
Effect of Penetration Enhancers on Transdermal Delivery of Oxcarbazepine, an Antiepileptic Drug Using Microemulsions



Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Solubility Determinations
2.2.2. High-Performance Liquid Chromatography (HPLC)
2.2.3. In Vitro Skin Permeation Study of OXC
2.2.4. Preparation of Microemulsions
Phase Diagrams
Placebo (No Drug) Microemulsion Preparation
Drug-Loaded Microemulsions
Drug-Loaded Microemulsion Gel Formulation
2.2.5. Characterization of the Microemulsions
pH
Viscosity
Refractive Index
Visual Observation
Droplet Size and Polydispersity Index
2.2.6. Data Analysis
3. Results and Discussion
3.1. Solubility Study
3.2. Effect of Penetration Enhancers
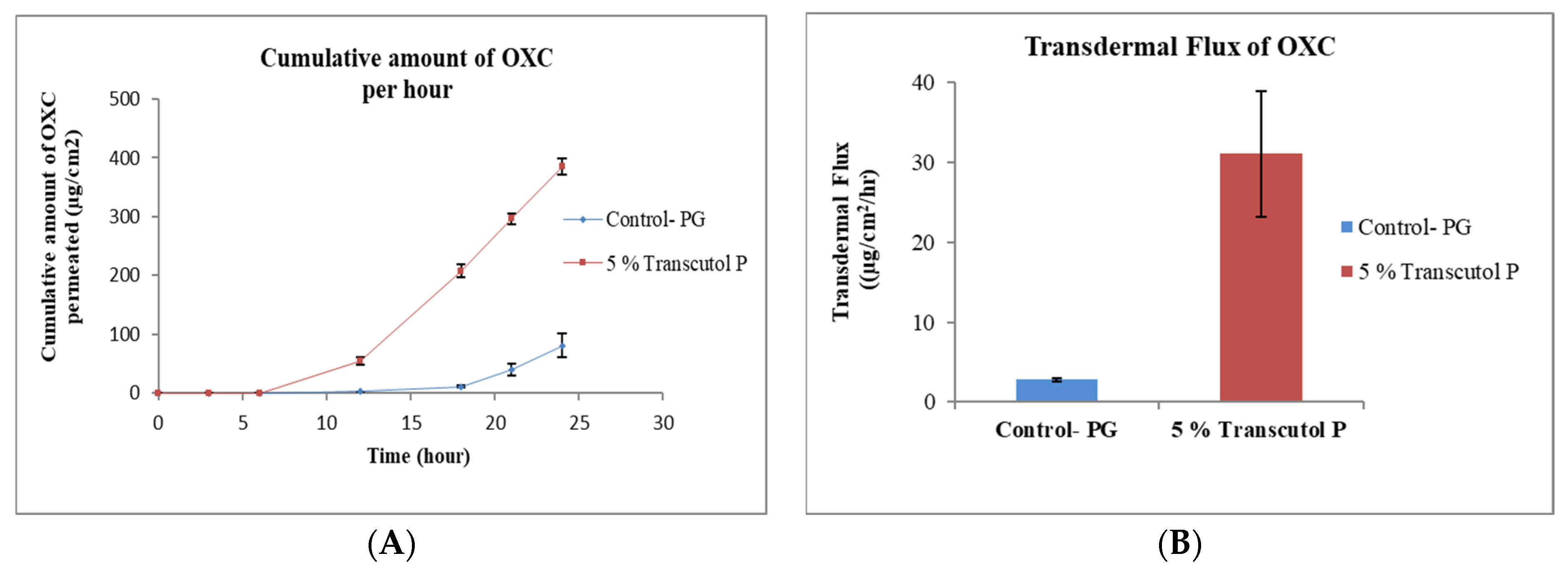
3.2.1. Effect of Transcutol® P
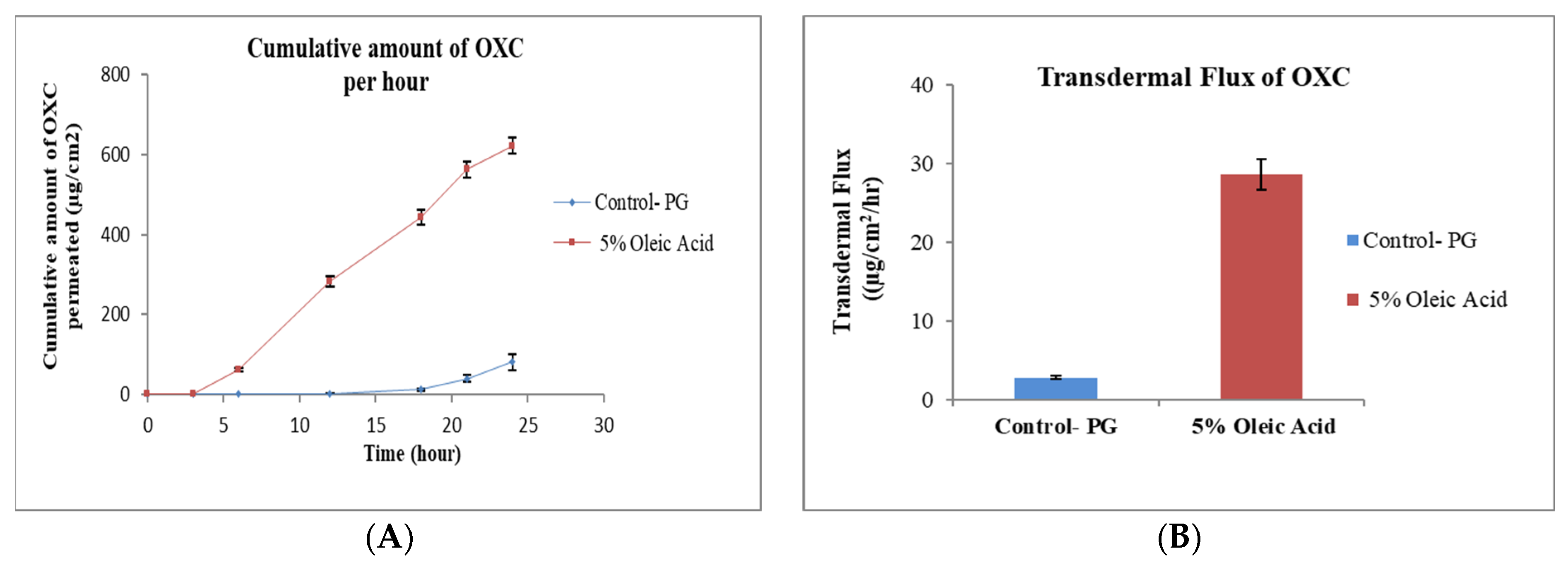
3.2.2. Effect of Oleic Acid
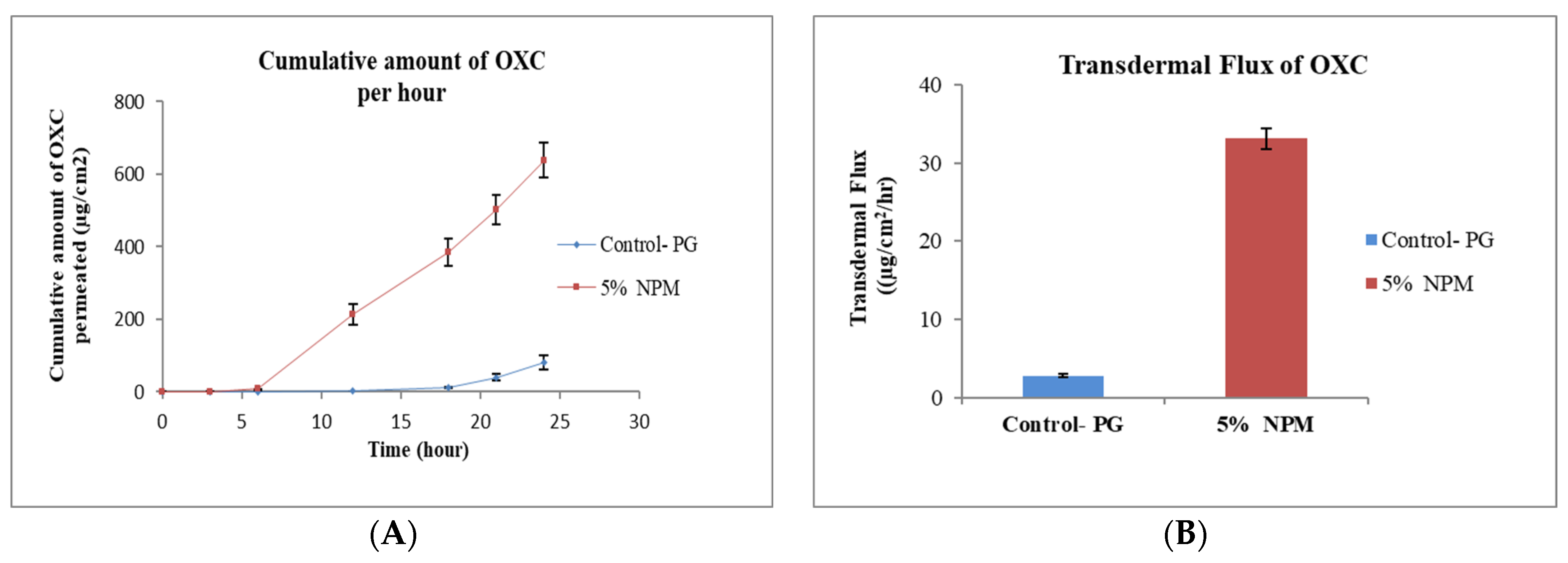
3.2.3. Effect of N-Methyl Pyrrolidone
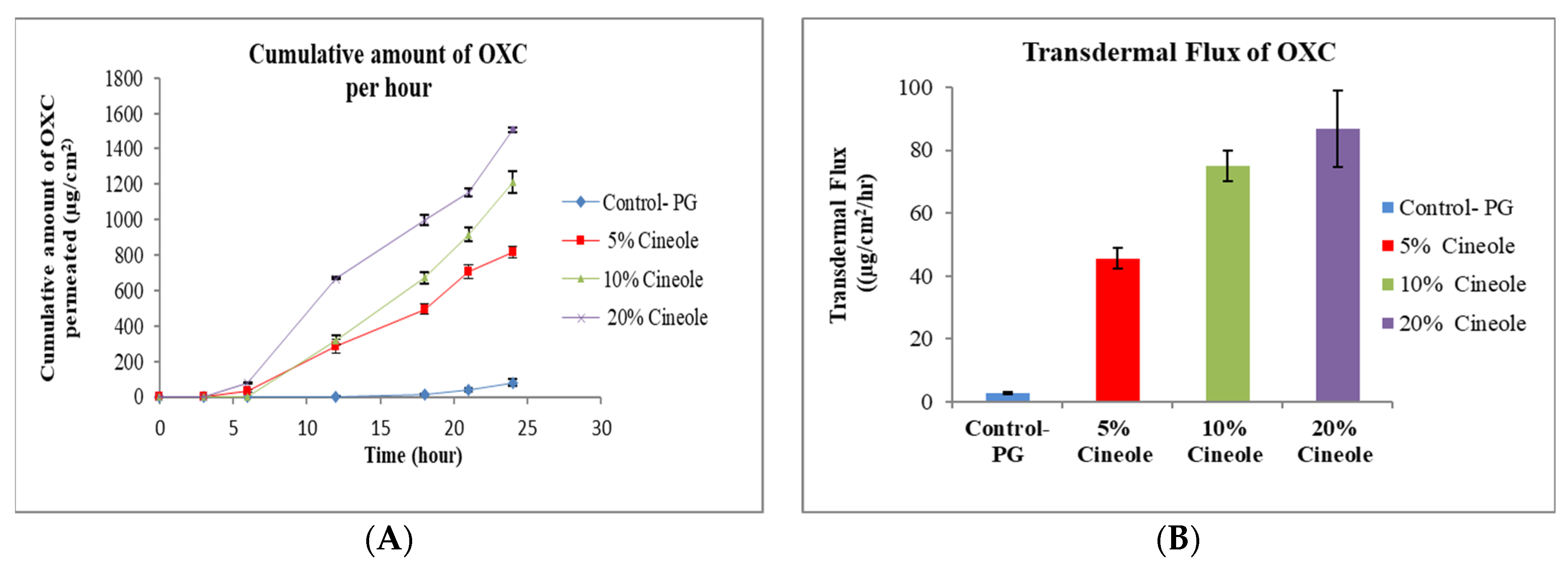
3.2.4. Effect of Cineole
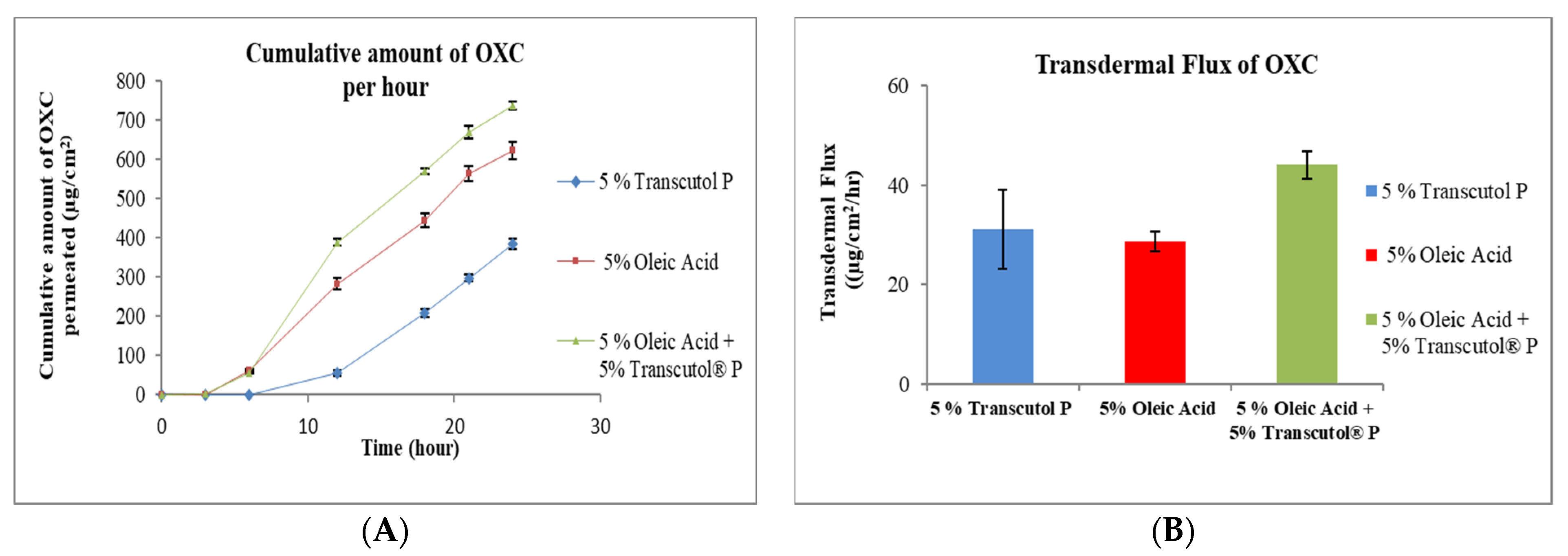
3.2.5. Combination of Transcutol® P and Oleic Acid
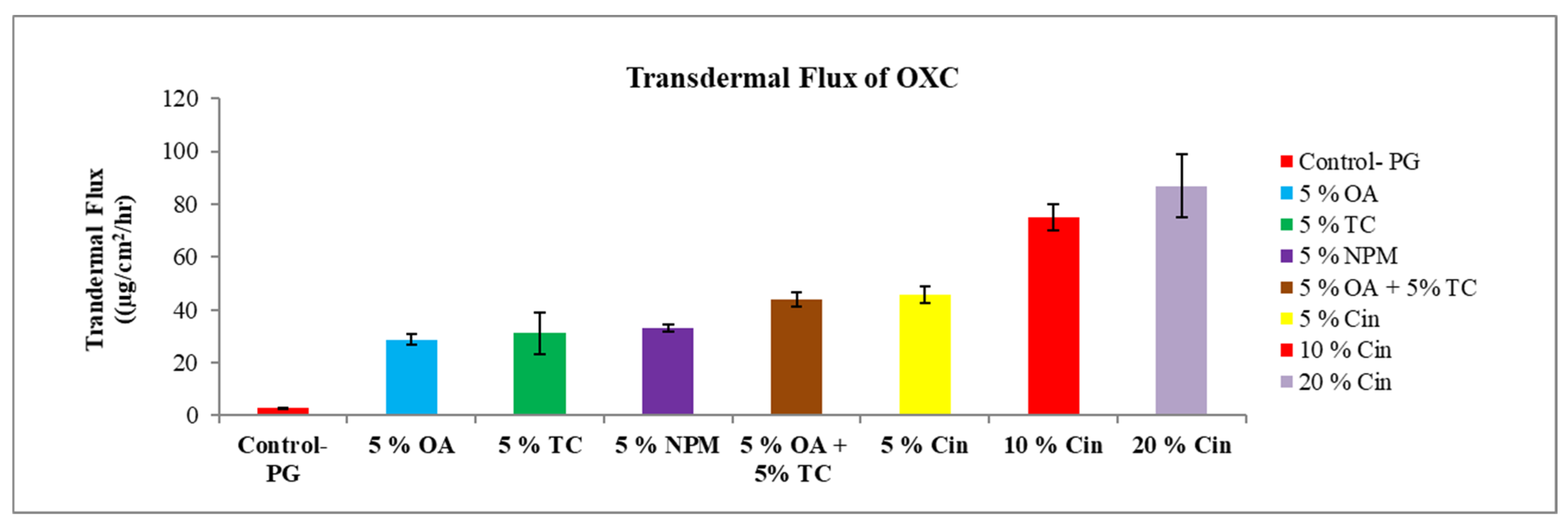
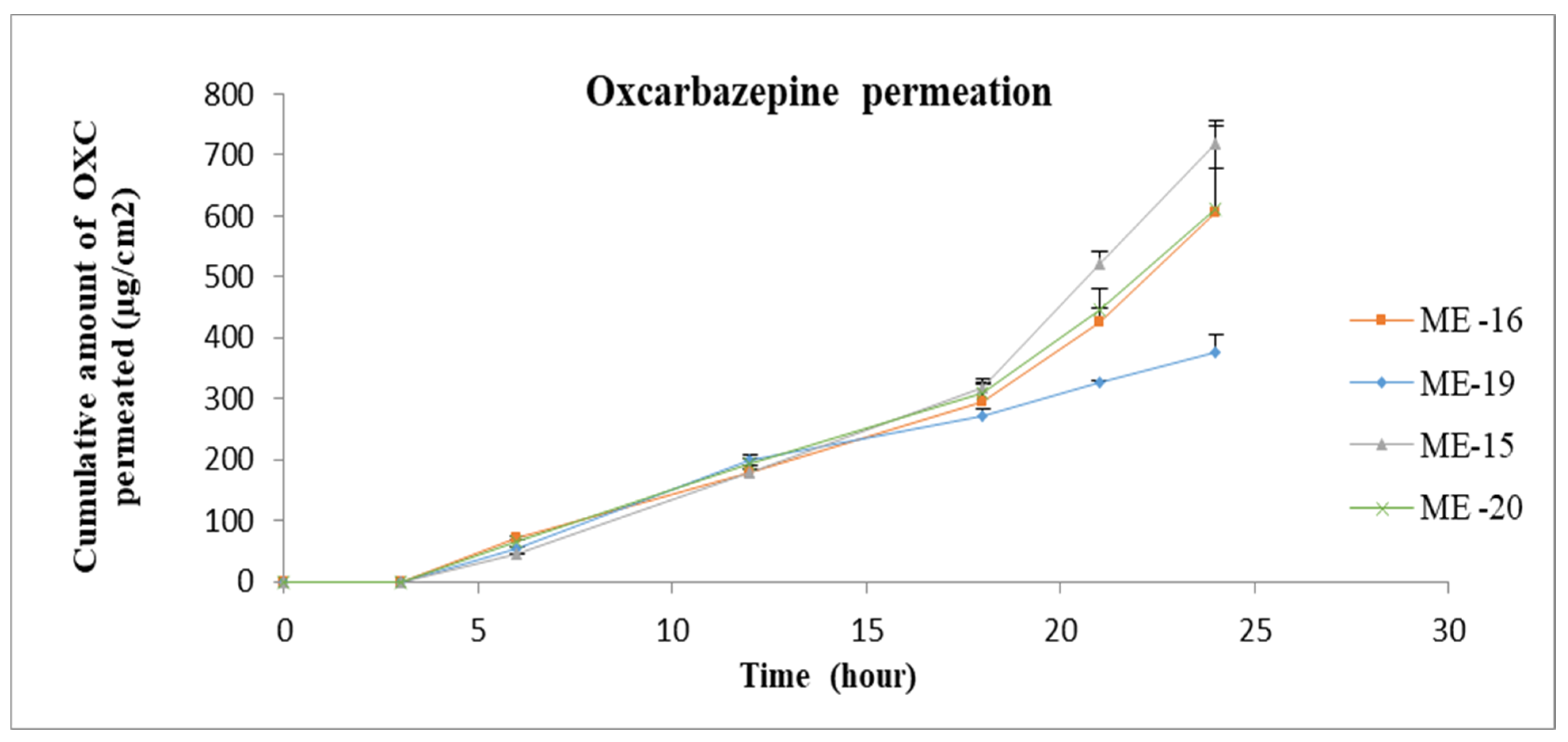
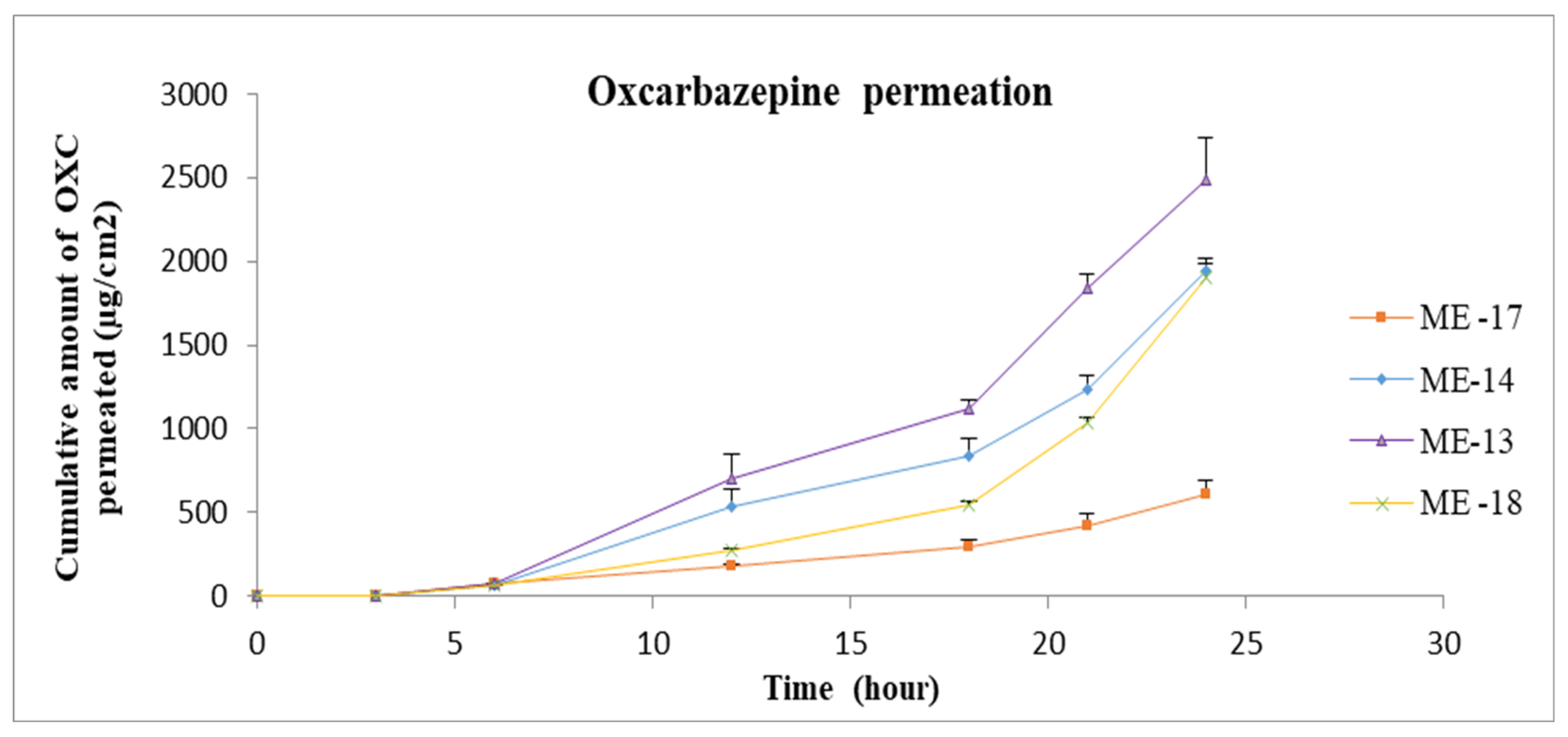
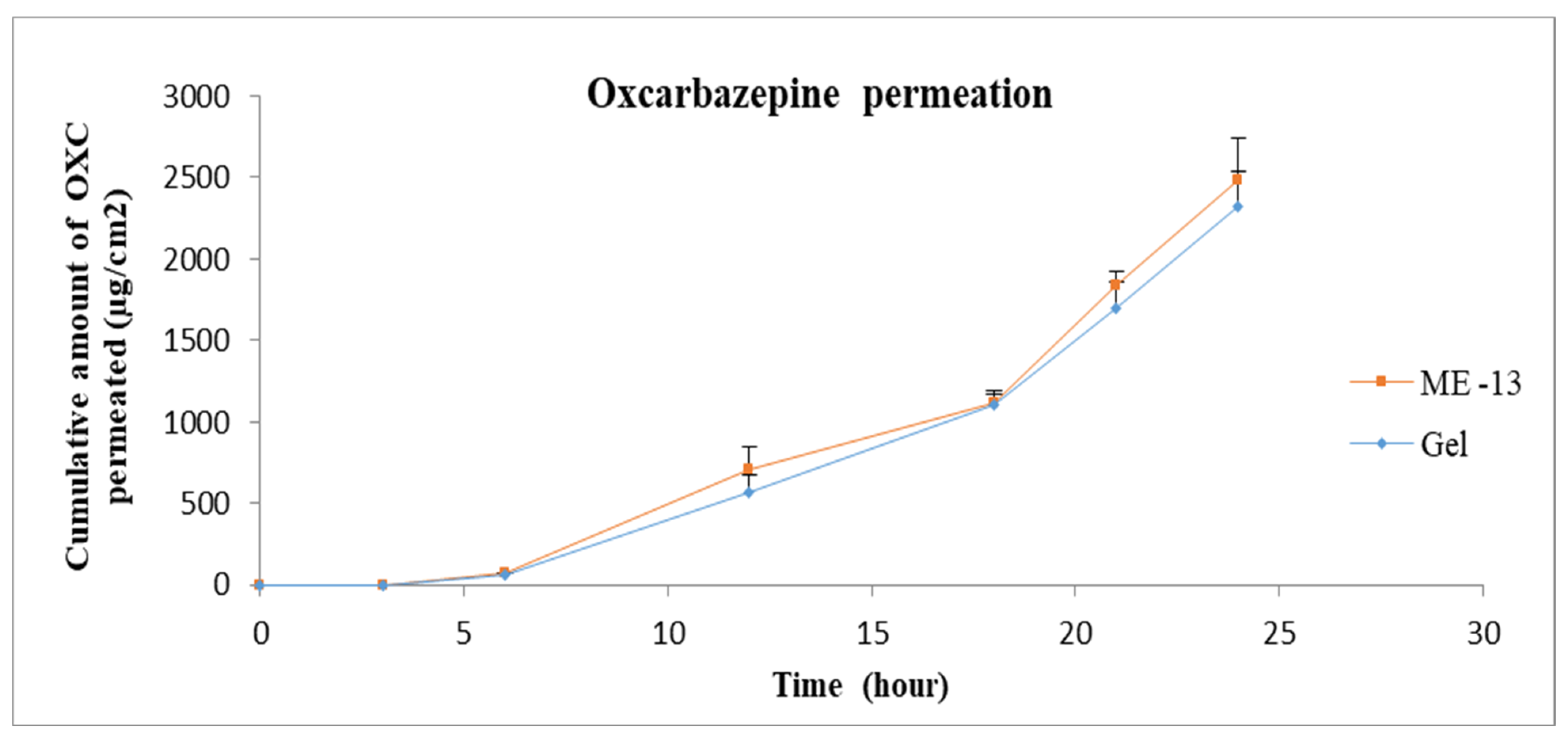
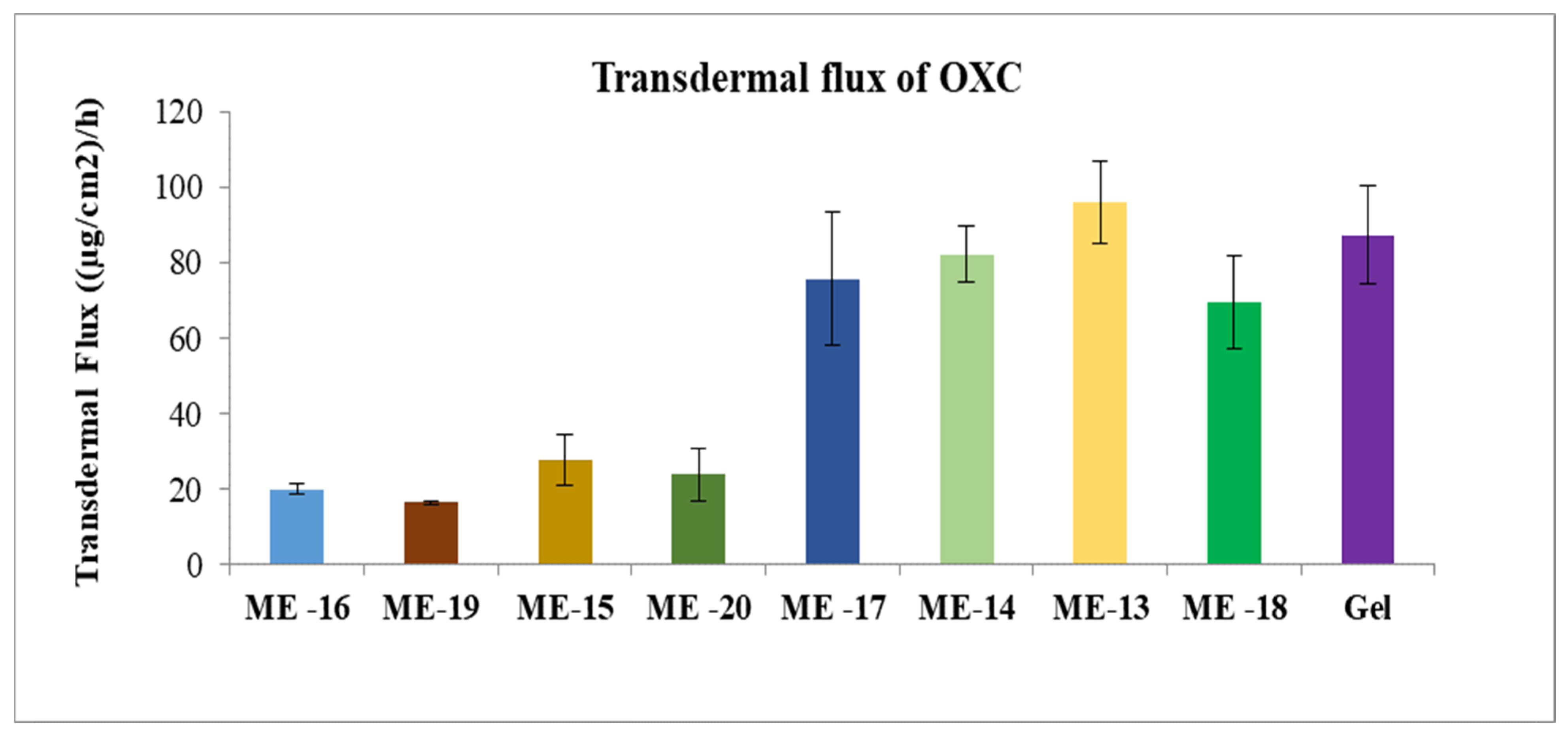
3.2.6. Transdermal Flux of Oxcarbazepine
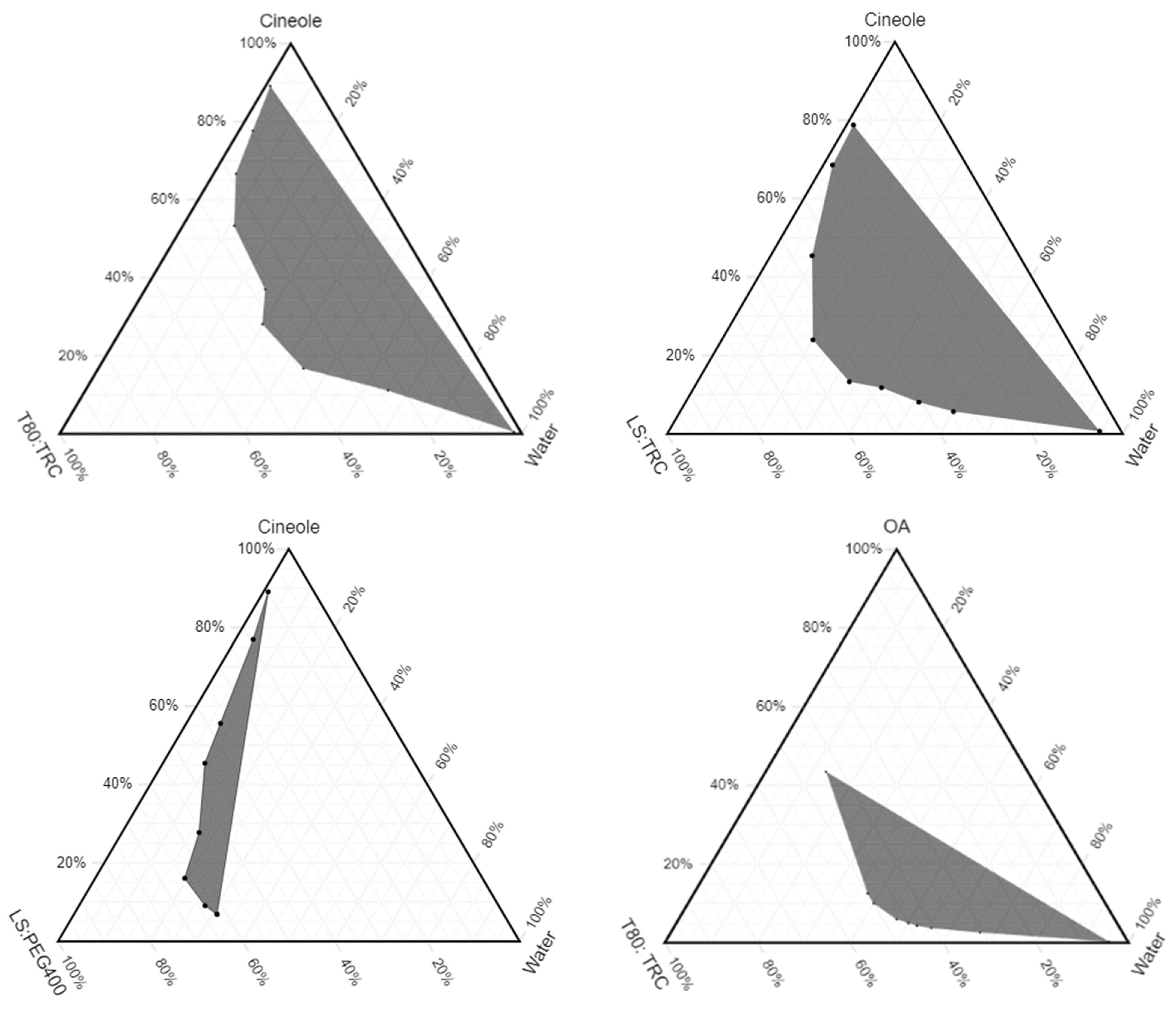
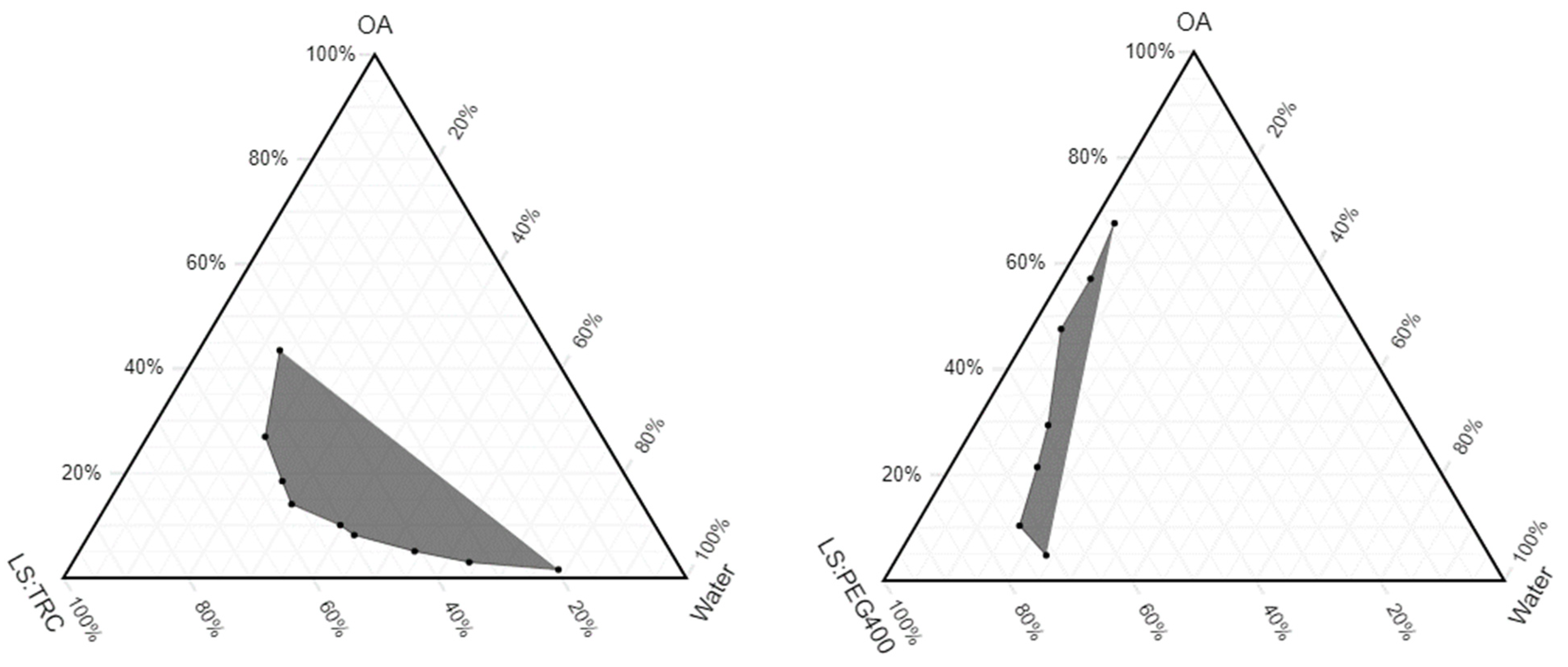
3.3. Pseudoternary Phase Diagrams
3.4. Microemulsion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| OXC | Oxcarbazepine |
| TRC | Transcutol® P |
| OA | Oleic Acid |
| Cin | Cineole |
| NMP | N-Methyl-Pyrrolidone |
| PG | Propylene Glycol |
| PBS | Phosphate Saline Buffer |
| LS | Labrasol |
| T80 | Tween 80 |
| PG | Propylene Glycol |
| IPM | Isopropyl Myristate |
| MCT | Medium Chain Triglyceride |
| MO | Mineral Oil |
| ME | Microemulsion (s) |
| TEA | Triethanolamine |
References
- Banerjee, P.N.; Filippi, D.; Hauser, W.A. The descriptive epidemiology of epilepsy—A review. Epilepsy Res. 2009, 85, 31–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penny, B.; Ensom, M.H.H. Does Oxcarbazepine Warrant Therapeutic Drug Monitoring? Clin. Pharmacokinet. 2008, 47, 767–778. [Google Scholar] [CrossRef]
- Mazza, M.; Della Marca, G.; Di Nicola, M.; Martinotti, G.; Pozzi, G.; Janiri, L.; Bria, P.; Mazza, S. Oxcarbazepine improves mood in patients with epilepsy. Epilepsy Behav. 2007, 10, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Prajapati, V.D.; Gandhi, A.K.; Patel, K.K.; Patel, B.N.; Chaudhari, A.M.; Jani, G.K. Development and optimization of modified release IPN macromolecules of oxcarbazepine using natural polymers. Int. J. Biol. Macromol. 2015, 73, 160–169. [Google Scholar] [CrossRef] [PubMed]
- PubChemCID:34312. National Center for Biotechnology Information. PubChem Database. Oxcarbazepine CID = 34312. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Oxcarbazepine (accessed on 8 August 2020).
- Nam, K.; Ha, E.-S.; Kim, J.-S.; Kuk, D.-H.; Ha, D.-H.; Kim, M.-S.; Cho, C.-W.; Hwang, S.-J. Solubility of oxcarbazepine in eight solvents within the temperature range T = (288.15–308.15) K. J. Chem. Thermodyn. 2017, 104, 45–49. [Google Scholar] [CrossRef]
- Sastry, S.V.; Nyshadham, J.R.; Fix, J.A. Recent technological advances in oral drug delivery–A review. Pharm. Sci. Tech. Today 2000, 3, 138–145. [Google Scholar] [CrossRef]
- Batchelor, H.K.; Marriott, J.F. Formulations for children: Problems and solutions. Br. J. Clin. Pharmacol. 2015, 79, 405–418. [Google Scholar] [CrossRef] [Green Version]
- Tirunagari, M.; Sameen, J.; Nandagopal, A. Formulation Development and Characterization of Oxcarbazepine Microemulsion for Intranasal Delivery. Acta Pharm. Sci. 2017, 55, 79–94. [Google Scholar] [CrossRef]
- Singh, M.P.; Kaushik, A. Preparation and evaluation of plga nanocarriers gel for topical delivery. Der. Pharmacia. Lettre. 2012, 4, 1675–1679. [Google Scholar]
- Lopalco, A.; Ali, H.; Denora, N.; Rytting, E. Oxcarbazepine-loaded polymeric nanoparticles: Development and permeability studies across in vitro models of the blood–brain barrier and human placental trophoblast. Int. J. Nanomed. 2015, 10, 1985. [Google Scholar]
- Liuzzi, R.; Carciati, A.; Guido, S.; Caserta, S. Transport efficiency in transdermal drug delivery: What is the role of fluid microstructure? Colloids Surf B Biointerfaces 2016, 139, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.S.; Cheruvu, H.S.; Mangion, S.E.; Alinaghi, A.; Benson, H.A.; Mohammed, Y.; Holmes, A.; van der Hoek, J.; Pastore, M.; Grice, J.E. Topical drug delivery: History, percutaneous absorption, and product development. Adv. Drug Deliv. Rev. 2021, 177, 113929. [Google Scholar] [CrossRef]
- Schoellhammer, C.M.; Blankschtein, D.; Langer, R. Skin permeabilization for transdermal drug delivery: Recent advances and future prospects. Expert Opin. Drug. Deliv. 2014, 11, 393–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marwah, H.; Garg, T.; Goyal, A.K.; Rath, G. Permeation enhancer strategies in transdermal drug delivery. Drug. Deliv. 2016, 23, 564–578. [Google Scholar] [CrossRef] [PubMed]
- Ita, K. Transdermal drug delivery: Progress and challenges. J. Drug Deliv. Sci. Technol. 2014, 24, 245–250. [Google Scholar] [CrossRef]
- Prausnitz, M.R.; Langer, R. Transdermal drug delivery. Nat. Biotechnol. 2008, 26, 1261. [Google Scholar] [CrossRef]
- Moffatt, K.; Wang, Y.; Singh, T.R.R.; Donnelly, R.F. Microneedles for enhanced transdermal and intraocular drug delivery. Curr. Opin. Pharmacol. 2017, 36, 14–21. [Google Scholar] [CrossRef]
- Nguyen, J.; Ita, K.; Morra, M.; Popova, I. The influence of solid microneedles on the transdermal delivery of selected antiepileptic drugs. Pharmaceutics 2016, 8, 33. [Google Scholar] [CrossRef]
- Ruan, J.; Liu, C.; Wang, J.; Zhong, T.; Quan, P.; Fang, L. Efficacy and safety of permeation enhancers: A kinetic evaluation approach and molecular mechanism study in the skin. Int. J. Pharm. 2022, 626, 122155. [Google Scholar] [CrossRef]
- William, A.; Barry, B. Penetration enhancer. Adv. Drug Deliv. 2004, 56, 603–618. [Google Scholar] [CrossRef]
- Morteza-Semnani, K.; Saeedi, M.; Akbari, J.; Eghbali, M.; Babaei, A.; Hashemi, S.M.H.; Nokhodchi, A. Development of a novel nanoemulgel formulation containing cumin essential oil as skin permeation enhancer. Drug Deliv. Transl. Res. 2022, 12, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Thong, H.-Y.; Zhai, H.; Maibach, H.I. Percutaneous penetration enhancers: An overview. Ski. Pharmacol. Physiol. 2007, 20, 272–282. [Google Scholar] [CrossRef]
- Tartaro, G.; Mateos, H.; Schirone, D.; Angelico, R.; Palazzo, G. Microemulsion microstructure(s): A tutorial review. Nanomaterials 2020, 10, 1657. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Xu, H.; Wu, S.; Ju, B.; Zhu, D.; Yan, Y.; Wang, M.; Hu, J. Preparation and evaluation of microemulsion-based transdermal delivery of Cistanche tubulosa phenylethanoid glycosides. Mol. Med. Rep. 2017, 15, 1109–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callender, S.P.; Mathews, J.A.; Kobernyk, K.; Wettig, S.D. Microemulsion utility in pharmaceuticals: Implications for multi-drug delivery. Int. J. Pharm. 2017, 526, 425–442. [Google Scholar] [CrossRef] [PubMed]
- Ameen, D.; Michniak-Kohn, B. Transdermal delivery of dimethyl fumarate for Alzheimer’s disease: Effect of penetration enhancers. Int. J. Pharm. 2017, 529, 465–473. [Google Scholar] [CrossRef]
- Haq, A.; Michniak-Kohn, B. Effects of solvents and penetration enhancers on transdermal delivery of thymoquinone: Permeability and skin deposition study. Drug Deliv. 2018, 25, 1943–1949. [Google Scholar] [CrossRef] [Green Version]
- Das, S.; Lee, S.H.; Chia, V.D.; Chow, P.S.; Macbeath, C.; Liu, Y.; Shlieout, G. Development of microemulsion based topical ivermectin formulations: Pre-formulation and formulation studies. Colloids Surf B Biointerfaces 2020, 189, 110823. [Google Scholar] [CrossRef]
- Bendas, B.; Schmalfuβ, U.; Neubert, R. Influence of propylene glycol as cosolvent on mechanisms of drug transport from hydrogels. Int. J. Pharm. 1995, 116, 19–30. [Google Scholar] [CrossRef]
- Sullivan, D.W.; Gad, S.C.; Julien, M. A review of the nonclinical safety of Transcutol®, a highly purified form of diethylene glycol monoethyl ether (DEGEE) used as a pharmaceutical excipient. Food Chem. Toxicol. 2014, 72, 40–50. [Google Scholar] [CrossRef]
- Osborne, D.W.; Musakhanian, J. Skin penetration and permeation properties of Transcutol®—Neat or diluted mixtures. AAPS PharmSciTech 2018, 19, 3512–3533. [Google Scholar] [CrossRef] [PubMed]
- Osborne, D.W. Diethylene glycol monoethyl ether: An emerging solvent in topical dermatology products. J. Cosmet. Dermatol. 2011, 10, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Haque, T.; Talukder, M.M.U. Chemical enhancer: A simplistic way to modulate barrier function of the stratum corneum. Adv. Pharm. Bull. 2018, 8, 169. [Google Scholar] [CrossRef] [Green Version]
- Chadha, G.; Sathigari, S.; Parsons, D.L.; Babu, J. In vitro percutaneous absorption of genistein from topical gels through human skin. Drug Dev. Ind. Pharm. 2011, 37, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Mura, P.; Faucci, M.; Bramanti, G.; Corti, P. Evaluation of transcutol as a clonazepam transdermal permeation enhancer from hydrophilic gel formulations. Eur. J. Pharm. Sci. 2000, 9, 365–372. [Google Scholar] [CrossRef]
- Mura, S.; Manconi, M.; Sinico, C.; Valenti, D.; Fadda, A.M. Penetration enhancer-containing vesicles (PEVs) as carriers for cutaneous delivery of minoxidil. Int. J. Pharm. 2009, 380, 72–79. [Google Scholar] [CrossRef]
- Manconi, M.; Mura, S.; Sinico, C.; Fadda, A.; Vila, A.; Molina, F. Development and characterization of liposomes containing glycols as carriers for diclofenac. Colloids Surf. A Physicochem. Eng. Asp. 2009, 342, 53–58. [Google Scholar] [CrossRef]
- Choi, J.; Choi, M.-K.; Chong, S.; Chung, S.-J.; Shim, C.-K.; Kim, D.-D. Effect of fatty acids on the transdermal delivery of donepezil: In vitro and in vivo evaluation. Int. J. Pharm. 2012, 422, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Santoyo, S.; Arellano, A.; Ygartua, P.; Martin, C. Penetration enhancer effects on the in vitro percutaneous absorption of piroxicam through rat skin. Int. J. Pharm. 1995, 117, 219–224. [Google Scholar] [CrossRef]
- Lane, M.E. Skin penetration enhancers. Int. J. Pharm. 2013, 447, 12–21. [Google Scholar] [CrossRef]
- Ammar, H.O.; Ghorab, M.; El-Nahhas, S.A.; Kamel, R. Evaluation of chemical penetration enhancers for transdermal delivery of aspirin. Asian J. Pharm. Sci. 2007, 2, 96–105. [Google Scholar]
- Koizumi, A.; Fujii, M.; Kondoh, M.; Watanabe, Y. Effect of N-methyl-2-pyrrolidone on skin permeation of estradiol. Eur. J. Pharm. Biopharm. 2004, 57, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Barry, B.W. Mode of action of penetration enhancers in human skin. J. Control. Release 1987, 6, 85–97. [Google Scholar] [CrossRef]
- Chen, J.; Jiang, Q.-D.; Chai, Y.-P.; Zhang, H.; Peng, P.; Yang, X.-X. Natural terpenes as penetration enhancers for transdermal drug delivery. Molecules 2016, 21, 1709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.H.; Gwak, H.S.; Chun, I.K. The effects of terpenes on the permeation of lidocaine and ofloxacin from moisture-activated patches. Drug Deliv. 2009, 16, 75–81. [Google Scholar] [CrossRef]
- Heard, C.M.; Kung, D.; Thomas, C.P. Skin penetration enhancement of mefenamic acid by ethanol and 1, 8-cineole can be explained by the ‘pull’effect. Int. J. Pharm. 2006, 321, 167–170. [Google Scholar] [CrossRef]
- Narishetty, S.T.K.; Panchagnula, R. Transdermal delivery of zidovudine: Effect of terpenes and their mechanism of action. J. Control. Release 2004, 95, 367–379. [Google Scholar] [CrossRef]
- Aboofazeli, R.; Zia, H.; Needham, T.E. Transdermal delivery of nicardipine: An approach to in vitro permeation enhancement. Drug Deliv. 2002, 9, 239–247. [Google Scholar] [CrossRef]
- Špaglová, M.; Čuchorová, M.; Čierna, M.; Poništ, S.; Bauerová, K. Microemulsions as solubilizers and penetration enhancers for minoxidil release from gels. Gels 2021, 7, 26. [Google Scholar] [CrossRef]
- de Araujo, G.R.S.; da Cruz Macieira, G.M.; de Oliveira, D.X.; Matos, S.S.; Dos Santos, Q.N.; Otubo, L.; de Souza Araújo, A.A.; Duarte, M.C.; Lira, A.A.M.; de Souza Nunes, R. Microemulsions formed by PPG-5-CETETH-20 at low concentrations for transdermal delivery of nifedipine: Structural and in vitro study. Colloids Surf. B Biointerfaces 2022, 214, 112474. [Google Scholar] [CrossRef]
- Song, H.; Liu, C.; Ruan, J.; Yang, D.; Zhong, T.; Liu, Y.; Fang, L. Effect of the combination of permeation enhancer and ion-pairs strategies on transdermal delivery of tofacitinib. Int. J. Pharm. 2022, 611, 121190. [Google Scholar] [CrossRef]
- Abd, E.; Namjoshi, S.; Mohammed, Y.H.; Roberts, M.S.; Grice, J.E. Synergistic skin penetration enhancer and nanoemulsion formulations promote the human epidermal permeation of caffeine and naproxen. J. Pharm. Sci. 2016, 105, 212–220. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| % w/w | |||||||
|---|---|---|---|---|---|---|---|
| Cin | OA | T80 | TRC | LS | PEG 400 | Water | |
| ME 1 | 10 | 0 | 25 | 25 | 0 | 0 | 40 |
| ME 2 | 10 | 0 | 0 | 30 | 30 | 0 | 30 |
| ME 3 | 10 | 0 | 0 | 0 | 40 | 40 | 10 |
| ME 4 | 0 | 10 | 30 | 30 | 0 | 0 | 30 |
| ME 5 | 0 | 10 | 0 | 30 | 30 | 0 | 30 |
| ME 6 | 0 | 10 | 0 | 0 | 40 | 40 | 10 |
| ME 7 | 5 | 0 | 20 | 20 | 0 | 0 | 55 |
| ME 8 | 5 | 0 | 0 | 25 | 25 | 0 | 45 |
| ME 9 | 5 | 0 | 0 | 0 | 35 | 35 | 25 |
| ME 10 | 0 | 5 | 25 | 25 | 0 | 0 | 45 |
| ME 11 | 0 | 5 | 0 | 25 | 25 | 0 | 45 |
| ME 12 | 0 | 5 | 0 | 0 | 40 | 40 | 15 |
| % w/w Oxcarbazepine (0.6%) | |||||||
|---|---|---|---|---|---|---|---|
| Cin | OA | T80 | TRC | LS | PEG 400 | Water | |
| ME 13 | 10 | 0 | 25 | 25 | 0 | 0 | 40 |
| ME 14 | 10 | 0 | 0 | 30 | 30 | 0 | 30 |
| ME 15 | 0 | 10 | 30 | 30 | 0 | 0 | 30 |
| ME 16 | 0 | 10 | 0 | 30 | 30 | 0 | 30 |
| ME 17 | 5 | 0 | 20 | 20 | 0 | 0 | 55 |
| ME 18 | 5 | 0 | 0 | 25 | 25 | 0 | 45 |
| ME 19 | 0 | 5 | 25 | 25 | 0 | 0 | 45 |
| ME 20 | 0 | 5 | 0 | 25 | 25 | 0 | 45 |
| Solvent | Solubility mg/mL |
|---|---|
| Propylene Glycol | 2.90 ± 0.05 |
| Isopropyl Myristate | 0.20 ± 0.01 |
| Medium Chain Triglycerides | 0.20 ± 0.01 |
| Polyethylene Glycol 400 | 9.7 0± 0.64 |
| Tween 80 | 4.40 ± 0.98 |
| Methanol | 3.50 ± 0.41 |
| Ethanol | 1.40 ± 0.14 |
| Phosphate Saline Buffer (pH 5.8) | 0.10 ± 0.01 |
| Phosphate Saline Buffer (pH 5.8) + 1% SLS | 0.60 ± 0.10 |
| Phosphate Saline Buffer (pH 5.8) + 3% SLS | 1.60 ± 0.12 |
| Phosphate Saline Buffer (pH 5.8) + 5% SLS | 2.50 ± 0.14 |
| Formulation | Solubility (mg/mL) ± SD | OXC Flux (µg/cm²/h) | OXC Q24 (µg/cm²) | P × 10−3 (cm/h) ± SD | ER b |
|---|---|---|---|---|---|
| Control | 2.90 ± 0.05 | 2.90 ± 0.22 | 81.00 ± 18.91 | 0.28 ± 0.02 | 1 |
| 5% Oleic Acid | 3.30 ± 0.30 | 28.60 ± 2.01 a | 621.90 ± 20.72 | 3.08 ± 0.77 | 9.86 |
| 5% Transcutol | 3.30 ± 0.07 | 31.10 ± 7.93 a | 385.40 ± 13.44 | 4.49 ± 0.28 | 10.72 |
| 5% N-Methyl-2-pyrrolidone | 3.70 ± 0.19 | 33.10 ± 1.32 a | 638.70 ± 47.41 | 2.84 ± 0.19 | 11.41 |
| 5% Oleic Acid + 5% Transcutol | 3.80 ± 0.01 | 44.00 ± 2.80 a | 736.40 ± 11.01 | 3.28 ± 0.11 | 15.17 |
| 5% Cineole | 3.30 ± 0.18 | 45.60 ± 3.22 a | 816.40 ± 31.51 | 4.39 ± 0.31 | 15.72 |
| 10% Cineole | 4.70 ± 0.01 | 74.90 ± 5.00 a | 1213.30 ± 60.32 | 7.42 ± 0.45 | 25.82 |
| 20% Cineole | 5.90 ± 0.05 | 86.90 ± 12.10 a | 1506.60 ± 10.02 | 9.01 ± 0.94 | 29.97 |
| Microemulsion | Mean Droplet Size (nm) | PDI | pH | Viscosity (cP) | RI |
|---|---|---|---|---|---|
| ME 1 | 38.70 ± 1.88 | 0.44 ± 0.056 | 4.41 | 32.50 | 1.41 |
| ME 2 | 82.14 ± 2.18 | 0.21 ± 0.01 | 3.75 | 26.40 | 1.42 |
| ME 3 | 203.40 ± 5.73 | 0.72 ± 0.02 | 6.37 | 60.20 | 1.45 |
| ME 4 | 156.90 ± 5.46 | 0.41 ± 0.10 | 4.74 | 34.20 | 1.41 |
| ME 5 | 91.13 ± 3.90 | 0.26 ± 0.02 | 4.23 | 27.40 | 1.40 |
| ME 6 | 272.90 ± 4.97 | 0.12 ± 0.01 | 5.92 | 61.40 | 1.45 |
| ME 7 | 26.96 ± 0.78 | 0.45 ± 0.18 | 4.10 | 18.50 | 1.38 |
| ME 8 | 66.52 ± 1.05 | 0.20 ± 0.00 | 3.94 | 17.60 | 1.39 |
| ME 9 | 193.60 ± 8.85 | 0.30 ± 0.07 | 6.37 | 45.80 | 1.42 |
| ME 10 | 35.24 ± 1.31 | 0.64 ± 0.123 | 4.40 | 21.40 | 1.40 |
| ME 11 | 87.26±1.38 | 0.22±0.02 | 4.82 | 19.20 | 1.39 |
| ME 12 | 135.20±3.55 | 0.22±0.01 | 6.05 | 48.60 | 1.45 |
| % w/w Oxcarbazepine (0.6%) | |||||
|---|---|---|---|---|---|
| Microemulsion | Mean Droplet Size (nm) | PDI | pH | Viscosity (cP) | RI |
| ME 13 | 41.42 ± 3.42 | 0.37 ± 0.03 | 5.61 | 31.60 | 1.41 |
| ME 14 | 94.13 ± 3.22 | 0.25 ± 0.03 | 6.84 | 27.10 | 1.41 |
| ME 15 | 161.40 ± 10.03 | 0.54 ± 0.10 | 5.38 | 33.20 | 1.41 |
| ME 16 | 109.70 ± 5.30 | 0.242 ± 0.05 | 5.42 | 28.10 | 1.41 |
| ME 17 | 31.44 ± 2.35 | 0.40 ± 0.12 | 5.20 | 17.40 | 1.38 |
| ME 18 | 68.28 ± 2.37 | 0.28 ± 0.04 | 6.14 | 16.90 | 1.38 |
| ME 19 | 42.98 ± 1.40 | 0.60 ± 1.40 | 5.13 | 21.90 | 1.41 |
| ME 20 | 87.24 ± 0.97 | 0.16 ± 0.02 | 5.86 | 17.20 | 1.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virani, A.; Puri, V.; Mohd, H.; Michniak-Kohn, B. Effect of Penetration Enhancers on Transdermal Delivery of Oxcarbazepine, an Antiepileptic Drug Using Microemulsions. Pharmaceutics 2023, 15, 183. https://doi.org/10.3390/pharmaceutics15010183
Virani A, Puri V, Mohd H, Michniak-Kohn B. Effect of Penetration Enhancers on Transdermal Delivery of Oxcarbazepine, an Antiepileptic Drug Using Microemulsions. Pharmaceutics. 2023; 15(1):183. https://doi.org/10.3390/pharmaceutics15010183
Chicago/Turabian StyleVirani, Amitkumar, Vinam Puri, Hana Mohd, and Bozena Michniak-Kohn. 2023. "Effect of Penetration Enhancers on Transdermal Delivery of Oxcarbazepine, an Antiepileptic Drug Using Microemulsions" Pharmaceutics 15, no. 1: 183. https://doi.org/10.3390/pharmaceutics15010183
APA StyleVirani, A., Puri, V., Mohd, H., & Michniak-Kohn, B. (2023). Effect of Penetration Enhancers on Transdermal Delivery of Oxcarbazepine, an Antiepileptic Drug Using Microemulsions. Pharmaceutics, 15(1), 183. https://doi.org/10.3390/pharmaceutics15010183