
Molecular and Entomological Characterization of 2023 Dengue Outbreak in Dhading District, Central Nepal

 , , , , and add
Show full author list
, , , , and add
Show full author list
Abstract
:1. Introduction
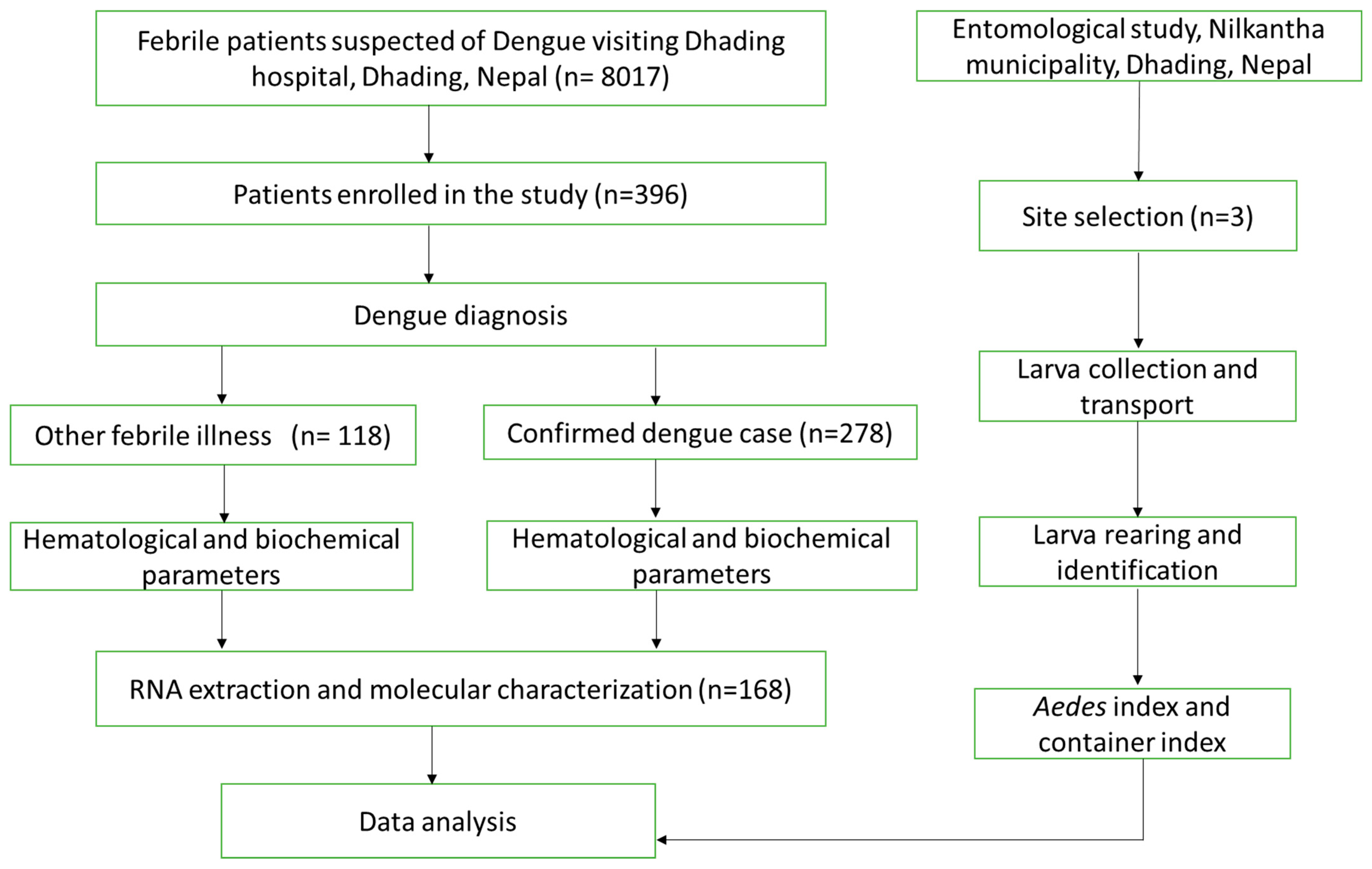
2. Materials and Methods
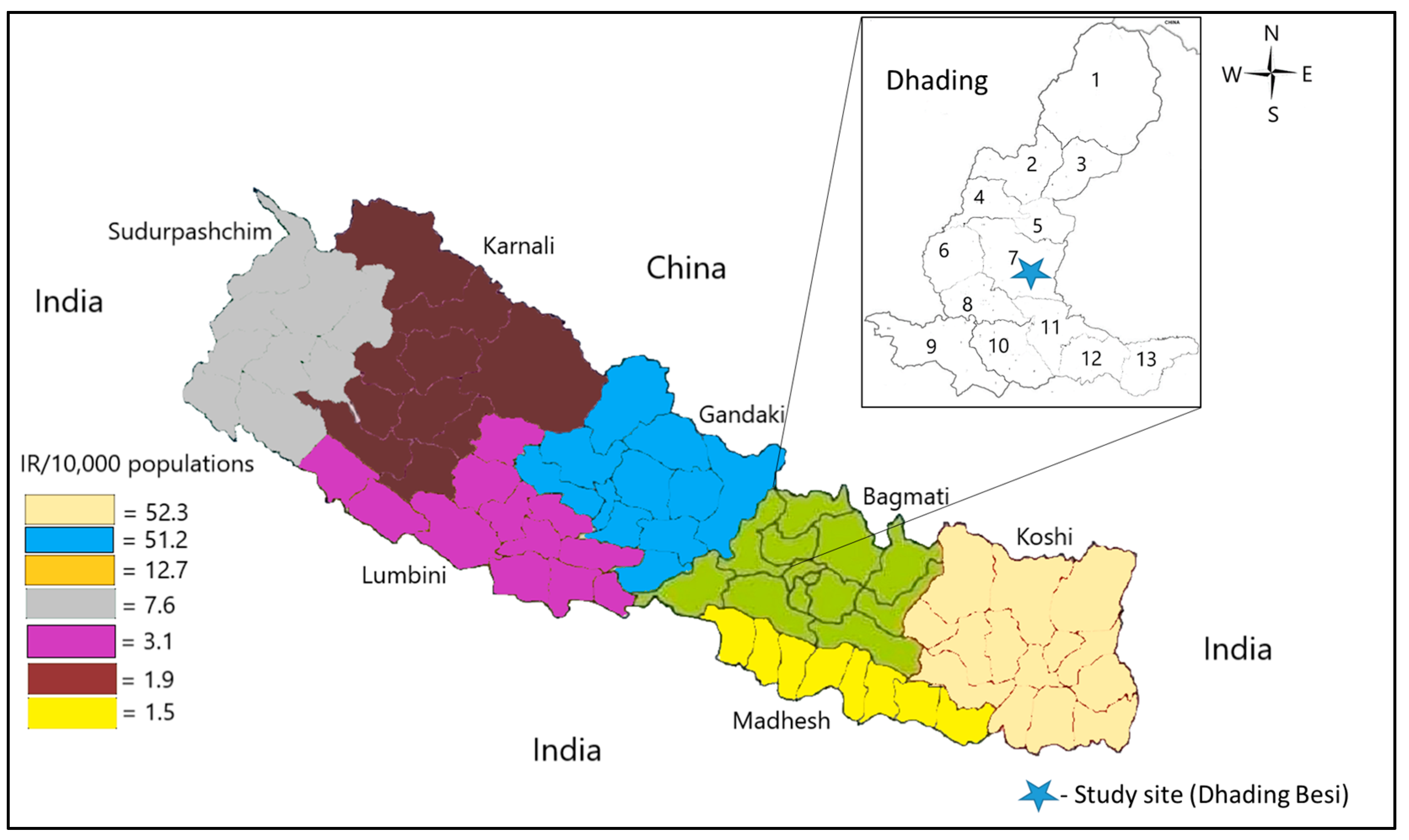
2.1. Study Design and Setting
2.2. Human Component
2.2.1. Patient Enrollment, Questionnaire, and Sample Collection
2.2.2. Dengue Diagnosis
2.2.3. Viral RNA Extraction
2.2.4. One-Step Reverse Transcription Polymerase Chain Reaction (RT-PCR)
2.3. Entomological Component
2.3.1. Site Selection
2.3.2. Larva/Pupa Collection and Transport
2.3.3. Larva/Pupa Rearing and Adult Identification
2.3.4. Estimation of Mosquito Distribution and Its Density
2.4. Data Analysis
3. Results
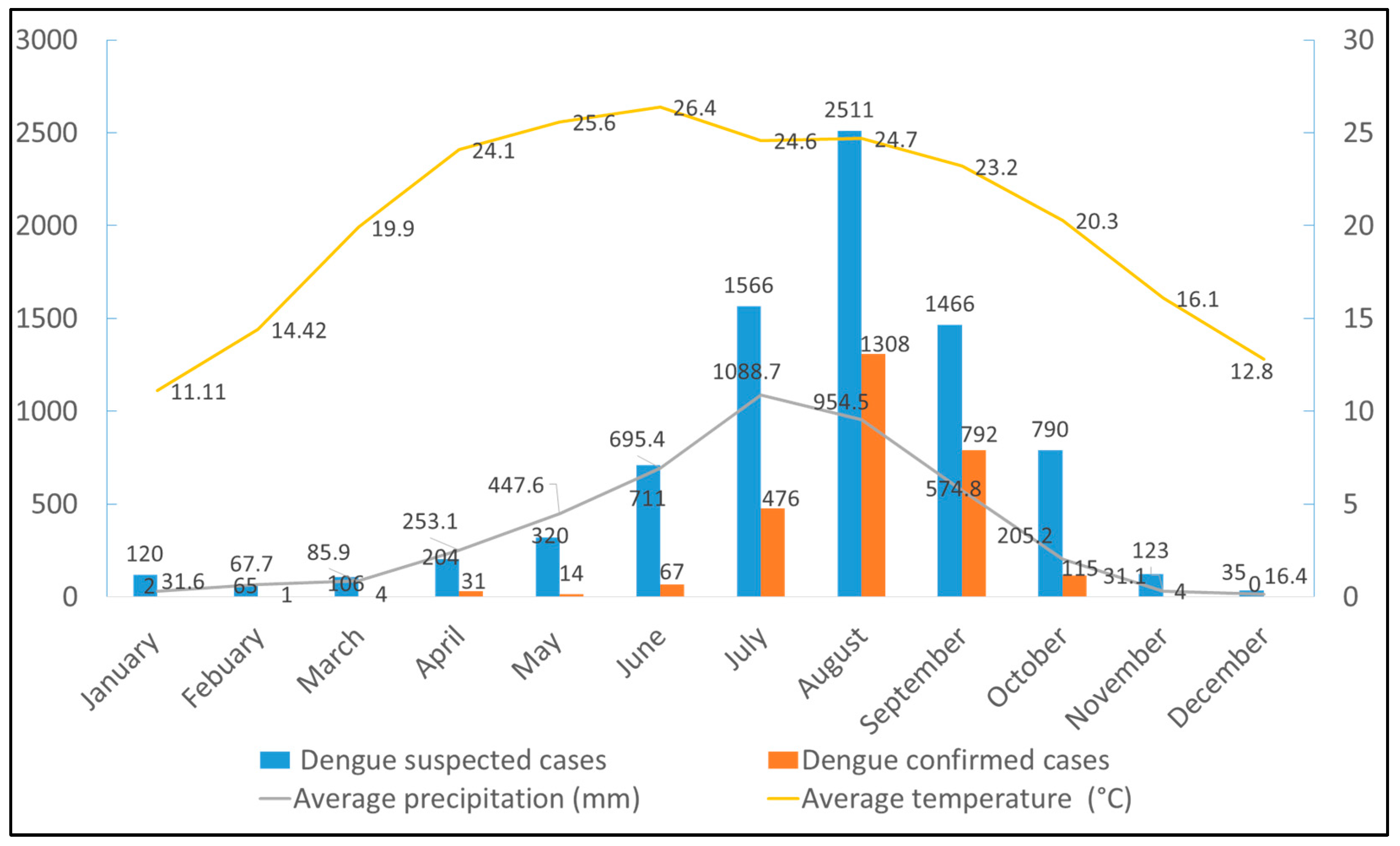
3.1. Seasonality Trend of Dengue and Climatic Conditions in Dhading, Nepal, 2023
3.2. Demographic, Clinical, and Laboratory Parameters of Dengue Patients
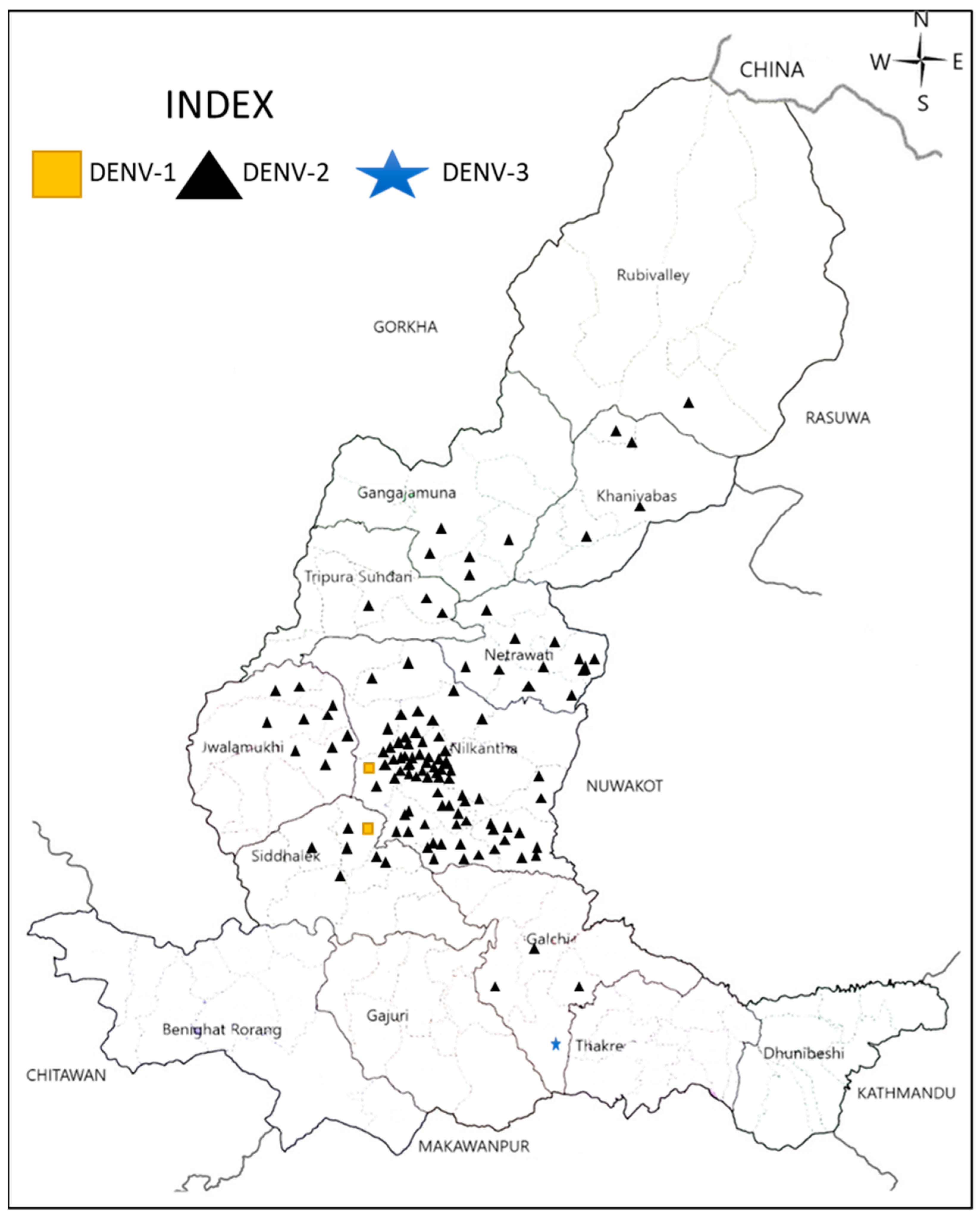
3.3. Distribution of Circulating DENV Serotypes in Dhading, Nepal, 2023
3.4. Mosquito Vector Distribution in the Selected Areas of Dhading during 2023 Dengue Outbreak
3.5. Mosquito Density by Its Habitat
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Gubler, D.; Nalim, S.; Eram, S. Epidemic dengue hemorrhagic fever in rural indonesia. III. Entomological studies. Am. J. Trop. Med. Hyg. 1979, 28, 717–724. [Google Scholar] [CrossRef]
- WHO. Dengue and Severe Dengue Key Facts; World Health Organization: Geneva, Switzerland, 2018.
- Halstead, S.B. Pathogenesis of dengue: Challenges to molecular biology. Science 1988, 239, 476–481. [Google Scholar] [CrossRef]
- Brady, O.J.; Hay, S.I. The global expansion of dengue: How Aedes aegypti mosquitoes enabled the first pandemic arbovirus. Annu. Rev. Entomol. 2020, 65, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Messina, J.P.; Brady, O.J.; Golding, N.; Kraemer, M.U.; Wint, G.W.; Ray, S.E.; Pigott, D.M.; Shearer, F.M.; Johnson, K.; Earl, L. The current and future global distribution and population at risk of dengue. Nat. Microbiol. 2019, 4, 1508–1515. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Sharif, N.; Sharif, N.; Khan, A.; Dey, S.K. The epidemiologic and clinical characteristics of the 2023 dengue outbreak in Bangladesh. In Open Forum Infectious Diseases; Oxford University Press US: Cary, NC, USA, 2024; p. ofae066. [Google Scholar]
- Takasaki, T.; Kotaki, A.; Nishimura, K.; Sato, Y.; Tokuda, A.; Lim, C.K.; Ito, M.; Tajima, S.; Nerome, R.; Kurane, I. Dengue virus type 2 isolated from an imported dengue patient in japan: First isolation of dengue virus from nepal. J. Travel Med. 2008, 15, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Pandey, B.D.; Rai, S.K.; Morita, K.; Kurane, I. First case of dengue virus infection in nepal. Nepal Med. Coll. J. 2004, 6, 157–159. [Google Scholar]
- Malla, S.; Thakur, G.D.; Shrestha, S.K.; Banjeree, M.K.; Thapa, L.B.; Gongal, G.; Ghimire, P.; Upadhyay, B.P.; Gautam, P.; Khanal, S.; et al. Identification of all dengue serotypes in nepal. Emerg. Infect. Dis. 2008, 14, 1669–1670. [Google Scholar] [CrossRef]
- Pandey, B.D.; Nabeshima, T.; Pandey, K.; Rajendra, S.P.; Shah, Y.; Adhikari, B.R.; Gupta, G.; Gautam, I.; Tun, M.M.; Uchida, R. First isolation of dengue virus from the 2010 epidemic in nepal. Trop. Med. Health 2013, 41, 103–111. [Google Scholar] [CrossRef]
- Poudyal, P.; Sharma, K.; Dumre, S.P.; Bastola, A.; Chalise, B.S.; Shrestha, B.; Poudel, A.; Giri, A.; Bhandari, P.; Shah, Y. Molecular study of 2019 dengue fever outbreaks in nepal. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 619–626. [Google Scholar] [CrossRef]
- Ngwe Tun, M.M.; Muthugala, R.; Nabeshima, T.; Soe, A.M.; Dumre, S.P.; Rajamanthri, L.; Jayawardana, D.; Attanayake, S.; Inoue, S.; Morita, K. Complete genome analysis and characterization of neurotropic dengue virus 2 cosmopolitan genotype isolated from the cerebrospinal fluid of encephalitis patients. PLoS ONE 2020, 15, e0234508. [Google Scholar] [CrossRef]
- Dumre, S.P.; Acharya, D.; Lal, B.K.; Brady, O.J. Dengue virus on the rise in nepal. Lancet Infect. Dis. 2020, 20, 889–890. [Google Scholar] [CrossRef] [PubMed]
- Rimal, S.; Shrestha, S.; Pandey, K.; Nguyen, T.V.; Bhandari, P.; Shah, Y.; Acharya, D.; Adhikari, N.; Rijal, K.R.; Ghimire, P. Co-circulation of dengue virus serotypes 1, 2, and 3 during the 2022 dengue outbreak in nepal: A cross-sectional study. Viruses 2023, 15, 507. [Google Scholar] [CrossRef]
- Gyawali, N.; Johnson, B.J.; Dixit, S.M.; Devine, G.J. Patterns of dengue in nepal from 2010–2019 in relation to elevation and climate. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 741–749. [Google Scholar] [CrossRef]
- Acharya, B.K.; Cao, C.; Xu, M.; Khanal, L.; Naeem, S.; Pandit, S. Present and future of dengue fever in nepal: Mapping climatic suitability by ecological niche model. Int. J. Environ. Res. Public Health 2018, 15, 187. [Google Scholar] [CrossRef] [PubMed]
- EDCD. Situation Updates of Dengue 2023; Epidemiology and Disease Control Division: Kathmandu, Nepal, 2023.
- Rauniyar, R.; Prajapati, S.; Manandhar, B.; Bastola, A.; Chalise, B.S.; Shrestha, S.; Khanal, C.; Thapa, M.; Napit, R.; Bajracharya, A.M. Dengue virus infection during window period of consecutive outbreaks in nepal and assessment of clinical parameters. Sci. Rep. 2023, 13, 9262. [Google Scholar] [CrossRef]
- Darsie, R., Jr.; Pradhan, S. The mosquitoes of nepal: Their identification, distribution and biology. Mosq. Syst. 1990, 22, 69–130. [Google Scholar]
- Peters, W.; Dewar, S.C. A preliminary record of the megarhine and culicine mosquitoes of nepal with notes on their taxonomy (diptera: Culicidae). Indian J. Malariol. 1956, 10, 37–51. [Google Scholar]
- Dhimal, M.; Gautam, I.; Joshi, H.D.; O’Hara, R.B.; Ahrens, B.; Kuch, U. Risk factors for the presence of chikungunya and dengue vectors (Aedes aegypti and Aedes albopictus), their altitudinal distribution and climatic determinants of their abundance in central Nepal. PLoS Neglected Trop. Dis. 2015, 9, e0003545. [Google Scholar] [CrossRef]
- Zuckerman, N.S.; Schwartz, E.; Pandey, P.; Erster, O.; Halpern, O.; Bucris, E.; Morad-Eliyahu, H.; Wax, M.; Lustig, Y. Dengue types 1 and 3 identified in travelers returning from Kathmandu, Nepal, during the October 2022 outbreak are related to strains recently identified in India. Viruses 2023, 15, 2334. [Google Scholar] [CrossRef]
- Knudsen, A.B.; Slooff, R. Vector-borne disease problems in rapid urbanization: New approaches to vector control. Bull. World Health Organ. 1992, 70, 1. [Google Scholar]
- Claeys, C.; Robles, C.; Bertaudiere-Montes, V.; Deschamps-Cottin, M.; Megnifo, H.T.; Pelagie-Moutenda, R.; Jeannin, C.; Sonor, F.; Dollin, C.; Sense, M. Socio-ecological factors contributing to the exposure of human populations to mosquito bites that transmit dengue fever, chikungunya and zika viruses: A comparison between mainland france and the french antilles. Environ. Risques Santé 2016, 15, 318–325. [Google Scholar] [CrossRef]
- Li, C.; Lu, Y.; Liu, J.; Wu, X. Climate change and dengue fever transmission in China: Evidences and challenges. Sci. Total Environ. 2018, 622, 493–501. [Google Scholar] [CrossRef]
- Colón-González, F.J.; Fezzi, C.; Lake, I.R.; Hunter, P.R. The effects of weather and climate change on dengue. PLoS Neglected Trop. Dis. 2013, 7, e2503. [Google Scholar] [CrossRef]
- NSO. National Population and Housing Census 2021; National Statistics Office (NSO): Kathmandu, Nepal, 2021. [Google Scholar]
- WorldData.info. The Climate in Nepal. 2023. Available online: https://www.worlddata.info/ (accessed on 28 February 2024).
- WHO. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control; WHO Library: Geneva, Switzerland, 2009; pp. 10–12.
- Lanciotti, R.S.; Calisher, C.H.; Gubler, D.J.; Chang, G.-J.; Vorndam, A.V. Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase-polymerase chain reaction. J. Clin. Microbiol. 1992, 30, 545–551. [Google Scholar] [CrossRef]
- Brown, J.; Wilkinson, R.; Davidson, R.; Wall, R.; Lloyd, G.; Howells, J.; Pasvol, G. Rapid diagnosis and determination of duration of viraemia in dengue fever using a reverse transcriptase polymerase chain reaction. Trans. R. Soc. Trop. Med. Hyg. 1996, 90, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Fang, M.; Chen, C.; Chen, H.; Tian, X.; Jiang, L.; Rao, Y.; Guo, H. Detection of flaviviruses by reverse transcriptase-polymerase chain reaction with the universal primer set. Microbiol. Immunol. 1997, 41, 209–213. [Google Scholar]
- SNR, S.; Norma-Rashid, Y.; Sofian–Azirun, M. Mosquitoes larval breeding habitat in urban and suburban areas, Peninsular Malaysia. Int. J. Bioeng. Life Sci. 2011, 5, 599–603. [Google Scholar]
- Gaffigan, T.; Pecor, J. Collecting, Rearing, Mounting and Shipping Mosquitoes; Walter Reed Biosystematics Unit, Division of Entomology, Walter Reed Army Institute of Research: Silver Spring, MD, USA, 1997; pp. 1–8. [Google Scholar]
- Collins, D.L. Manual for Mosquito Rearing and Experimental Technique; American Mosquito Control Association: Fresno, CA, USA, 1970. [Google Scholar]
- Rueda, L.M. Pictorial keys for the identification of mosquitoes (Diptera: Culicidae) associated with dengue virus transmission. Zootaxa 2004, 589, 1–60. [Google Scholar] [CrossRef]
- WHO. Pictorial Identification Key of Important Disease Vectors in the WHO South-East Asia Region; World Health Organization: Geneva, Switzerland, 2020.
- Vani, H.C.; Sujit, N.N.; Jaiswal, M.K.; Tiwari, R.P.; Bharathi, P.; Asmita, B.; Shankar, G.; Jithen, C.; Pallavi, V.D.; Srinivas, V.; et al. Unraveling Dengue Dynamics: In-Depth Epidemiological and Entomological Analyses in Bengaluru, India. J. Trop. Med. 2024, 2024, 7247263. [Google Scholar]
- EDCD. Situation Updates of Dengue; Epidemiology and Disease Control Division: Kathmandu, Nepal, 2022.
- DoHS. Annual Health Report; Government of Nepal, Ministry of Health and Population, Department of Health Services (DoHS): Kathmandu, Nepal, 2019.
- Dumre, S.P.; Bhandari, R.; Shakya, G.; Shrestha, S.K.; Cherif, M.S.; Ghimire, P.; Klungthong, C.; Yoon, I.-K.; Hirayama, K.; Na-Bangchang, K. Dengue virus serotypes 1 and 2 responsible for major dengue outbreaks in nepal: Clinical, laboratory, and epidemiological features. Am. J. Trop. Med. Hyg. 2017, 97, 1062–1069. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, N.; Subedi, D. The alarming outbreaks of dengue in Nepal. Trop. Med. Health 2020, 48, 5. [Google Scholar] [CrossRef] [PubMed]
- Pandey, B.D.; Pandey, K.; Dumre, S.P.; Morita, K.; Costello, A. Struggling with a new dengue epidemic in Nepal. Lancet Infect. Dis. 2023, 23, 16–17. [Google Scholar] [CrossRef] [PubMed]
- Prajapati, S.; Napit, R.; Bastola, A.; Rauniyar, R.; Shrestha, S.; Lamsal, M.; Adhikari, A.; Bhandari, P.; Yadav, S.R.; Manandhar, K.D. Molecular phylogeny and distribution of dengue virus serotypes circulating in nepal in 2017. PLoS ONE 2020, 15, e0234929. [Google Scholar] [CrossRef] [PubMed]
- Nisalak, A.; Endy, T.P.; Nimmannitya, S.; Kalayanarooj, S.; Thisayakorn, U.; Scott, R.M.; Burke, D.S.; Hoke, C.H.; Innis, B.L.; Vaughn, D.W. Serotype-specific dengue virus circulation and dengue disease in bangkok, thailand from 1973 to 1999. Am. J. Trop. Med. Hyg. 2003, 68, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Lourenço, J.; Recker, M. Natural, persistent oscillations in a spatial multi-strain disease system with application to dengue. PLoS Comput. Biol. 2013, 9, e1003308. [Google Scholar] [CrossRef] [PubMed]
- Parreira, R.; Sousa, C.A. Dengue fever in europe: Could there be an epidemic in the future? Expert Rev. Anti-Infect. Ther. 2015, 13, 29–40. [Google Scholar] [CrossRef]
- Katuwal, N.; Shrestha, A.; Ranjitkar, U.; Jakibanjar, S.; Madhup, S.K.; Tamrakar, D.; Shrestha, R. Molecular investigation of denv serotypes in the dengue outbreak of 2022 in nepal. medRxiv 2023. [Google Scholar] [CrossRef]
- Shirin, T.; Muraduzzaman, A.; Alam, A.; Sultana, S.; Siddiqua, M.; Khan, M.; Akram, A.; Sharif, A.; Hossain, S.; Flora, M. Largest dengue outbreak of the decade with high fatality may be due to reemergence of den-3 serotype in dhaka, bangladesh, necessitating immediate public health attention. New Microbes New Infect. 2019, 29, 100511. [Google Scholar] [CrossRef]
- Gautam, I.; Aradhana, K.; Tuladhar, R.; Pandey, B.D.; Tamrakar, A.S.; Byanju, R.; Dhimal, M.; Aryal, K.; Kuch, U. Container preference of the asian tiger mosquito (Aedes albopictus) in kathmandu and lalitpur districts of nepal. J. Nat. Hist. Mus. 2012, 26, 181–193. [Google Scholar] [CrossRef]
- Gupta, B.P.; Tuladhar, R.; Kurmi, R.; Manandhar, K.D. Dengue periodic outbreaks and epidemiological trends in nepal. Ann. Clin. Microbiol. Antimicrob. 2018, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.W.; Comrie, A.C.; Ernst, K. Climate and dengue transmission: Evidence and implications. Environ. Health Perspect. 2013, 121, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Xu, L.; Bjørnstad, O.N.; Liu, K.; Song, T.; Chen, A.; Xu, B.; Liu, Q.; Stenseth, N.C. Climate-driven variation in mosquito density predicts the spatiotemporal dynamics of dengue. Proc. Natl. Acad. Sci. USA 2019, 116, 3624–3629. [Google Scholar] [CrossRef] [PubMed]
- Dhimal, M.; Ahrens, B.; Kuch, U. Climate change and spatiotemporal distributions of vector-borne diseases in nepal–a systematic synthesis of literature. PLoS ONE 2015, 10, e0129869. [Google Scholar] [CrossRef] [PubMed]
- Tsantalidou, A.; Arvanitakis, G.; Georgoulias, A.K.; Akritidis, D.; Zanis, P.; Fornasiero, D.; Wohlgemuth, D.; Kontoes, C. A data driven approach for analyzing the effect of climate change on mosquito abundance in europe. Remote Sens. 2023, 15, 5649. [Google Scholar] [CrossRef]
- Williams, C.R.; Bader, C.A.; Kearney, M.R.; Ritchie, S.A.; Russell, R.C. The extinction of dengue through natural vulnerability of its vectors. PLoS Neglected Trop. Dis. 2010, 4, e922. [Google Scholar] [CrossRef] [PubMed]
- Tsuzuki, A.; Duoc, V.T.; Higa, Y.; Yen, N.T.; Takagi, M. High potential risk of dengue transmission during the hot-dry season in nha trang city, vietnam. Acta Trop. 2009, 111, 325–329. [Google Scholar] [CrossRef] [PubMed]
- GCP. Fossil CO2 Emissions at Record High in 2023; Global Carbon Project (GCP): Tsukuba, Japan, 2023. [Google Scholar]
- NOAA. National Centers for Environmental Information; National Centers for Environmental Information (NOAA): Asheville, NC, USA, 2024. [Google Scholar]
- Deichstetter, P. The effect of climate change on mosquito-borne diseases. Am. Biol. Teach. 2017, 79, 169–173. [Google Scholar] [CrossRef]
- Kamath, V.; Aishwarya, A. Dengue vaccines: Current status and future perspectives. APIK J. Intern. Med. 2024. [Google Scholar] [CrossRef]
- Alves, L. Brazil to start widespread dengue vaccinations. Lancet 2024, 403, 133. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Category | Outpatients | Inpatients | p-Value |
|---|---|---|---|---|
| Age | Child | 45 (93.7) | 3 (6.3) | <0.001 |
| Adult | 189 (82.2) | 41 (17.8) | ||
| Gender | Female | 126 (82.4) | 27 (17.6) | 0.303 |
| Male | 112 (86.4) | 17 (13.2) | ||
| Travel history | No | 52 (65.0) | 28 (35.0) | 0.145 |
| Yes | 3 (37.5) | 5 (62.5) | ||
| Myalgia | No | 22 (84.6) | 4 (15.4) | 0.007 |
| Yes | 33 (53.2) | 29 (46.8) | ||
| Rash | No | 43 (72.9) | 16 (27.1) | 0.004 |
| Yes | 12(41.4) | 17 (58.6) | ||
| Vomiting | No | 50 (84.7) | 9 (15.3) | <0.001 |
| Yes | 5 (17.2) | 24 (82.8) | ||
| Persistent | No | 55 (77.5) | 16 (22.5) | <0.001 |
| vomiting | Yes | 0 (0.0) | 17 (100.0) | |
| Nausea | No | 38 (90.5) | 4 (9.5) | <0.001 |
| Yes | 17 (37.0) | 29 (63.0) | ||
| Retro-orbital pain | No | 24 (66.7) | 12 (33.3) | 0.502 |
| Yes | 31 (59.6) | 21 (40.4) | ||
| Any bleeding | No | 55 (62.5) | 33 (37.5) | - |
| Anorexia | No | 25 (78.1) | 7 (21.9) | 0.022 |
| Yes | 30 (53.6) | 26 (46.4) | ||
| Diarrhea | No | 53 (67.9) | 25 (32.1) | 0.005 |
| Yes | 2 (20.0) | 8 (80.0) | ||
| Abdominal pain | No | 55 (72.4) | 21 (30.5) | <0.001 |
| Yes | 0 (0.0) | 12 (100.0) |
| Blood Parameters | Outpatient, Median (IQR) | Inpatient, Median (IQR) | p-Value |
|---|---|---|---|
| Hemoglobin | 12.8 (11.7–14.3) | 12.6 (11.4–14.3) | 0.579 |
| Total count (WBC) | 5280 (3785–6530) | 4945 (2820–6705) | 0.142 |
| Neutrophils | 67.5 (56.0–75.0) | 69.5 (57.3–75.0) | 0.414 |
| Lymphocytes | 21.0 (16.0–31.0) | 21.5 (14.0–29.0) | 0.579 |
| Eosinophils | 1.0 (1.0–3.0) | 1.5 (1.0–2.0) | 0.648 |
| Monocytes | 8.0 (5.0–11.0) | 7.5 (5.0–11.0) | 0.518 |
| Platelets | 173.5 (127.3–238.5) | 138.0 (54.0–174.0) | <0.001 |
| HCT | 40.3 (36.5–44.3) | 40.6 (36.2–44.2) | 0.838 |
| Serum urea | 41.0 (33.0–50.5) | 42.0 (28.0–57.0) | 0.704 |
| Creatinine | 1.0 (0.9–1.1) | 1.0 (0.9–1.1) | 0.708 |
| Sodium | 136.0 (134.0–138.0) | 137.0 (136.0–139.0) | 0.107 |
| Potassium | 3.8 (3.5–4.0) | 3.8 (3.2–4.0) | 0.651 |
| SGPT | 46.0 (23.5–67.0) | 32.5 (25.8–55.5) | 0.276 |
| SGOT | 42.0 (31.5–83.5) | 34.5 (25.3–51.8) | 0.271 |
| ALP | 234.0 (185.0–316.0) | 245.0 (196.0–342.0) | 0.252 |
| Bilirubin—total | 0.6 (0.6–0.8) | 0.6 (0.6–0.7) | 0.459 |
| Bilirubin—direct | 0.2 (0.1–0.2) | 0.2 (0.1–0.2) | 0.122 |
| Location | Number of Households Inspected | Types of Habitats | Number of Containers with Larvae (%) | Identified Mosquitoes |
|---|---|---|---|---|
| Nilkantha-3 | 30 | Tires (n = 13) | 3 (23.1) | Aedes spp. |
| Drums (n = 12) | 0 (0.0) | |||
| Plastic containers (n = 8) | 3 (37.5) | Aedes spp.; Culex spp. | ||
| Metal container (n = 6) | 0 (0.0) | |||
| Nilkantha-4 | 40 | Tires (n = 4) | 0 (0.0) | |
| Drums (n = 16) | 2 (12.5) | Culex spp.; Aedes spp. | ||
| Plastic Containers (n = 10) | 2 (20.0) | Aedes spp. | ||
| Metal container (n = 7) | 0 (0.0) | |||
| Garbage containers (n = 6) | 0 (0.0) | |||
| Flowerpots (n = 9) | 3 (33.3) | Aedes spp. | ||
| Nilkantha-6 | 30 | Tires (n = 18) | 6 (30.0) | Aedes spp. |
| Drums (n = 6) | 0 (0.0) | |||
| Plastic container (n = 7) | 1 (14.3) | Culex spp. | ||
| Flowerpots (n = 4) | 1 (25.0) | Aedes spp. | ||
| Total | 100 | 126 | 21 (16.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rimal, S.; Shrestha, S.; Paudel, S.W.; Shah, Y.; Bhandari, G.; Pandey, K.; Kharbuja, A.; Kapandji, M.; Gautam, I.; Bhujel, R.; et al. Molecular and Entomological Characterization of 2023 Dengue Outbreak in Dhading District, Central Nepal. Viruses 2024, 16, 594. https://doi.org/10.3390/v16040594
Rimal S, Shrestha S, Paudel SW, Shah Y, Bhandari G, Pandey K, Kharbuja A, Kapandji M, Gautam I, Bhujel R, et al. Molecular and Entomological Characterization of 2023 Dengue Outbreak in Dhading District, Central Nepal. Viruses. 2024; 16(4):594. https://doi.org/10.3390/v16040594
Chicago/Turabian StyleRimal, Sandesh, Sabin Shrestha, Sunita Wagle Paudel, Yogendra Shah, Govinda Bhandari, Kishor Pandey, Anjana Kharbuja, Merveille Kapandji, Ishan Gautam, Rajshree Bhujel, and et al. 2024. "Molecular and Entomological Characterization of 2023 Dengue Outbreak in Dhading District, Central Nepal" Viruses 16, no. 4: 594. https://doi.org/10.3390/v16040594
APA StyleRimal, S., Shrestha, S., Paudel, S. W., Shah, Y., Bhandari, G., Pandey, K., Kharbuja, A., Kapandji, M., Gautam, I., Bhujel, R., Takamatsu, Y., Bhandari, R., Klungthong, C., Shrestha, S. K., Fernandez, S., Malavige, G. N., Pandey, B. D., Urano, T., Morita, K., ... Dumre, S. P. (2024). Molecular and Entomological Characterization of 2023 Dengue Outbreak in Dhading District, Central Nepal. Viruses, 16(4), 594. https://doi.org/10.3390/v16040594