
In Vitro Antimicrobial Photodynamic Therapy for Pseudomonas aeruginosa (P. aeruginosa) and methicillin-resistant Staphylococcus aureus (MRSA) Inhibition Using a Green Light Source

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. In Vitro Antimicrobial Photodynamic Therapy
2.1.1. Photosensitizer (PS)
2.1.2. Pathogens Cell Culture
2.1.3. Protocol for aPDT
2.1.4. Bacterial Photosensitization and Viable Cell Counting
2.2. Green Light Source Characterization
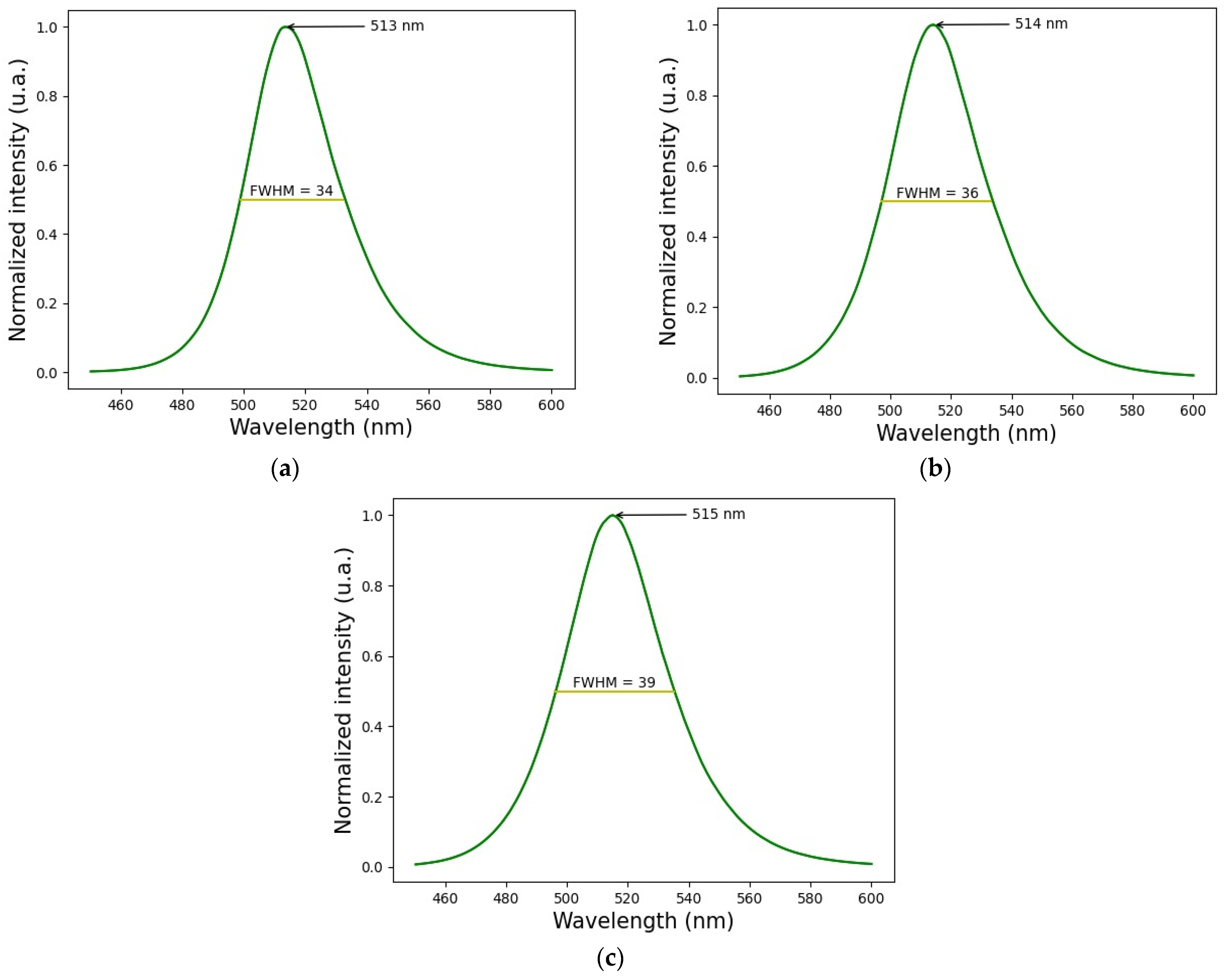
2.2.1. Wavelength
2.2.2. Light Source Stability
2.2.3. Light Source Principal Parameters
2.2.4. Light Source Control
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Correia, J.H.; Rodrigues, J.A.; Pimenta, S.; Dong, T.; Yang, Z. Photodynamic Therapy Review: Principles, Photosensitizers, Applications, and Future Directions. Pharmaceutics 2021, 13, 1332. [Google Scholar] [CrossRef] [PubMed]
- Plaetzer, K.; Berneburg, M.; Kiesslich, T.; Maisch, T. New applications of photodynamic therapy in biomedicine and biotechnology. Biomed. Res. Int. 2013, 2013, 161362. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.W.; Oh, G.; Ahn, J.C.; Chung, E. 0 Non-Oncologic Applications of Nanomedicine-Based Phototherapy. Biomedicines 2021, 9, 113. [Google Scholar] [CrossRef] [PubMed]
- Calzavara-Pinton, P.G.; Rossi, M.T.; Aronson, E.; Sala, R.; Italian Group For Photodynamic Therapy. A retrospective analysis of real-life practice of off-label photodynamic therapy using methyl aminolevulinate (MAL-PDT) in 20 Italian dermatology departments. Part 1, inflammatory and aesthetic indications. Photochem. Photobiol. Sci. 2013, 12, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Stender, I.M.; Na, R.; Fogh, H.; Gluud, C.; Wulf, H.C. Photodynamic therapy with 5-aminolaevulinic acid or placebo for recalcitrant foot and hand warts: Randomised double-blind trial. Lancet 2000, 355, 963–966. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.T.; Kim, J.H.; Shim, J.; Lee, J.H.; Lee, D.Y.; Lee, J.H.; Yang, J.M. Photodynamic therapy using a new formulation of 5-aminolevulinic acid for wrinkles in Asian skin: A randomized controlled split face study. J. Dermatol. Treat. 2015, 26, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.M.; Adelzadeh, L.; Wu, J.J. Photodynamic therapy for psoriasis. J. Dermatol. Treat. 2015, 26, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Jerjes, W.; Upile, T.; Hamdoon, Z.; Mosse, C.A.; Akram, S.; Morley, S.; Hopper, C. Interstitial PDT for vascular anomalies. Lasers Surg. Med. 2011, 43, 357–365. [Google Scholar] [CrossRef]
- Comacchi, C.; Bencini, P.L.; Galimberti, M.G.; Cappugi, P.; Torchia, D. Topical photodynamic therapy for idiopathic hirsutism and hypertrichosis. Plast. Reconstr. Surg. 2012, 129, 1012e–1014e. [Google Scholar] [CrossRef]
- Bruscino, N.; Lotti, T.; Rossi, R. Photodynamic therapy for hypertrophic scarring: A promising choice. Photodermatol. Photoimmunol. Photomed. 2011, 27, 334–335. [Google Scholar] [CrossRef]
- Linares-González, L.; Ródenas-Herranz, T.; Sáenz-Guirado, S.; Ruiz-Villaverde, R. Successful response to photodynamic therapy with 5-aminolevulinic acid nanoemulsified gel in a patient with universal alopecia areata refractory to conventional treatment. Dermatol. Ther. 2020, 33, e13416. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, E.H.C.; Fauser, S.; Breukink, M.B.; Blanco-Garavito, R.; Groenewoud, J.M.M.; Keunen, J.E.E.; Peters, P.J.H.; Dijkman, G.; Souied, E.H.; Maclaren, R.E.; et al. Half-dose photodynamic therapy versus high-density subthreshold micropulse laser treatment in patients with chronic central serous chorioretinopathy. Ophthalmology 2018, 125, 1547–1555. [Google Scholar] [CrossRef]
- Díaz-Dávalos, C.D.; Carrasco-Quiroz, A.; Rivera-Díez, D. Neovascularization corneal regression in patients treated with photodynamic therapy with verteporfin. Rev. Med. Inst. Mex. Seguro Soc. 2016, 54, 164–169. [Google Scholar]
- Houthoofd, S.; Vuylsteke, M.; Mordon, S.; Fourneau, I. Photodynamic therapy for atherosclerosis. The potential of indocyanine green. Photodiagnosis Photodyn. Ther. 2020, 29, 101568. [Google Scholar] [CrossRef]
- Li, C.Z.; Cheng, L.F.; Wang, Z.Q.; Gu, Y. Attempt of photodynamic therapy on esophageal varices. Lasers Med. Sci. 2009, 24, 167–171. [Google Scholar] [CrossRef]
- Mitton, D.; Ackroyd, R. A brief overview of photodynamic therapy in Europe. Photodiagnosis Photodyn. Ther. 2008, 5, 103–111. [Google Scholar] [CrossRef]
- Lee, C.N.; Hsu, R.; Chen, H.; Wong, T.W. Daylight Photodynamic Therapy: An Update. Molecules 2020, 25, 5195. [Google Scholar] [CrossRef] [PubMed]
- Kharkwal, G.; Sharma, S.; Huang, Y.; Dai, T.; Hamblin, M. Photodynamic therapy for infections: Clinical applications. Lasers Surg. Med. 2011, 43, 755–767. [Google Scholar] [CrossRef] [PubMed]
- Van Der Snoek, E.; Robinson, D.; Van Hellemond, J.; Neumann, H. A review of photodynamic therapy in cutaneous leishmaniasis. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 918–922. [Google Scholar] [CrossRef]
- Demartis, S.; Obinu, A.; Gavini, E.; Giunchedi, P.; Rassu, G. Nanotechnology-based rose Bengal: A broad-spectrum biomedical tool. Dye. Pigment. 2021, 188, 109236. [Google Scholar] [CrossRef]
- Yoon, I.; Li, J.Z.; Shim, Y.K. Advance in photosensitizers and light delivery for photodynamic therapy. Clin. Endosc. 2013, 46, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Austin, E.; Jagdeo, J. An In Vitro Approach to Photodynamic Therapy. J. Vis. Exp. 2018, 138, 58190. [Google Scholar]
- Dolmans, D.E.J.G.J.; Fukumura, D.; Jain, R.K. Photodynamic therapy for cancer. Nat. Rev. Cancer 2003, 3, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Chilakamarthi, U.; Giribabu, L. Photodynamic Therapy: Past, Present and Future. Chem. Rec. 2017, 17, 775–802. [Google Scholar] [CrossRef] [PubMed]
- Rezzoug, H.; Bezdetnaya, L.; A’amar, O.; Merlin, J.L.; Guillemin, F. Parameters affecting photodynamic activity of Foscan® or metatetra(hydroxyphenyl)chlorin (mTHPC) in vitro and in vivo. Lasers Med. Sci. 1998, 13, 119–125. [Google Scholar] [CrossRef]
- Coutier, S.; Mitra, S.; Bezdetnaya, L.N.; Parache, R.M.; Georgakoudi, I.; Foster, T.H.; Guillemin, F. Effects of fluence rate on cell survival and photobleaching in meta-tetra-(hydroxyphenyl) chlorin-photosensitized Colo 26 multicell tumor spheroids. Photochem. Photobiol. 2001, 73, 297–303. [Google Scholar] [CrossRef]
- Chen, D.; Zheng, H.; Huang, Z.; Lin, H.; Ke, Z.; Xie, S.; Li, B. Light-emitting diode-based illumination system for in vitro photodynamic therapy. Int. J. Photoenergy 2012, 2012, 920671. [Google Scholar] [CrossRef]
- Hartl, B.A.; Hirschberg, H.; Marcu, L.; Cherry, S.R. Characterizing low fluence thresholds for in vitro photodynamic therapy. Biomed. Opt. Express. 2015, 6, 770–779. [Google Scholar] [CrossRef] [PubMed]
- Stolik, S.; Gallegos, E.; de la Rosa, J.M.; Yonadab, F. Sistema Para La Fotoirradiación De Medios Biológicos, Físicos Y Quimicos Con Controlador De Temperatura. Mexico Patent MX 343487 B, 9 November 2016. [Google Scholar]
- Hernández-Quintanar, L.; Stolik, S.; de la Rosa, J.M. Development of an irradiation system for photodynamic therapy with dosimetric control. In Proceedings of the CONIELECOMP 2011, 21st International Conference on Electrical Communications and Computers, San Andres Cholula, Mexico, 28 February–2 March 2011. [Google Scholar]
- Kim, M.M.; Darafsheh, A. Light Sources and Dosimetry Techniques for Photodynamic Therapy. Photochem. Photobiol. 2020, 96, 280–294. [Google Scholar] [CrossRef]
- LabX. Available online: https://www.labx.com/item/well-plate-illuminator-in-various-colours/13619913 (accessed on 27 August 2023).
- Zhang, K.; Timilsina, S.; Waguespack, M.; Kercher, E.M.; Spring, B.Q. An open-source LED array illumination system for automated multiwell plate cell culture photodynamic therapy experiments. Sci. Rep. 2022, 12, 19341. [Google Scholar] [CrossRef]
- Bounds, A.D.; Bailey, R.D.; Adams, C.T.; Callaghan, D.C.; Girkin, J.M. LightBox: A multiwell plate illumination system for photoactive molecule characterization. J. Biophotonics. 2021, 14, e202000481. [Google Scholar] [CrossRef] [PubMed]
- Navarro, J.; Morales, O.; Hernández, L.; López, F.; Fabila, D.; de la Rosa, J.; Valor, A.; Bridin, P.; Guha, C.; Tomé, W.; et al. Photoirradiation Systems for In-Vitro Cultured Cells Phototherapy and Photobiology experiments. In Proceedings of the VIII Internacional Tecnolaser, Havana, Cuba, 1 April 2016. [Google Scholar]
- Liu, H.; Daly, L.; Rudd, G.; Khan, A.P.; Mallidi, S.; Liu, Y.; Cuckov, F.; Hasan, T.; Celli, J.P. Development and evaluation of a low-cost, portable, LED-based device for PDT treatment of early-stage oral cancer in resource-limited settings. Lasers Surg. Med. 2019, 51, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Moloudi, K.; Sarbadhikary, P.; Abrahamse, H.; George, B.P. Understanding the Photodynamic Therapy Induced Bystander and Abscopal Effects: A Review. Antioxidants 2023, 12, 1434. [Google Scholar] [CrossRef] [PubMed]
- Morley, V.J.; Woods, R.J.; Read, A.F. Bystander Selection for Antimicrobial Resistance: Implications for Patient Health. Trends Microbiol. 2019, 27, 864–877. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Shao, C. Research progress of radiation induced bystander and abscopal effects in normal tissue. Radiat. Med. Prot. 2020, 1, 69–74. [Google Scholar] [CrossRef]
- Mothersill, C.; Seymour, C. Radiation-induced bystander effects: Past history and future directions. Radiat. Res. 2001, 155, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Dahle, J.; Bagdonas, S.; Kaalhus, O.; Olsen, G.; Steen, H.B.; Moan, J. The bystander effect in photodynamic inactivation of cells. Biochim. Biophys. Acta 2000, 1475, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, Y.; Yoshii, D.; Katsuragi, H.; Shinkai, K. Effect of Laser Irradiation Modes and Photosensitizer Types on Antimicrobial Photodynamic Therapy (aPDT) for Streptococcus sobrinus in the Crown Dentin of Bovine Teeth: An Experimental In Vitro Study. Dent. J. 2024, 12, 59. [Google Scholar] [CrossRef]
- Silva Furtado, G.; Benini Paschoal, M.; Santos Grenho, L.; Dias Neves Lago, A. Does pre-irradiation time influence the efficacy of antimicrobial photodynamic therapy? Photodiagnosis Photodyn. Ther. 2020, 31, 101884, ISSN 1572-1000. [Google Scholar] [CrossRef]
- Hernández Quintanar, L.F.; López Silva, F.Y.; Fabila Bustos, D.A.; Serrano Navarro, J.; de La Rosa Vázquez, J.M.; Brodin, P.N.; Guha, C.; Tomé, W.A.; Stolik Isakina, S. In Vitro Photoirradiation System for Simultaneous Irradiation with Different Light Doses at a Fixed Temperature. Photomed. Laser Surg. 2016, 34, 108–115. [Google Scholar] [CrossRef]
- Larraga-Urdaz, A.L.; Vizcaíno, A.; Valledor, M.; Ferrero, F.; Campo, J.C.; López, A.; Costa-Fernández, J.M.; Fernández-Sánchez, M.L. An affordable automated LED array system for optimizing photodynamic therapy protocols. Biosens. Bioelectron. X 2023, 14, 100383. [Google Scholar] [CrossRef]
- Katz, S.; Backeris, P.; Merck, C.; Suprun, M.; D’Souza, S.; Bishop, D.F.; Desnick, R.J.; Moore, K.; Ubarretxena-Belandia, I.; Lemischka, I.R. Design and validation of an open-source modular Microplate Photoirradiation System for high-throughput photobiology experiments. PLoS ONE 2018, 10, e0203597. [Google Scholar] [CrossRef] [PubMed]
- Gholami, L.; Shahabi, S.; Jazaeri, M.; Hadilou, M.; Fekrazad, R. Clinical applications of antimicrobial photodynamic therapy in dentistry. Front. Microbiol. 2023, 13, 1020995. [Google Scholar] [CrossRef] [PubMed]
- Nakonieczna, J.; Wolnikowska, K.; Ogonowska, P.; Neubauer, D.; Bernat, A.; Kamysz, W. Rose bengal-mediated photoinactivation of multidrug resistant Pseudomonas aeruginosa is enhanced in the presence of antimicrobial peptides. Front. Microbiol. 2018, 9, 398683. [Google Scholar] [CrossRef] [PubMed]
- Piksa, M.; Lian, C.; Samuel, I.; Pawlik, K.; Samuel, I.; Matczyszyn, K. The role of the light source in antimicrobial photodynamic therapy. Chem. Soc. Rev. 2023, 52, 1697–1722. [Google Scholar] [CrossRef] [PubMed]
- Maisch, T.; Baier, J.; Franz, B.; Maier, M.; Landthaler, M.; Szeimies, R.M.; Bäumler, W. The role of singlet oxygen and oxygen concentration in photodynamic inactivation of bacteria. Proc. Natl. Acad. Sci. USA 2007, 104, 7223–7228. [Google Scholar] [CrossRef] [PubMed]
- Mammari, N.; Lamouroux, E.; Boudier, A.; Duval, R.E. Current knowledge on the oxidative-stress-mediated antimicrobial properties of metal-based nanoparticles. Microorganisms 2022, 10, 437. [Google Scholar] [CrossRef] [PubMed]
- Fasnacht, M.; Polacek, N. Oxidative stress in bacteria and the central dogma of molecular biology. Front. Mol. Biosci. 2021, 8, 671037. [Google Scholar] [CrossRef] [PubMed]
- Cieplik, F.; Deng, D.; Crielaard, W.; Buchalla, W.; Hellwig, E.; Al-Ahmad, A.; Maisch, T. Antimicrobial photodynamic therapy–what we know and what we don’t. Crit. Rev. Microbiol. 2018, 44, 571–589. [Google Scholar] [CrossRef]
- Sperandio, F.F.; Huang, Y.Y.; Hamblin, M.R. Antimicrobial photodynamic therapy to kill Gram-negative bacteria. Recent. Pat. Anti-Infect. Drug Discov. 2013, 8, 108–120. [Google Scholar] [CrossRef]
- Hamblin, M.R. Drug efflux pumps in photodynamic therapy in Cancer Sensitizing Agents for Chemotherapy. In Drug Efflux Pumps Cancer Resistance Pathways: From Mol. Recognition Characterization Possible Inhibition Strat. Chemotherapy; Sosnik, A., Bendayan, R., Eds.; Academic Press: Cambridge, MA, USA, 2020; Volume 7, pp. 251–276. [Google Scholar]
- Songsantiphap, C.; Vanichanan, J.; Chatsuwan, T.; Asawanonda, P.; Boontaveeyuwat, E. Methylene Blue–Mediated Antimicrobial Photodynamic Therapy Against Clinical Isolates of Extensively Drug Resistant Gram-Negative Bacteria Causing Nosocomial Infections in Thailand, An In Vitro Study. Front. Cell. Infect. Microbiol. 2022, 12, 929242. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Tonon, C.C.; Ashraf, S.; Hasan, T. Photodynamic and antibiotic therapy in combination against bacterial infections: Efficacy, determinants, mechanisms, and future perspectives. Adv. Drug Deliver. Rev. 2021, 177, 113941. [Google Scholar] [CrossRef] [PubMed]
- Meerovich, G.A.; Akhlyustina, E.V.; Tiganova, I.G.; Makarova, E.A.; Tolordava, E.R.; Zhizhimova, Y.S.; Loschenov, V.B. Photodynamic inactivation of Pseudomonas aeruginosa bacterial biofilms using photosensitizers based on octacationic derivatives of phthalocyanines and bacteriochlorins. J. Phys. Conf. Ser. 2020, 1439, 12036. [Google Scholar] [CrossRef]
- Camacho Silvas, L.A. Resistencia bacteriana, una crisis actual Bacterial resistance, a current crisis. Rev. Esp. Salud Publica 2023, 97, e202302013. [Google Scholar] [PubMed]
- Gauba, A.; Rahman, K.M. Evaluation of Antibiotic Resistance Mechanisms in Gram-Negative Bacteria. Antibiotics 2023, 12, 1590. [Google Scholar] [CrossRef] [PubMed]
- Mlynarczyk-Bonikowska, B.; Kowalewski, C.; Krolak-Ulinska, A.; Marusza, W. Molecular Mechanisms of Drug Resistance in Staphylococcus aureus. Int. J. Mol. Sci. 2022, 23, 8088. [Google Scholar] [CrossRef] [PubMed]
- Paz-Zarza, V.M.; Mangwani-Mordani, S.; Martínez-Maldonado, A.; Álvarez-Hernández, D.; Solano-Gálvez, S.G.; Vázquez-López, R. Pseudomonas aeruginosa: Patogenicidad y resistencia antimicrobiana en la infección urinaria. Rev. Chil. Infectología 2019, 36, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Kirar, S.; Thakur, N.; Laha, J.; Bhaumik, J.; Banerjee, U. Development of Gelatin Nanoparticle-Based Biodegradable Phototheranostic Agents: Advanced System to Treat Infectious Diseases. ACS Biomater. Sci. Eng. 2018, 4, 473–482. [Google Scholar] [CrossRef]
- Alexandrino, F.; Bezerra, E.; Da Costa, R.; Cavalcante, L.; Sales, F.; Francisco, T.; Rodrigues, L.; Almeida, D.; Ricardo, N.; Costa, S.; et al. Rose Bengal incorporated to α-cyclodextrin microparticles for photodynamic therapy against the cariogenic microorganism Streptococcus mutans. Photodiagnosis Photodyn. Ther. 2019, 25, 111–118. [Google Scholar] [CrossRef]
- Durkee, H.; Arboleda, A.; Aguilar, M.; Martinez, J.; Alawa, K.; Relhan, N.; Maestre-Mesa, J.; Amescua, G.; Miller, D.; Parel, J. Rose bengal photodynamic antimicrobial therapy to inhibit Pseudomonas aeruginosa keratitis isolates. Lasers Med. Sci. 2020, 53, 861–866. [Google Scholar] [CrossRef]
- Anju, V.; Paramanantham, P.; Lal, S.; Sharan, A.; Alsaedi, M.; Dawoud, T.; Asad, S.; Busi, S. Antimicrobial photodynamic activity of rose bengal conjugated multi walled carbon nanotubes against planktonic cells and biofilm of Escherichia coli. Photodiagnosis Photodyn. Ther. 2018, 24, 300–310. [Google Scholar]
- Pérez-Laguna, V.; García-Luque, I.; Ballesta, A.; Pérez-Artiaga, L.; Lampaya-Pérez, V.; Samper, S.; Soria-Lozano, P.; Rezusta, A.; Gilaberte, Y. Antimicrobial photodynamic activity of Rose Bengal, alone or in combination with Gentamicin, against planktonic and biofilm Staphylococcus aureus. Photodiagnosis Photodyn. Ther. 2018, 21, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Gualdesi, M.S.; Aiassa, V.; Vara, J.; Alvarez Igarzabal, C.I.; Ortiz, C.S. Development and evaluation of novel nanophotosensitizers as photoantimicrobial agents against Staphylococcus aureus. Mater. Sci. Eng. C. 2019, 94, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Ghorbani, J.; Rahban, D.; Aghamiri, S.; Teymouri, A.; Bahador, A. Photosensitizers in antibacterial photodynamic therapy: An overview. Laser Ther. 2018, 27, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Polat, E.; Kang, K. Natural photosensitizers in antimicrobial photodynamic therapy. Biomedicines 2021, 9, 584. [Google Scholar] [CrossRef] [PubMed]
- Sanches, C.V.G.; Sardi, J.D.C.O.; Terada, R.S.S.; Lazarini, J.G.; Freires, I.A.; Polaquini, C.R.; Torrezan, G.S.; Regasini, L.O.; Fujimaki, M.; Rosalen, P.L. Diacetylcurcumin: A new photosensitizer for antimicrobial photodynamic therapy in Streptococcus mutans biofilms. Biofouling 2019, 35, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Fabio, G.B.; Martin, B.A.; Dalmolin, L.F.; Lopez, R.F.V. Antimicrobial photodynamic therapy and the advances impacted by the association with nanoparticles. J. Drug Deliv. Sci. Technol. 2023, 80, 104147. [Google Scholar] [CrossRef]
- Liu, H.; Jiang, Y.; Wang, Z.; Zhao, L.; Yin, Q.; Liu, M. Nanomaterials as carriers to improve photodynamic antibacterial therapy. Front. Chem. 2022, 10, 1044627. [Google Scholar] [CrossRef] [PubMed]
- Thomas-Moore, B.A.; del Valle, C.A.; Field, R.A.; Marín, M.J. Recent advances in nanoparticle-based targeting tactics for antibacterial photodynamic therapy. Photochem. Photobiol. Sci. 2022, 21, 1111–1131. [Google Scholar] [CrossRef]
- Maliszewska, I.; Wanarska, E.; Thompson, A.C.; Samuel, I.D.W.; Matczyszyn, K. Biogenic Gold Nanoparticles Decrease Methylene Blue Photobleaching and Enhance Antimicrobial Photodynamic Therapy. Molecules 2021, 26, 623. [Google Scholar] [CrossRef]
- Akhtar, F.; Khan, A.; Qazi, B.; Kulanthaivel, S.; Mishra, P.; Akhtar, K.; Ali, A. A nano phototheranostic approach of toluidine blue conjugated gold silver core shells mediated photodynamic therapy to treat diabetic foot ulcer. Sci. Rep. 2021, 11, 24464. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Rogelj, S.; Zhang, P. Rose Bengal-decorated silica nanoparticles as photosensitizers for inactivation of gram-positive bacteria. Nanotechnology 2010, 21, 065102. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Carter, K.A.; Lovell, J.F. Liposomal formulations of photosensitizers. Biomaterials 2019, 218, 119341. [Google Scholar] [CrossRef]
- Nisnevitch, M.; Nakonechny, F.; Nitzan, Y. Photodynamic Antimicrobial Chemotherapy by Liposome-Encapsulated Water-Soluble Photosensitizers. Russ. J. Bioorg. Chem. 2010, 36, 363–369. [Google Scholar] [CrossRef]
- Białowąs, W.; Boudjemaa, R.; Steenkeste, K.; Nyssen, P.; Hoebeke, M.; Lulek, J.; Fontaine-Aupart, M.P.; Schneider, R. Reactive oxygen species production by photoexcited (CuInS2)x(ZnS)1−x quantum dots and their phototoxicity towards Staphylococcus aureus bacteria. J. Photochem. Photobiol. A Chem. 2024, 446, 115165. [Google Scholar] [CrossRef]
- Yin, R.; Wang, M.; Huang, Y.; Landi, G.; Vecchio, D.; Chiang, L.; Hamblin, M. Antimicrobial photodynamic inactivation with decacationic functionalized fullerenes: Oxygen independent photokilling in presence of aside and new mechanistic insights. Free Radic. Biol. Med. 2015, 79, 14–27. [Google Scholar] [CrossRef] [PubMed]
- McCollum, C.R.; Bertram, J.R.; Nagpal, P.; Chatterjee, A. Photoactivated Indium Phosphide Quantum Dots Treat Multidrug-Resistant Bacterial Abscesses In Vivo. ACS Appl. Mater. Interfaces 2021, 13, 30404–30419. [Google Scholar] [CrossRef] [PubMed]
- Martins Antunes de Melo, W.d.C.; Celiešiūtė-Germanienė, R.; Šimonis, P.; Stirkė, A. Antimicrobial photodynamic therapy (aPDT) for biofilm treatments. Possible synergy between aPDT and pulsed electric fields. Virulence 2021, 12, 2247–2272. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Huang, Y.Y.; Wang, Y.; Wang, X.; Hamblin, M.R. Antimicrobial photodynamic therapy to control clinically relevant biofilm infections. Front. Microbiol. 2018, 9, 377371. [Google Scholar] [CrossRef]
- Decraene, V.; Pratten, J.; Wilson, M. Assessment of the Activity of a Novel Light-Activated Antimicrobial. Infect. Control Hosp. Epidemiol. 2014, 29, 1181–1184. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Units | Low (−1) | High (+1) |
|---|---|---|---|
| RB concentration | µg/mL | 1.75 | 3.00 |
| Exposure time | min | 15 | 30 |
| Green light irradiance | mW/cm2 | 17.8 | 38.3 |
| Response: Microbial inhibition rate (%) | |||
| Light Parameter | Description and Values |
|---|---|
| Wavelength (nm) | 514 ± 1 |
| Light source technology | LED |
| Irradiation area (cm2) | 2.97 ± 0.03 |
| Distance between light and sample (mm) | 10 ± 1 |
| Exposure time (s) | 900, 1329, 1800 |
| Irradiance (mW/cm2) | 17.8, 30.3, 38.3 |
| Light fluence (J/cm2) | 16.03, 32.04, 34.51, 40.86, 69.00 |
| Experiment | RB Concentration (µg/mL) | Exposure Time (min) | Green Light Irradiance (mW/cm2) | Microbial Inhibition (%) |
|---|---|---|---|---|
| A | 2.38 | 22.5 | 30.3 | 100 |
| B | 1.75 | 30 | 38.3 | 100 |
| C | 3 | 30 | 17.8 | 100 |
| D | 1.75 | 15 | 17.8 | 100 |
| E | 3 | 30 | 38.3 | 100 |
| F | 1.75 | 15 | 38.3 | 100 |
| G | 1.75 | 30 | 17.8 | 100 |
| H | 3 | 15 | 38.3 | 100 |
| I | 3 | 15 | 17.8 | 100 |
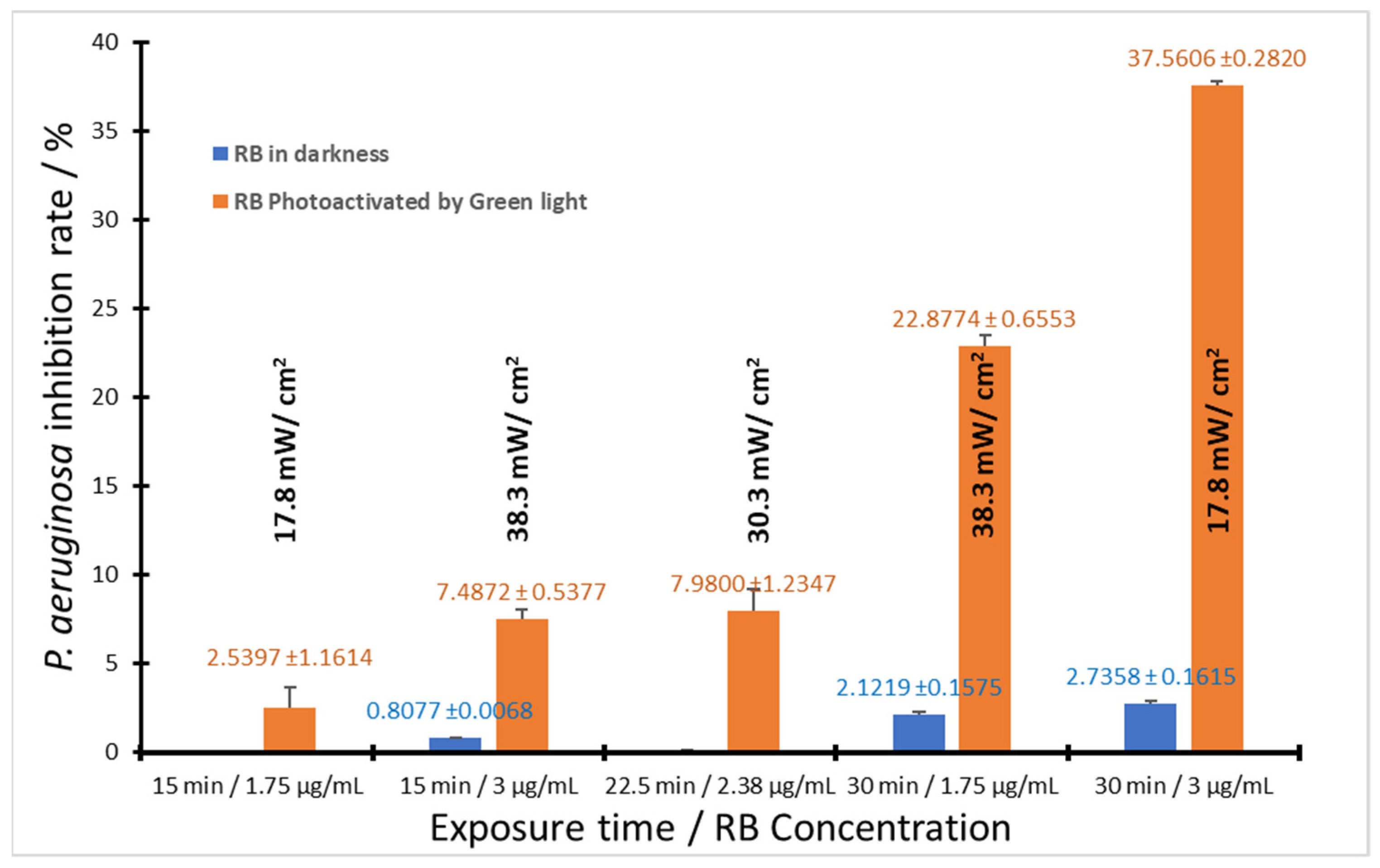
| Experiment | RB Concentration (µg/mL) | Exposure Time (min) | Green Light Irradiance (mW/cm2) | Microbial Inhibition (%) |
|---|---|---|---|---|
| A | 1.75 | 15 | 17.8 | 2.54 ± 1.16 |
| B | 1.75 | 30 | 17.8 | 7.49 ± 0.54 |
| C | 3 | 30 | 17.8 | 37.56 ± 0.28 |
| D | 3 | 15 | 38.3 | 22.88 ± 0.66 |
| E | 1.75 | 15 | 38.3 | 0.71 ± 0.41 |
| F | 3 | 30 | 38.3 | 14.17 ± 2.32 |
| G | 1.75 | 30 | 38.3 | 5.43 ± 1.02 |
| H | 3 | 15 | 17.8 | 6.94 ± 0.45 |
| I | 2.375 | 22.5 | 30.3 | 7.98 ± 1.24 |
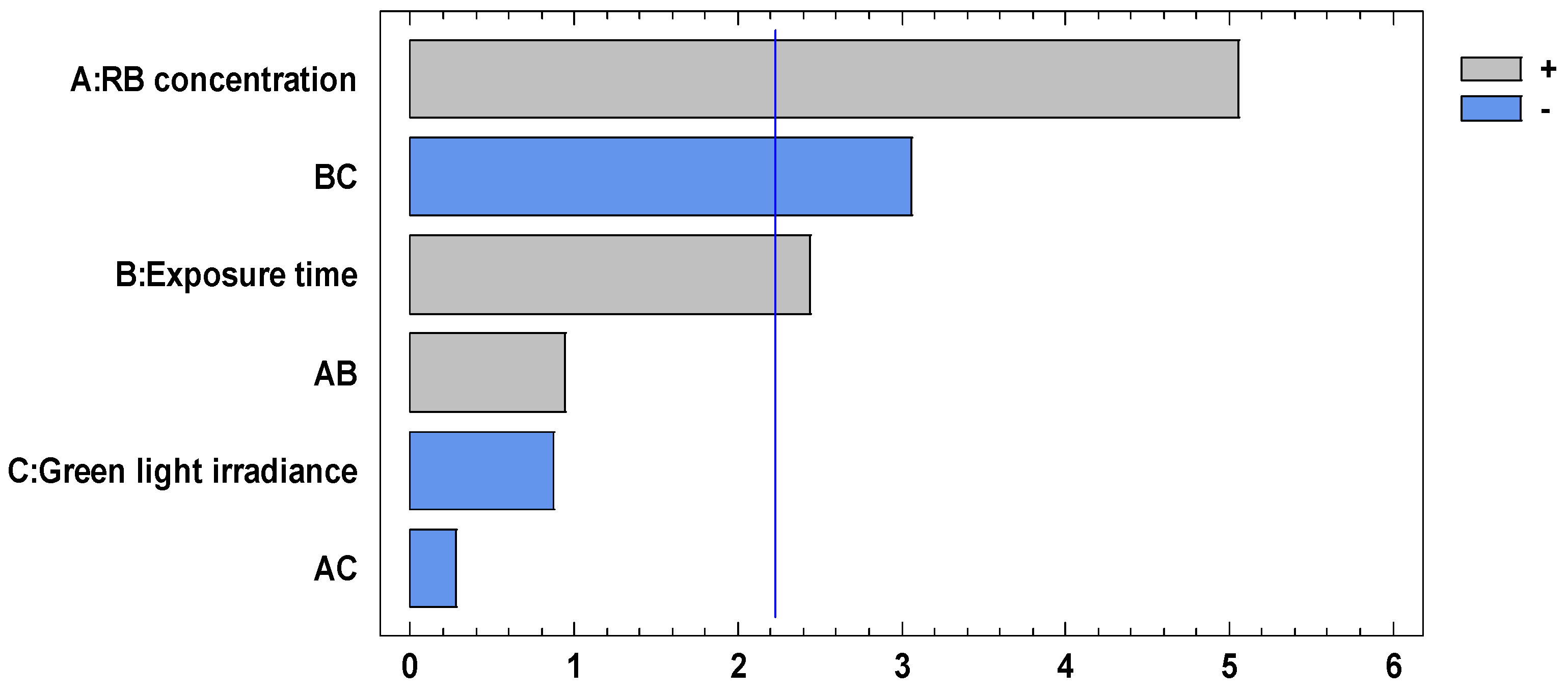
| Source | Sum of Squares | dF | Mean Squares | F-Reason | p-Value |
|---|---|---|---|---|---|
| A: RB concentration | 1069.13 | 1 | 1069.13 | 25.54 | 0.0005 |
| B: Exposure time | 249.403 | 1 | 249.403 | 5.96 | 0.0348 |
| C: Green Light irradiance | 32.1773 | 1 | 32.1773 | 0.77 | 0.4012 |
| AB | 37.3627 | 1 | 37.3627 | 0.89 | 0.3671 |
| AC | 3.17731 | 1 | 3.17731 | 0.08 | 0.7886 |
| BC | 391.15 | 1 | 391.15 | 9.34 | 0.0121 |
| Groups | 5.87102 | 1 | 5.87102 | 0.14 | 0.7159 |
| Error total | 418.664 | 10 | 41.8664 | ||
| Total (corr.) | 2206.93 | 17 |
| Bacteria | Energy Fluence (J/cm2) | Exposure Time | RB Concentration | Microbial Inhibition | Irradiation Module | System | Reference |
|---|---|---|---|---|---|---|---|
| Escherichia coli Serratia marcescens Pseudomonas putida Bacillus subtilis | NE | 5 ± 0.1 h 3 ± 0.3 h 4 ± 0.8 h 1.5 ± 0.1 h | 0.089 mM | IC50 = 22 ± 2 µg/mL IC50 = 22 ± 1.7 µg/mL IC50 = 29 ± 2 µg/mL IC50 = 2.6 ± 1.2 µg/mL | ------- | Gelatin nanoparticles | [63] |
| Streptococcus mutans | 3.35 6.70 10.05 | 60 s 120 s 180 s | 62 mM | Log 7 reduction | ------- | α-cyclodextrin microparticles | [64] |
| Pseudomonas aeruginosa | 5.4 | 15 min | 1 mM | 89–99% increase in inhibition compared with non-irradiated agar plates | Agar plates in a custom-made plate. | RB solution | [65] |
| Escherichia coli | 1674.7 | 10 min | 50 mg/mL | Reduction in the biofilm formation: 64.94 ± 2.91% | ------- | Carbon nanotubes | [66] |
| Staphylococcus aureus | 18 | NE * | 0.62 mg/mL | Log 6 reduction | ------- | RB solution | [67] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roa-Tort, K.; Saavedra, Y.; Villanueva-Martínez, A.; Ganem-Rondero, A.; Pérez-Carranza, L.A.; de la Rosa-Vázquez, J.M.; Ugalde-Femat, G.; Molina-Alejandre, O.; Becerril-Osnaya, A.A.; Rivera-Fernández, J.D. In Vitro Antimicrobial Photodynamic Therapy for Pseudomonas aeruginosa (P. aeruginosa) and methicillin-resistant Staphylococcus aureus (MRSA) Inhibition Using a Green Light Source. Pharmaceutics 2024, 16, 518. https://doi.org/10.3390/pharmaceutics16040518
Roa-Tort K, Saavedra Y, Villanueva-Martínez A, Ganem-Rondero A, Pérez-Carranza LA, de la Rosa-Vázquez JM, Ugalde-Femat G, Molina-Alejandre O, Becerril-Osnaya AA, Rivera-Fernández JD. In Vitro Antimicrobial Photodynamic Therapy for Pseudomonas aeruginosa (P. aeruginosa) and methicillin-resistant Staphylococcus aureus (MRSA) Inhibition Using a Green Light Source. Pharmaceutics. 2024; 16(4):518. https://doi.org/10.3390/pharmaceutics16040518
Chicago/Turabian StyleRoa-Tort, Karen, Yael Saavedra, Angélica Villanueva-Martínez, Adriana Ganem-Rondero, Laura Abril Pérez-Carranza, José M. de la Rosa-Vázquez, Gabriel Ugalde-Femat, Omar Molina-Alejandre, Andrea Angela Becerril-Osnaya, and Josué D. Rivera-Fernández. 2024. "In Vitro Antimicrobial Photodynamic Therapy for Pseudomonas aeruginosa (P. aeruginosa) and methicillin-resistant Staphylococcus aureus (MRSA) Inhibition Using a Green Light Source" Pharmaceutics 16, no. 4: 518. https://doi.org/10.3390/pharmaceutics16040518
APA StyleRoa-Tort, K., Saavedra, Y., Villanueva-Martínez, A., Ganem-Rondero, A., Pérez-Carranza, L. A., de la Rosa-Vázquez, J. M., Ugalde-Femat, G., Molina-Alejandre, O., Becerril-Osnaya, A. A., & Rivera-Fernández, J. D. (2024). In Vitro Antimicrobial Photodynamic Therapy for Pseudomonas aeruginosa (P. aeruginosa) and methicillin-resistant Staphylococcus aureus (MRSA) Inhibition Using a Green Light Source. Pharmaceutics, 16(4), 518. https://doi.org/10.3390/pharmaceutics16040518