

Dispensing Oral Temozolomide in Children: Precision and Stability of a Novel and Ready to Use Liquid Formulation in Comparison with Capsule Derived Mixtures
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dosage Forms
2.2. Liquid and Soft Food Vehicles
2.3. Accuracy of the Delivered Dose Study (TMZ Assay)
2.4. Stability of TMZ Study
2.5. Samples Analysis
2.6. Statistical Analysis
3. Results
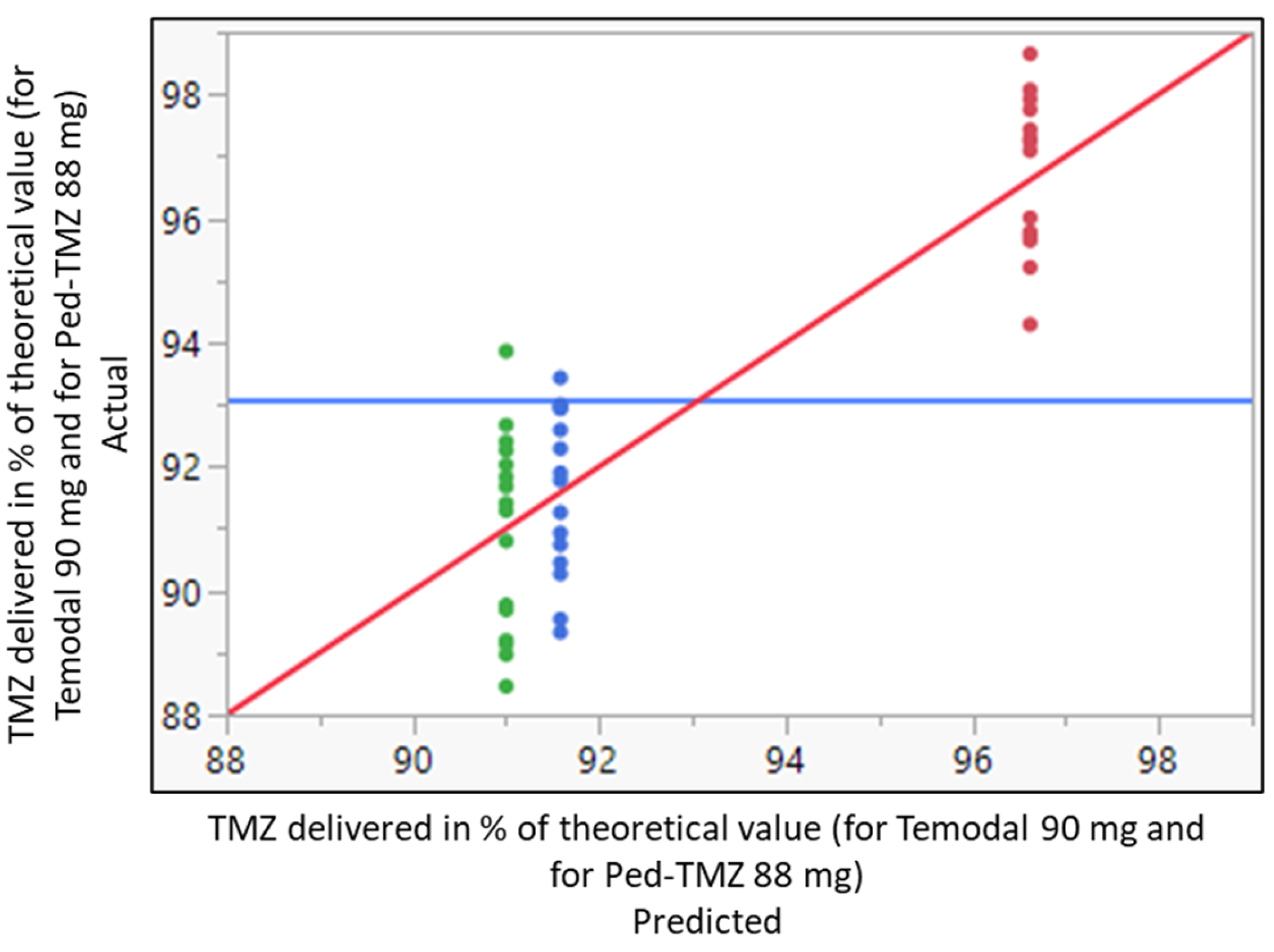
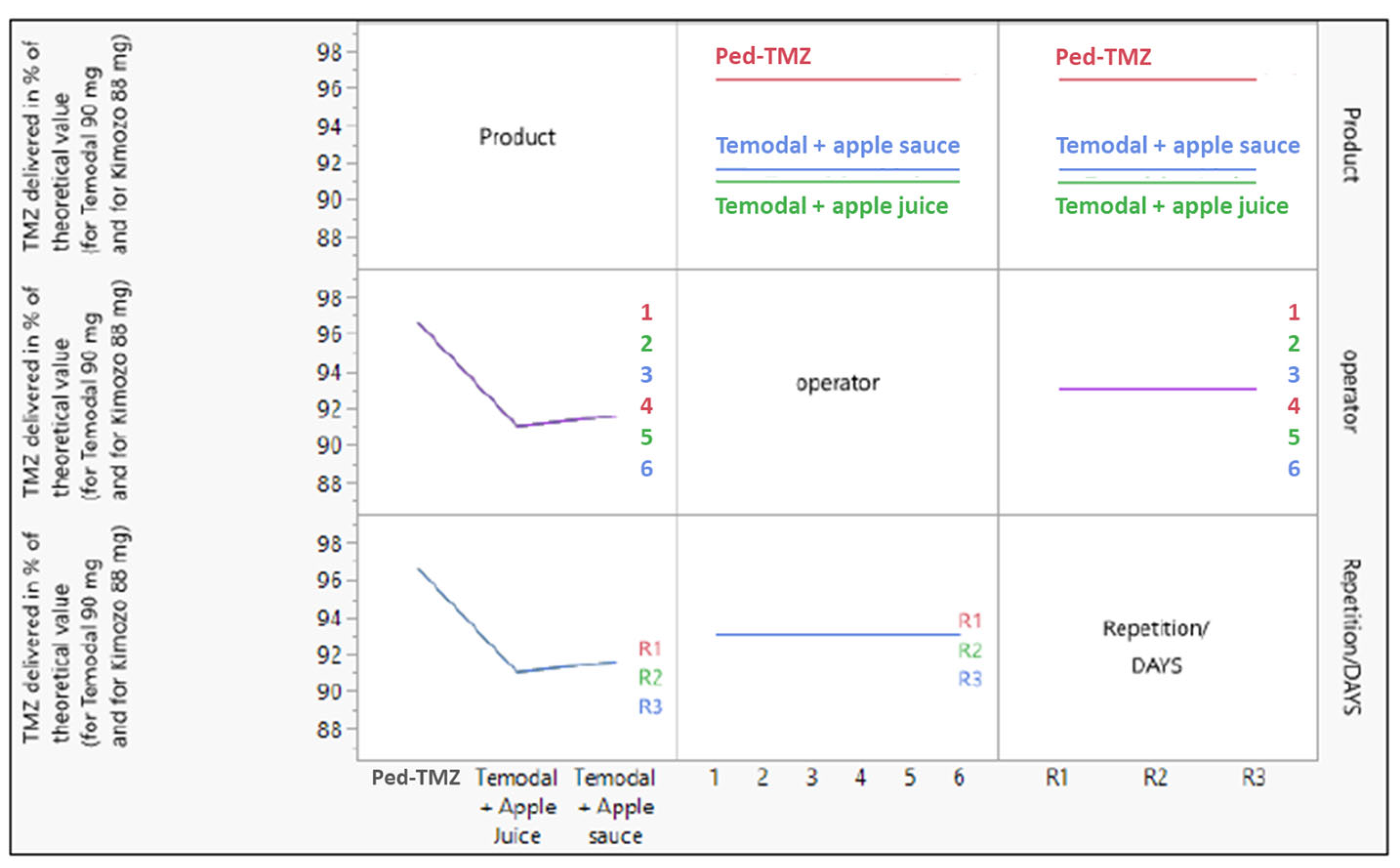
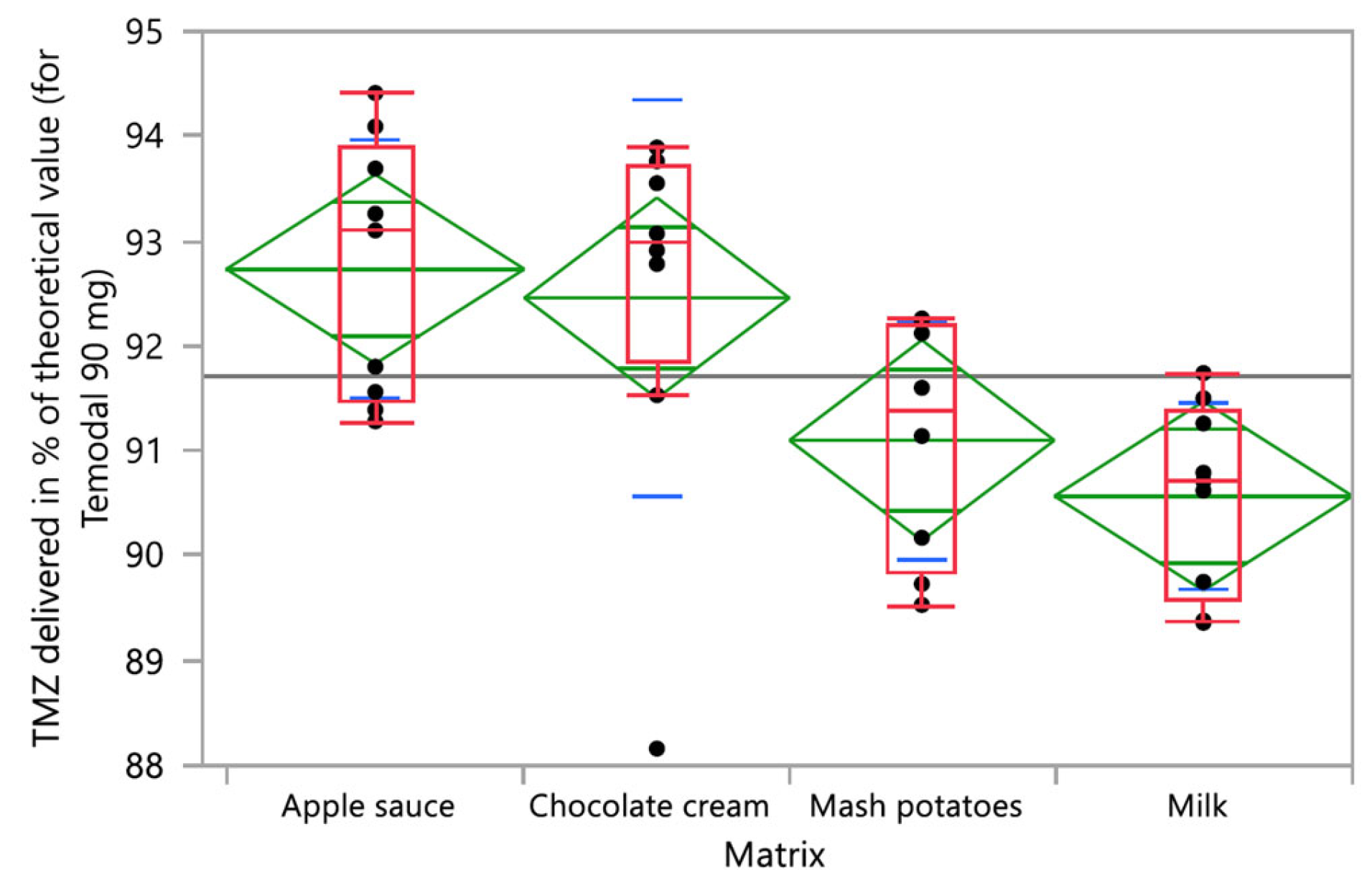
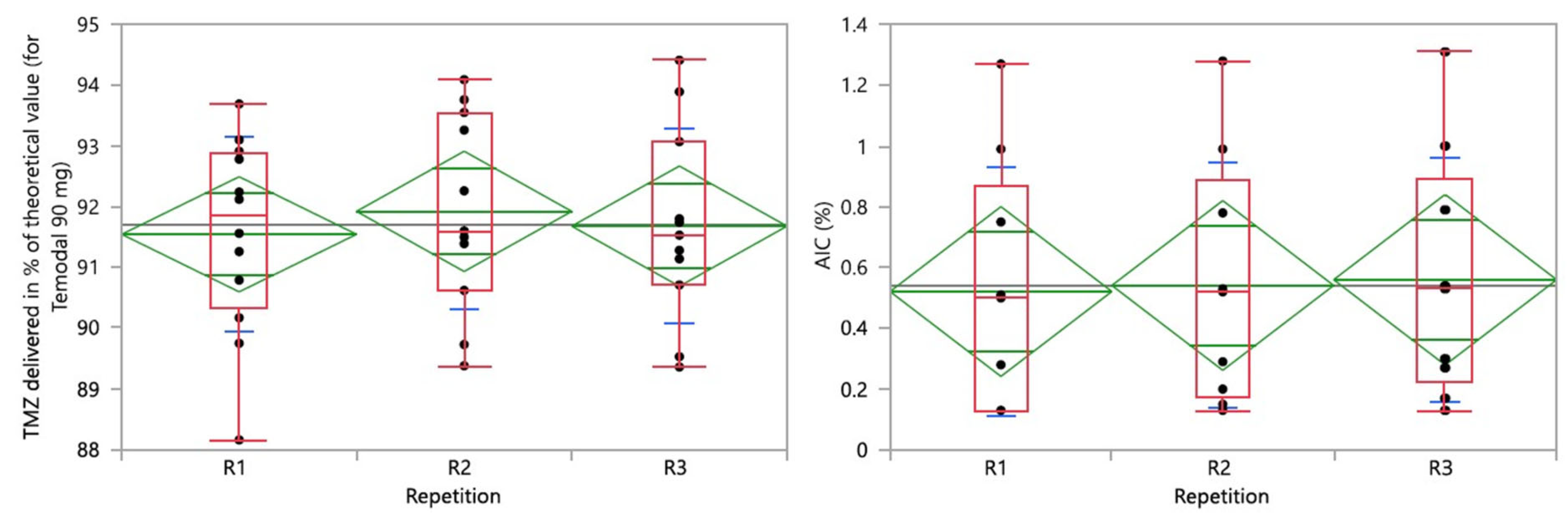
3.1. Accuracy of the Delivered Dose
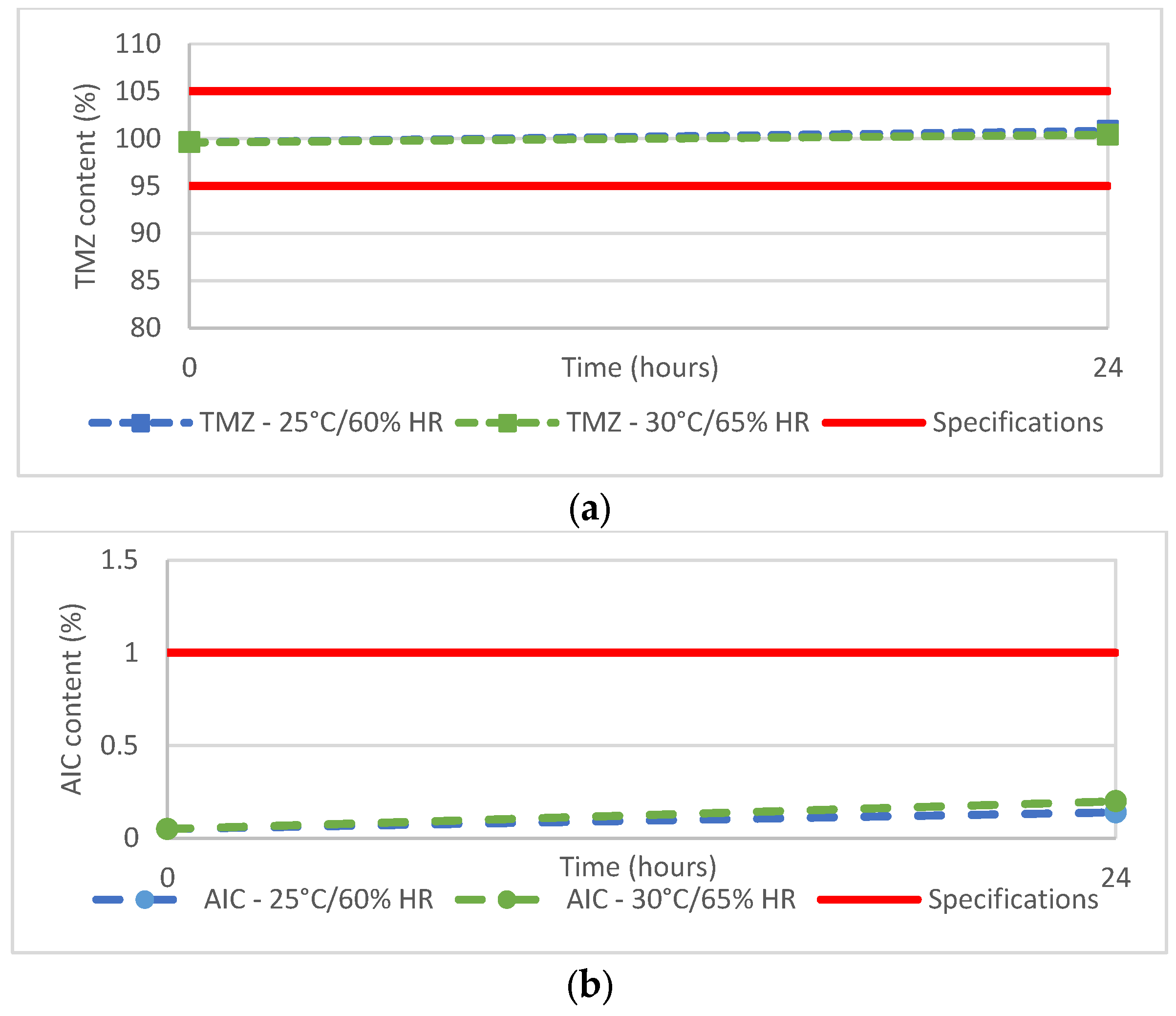
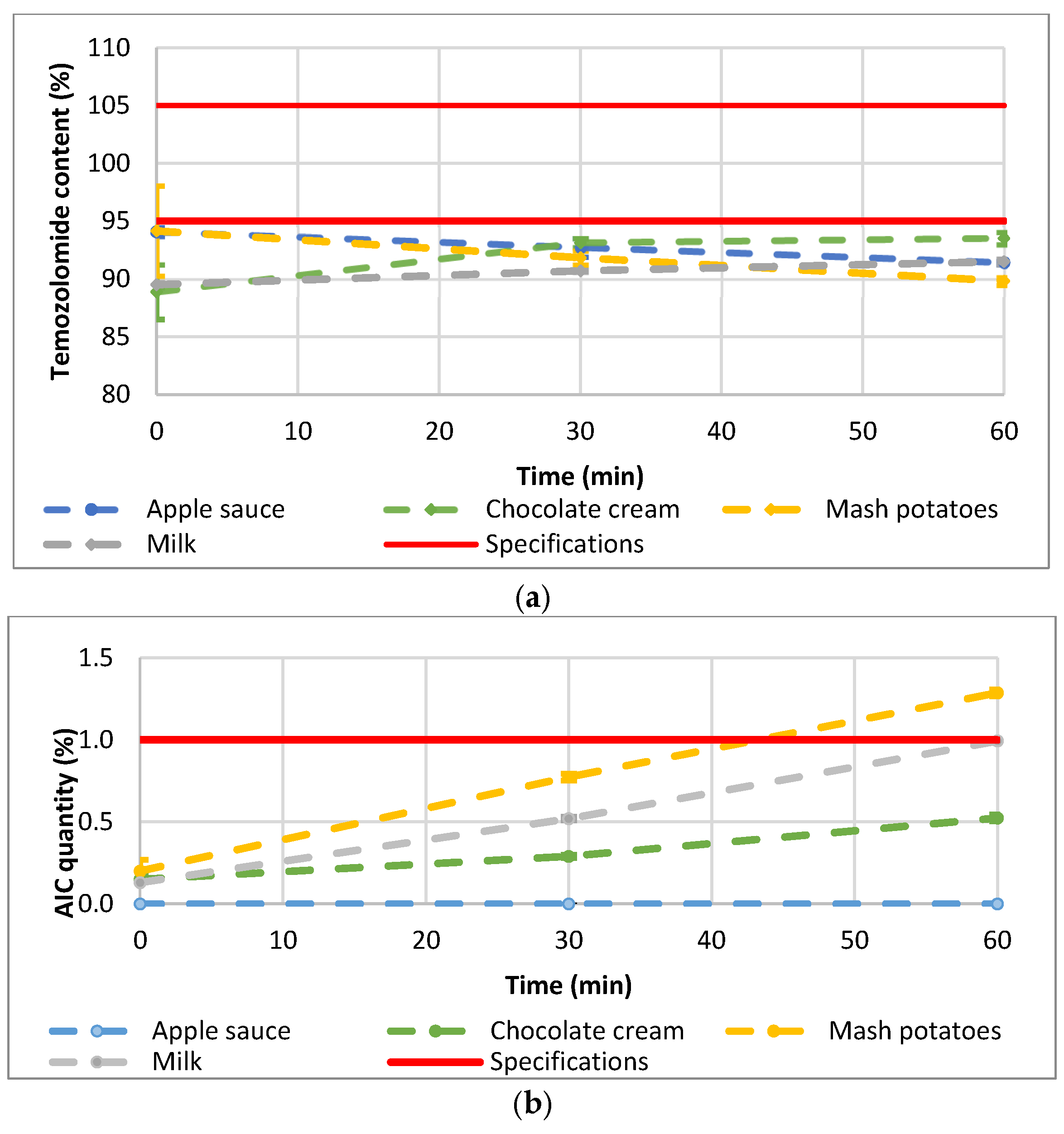
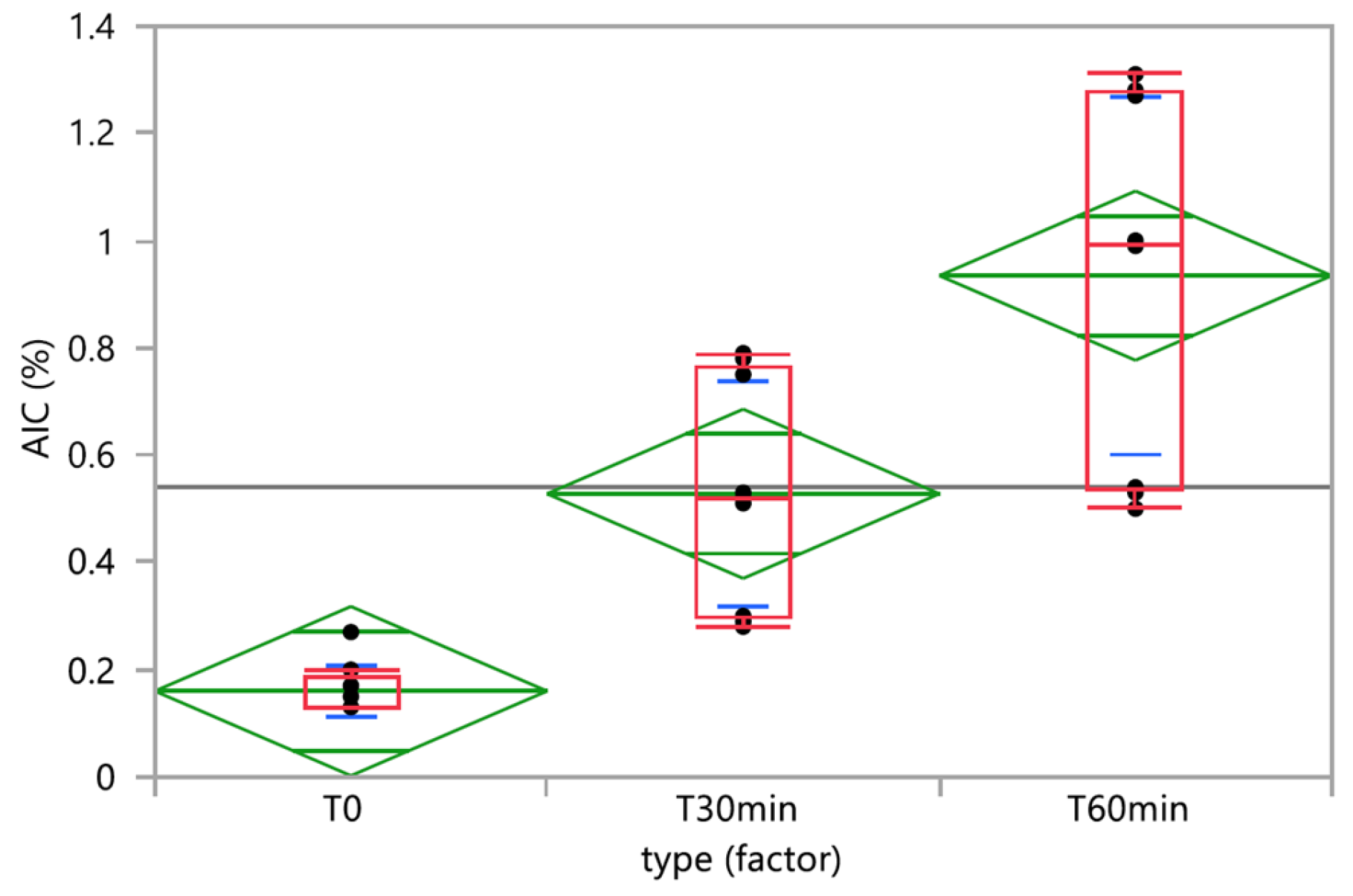
3.2. Chemical and Physical Stability
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brada, M.; Judson, I.; Beale, P.; Moore, S.; Reidenberg, P.; Statkevich, P.; Dugan, M.; Batra, V.; Cutler, D. Phase I dose-escalation and pharmacokinetic study of temozolomide (SCH 52365) for refractory or relapsing malignancies. Br. J. Cancer 1999, 81, 1022–1030. [Google Scholar] [CrossRef]
- EMA. Temodal SmPC. Available online: https://www.ema.europa.eu/en/documents/product-information/temodal-epar-product-information_en.pdf (accessed on 23 November 2023).
- Parikh, N.S.; Howard, S.C.; Chantada, G.; Israels, T.; Khattab, M.; Alcasabas, P.; Lam, C.G.; Faulkner, L.; Park, J.R.; London, W.B.; et al. SIOP-PODC adapted risk stratification and treatment guidelines: Recommendations for neuroblastoma in low- and middle-income settings. Pediatr. Blood Cancer 2015, 62, 1305–1316. [Google Scholar] [CrossRef]
- Moreno, L.; Rubie, H.; Varo, A.; Le Deley, M.C.; Amoroso, L.; Chevance, A.; Garaventa, A.; Gambart, M.; Bautista, F.; Valteau-Couanet, D.; et al. Outcome of children with relapsed or refractory neuroblastoma: A meta-analysis of ITCC/SIOPEN European phase II clinical trials. Pediatr. Blood Cancer 2017, 64, 25–31. [Google Scholar] [CrossRef]
- Children’s Cancer and Leukaemia Group. Options for the Treatment of Patients with Relapsed/Progressive High-Risk Neuroblastoma. 2015. Available online: https://www.cclg.org.uk/write/MediaUploads/Member%20area/Treatment%20guidelines/CCLG_Relapsed_Progressive_High_Risk_Neuroblastoma_Guidelines_March_2015_FINAL.pdf (accessed on 23 November 2023).
- Hill, R.M.; Plasschaert, S.L.A.; Timmermann, B.; Dufour, C.; Aquilina, K.; Avula, S.; Donovan, L.; Lequin, M.; Pietsch, T.; Thomale, U.; et al. Relapsed Medulloblastoma in Pre-Irradiated Patients: Current Practice for Diagnostics and Treatment. Cancers 2022, 14, 126. [Google Scholar] [CrossRef]
- Defachelles, A.S.; Bogart, E.; Casanova, M.; Merks, J.H.M.; Bisogno, G.; Calareso, G.; Gallego Melcon, S.; Gatz, S.A.; Le Deley, M.C.; McHugh, K.; et al. Randomized Phase II Trial of Vincristine-Irinotecan With or Without Temozolomide, in Children and Adults With Relapsed or Refractory Rhabdomyosarcoma: A European Paediatric Soft Tissue Sarcoma Study Group and Innovative Therapies for Children With Cancer Trial. J. Clin. Oncol. 2021, 39, 2979–2990. [Google Scholar] [CrossRef]
- Nygren, H.; Eksborg, S. Stability of temozolomide in solutions aimed for oral treatment prepared from a commercially available powder for infusion. Pharm. Methods 2012, 3, 198–202. [Google Scholar] [CrossRef]
- EMA. EMEA/CHMP/PEG/194810/2005, Reflection Paper: Formulations of Choice for the Paediatric Population. 2006. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-formulations-choice-paediatric-population_en.pdf (accessed on 23 November 2023).
- Bracken, L.; McDonough, E.; Ashleigh, S.; Wilson, F.; Shakeshaft, J.; Ohia, U.; Mistry, P.; Jones, H.; Kanji, N.; Liu, F.; et al. Can children swallow tablets? Outcome data from a feasibility study to assess the acceptability of different-sized placebo tablets in children (creating acceptable tablets (CAT)). BMJ Open 2020, 10, e036508. [Google Scholar] [CrossRef]
- Venables, R.; Batchelor, H.; Hodson, J.; Stirling, H.; Marriott, J. Determination of formulation factors that affect oral medicines acceptability in a domiciliary peadiatric population. Int. J. Pharm. 2015, 480, 55–62. [Google Scholar] [CrossRef]
- Richey, R.H.; Craig, J.V.; Shah, U.U.; Nunn, A.J.; Turner, M.A.; Barker, C.E.; Ford, J.L.; Peak, M. MODRIC–Manipulation of drugs in children. Int. J. Pharm. 2013, 457, 339–341. [Google Scholar] [CrossRef]
- Bordes-Picard, F.; Buffangeix, C.; Celadon, M.-J.; Edeline, J.; Fayolle, N.; Gestin, P.; Lemarchand, C.; Levacher, E.; Marçon, F.; Mamecier, L.; et al. Tailor-made medication: Practices and prospects. STP Pharma Prat. 2020, 6, 2–6. [Google Scholar]
- EMA. EMA/CHMP/QWP/805880/2012_Rev.2, Guideline on Pharmaceutical Development of Medicines for Paediatric Use. 2013. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-pharmaceutical-development-medicines-paediatric-use_en.pdf (accessed on 23 November 2023).
- Annereau, M.; Hinterlang, M.; Bienayme, H.; Vassal, G.; Pinon, A.; Schmitt, M.; Denis, L.; Lemarchand, C.; Martin, L.; Lemare, F.; et al. Development of a Hospital Compounded, Taste-Masked, Temozolomide Oral Suspension and 5-Year Real-Life Experience in Treating Paediatric Patients. Pharmaceuticals 2022, 15, 555. [Google Scholar] [CrossRef]
- Richey, R.H.; Shah, U.U.; Peak, M.; Craig, J.V.; Ford, J.L.; Barker, C.E.; Nunn, A.J.; Turner, M.A. Manipulation of drugs to achieve the required dose is intrinsic ot peadiatric practice but is not supported by guidelines or evidence. BMC Pediatr. 2013, 13, 81. [Google Scholar] [CrossRef]
- Zahn, J.; Hoerning, A.; Trollmann, R.; Rascher, W.; Neubert, A. Manipulation of medicinal products for oral Adminitration to paediatric patients at a german university hospital: An observational study. Pharmaceutics 2020, 12, 583. [Google Scholar] [CrossRef]
- FDA. Use of Liquids and/or Soft Foods as Vehicles for Drug Administration: General Considerations for Selection and In Vitro Methods for Product Quality Assessments. 2018. Available online: https://www.fda.gov/media/114872/download (accessed on 23 November 2023).
- EMA. EMA/PDCO/381728/2014, Draft Inventory of Paediatric Therapeutic Needs–Paediatric Oncology. 2014. Available online: https://www.ema.europa.eu/en/documents/other/draft-inventory-paediatric-therapeutic-needs-paediatric-oncology_en.pdf (accessed on 23 November 2023).
- Martir, J.; Flanagan, T.; Mann, J.; Fotaki, N. Co-administration of Paediatric Medicines with Food and Drinks in the Context of Their Physicochemical Properties—A Global Perspective on Practices and Recommendations. AAPS J. 2020, 22, 54. [Google Scholar] [CrossRef]
- Denny, B.J.; Wheelhouse, R.T.; Stevens, M.F.; Tsang, L.L.; Slack, J.A. NMR and molecular modeling investigation of the mechanism of activation of the antitumor drug temozolomide and its interaction with DNA. Biochemistry 1994, 33, 9045–9051. [Google Scholar] [CrossRef]
- Annereau, M.; Bastid, J.; Bienayme, H.; Lemare, F.; Schmitt, M.; Tortolano, L.; Abbou, S. Oral Suspension of Temozolomide. European Patent EP 3,613,436, 26 February 2020. [Google Scholar]
- EMA. CPMP/ICH/381/95, ICH Topic Q 2 (R1) Validation of Analytical Procedures: Text and Methodology. 1995. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-q-2-r1-validation-analytical-procedures-text-methodology-step-5_en.pdf (accessed on 23 November 2023).
- Van der Vossen, A.; Al-Hassany, L.; Buljac, S.; Brugma, J.D.; Vulto, A.; Hanff, L. Manipulation of oral medication for children by parents and nurses occurs frequently and is often not supported by instructions. Acta Paediatr. 2019, 108, 1475–1481. [Google Scholar] [CrossRef]
- Allen, L.V., Jr.; Stiles, M.L.; Prince, S.J.; McLaury, H.J.; Sylvestri, M.F. Stability of ramipril in water, apple juice, and applesauce. Am. J. Health-Syst. Pharm. 1995, 52, 2433–2436. [Google Scholar] [CrossRef]
- Carrier, M.N.; Garinot, O.; Vitzling, C. Stability and compatibility of tegaserod from crushed tablets mixed in beverages and foods. Am. J. Health-Syst. Pharm. 2004, 61, 1135–1142. [Google Scholar] [CrossRef]
- Manrique, Y.J.; Lee, D.J.; Islam, F.; Nissen, L.M.; Cichero, J.A.; Stokes, J.R.; Steadman, K.J. Crushed tablets: Does the administration of food vehicles and thickened fluids to aid medication swallowing alter drug release? J. Pharm. Pharm. Sci. 2014, 17, 207–219. [Google Scholar] [CrossRef]
- Wu, K.W.; Zheng, K.; Tian, L.; Xia, L.; Hwang, S.Y.; Nwakama, P.E.; Sun, W.J.; Kim, M.J.; Tampal, N.; Xu, X.; et al. The effect of food vehicles on in vitro performance of pantoprazole sodium delayed release sprinkle formulation. Int. J. Pharm. 2023, 635, 122737. [Google Scholar] [CrossRef]
- Freerks, L.; Sucher, W.; Tarnow, M.-J.; Eckert, C.; Klein, S. Vehicles for durg adminitration to children: Results and learnings form an in-depth screening of FDA-recommended liquids and soft foods for prodcut quality assessment. Pharm. Res. 2022, 39, 497–509. [Google Scholar]
- Nguyen, D.; Secretan, P.-H.; Auvity, S.; Vidal, F.; Postaire, M.; Cisternino, S.; Schlatter, J. Assessment of practices for suspensed oral durgs by tablet crushing in pediatric units. Eur. J. Pharm. Biopharm. 2020, 157, 175–182. [Google Scholar] [CrossRef]
- Kersten, E.; Barry, A.; Klein, S. Physicochemical characterisation of fluids and soft foods frequently mixed with oral drug formulations prior to administration to children. Pharmazie 2016, 71, 122–127. [Google Scholar]
- Bakshi, R.A.; Aslam, A.; Khan, Z.S.; Fayaz, S.; Dar, B.N. Physiochemical, sensorial, and rheological characteristics of sauce developed from Kashmiri apples: Influence of cultivars and storage conditions. Food Sci. Nutr. 2022, 10, 1685–1693. [Google Scholar] [CrossRef]
- Batchelor, H.; Kaukonen, A.M.; Klein, S.; Davit, B.; Ju, R.; Ternik, R.; Heimbach, T.; Lin, W.; Wnag, J.; Storey, D. Fodd effects in paediatric medicines development for products co-administered with food. Int. J. Pharm. 2018, 536, 530–535. [Google Scholar] [CrossRef]
- Ernest, T.B.; Elder, D.P.; Martini, L.G.; Roberts, M.; Ford, J.L. Developing paediatric medicines: Identifying the needs and recognizing the challenges. J. Pharm. Pharmacol. 2007, 59, 1043–1055. [Google Scholar] [CrossRef] [PubMed]
- Standing, J.F.; Tuleu, C. Paediatric formulations–Getting to the heart of the problem. Int. J. Pharm. 2005, 300, 56–66. [Google Scholar] [CrossRef] [PubMed]
- WHO. Development of Paediatric Medicines: Points to Consider in Formulation. Annex 5, WHO Technical Report Series 970. 2012. Available online: https://cdn.who.int/media/docs/default-source/medicines/norms-and-standards/guidelines/trs970/annex5trs-970.pdf?sfvrsn=699cdb68_8&download=true (accessed on 23 November 2023).
- Ducray, F.; Ramirez, C.; Robert, M.; Maxime, F.; Bronnimann, C.; Chinot, O.L.; Estrade, F.; Durando, X.; Bastid, J.; Bienaymé, H.; et al. A bioequivalence study of a novel liquid and ready-to-use temozolomide oral suspension and temozolomide capsules in patients with primary tumors central nervous system malignancies. J. Clin. Oncol. 2022, 40, e22008. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Liquid/Soft Food | Brand Name | Packaging | pH | Texture |
|---|---|---|---|---|
| Apple juice | Joker | 1 L bottle | 3.5 | Liquid |
| Apple sauce | Andros | 100 g pot | 3.8 | Soft food |
| Chocolate cream | Danette | 125 g pot | 6.8 | Soft food |
| Infant milk * | Candia baby | 250 mL bottle | 6.8 | Liquid |
| Mash potatoes | Mousseline | 130 g sachet | 6.4 | Soft food |
| Apple Juice | Apple Sauce | Chocolate Cream | Infant Milk | Mash Potatoes | |
|---|---|---|---|---|---|
| Calories (kJ) | 187 | 296 | 516 | 261 | 280 |
| Calories (kcal) | 44 | 70 | 122 | 62 | 67 |
| Fat (g) | 0 | 0.2 | 3.0 | 3.2 | 0.8 |
| Carbohydrates (g) | 10 | 16.0 | 20.0 | 7.0 | 2.5 |
| Proteins (g) | 0 | 0.3 | 3.3 | 1.4 | 2.4 |
| Group | Standard Deviation | Median Absolution Deviation (Robust Deviation Measure) |
|---|---|---|
| Ped-TMZ | 1.246784 | 1.104444 |
| Temodal + apple juice | 1.488973 | 1.156667 |
| Temodal + apple sauce | 1.356263 | 1.155000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lemarchand, C.; Bienaymé, H.; Rieutord, A.; Abbou, S.; Annereau, M.; Bastid, J. Dispensing Oral Temozolomide in Children: Precision and Stability of a Novel and Ready to Use Liquid Formulation in Comparison with Capsule Derived Mixtures. Pharmaceutics 2023, 15, 2711. https://doi.org/10.3390/pharmaceutics15122711
Lemarchand C, Bienaymé H, Rieutord A, Abbou S, Annereau M, Bastid J. Dispensing Oral Temozolomide in Children: Precision and Stability of a Novel and Ready to Use Liquid Formulation in Comparison with Capsule Derived Mixtures. Pharmaceutics. 2023; 15(12):2711. https://doi.org/10.3390/pharmaceutics15122711
Chicago/Turabian StyleLemarchand, Caroline, Hugues Bienaymé, André Rieutord, Samuel Abbou, Maxime Annereau, and Jeremy Bastid. 2023. "Dispensing Oral Temozolomide in Children: Precision and Stability of a Novel and Ready to Use Liquid Formulation in Comparison with Capsule Derived Mixtures" Pharmaceutics 15, no. 12: 2711. https://doi.org/10.3390/pharmaceutics15122711
APA StyleLemarchand, C., Bienaymé, H., Rieutord, A., Abbou, S., Annereau, M., & Bastid, J. (2023). Dispensing Oral Temozolomide in Children: Precision and Stability of a Novel and Ready to Use Liquid Formulation in Comparison with Capsule Derived Mixtures. Pharmaceutics, 15(12), 2711. https://doi.org/10.3390/pharmaceutics15122711