
A Multicenter Randomized Bioequivalence Study of a Novel Ready-to-Use Temozolomide Oral Suspension vs. Temozolomide Capsules

 , ,
, ,
Abstract
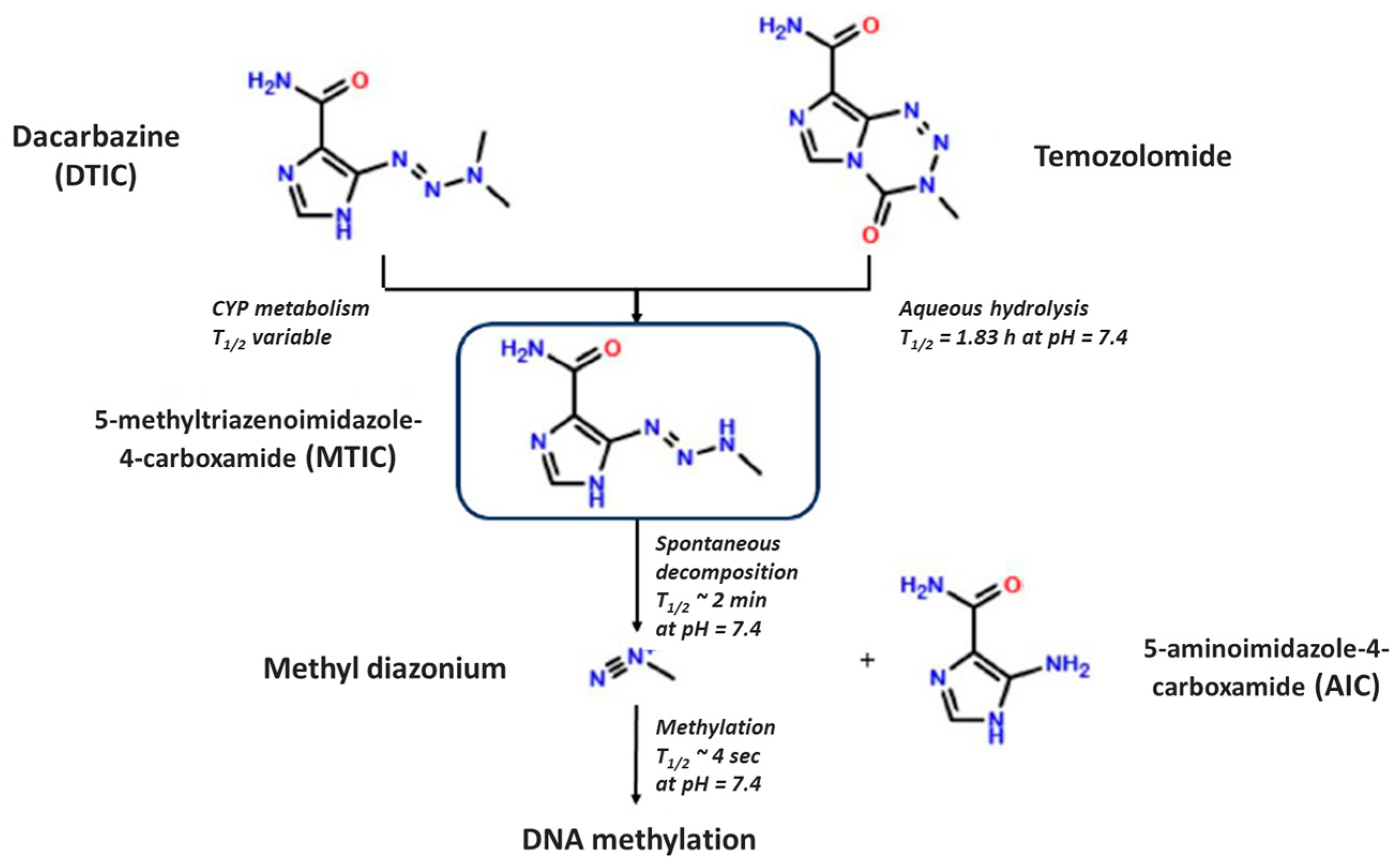
:1. Introduction
2. Materials and Methods
2.1. Products
2.2. Reagents and Chemicals
2.3. In Vitro Dissolution Testing
2.4. Bioequivalence Study Design and Oversight
2.5. Participants
2.6. Interventions
2.7. Blood Sample Collection
2.8. TMZ Bioanalysis
2.8.1. Sample Preparation
2.8.2. Chromatographic Conditions
2.9. Calculation of Pharmacokinetic Parameters
2.10. Statistical Analyses
3. Results
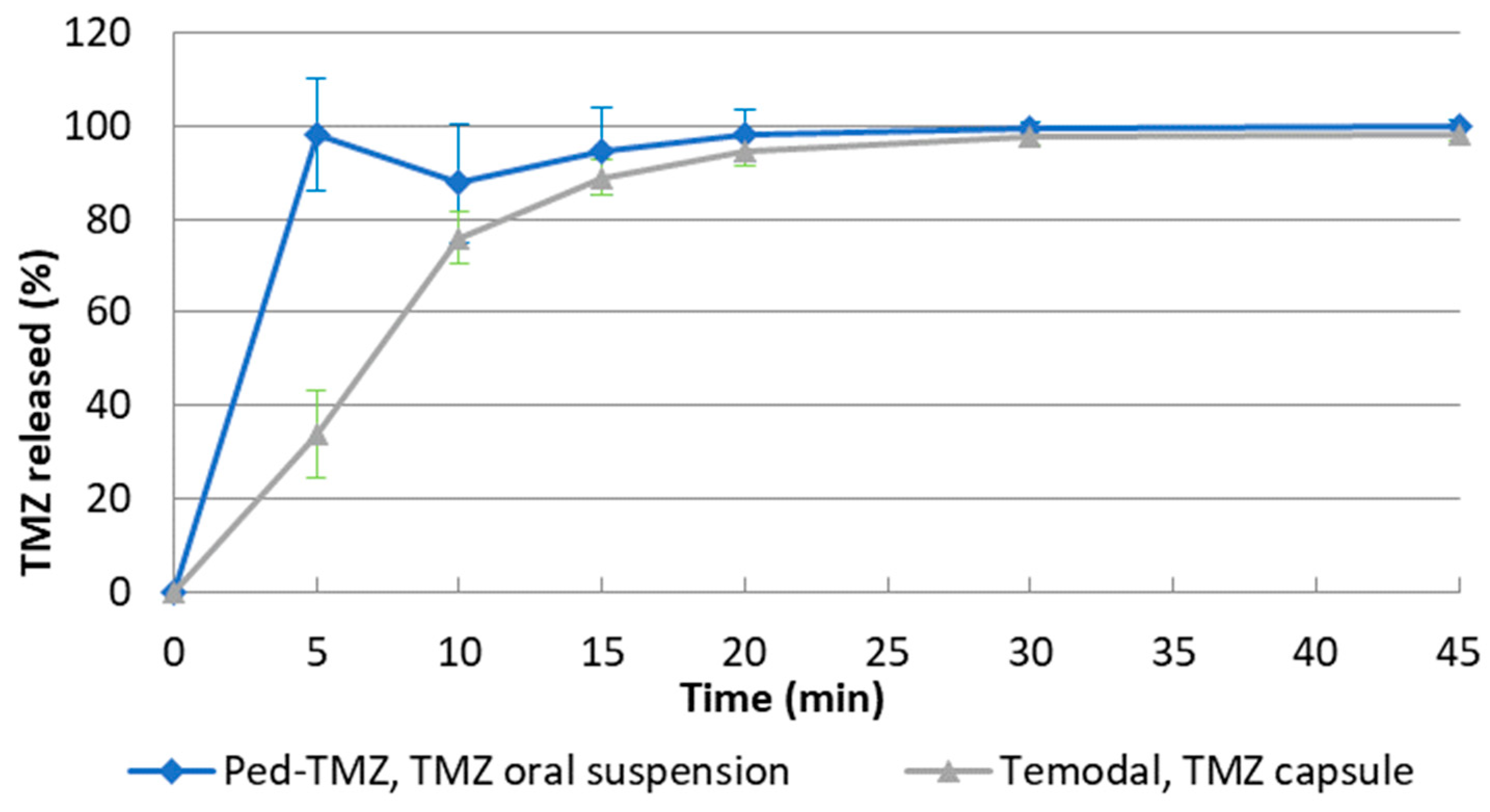
3.1. In Vitro Dissolution Testing
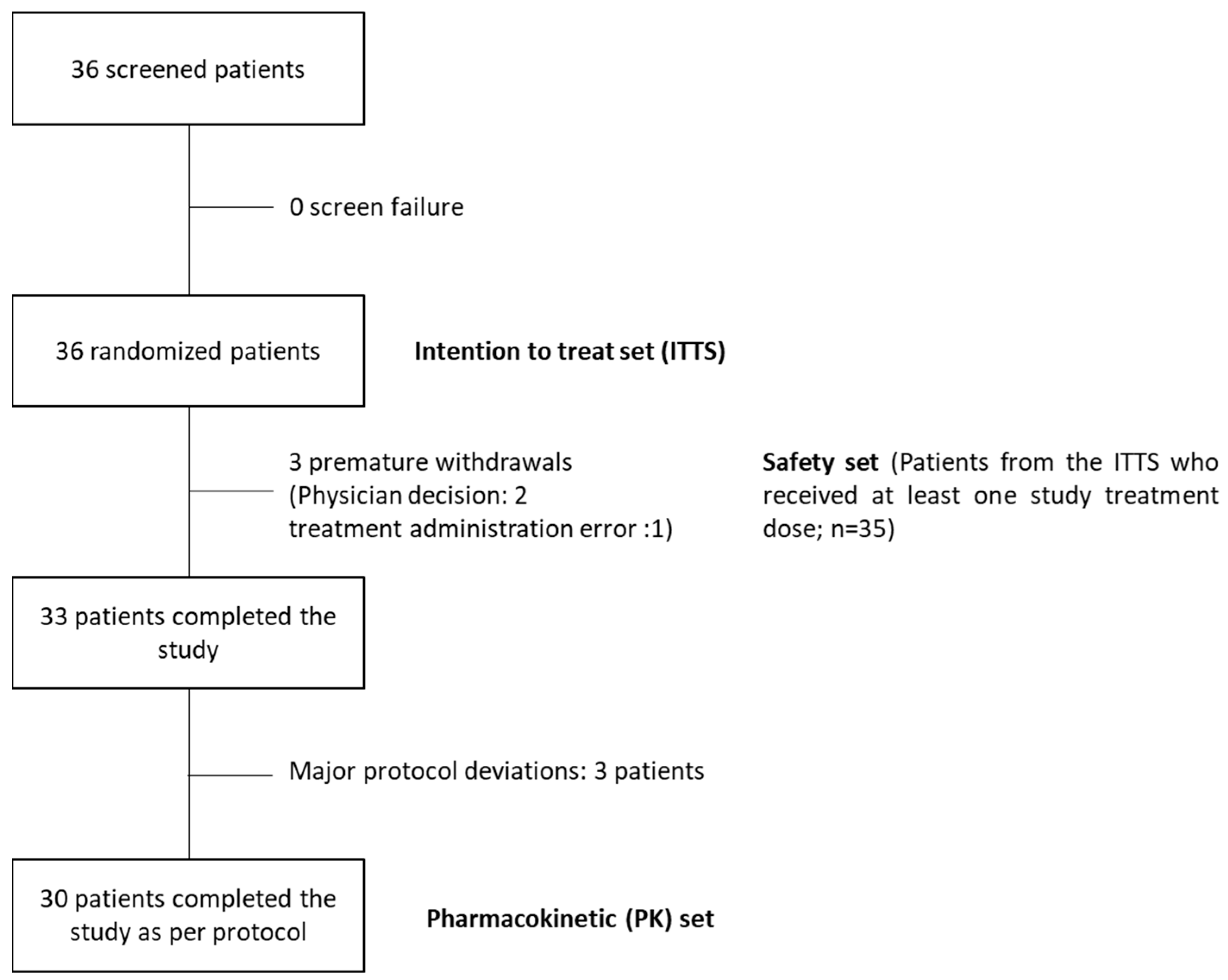
3.2. Pharmacokinetic Bioequivalence Study
3.2.1. Baseline Demographics
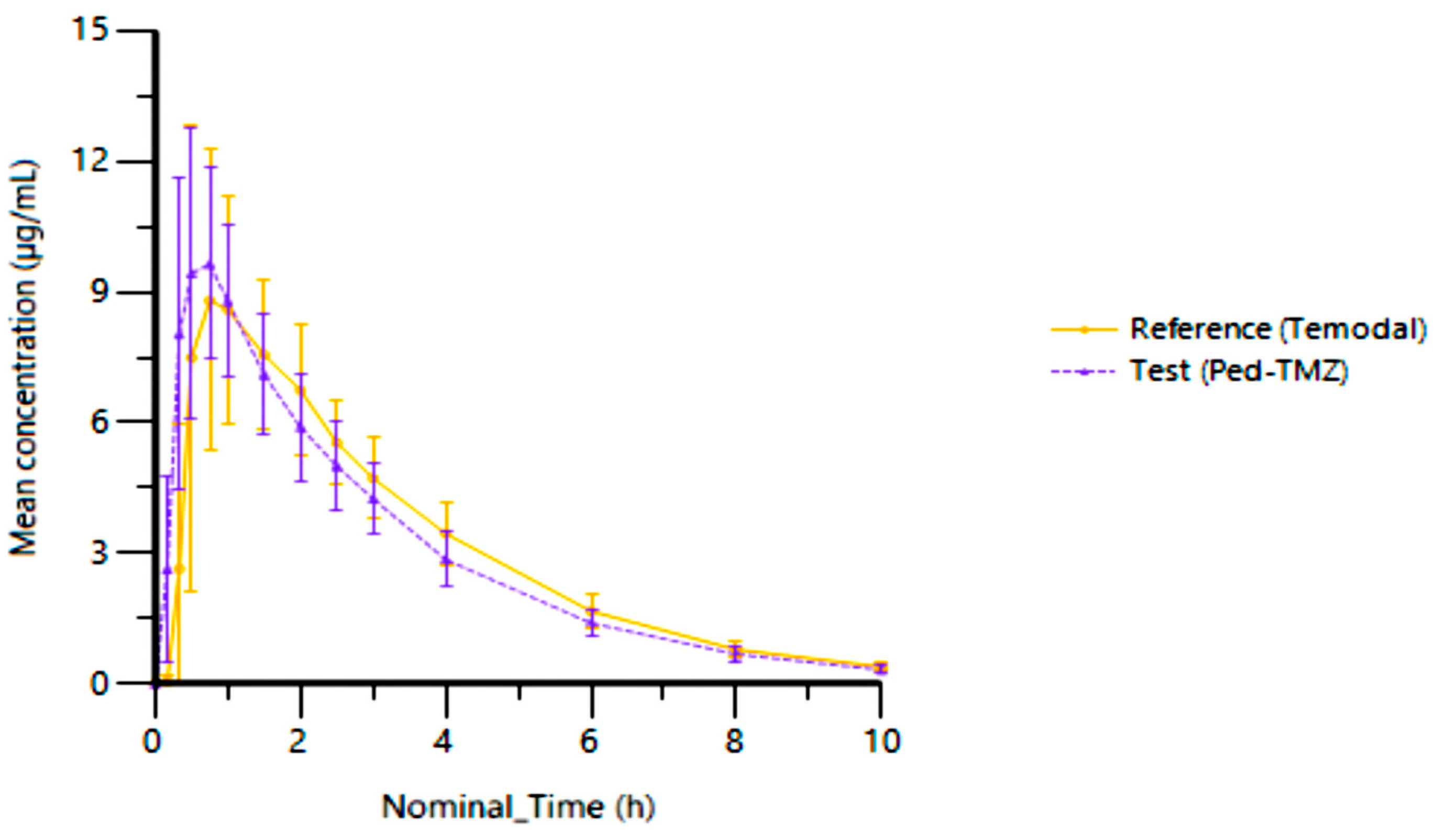
3.2.2. Pharmacokinetic Parameters and Plasma Concentrations
3.2.3. Bioequivalence of Ped-TMZ Oral Suspension vs. TMZ Capsules
3.2.4. Safety Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Strobel, H.; Baisch, T.; Fitzel, R.; Schilberg, K.; Siegelin, M.D.; Karpel-Massler, G.; Debatin, K.M.; Westhoff, M.A. Temozolomide and Other Alkylating Agents in Glioblastoma Therapy. Biomedicines 2019, 7, 69. [Google Scholar] [CrossRef]
- Denny, B.J.; Wheelhouse, R.T.; Stevens, M.F.; Tsang, L.L.; Slack, J.A. NMR and molecular modeling investigation of the mechanism of activation of the antitumor drug temozolomide and its interaction with DNA. Biochemistry 1994, 33, 9045–9051. [Google Scholar] [CrossRef]
- Baker, S.D.; Wirth, M.; Statkevich, P.; Reidenberg, P.; Alton, K.; Sartorius, S.E.; Dugan, M.; Cutler, D.; Batra, V.; Grochow, L.B.; et al. Absorption, metabolism, and excretion of 14C-temozolomide following oral administration to patients with advanced cancer. Clin. Cancer Res. 1999, 5, 309–317. [Google Scholar]
- El Mubarak, M.A.; Stylos, E.K.; Chatziathanasiadou, M.V.; Danika, C.; Alexiou, G.A.; Tsekeris, P.; Renziehausen, A.; Crook, T.; Syed, N.; Sivolapenko, G.B.; et al. Development and validation of simple step protein precipitation UHPLC-MS/MS methods for quantitation of temozolomide in cancer patient plasma samples. J. Pharm. Biomed. Anal. 2019, 162, 164–170. [Google Scholar] [CrossRef]
- Peer, C.J.; Ronner, L.; Rodgers, L.; Lester McCully, C.M.; Warren, K.E.; Figg, W.D. Quantification of Temozolomide in Nonhuman Primate Fluids by Isocratic Ultra-High Performance Liquid Chromatography-Tandem Mass Spectrometry to Study Brain Tissue Penetration Following Intranasal or Intravenous Delivery. Separations 2016, 3, 4. [Google Scholar] [CrossRef] [PubMed]
- Muggeri, A.; Vago, M.; Perez, S.; Rubio, M.; Gonzalez, C.; Magarinos, C.; Rosenberg, M.; Costa, F.; Perez-Lloret, S. A Randomized, Open-Label, Two-Way Crossover, Single-Dose Bioequivalence Study of Temozolomide 200 mg/m2 (Dralitem¯ vs. Temodal¯ Capsules) in Patients with Primary Tumors of the Central Nervous System Under Fasting Conditions. Drugs R D 2017, 17, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Waghule, T.; Narayan Saha, R.; Singhvi, G. UV spectroscopic method for estimation of temozolomide: Application in stability studies in simulated plasma pH, degradation rate kinetics, formulation design, and selection of dissolution media. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2021, 258, 119848. [Google Scholar] [CrossRef]
- EMA. Temodal SmPC. Available online: https://www.ema.europa.eu/en/documents/product-information/temodal-epar-product-information_en.pdf (accessed on 13 September 2023).
- Children’s Cancer and Leukaemia Group. Options for the Treatment of Patients with Relapsed/Progressive High-Risk Neuroblastoma. 2015. Available online: https://www.cclg.org.uk/write/MediaUploads/Member%20area/Treatment%20guidelines/CCLG_Relapsed_Progressive_High_Risk_Neuroblastoma_Guidelines_March_2015_FINAL.pdf (accessed on 13 September 2023).
- Moreno, L.; Rubie, H.; Varo, A.; Le Deley, M.C.; Amoroso, L.; Chevance, A.; Garaventa, A.; Gambart, M.; Bautista, F.; Valteau-Couanet, D.; et al. Outcome of children with relapsed or refractory neuroblastoma: A meta-analysis of ITCC/SIOPEN European phase II clinical trials. Pediatr. Blood Cancer 2017, 64, 25–31. [Google Scholar] [CrossRef]
- Parikh, N.S.; Howard, S.C.; Chantada, G.; Israels, T.; Khattab, M.; Alcasabas, P.; Lam, C.G.; Faulkner, L.; Park, J.R.; London, W.B.; et al. SIOP-PODC adapted risk stratification and treatment guidelines: Recommendations for neuroblastoma in low- and middle-income settings. Pediatr. Blood Cancer 2015, 62, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Hill, R.M.; Plasschaert, S.L.A.; Timmermann, B.; Dufour, C.; Aquilina, K.; Avula, S.; Donovan, L.; Lequin, M.; Pietsch, T.; Thomale, U.; et al. Relapsed Medulloblastoma in Pre-Irradiated Patients: Current Practice for Diagnostics and Treatment. Cancers 2022, 14, 126. [Google Scholar] [CrossRef] [PubMed]
- Defachelles, A.S.; Bogart, E.; Casanova, M.; Merks, J.H.M.; Bisogno, G.; Calareso, G.; Gallego Melcon, S.; Gatz, S.A.; Le Deley, M.C.; McHugh, K.; et al. Randomized Phase II Trial of Vincristine-Irinotecan with or without Temozolomide, in Children and Adults with Relapsed or Refractory Rhabdomyosarcoma: A European Paediatric Soft Tissue Sarcoma Study Group and Innovative Therapies for Children with Cancer Trial. J. Clin. Oncol. 2021, 39, 2979–2990. [Google Scholar] [CrossRef]
- EMA. EMA/PDCO/381728/2014, Draft Inventory of Paediatric Therapeutic Needs—Paediatric Oncology. 2014. Available online: https://www.ema.europa.eu/en/documents/other/draft-inventory-paediatric-therapeutic-needs-paediatric-oncology_en.pdf (accessed on 13 September 2023).
- Garcia, M.; Clopès, A.; Bruna, J.; Martinez, M.; Fort, E.; Gil, M. Critical appraisal of temozolomide formulations in the treatment of primary brain tumors: Patient considerations. Cancer Manag. Res. 2009, 1, 137–150. [Google Scholar] [CrossRef]
- Eek, D.; Krohe, M.; Mazar, I.; Horsfield, A.; Pompilus, F.; Friebe, R.; Shields, A.L. Patient-reported preferences for oral versus intravenous administration for the treatment of cancer: A review of the literature. Patient Prefer. Adherence 2016, 10, 1609–1621. [Google Scholar]
- Lemarchand, C.; Bienaymé, H.; Rieutord, A.; Tortolano, L.; Annereau, M.; Bastid, J. Dispensing oral temozolomide in children: Precision and stability of a novel ready-to-use liquid formulation in comparison with capsule derived mixtures. In Supplement: Abstracts from the 54th Congress of the International Society of Paediatric Oncology (SIOP) September 28–October 1, 2022; Wiley: New York, NY, USA, 2022; Volume 69. [Google Scholar] [CrossRef]
- EMA. EMA/CPMP/EWP/QWP/1401/98, Guideline on the Investigation of Bioequivalence. 2010. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-investigation-bioequivalence-rev1_en.pdf (accessed on 13 September 2023).
- FDA. Bioavailability and Bioequivalence Studies Submitted in NDAs or INDs—General Considerations. 2014. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/bioavailability-and-bioequivalence-studies-submitted-ndas-or-inds-general-considerations (accessed on 13 September 2023).
- EMA. Temozolomide Teva EPAR. 2010. Available online: https://www.ema.europa.eu/en/documents/assessment-report/temozolomide-teva-epar-public-assessment-report_en.pdf (accessed on 13 September 2023).
- FDA. Draft Guidance on Temozolomide. 2008. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/psg/Temozolomide_cap_21029_RC12-08.pdf (accessed on 13 September 2023).
- FDA. Dissolution Testing and Acceptance Criteria for Immediate-Release Solid Oral Dosage form Drug Products Containing High Solubility Drug Substances. 2018. Available online: https://www.fda.gov/files/drugs/published/Dissolution-Testing-and-Acceptance-Criteria-for-Immediate-Release-Solid-Oral-Dosage-Form-Drug-Products-Containing-High-Solubility-Drug-Substances-Guidance-for-Industry.pdf (accessed on 13 September 2023).
- European Pharmacopoeia 11.0. Temozolomide Monograph, 04/2019:2780. 3973-3974. Available online: https://pheur.edqm.eu/app/11-0/content/11-0/2780E.htm (accessed on 15 November 2023).
- European Pharmacopoeia 11.0. 2.9.3. Dissolution Test for Solid Dosage Forms, 01/2023:20903. 2023, pp. 348–355. Available online: https://pheur.edqm.eu/app/11-0/content/11-0/20903E.htm?highlight=on&terms=dissolution (accessed on 15 November 2023).
- United States Pharmacopeial. General Chapter, <711> Dissolution; USP-NF; United States Pharmacopeia: Rockville, MD, USA, 2023. [Google Scholar] [CrossRef]
- EMA. CPMP/ICH/381/95, ICH Topic Q 2 (R1) Validation of Analytical Procedures: Text and Methodology. 1995. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-q-2-r1-validation-analytical-procedures-text-methodology-step-5_en.pdf (accessed on 13 September 2023).
- FDA. Bioanalytical Method Validation—Guidance for Industry. 2018. Available online: https://www.fda.gov/files/drugs/published/Bioanalytical-Method-Validation-Guidance-for-Industry.pdf (accessed on 13 September 2023).
- EMA. CHMP/EWP/192217/2009 Rev. 1 Corr. 2**, Guideline on Bioanalytical Method Validation. 2011. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-bioanalytical-method-validation_en.pdf (accessed on 13 September 2023).
- FDA. NDA# 22-277, Schering-Plough, Pivotal Bioequivalence Study P02467. 2008. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022277s000_ClinPharmR.pdf (accessed on 15 November 2023).
- EMA. Temozolomide Sandoz SmPC. Available online: https://www.ema.europa.eu/en/documents/product-information/temozolomide-sandoz-epar-product-information_en.pdf (accessed on 13 September 2023).
- EMA. Temozolomide TEVA SmPC. Available online: https://www.ema.europa.eu/en/documents/product-information/temozolomide-teva-epar-product-information_en.pdf (accessed on 13 September 2023).
- FDA. DRAFT Guidance for Industry. Bioequivalence Studies with Pharmacokinetic Endpoints for Drugs Submitted Under an ANDA. 2021. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/bioequivalence-studies-pharmacokinetic-endpoints-drugs-submitted-under-abbreviated-new-drug (accessed on 13 September 2023).
- EMA. Temodal EPAR. 2005. Available online: https://www.ema.europa.eu/en/documents/scientific-discussion/temodal-epar-scientific-discussion_en.pdf (accessed on 13 September 2023).
- Agarwala, S.S.; Kirkwood, J.M. Temozolomide in combination with interferon alpha-2b in patients with metastatic melanoma: A phase I dose-escalation study. Cancer 2003, 97, 121–127. [Google Scholar] [CrossRef]
- Aoki, T.; Nishikawa, R.; Mizutani, T.; Nojima, K.; Mishima, K.; Adachi, J.; Matsutani, M. Pharmacokinetic study of temozolomide on a daily-for-5-days schedule in Japanese patients with relapsed malignant gliomas: First study in Asians. Int. J. Clin. Oncol. 2007, 12, 341–349. [Google Scholar] [CrossRef]
- Azzabi, A.; Hughes, A.N.; Calvert, P.M.; Plummer, E.R.; Todd, R.; Griffin, M.J.; Lind, M.J.; Maraveyas, A.; Kelly, C.; Fishwick, K.; et al. Phase I study of temozolomide plus paclitaxel in patients with advanced malignant melanoma and associated in vitro investigations. Br. J. Cancer 2005, 92, 1006–1012. [Google Scholar] [CrossRef]
- Beale, P.; Judson, I.; Moore, S.; Statkevich, P.; Marco, A.; Cutler, D.L.; Reidenberg, P.; Brada, M. Effect of gastric pH on the relative oral bioavailability and pharmacokinetics of temozolomide. Cancer Chemother. Pharmacol. 1999, 44, 389–394. [Google Scholar] [CrossRef]
- Brada, M.; Judson, I.; Beale, P.; Moore, S.; Reidenberg, P.; Statkevich, P.; Dugan, M.; Batra, V.; Cutler, D. Phase I dose-escalation and pharmacokinetic study of temozolomide (SCH 52365) for refractory or relapsing malignancies. Br. J. Cancer 1999, 81, 1022–1030. [Google Scholar]
- Britten, C.; Rowinsky, E.; Baker, S.; Agarwala, S.; Eckardt, J.; Barrington, R.; Diab, S.; Hammond, L.; Johnson, T.; Villalona-Calero, M.; et al. A Phase I and Pharmacokinetic Study of Temozolomide and Cisplatin in Patients with Advanced Solid Malignancies. Clin. Cancer Res. 1999, 5, 1629–1637. [Google Scholar]
- Brock, C.S.; Newlands, E.S.; Wedge, S.R.; Bower, M.; Evans, H.; Colquhoun, I.; Roddie, M.; Glaser, M.; Brampton, M.H.; Rustin, G.J. Phase I Trial of Temozolomide Using an Extended Continuous Oral Schedule. Cancer Res. 1998, 58, 4363–4367. [Google Scholar]
- Dhodapkar, M.; Rubin, J.; Reid, J.M.; Burch, P.A.; Pitot, H.C.; Buckner, J.C.; Ames, M.M.; Suman, V.J. Phase I trial of temozolomide in patients with advanced cancer. Clin. Cancer Res. 1997, 3, 1093–1100. [Google Scholar] [PubMed]
- Diez, B.D.; Statkevich, P.; Zhu, Y.; Abutarif, M.A.; Xuan, F.; Kantesaria, B.; Cutler, D.; Cantillon, M.; Schwarz, M.; Pallotta, M.G.; et al. Evaluation of the exposure equivalence of oral versus intravenous temozolomide. Cancer Chemother. Pharmacol. 2010, 65, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Gander, M.; Leyvraz, S.; Decosterd, L.; Bonfanti, M.; Marzolini, C.; Shen, F.; Lienard, D.; Perey, L.; Colella, G.; Biollaz, J.; et al. Sequential administration of temozolomide and fotemustine: Depletion of O6-alkyl guanine-DNA transferase in blood lymphocytes and in tumours. Ann. Oncol. 1999, 10, 831–838. [Google Scholar] [CrossRef]
- Gojo, I.; Beumer, J.H.; Pratz, K.W.; McDevitt, M.A.; Baer, M.R.; Blackford, A.L.; Smith, B.D.; Gore, S.D.; Carraway, H.E.; Showel, M.M.; et al. A Phase 1 Study of the PARP Inhibitor Veliparib in Combination with Temozolomide in Acute Myeloid Leukemia. Clin. Cancer Res. 2017, 23, 697–706. [Google Scholar] [CrossRef]
- Hammond, L.A.; Eckardt, J.R.; Baker, S.D.; Eckhardt, S.G.; Dugan, M.; Forral, K.; Reidenberg, P.; Statkevich, P.; Weiss, G.R.; Rinaldi, D.A.; et al. Phase I and pharmacokinetic study of temozolomide on a daily-for-5-days schedule in patients with advanced solid malignancies. J. Clin. Oncol. 1999, 17, 2604–2613. [Google Scholar] [CrossRef] [PubMed]
- Hammond, L.A.; Eckardt, J.R.; Kuhn, J.G.; Gerson, S.L.; Johnson, T.; Smith, L.; Drengler, R.L.; Campbell, E.; Weiss, G.R.; Von Hoff, D.D.; et al. A randomized phase I and pharmacological trial of sequences of 1,3-bis(2-chloroethyl)-1-nitrosourea and temozolomide in patients with advanced solid neoplasms. Clin. Cancer Res. 2004, 10, 1645–1656. [Google Scholar] [CrossRef] [PubMed]
- Hottinger, A.F.; Aissa, A.B.; Espeli, V.; Squiban, D.; Dunkel, N.; Vargas, M.I.; Hundsberger, T.; Mach, N.; Schaller, K.; Weber, D.C.; et al. Phase I study of sorafenib combined with radiation therapy and temozolomide as first-line treatment of high-grade glioma. Br. J. Cancer 2014, 110, 2655–2661. [Google Scholar] [CrossRef]
- Jackson, S.; Weingart, J.; Nduom, E.K.; Harfi, T.T.; George, R.T.; McAreavey, D.; Ye, X.; Anders, N.M.; Peer, C.; Figg, W.D.; et al. The effect of an adenosine A2A agonist on intra-tumoral concentrations of temozolomide in patients with recurrent glioblastoma. Fluids Barriers CNS 2018, 15, 2. [Google Scholar] [CrossRef]
- Jen, J.F.; Cutler, D.L.; Pai, S.M.; Batra, V.K.; Affrime, M.B.; Zambas, D.N.; Heft, S.; Hajian, G. Population Pharmacokinetics of Temozolomide in Cancer Patients. Pharm. Res. 2000, 17, 1284–1289. [Google Scholar] [CrossRef]
- Lassman, A.B.; Van Den Bent, M.J.; Gan, H.K.; Reardon, D.A.; Kumthekar, P.; Butowski, N.; Lwin, Z.; Mikkelsen, T.; Nabors, L.B.; Papadopoulos, K.P.; et al. Safety and efficacy of depatuxizumab mafodotin + temozolomide in patients with EGFR-amplified, recurrent glioblastoma: Results from an international phase I multicenter trial. Neuro Oncol. 2019, 21, 106–114. [Google Scholar] [CrossRef]
- Lee, E.Q.; Puduvalli, V.K.; Reid, J.M.; Kuhn, J.G.; Lamborn, K.R.; Cloughesy, T.F.; Chang, S.M.; Drappatz, J.; Yung, W.K.; Gilbert, M.R.; et al. Phase I study of vorinostat in combination with temozolomide in patients with high-grade gliomas: North American Brain Tumor Consortium Study 04-03. Clin. Cancer Res. 2012, 18, 6032–6039. [Google Scholar] [CrossRef]
- Marzolini, C.; Decosterd, L.A.; Shen, F.; Gander, M.; Leyvraz, S.; Bauer, J.; Buclin, T.; Biollaz, J.; Lejeune, F. Pharmacokinetics of temozolomide in association with fotemustine in malignant melanoma and malignant glioma patients: Comparison of oral, intravenous, and hepatic intra-arterial administration. Cancer Chemother. Pharmacol. 1998, 42, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Middleton, M.R.; Grob, J.J.; Aaronson, N.; Fierlbeck, G.; Tilgen, W.; Seiter, S.; Gore, M.; Aamdal, S.; Cebon, J.; Coates, A.; et al. Randomized phase III study of temozolomide versus dacarbazine in the treatment of patients with advanced metastatic malignant melanoma. J. Clin. Oncol. 2000, 18, 158–166. [Google Scholar] [CrossRef]
- Newlands, E.S.; Blackledge, G.R.P.; Slack, J.A.; Rustin, G.J.; Smith, D.B.; Stuart, N.S.; Quarterman, C.P.; Hoffman, R.; Stevens, M.F.G.; Brampton, M.H.; et al. Phase I trial of temozolomide. Br. J. Cancer 1992, 65, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, S.; Csajka, C.; Buclin, T.; Leyvraz, S.; Lejeune, F.; Decosterd, L.A.; Stupp, R. Plasma and cerebrospinal fluid population pharmacokinetics of temozolomide in malignant glioma patients. Clin. Cancer Res. 2004, 10, 3728–3736. [Google Scholar] [CrossRef] [PubMed]
- Portnow, J.; Badie, B.; Chen, M.; Liu, A.; Blanchard, S.; Synold, T.W. The neuropharmacokinetics of temozolomide in patients with resectable brain tumors: Potential implications for the current approach to chemoradiation. Clin. Cancer Res. 2009, 15, 7092–7098. [Google Scholar] [CrossRef] [PubMed]
- Reardon, D.A.; Nabors, L.B.; Mason, W.P.; Perry, J.R.; Shapiro, W.; Kavan, P.; Mathieu, D.; Phuphanich, S.; Cseh, A.; Fu, Y.; et al. Phase I/randomized phase II study of afatinib, an irreversible ErbB family blocker, with or without protracted temozolomide in adults with recurrent glioblastoma. Neuro Oncol. 2015, 17, 430–439. [Google Scholar] [CrossRef]
- Riccardi, A.; Mazzarella, G.; Cefalo, G.; Garre, M.L.; Massimino, M.; Barone, C.; Sandri, A.; Ridola, V.; Ruggiero, A.; Mastrangelo, S.; et al. Pharmacokinetics of temozolomide given three times a day in pediatric and adult patients. Cancer Chemother. Pharmacol. 2003, 52, 459–464. [Google Scholar] [CrossRef]
- Rudek, M.A.; Donehower, R.C.; Statkevich, P.; Batra, V.K.; Cutler, D.L.; Baker, S.D. Temozolomide in patients with advanced cancer: Phase I and pharmacokinetic study. Pharmacotherapy 2004, 24, 16–25. [Google Scholar] [CrossRef]
- Schold, S.C., Jr.; Kuhn, J.G.; Chang, S.M.; Bosik, M.E.; Robins, H.I.; Mehta, M.P.; Spence, A.M.; Fulton, D.; Fink, K.L.; Prados, M.D. A phase I trial of 1,3-bis(2-chloroethyl)-1-nitrosourea plus temozolomide: A North American Brain Tumor Consortium study. Neuro Oncol. 2000, 2, 34–39. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Beumer, J.H.; Tarhini, A.A.; Moschos, S.; Buch, S.C.; Egorin, M.J.; Lin, Y.; Christner, S.; Kirkwood, J.M. Safety and efficacy of decitabine in combination with temozolomide in metastatic melanoma: A phase I/II study and pharmacokinetic analysis. Ann. Oncol. 2013, 24, 1112–1119. [Google Scholar] [CrossRef]
- Wen, P.Y.; Omuro, A.; Ahluwalia, M.S.; Fathallah-Shaykh, H.M.; Mohile, N.; Lager, J.J.; Laird, A.D.; Tang, J.; Jiang, J.; Egile, C.; et al. Phase I dose-escalation study of the PI3K/mTOR inhibitor voxtalisib (SAR245409, XL765) plus temozolomide with or without radiotherapy in patients with high-grade glioma. Neuro Oncol. 2015, 17, 1275–1283. [Google Scholar] [CrossRef]
- Baruchel, S.; Diezi, M.; Hargrave, D.; Stempak, D.; Gammon, J.; Moghrabi, A.; Coppes, M.J.; Fernandez, C.V.; Bouffet, E. Safety and pharmacokinetics of temozolomide using a dose-escalation, metronomic schedule in recurrent paediatric brain tumours. Eur. J. Cancer 2006, 42, 2335–2342. [Google Scholar] [CrossRef]
- Broniscer, A.; Chintagumpala, M.; Fouladi, M.; Krasin, M.J.; Kocak, M.; Bowers, D.C.; Iacono, L.C.; Merchant, T.E.; Stewart, C.F.; Houghton, P.J.; et al. Temozolomide after radiotherapy for newly diagnosed high-grade glioma and unfavorable low-grade glioma in children. J. Neurooncol. 2006, 76, 313–319. [Google Scholar] [CrossRef]
- Broniscer, A.; Gururangan, S.; MacDonald, T.J.; Goldman, S.; Packer, R.J.; Stewart, C.F.; Wallace, D.; Danks, M.K.; Friedman, H.S.; Poussaint, T.Y.; et al. Phase I trial of single-dose temozolomide and continuous administration of o6-benzylguanine in children with brain tumors: A pediatric brain tumor consortium report. Clin. Cancer Res. 2007, 13, 6712–6718. [Google Scholar] [CrossRef] [PubMed]
- Broniscer, A.; Iacono, L.; Chintagumpala, M.; Fouladi, M.; Wallace, D.; Bowers, D.C.; Stewart, C.; Krasin, M.J.; Gajjar, A. Role of temozolomide after radiotherapy for newly diagnosed diffuse brainstem glioma in children: Results of a multiinstitutional study (SJHG-98). Cancer 2005, 103, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Estlin, E.; Lashford, L.; Ablett, S.; Price, L.; Gowing, R.; Gholkar, A.; Kohler, J.; Lewis, I.; Morland, B.; Pinkerton, C.R.; et al. Phase I study of temozolomide in paediatric patients with advanced cancer. Br. J. Cancer 1998, 78, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Horton, T.M.; Thompson, P.A.; Berg, S.L.; Adamson, P.C.; Ingle, A.M.; Dolan, M.E.; Delaney, S.M.; Hedge, M.; Weiss, H.L.; Wu, M.F.; et al. Phase I pharmacokinetic and pharmacodynamic study of temozolomide in pediatric patients with refractory or recurrent leukemia: A Children’s Oncology Group Study. J. Clin. Oncol. 2007, 25, 4922–4928. [Google Scholar] [CrossRef] [PubMed]
- Meany, H.J.; Warren, K.E.; Fox, E.; Cole, D.E.; Aikin, A.A.; Balis, F.M. Pharmacokinetics of temozolomide administered in combination with O6-benzylguanine in children and adolescents with refractory solid tumors. Cancer Chemother. Pharmacol. 2009, 65, 137–142. [Google Scholar] [CrossRef]
- Panetta, J.C.; Kirstein, M.N.; Gajjar, A.; Nair, G.; Fouladi, M.; Heideman, R.L.; Wilkinson, M.; Stewart, C.F. Population pharmacokinetics of temozolomide and metabolites in infants and children with primary central nervous system tumors. Cancer Chemother. Pharmacol. 2003, 52, 435–441. [Google Scholar] [CrossRef]
- Rubie, H.; Geoerger, B.; Frappaz, D.; Schmitt, A.; Leblond, P.; Ndiaye, A.; Aerts, I.; Le Deley, M.C.; Gentet, J.C.; Paci, A.; et al. Phase I study of topotecan in combination with temozolomide (TOTEM) in relapsed or refractory paediatric solid tumours. Eur. J. Cancer 2010, 46, 2763–2770. [Google Scholar] [CrossRef]
- Wagner, L.M.; Crews, K.R.; Iacono, L.C.; Houghton, P.J.; Fuller, C.E.; McCarville, M.B.; Goldsby, R.E.; Albritton, K.; Stewart, C.F.; Santana, V.M. Phase I trial of temozolomide and protracted irinotecan in pediatric patients with refractory solid tumors. Clin. Cancer Res. 2004, 10, 840–848. [Google Scholar] [CrossRef]
- Wagner, L.M.; Villablanca, J.G.; Stewart, C.F.; Crews, K.R.; Groshen, S.; Reynolds, C.P.; Park, J.R.; Maris, J.M.; Hawkins, R.A.; Daldrup-Link, H.E.; et al. Phase I trial of oral irinotecan and temozolomide for children with relapsed high-risk neuroblastoma: A new approach to neuroblastoma therapy consortium study. J. Clin. Oncol. 2009, 27, 1290–1296. [Google Scholar] [CrossRef]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- DuBois, S.G.; Marachelian, A.; Fox, E.; Kudgus, R.A.; Reid, J.M.; Groshen, S.; Malvar, J.; Bagatell, R.; Wagner, L.; Maris, J.M.; et al. Phase I Study of the Aurora A Kinase Inhibitor Alisertib in Combination with Irinotecan and Temozolomide for Patients with Relapsed or Refractory Neuroblastoma: A NANT (New Approaches to Neuroblastoma Therapy) Trial. J. Clin. Oncol. 2016, 34, 1368–1375. [Google Scholar] [CrossRef]
- Chavelli-Lopez, B. Oral toxicity produced by chemotherapy: A systematic review. J. Clin. Exp. Dent. 2014, 6, 81–90. [Google Scholar] [CrossRef]
- Annereau, M.; Hinterlang, M.; Bienayme, H.; Vassal, G.; Pinon, A.; Schmitt, M.; Denis, L.; Lemarchand, C.; Martin, L.; Lemare, F.; et al. Development of a Hospital Compounded, Taste-Masked, Temozolomide Oral Suspension and 5-Year Real-Life Experience in Treating Paediatric Patients. Pharmaceuticals 2022, 15, 555. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ITTS (n = 36) | Safety Set (n = 35) | PK Set (n = 30) | |
|---|---|---|---|
| Age (years) | |||
| Mean ± SD | 52.3 ± 14.8 | 52.0 ± 14.9 | 52.8 ± 14.6 |
| Min/Max | 20/79 | 20/79 | 20/79 |
| Sex, n (%) | |||
| Female | 9 (25.0) | 9 (25.7) | 8 (26.7) |
| Male | 27 (75.0) | 26 (74.3) | 22 (73.3) |
| Height (cm) | |||
| Mean ± SD | 173.22 ± 8.00 | 173.11 ± 8.09 | 172.93 ± 7.97 |
| Min/Max | 157/188 | 157/188 | 157/188 |
| Weight (kg) | |||
| Mean ± SD | 74.45 ± 10.96 | 74.38 ± 11.11 | 74.40 ± 11.79 |
| Min/Max | 58.0/102.0 | 58.0/102.0 | 58.0/102.0 |
| BMI (kg/m2) | |||
| Mean ± SD | 24.79 ± 2.91 | 24.79 ± 2.95 | 24.82 ± 2.93 |
| Min/Max | 19.8/30.6 | 19.8/30.6 | 19.8/30.6 |
| BSA (m2) | |||
| Mean ± SD | 1.89 ± 0.17 | 1.89 ± 0.17 | 1.89 ± 0.18 |
| Min/Max | 1.6/2.3 | 1.6/2.3 | 1.6/2.3 |
| Parameter (Unit) | Statistic | TMZ Capsule (Reference) (n = 30) | Ped-TMZ Oral Suspension (Test) (n = 30) |
|---|---|---|---|
| Tmax (h) | Mean | 0.909 | 0.649 |
| SD | 0.405 | 0.302 | |
| Median | 0.77 | 0.63 | |
| Min-max | 0.33–2.00 | 0.33–1.53 | |
| Cmax (µg/mL) | Mean | 10.506 | 10.939 |
| SD | 3.894 | 2.540 | |
| % CV | 37.1 | 23.2 | |
| AUCt (h·µg/mL) | Mean | 31.471 | 30.467 |
| SD | 5.727 | 4.939 | |
| % CV | 18.2 | 16.2 | |
| AUCinf (h·µg/mL) | Mean | 32.584 | 31.376 |
| SD | 5.840 | 5.062 | |
| % CV | 17.9 | 16.1 | |
| Kel (1/h) | Mean | 0.362 | 0.367 |
| SD | 0.031 | 0.035 | |
| % CV | 9.5 | 9.5 | |
| t1/2 (h) | Mean | 1.928 | 1.909 |
| SD | 0.163 | 0.205 | |
| % CV | 8.4 | 10.7 | |
| %AUCextra (%) | Mean | 3.454 | 2.901 |
| SD | 0.954 | 0.895 | |
| % CV | 27.6 | 30.8 |
| TMZ Oral Capsule (Reference) (n = 30) | Ped-TMZ Oral Suspension (Test) (n = 30) | |
|---|---|---|
| Cmax (µg/mL) | 9.92 | 10.67 |
| Cmax ratio (%) (90% CI) | 107.62 (98.07;118.09) | |
| Cmax % CV | 4.47 | |
| AUCt (h·µg/mL) | 30.96 | 30.09 |
| AUCt ratio (%) (90% CI) | 97.18 (95.05;99.35) | |
| AUCt % CV | 2.53 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ducray, F.; Ramirez, C.; Robert, M.; Fontanilles, M.; Bronnimann, C.; Chinot, O.; Estrade, F.; Durando, X.; Cartalat, S.; Bastid, J.; et al. A Multicenter Randomized Bioequivalence Study of a Novel Ready-to-Use Temozolomide Oral Suspension vs. Temozolomide Capsules. Pharmaceutics 2023, 15, 2664. https://doi.org/10.3390/pharmaceutics15122664
Ducray F, Ramirez C, Robert M, Fontanilles M, Bronnimann C, Chinot O, Estrade F, Durando X, Cartalat S, Bastid J, et al. A Multicenter Randomized Bioequivalence Study of a Novel Ready-to-Use Temozolomide Oral Suspension vs. Temozolomide Capsules. Pharmaceutics. 2023; 15(12):2664. https://doi.org/10.3390/pharmaceutics15122664
Chicago/Turabian StyleDucray, François, Carole Ramirez, Marie Robert, Maxime Fontanilles, Charlotte Bronnimann, Olivier Chinot, Florian Estrade, Xavier Durando, Stéphanie Cartalat, Jeremy Bastid, and et al. 2023. "A Multicenter Randomized Bioequivalence Study of a Novel Ready-to-Use Temozolomide Oral Suspension vs. Temozolomide Capsules" Pharmaceutics 15, no. 12: 2664. https://doi.org/10.3390/pharmaceutics15122664
APA StyleDucray, F., Ramirez, C., Robert, M., Fontanilles, M., Bronnimann, C., Chinot, O., Estrade, F., Durando, X., Cartalat, S., Bastid, J., Bienayme, H., & Lemarchand, C. (2023). A Multicenter Randomized Bioequivalence Study of a Novel Ready-to-Use Temozolomide Oral Suspension vs. Temozolomide Capsules. Pharmaceutics, 15(12), 2664. https://doi.org/10.3390/pharmaceutics15122664