J.M.; Avila, M.; Gonzalez, P.; de la Cruz, M.; Zaldivar, Y.; Mendoza, Y.; Gracia, F.; et al. Hantavirus Infection and Habitat Associations among Rodent Populations in Agroecosystems of Panama: Implications for Human Disease Risk. Am. J. Trop. Med. Hyg. 2009, 81, 59–66. [Google Scholar] [CrossRef]
- Armien, B.; Pascale, J.M.; Munoz, C.; Marinas, J.; Núnez, H.; Herrera, M.; Trujillo, J.; Sánchez, D.; Mendoza, Y.; Hjelle, B.; et al. Hantavirus Fever without Pulmonary Syndrome in Panama. Am. J. Trop. Med. Hyg. 2013, 89, 489–494. [Google Scholar] [CrossRef]
- MINSA-ICGES. Guia de Manejo de La Enfermedad Por Hantavirus En Panamá; Instituto Conmemorativo Gorgas de Estudios de la Salud: Panama City, Panama, 2016. [Google Scholar]
- MINSA-Panamá. Guía Nacional de Epidemiología—Ministerio de Salud, Panamá; Ministerio de Salud: Panama City, Panama, 2004. [Google Scholar]
- Gonzalez, P.; Salinas, T.; Salazar, J.R.; Avila, M.; Colella, J.P.; Dunnum, J.L.; Glass, G.E.; Gonzalez, G.; Juarez, E.; Lindblade, K.; et al. Two Decades of Wildlife Pathogen Surveillance: Case Study of Choclo Orthohantavirus and Its Wild Reservoir Oligoryzomys costaricensis. Viruses, 2023; in press. [Google Scholar]
- Bayard, V.; Ortega, E.; Garcia, A.; Caceres, L.; Castillo, Z.; Quiroz, E.; Armien, B.; Gracia, F. Hantavirus Pulmonary Syndrome--Panama, 1999–2000. MMWR Morb. Mortal. Wkly. Rep. 2000, 49, 205–207. [Google Scholar] [CrossRef]
- Salazar-Bravo, J.; Armién, B.; Suzán, G.; Armién, A.; Ruedas, L.A.; Avila, M.; Zaldívar, Y.; Pascale, J.M.; Gracia, F.; Yates, T.L. Serosurvey of Wild Rodents for Hantaviruses in Panama, 2000–2002. J. Wildl. Dis. 2004, 40, 103–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, R.; Cañate, R.; Pascale, J.M.; Dragoo, J.W.; Armien, B.; Armien, A.G.; Koster, F. Confirmation of Choclo Virus as the Cause of Hantavirus Cardiopulmonary Syndrome and High Serum Antibody Prevalence in Panama. J. Med. Virol. 2010, 82, 1586–1593. [Google Scholar] [CrossRef] [Green Version]
- Hesse, S.; Nuñez, H.; Salazar, J.R.; Salinas, T.P.; Barrera, E.; Chong, R.; Torres, S.; Cumbrera, A.; Olivares, I.; Junco, A.; et al. Case Report: First Confirmed Case of Coinfection of SARS-CoV-2 With Choclo Orthohantavirus. Front. Trop. Dis. 2021, 2, 39. [Google Scholar] [CrossRef]
- Jonsson, C.B.; Figueiredo, L.T.; Vapalahti, O. A Global Perspective on Hantavirus Ecology, Epidemiology, and Disease. Clin. Microbiol. Rev. 2010, 23, 412–441. [Google Scholar] [CrossRef] [Green Version]
- Pan American Health Organization. Hantavirus in the Americas: Guidelines for Diagnosis, Treatment, Prevention, and Control; Pan American Health Organization, Pan American Sanitary Bureau, Regional Office of the World Health Organization: Washington, DC, USA, 1999; ISBN 9275130477. [Google Scholar]
- MINSAL-Chile. Guía Clínica de Prevención, Diagnóstico y Tratamiento Del Síndrome Cardiopulmonar Por Hantavirus; Ministerio de Salud de Chile: Santiago City, Chile, 2013. [Google Scholar]
- MINSAL-Chile. Circular B51-24 Vigilancia y Control Hanta—Ministerio de Salud de Chile; Ministerio de Salud de Chile: Santiago City, Chile, 2012. [Google Scholar]
- MacNeil, A.; Ksiazek, T.G.; Rollin, P.E. Hantavirus Pulmonary Syndrome, United States, 1993–2009. Emerg. Infect. Dis. 2011, 17, 1195–1201. [Google Scholar] [CrossRef]
- Torales, M.; Martínez, B.; Román, J.; Rojas, K.; de Egea, V.; Torres, J.; Vázquez, C.; Sequera, G. Actualización de Áreas de Riesgo y Perfil Epidemiológico de Hantavirus En Paraguay (2013–2020). Mem. Del Inst. Investig. En Cienc. La Salud 2022, 20, 108–116. [Google Scholar] [CrossRef]
- Martinez, V.P.; Bellomo, C.M.; Cacace, M.L.; Suárez, P.; Bogni, L.; Padula, P.J. Hantavirus Pulmonary Syndrome in Argentina, 1995–2008. Emerg. Infect. Dis. 2010, 16, 1853–1860. [Google Scholar] [CrossRef]
- Reyes Zaldívar, F.T.; Ferrés, M. Hantavirus: Descripción de Dos Décadas de Endemia y Su Letalidad. ARS Med. Rev. Cienc. Médicas 2019, 44, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, L.T.M.; de Souza, W.M.; Ferrés, M.; Enria, D.A. Hantaviruses and Cardiopulmonary Syndrome in South America. Virus Res. 2014, 187, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Armién, B.; Ortiz, P.L.; Gonzalez, P.; Cumbrera, A.; Rivero, A.; Avila, M.; Armién, A.G.; Koster, F.; Glass, G. Spatial-Temporal Distribution of Hantavirus Rodent-Borne Infection by Oligoryzomys fulvescens in the Agua Buena Region—Panama. PLoS Negl. Trop. Dis. 2016, 10, e0004460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz, Y.; Chen-Germán, M.; Quiroz, E.; Carrera, J.-P.; Cisneros, J.; Moreno, B.; Cerezo, L.; Martinez-Torres, A.O.; Moreno, L.; De Mosca, I.B.; et al. Molecular Epidemiology of Dengue in Panama: 25 Years of Circulation. Viruses 2019, 11, 764. [Google Scholar] [CrossRef] [Green Version]
- Hurtado, L.; Cumbrera, A.; Rigg, C.; Perea, M.; Santamaría, A.M.; Chaves, L.F.; Moreno, D.; Romero, L.; Lasso, J.; Caceres, L.; et al. Long-Term Transmission Patterns and Public Health Policies Leading to Malaria Elimination in Panamá. Malar. J. 2020, 19, 265. [Google Scholar] [CrossRef] [PubMed]
- MINSA-Panama. Informe de Malaria: Semana: No. 49 (02-01-2022 a 10-12-2022) Ministerio de Salud; Ministerio de Salud: Panama City, Panama, 2022. [Google Scholar]
- MINSA-Panama. Guia de Leishmaniasis 2015; Ministerio de Salud: Panama City, Panama, 2015; pp. 1–65. [Google Scholar]
- Salinas, T.P.; Garrido, J.L.; Salazar, J.R.; Gonzalez, P.; Zambrano, N.; Fuentes-Villalobos, F.; Bravo, F.; Fica-Leon, V.; Salas-Burgos, A.; Calvo, M.; et al. Cytokine Profiles and Antibody Response Associated to Choclo Orthohantavirus Infection. Front. Immunol. 2021, 12, 603228. [Google Scholar] [CrossRef] [PubMed]
- Armien, B.; Pascale, J.M.; Bayard, V.; Munoz, C.; Mosca, I.; Guerrero, G.; Armien, A.; Quiroz, E.; Castillo, Z.; Zaldivar, Y.; et al. High Seroprevalence of Hantavirus Infection on the Azuero Peninsula of Panama. Am. J. Trop. Med. Hyg. 2004, 70, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Armien, B.; Pascale, J.M.; Munoz, C.; Lee, S.J.; Choi, K.L.; Avila, M.; Broce, C.; Armien, A.G.; Gracia, F.; Hjelle, B.; et al. Incidence Rate for Hantavirus Infections without Pulmonary Syndrome, Panama. Emerg. Infect. Dis. 2011, 17, 1936–1939. [Google Scholar] [CrossRef]
- Hjelle, B.; Jenison, S.; Torrez-martinez, N.; Herring, B.; Quan, S.; Polito, A.; Pichuantes, S.; Yamada, T.; Morris, C.; Elgh, F.; et al. Rapid and Specific Detection of Sin Nombre Virus Antibodies in Patients with Hantavirus Pulmonary Syndrome by a Strip Immunoblot Assay Suitable for Field Diagnosis. J. Clin. Microbiol. 1997, 35, 600–608. [Google Scholar] [CrossRef] [Green Version]
- Bermúdez, S.E.; Domínguez, L.; Suárez, J.A.; Daza, C.; Cumbrera, A.; González, J. Pasado y Presente de Las Rickettsiosis En Panamá; Instituto Conmemorativo Gorgas de Estudios de la Salud: Panama City, Panama, 2018. [Google Scholar]
- Vazquez Guillamet, L.J.; Arauz, A.B.; Suarez, J.A.; Gonzalez, E.; de Obaldıa, J.D.; Moreno, D.; Henostroza, G.; Armien, B. Leptospirosis: Epidemiological and Clinical Characteristics at the National Reference Hospital in Panama. Am. J. Trop. Med. Hyg. 2022, 107, 1261–1266. [Google Scholar] [CrossRef]
- Khaddour, K.; Sikora, A.; Tahir, N.; Nepomuceno, D.; Huang, T. Case Report: The Importance of Novel Coronavirus Disease (COVID-19) and Coinfection with Other Respiratory Pathogens in the Current Pandemic. Am. J. Trop. Med. Hyg. 2020, 102, 1208–1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Endemic Area | |||||
|---|---|---|---|---|---|---|
| Coclé | Herrera | Los Santos | Veraguas | Panamá | Total | |
| n | 49 | 22 | 550 | 84 | 7 | 712 # |
| Male sex (%) | 57.1 | 45.5 | 55.6 | 64.3 | 57.1 | 56.5 |
| Mean age (±SD) years | 40.2 (±15.0) | 45.3 (±15.9) | 36.3 (±19.1) | 38.6 (±17.1) | 45.6 (±16.4) | 37.1 (±18.5) |
| Age group | ||||||
| <18 years | 3 | 0 | 103 | 10 | 1 | 117 |
| ≥18 years | 46 | 22 | 447 | 74 | 6 | 595 |
| Spectrum | ||||||
| Hantavirus fever | 9 | 2 | 234 | 21 | 0 | 266 |
| <18 years | 0 | 0 | 73 | 6 | 0 | 79 |
| ≥18 years | 9 | 2 | 161 | 15 | 0 | 187 |
| Hantavirus pulmonary syndrome | 40 | 20 | 316 | 63 | 7 | 446 |
| <18 years | 3 | 0 | 30 | 4 | 1 | 38 |
| ≥18 years | 37 | 20 | 286 | 59 | 6 | 408 |
| Deaths | 12 * | 4 * | 29 | 8 | 3 | 56 |
| <18 years | 2 | 0 | 0 | 0 | 1 | 3 |
| ≥18 years | 10 | 4 | 29 | 8 | 2 | 53 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armién, B.; Muñoz, C.; Cedeño, H.; Salazar, J.R.; Salinas, T.P.; González, P.; Trujillo, J.; Sánchez, D.; Mariñas, J.; Hernández, A.; et al. Hantavirus in Panama: Twenty Years of Epidemiological Surveillance Experience. Viruses 2023, 15, 1395. https://doi.org/10.3390/v15061395
Armién B, Muñoz C, Cedeño H, Salazar JR, Salinas TP, González P, Trujillo J, Sánchez D, Mariñas J, Hernández A, et al. Hantavirus in Panama: Twenty Years of Epidemiological Surveillance Experience. Viruses. 2023; 15(6):1395. https://doi.org/10.3390/v15061395
Chicago/Turabian StyleArmién, Blas, Carlos Muñoz, Hector Cedeño, Jacqueline R. Salazar, Tybbyssay P. Salinas, Publio González, José Trujillo, Deyanira Sánchez, Jamileth Mariñas, Ayvar Hernández, and et al. 2023. "Hantavirus in Panama: Twenty Years of Epidemiological Surveillance Experience" Viruses 15, no. 6: 1395. https://doi.org/10.3390/v15061395
APA StyleArmién, B., Muñoz, C., Cedeño, H., Salazar, J. R., Salinas, T. P., González, P., Trujillo, J., Sánchez, D., Mariñas, J., Hernández, A., Cruz, H., Villarreal, L. Y., Grimaldo, E., González, S., Nuñez, H., Hesse, S., Rivera, F., Edwards, G., Chong, R., ... de Mosca, I. (2023). Hantavirus in Panama: Twenty Years of Epidemiological Surveillance Experience. Viruses, 15(6), 1395. https://doi.org/10.3390/v15061395