Augmented Renal Clearance in Critical Illness: An Important Consideration in Drug Dosing


Abstract
:1. Introduction
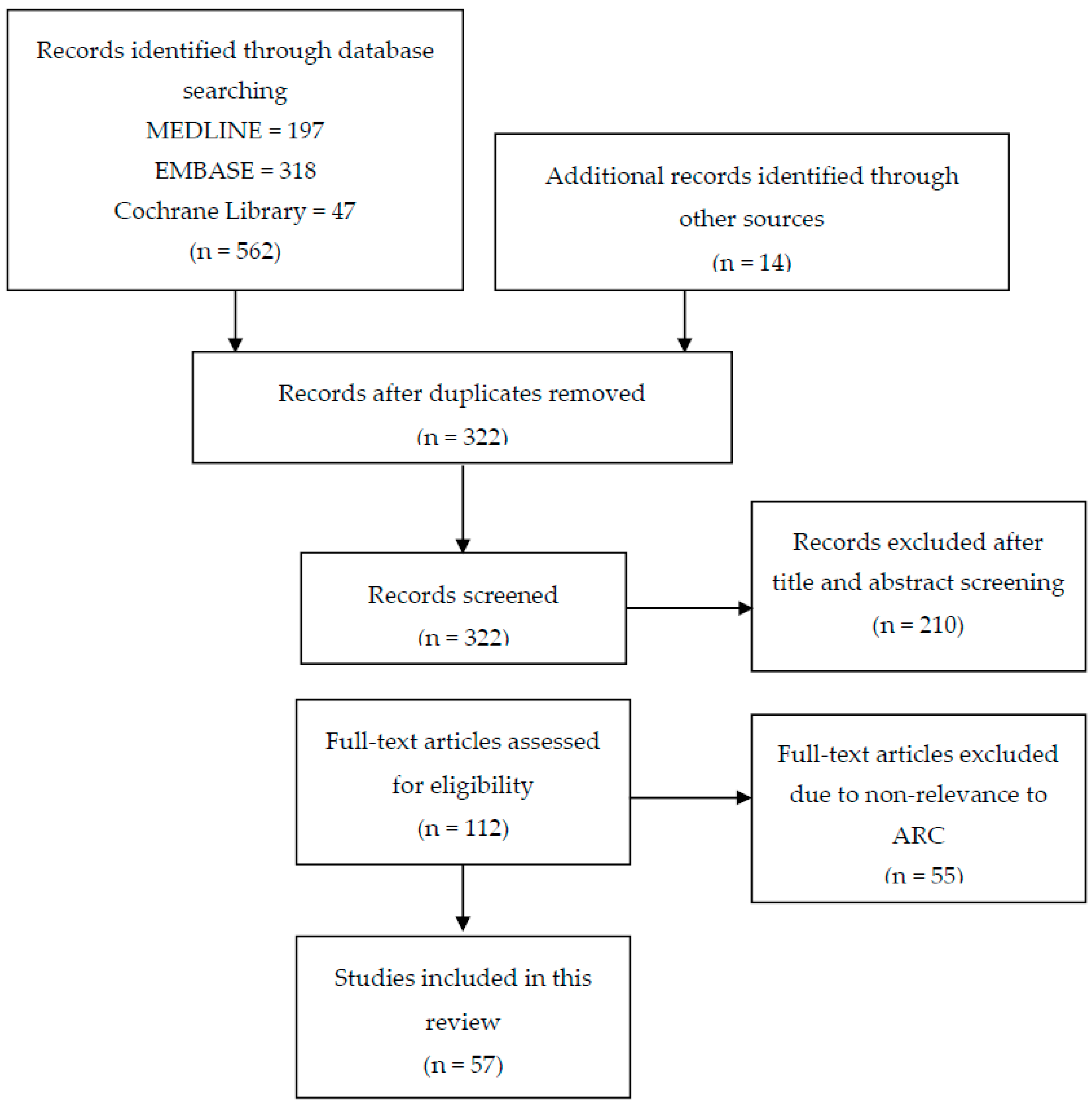
2. Methods
3. Results and Discussion
3.1. ARC Definition and Prevalence
3.2. Pathophysiology
3.3. ARC Risk Factors
3.4. Creatinine Clearance: Estimation Methods and ARC
3.5. Drug Therapy in ARC Population
3.5.1. Pharmacokinetic Changes in ARC
3.5.2. Vancomycin
3.5.3. Beta-Lactam Antimicrobials
Carbapenems
Piperacillin/Tazobactam
Other Beta-Lactam Antimicrobials
3.5.4. Other Medications
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Udy, A.A.; Putt, M.T.; Boots, R.J.; Lipman, J. ARC—Augmented renal clearance. Curr. Pharm. Biotechnol. 2011, 12, 2020–2029. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.A.; Roberts, J.A.; Boots, R.J.; Paterson, D.L.; Lipman, J. Augmented renal clearance: Implications for antibacterial dosing in the critically ill. Clin. Pharmacokinet. 2010, 49, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.A.; Putt, M.T.; Shanmugathasan, S.; Roberts, J.A.; Lipman, J. Augmented renal clearance in the intensive care unit: An illustrative case series. Int. J. Antimicrob. Agents 2010, 35, 606–608. [Google Scholar] [CrossRef] [PubMed]
- Barletta, J.F.; Mangram, A.J.; Byrne, M.; Sucher, J.F.; Hollingworth, A.K.; AliOsman, F.R.; Shirah, G.R.; Haley, M.; Dzandu, J.K. Identifying augmented renal clearance in trauma patients: Validation of the augmented renal clearance in trauma intensive care (arctic) scoring system. J. Trauma Acute Care Surg. 2017, 82, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Abdel El Naeem, H.E.M.; Abdelhamid, M.H.E.; Atteya, D.A.M. Impact of augmented renal clearance on enoxaparin therapy in critically ill patients. Egypt. J. Anaesth. 2017, 33, 113–117. [Google Scholar] [CrossRef]
- Udy, A.A.; Dulhunty, J.M.; Roberts, J.A.; Davis, J.S.; Webb, S.A.R.; Bellomo, R.; Gomersall, C.; Shirwadkar, C.; Eastwood, G.M.; Myburgh, J.; et al. Association between augmented renal clearance and clinical outcomes in patients receiving β-lactam antibiotic therapy by continuous or intermittent infusion: A nested cohort study of the BLING-II randomised, placebo-controlled, clinical trial. Int. J. Antimicrob. Agents 2017, 49, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.A.; Jarrett, P.; LassigSmith, M.; Stuart, J.; Starr, T.; Dunlop, R.; Deans, R.; Roberts, J.A.; Senthuran, S.; Boots, R.; et al. Augmented renal clearance in traumatic brain injury: A single-center observational study of atrial natriuretic peptide, cardiac output, and creatinine clearance. J. Neurotrauma 2017, 34, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Barletta, J.F.; Mangram, A.J.; Byrne, M.; Hollingworth, A.K.; Sucher, J.F.; AliOsman, F.R.; Shirah, G.R.; Dzandu, J.K. The importance of empiric antibiotic dosing in critically ill trauma patients: Are we under-dosing based on augmented renal clearance and inaccurate renal clearance estimates? J. Trauma Acute Care Surg. 2016, 81, 1115–1120. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.; Luo, Y.; Qu, L.; Zhao, C.; Jiang, M. Application of vancomycin in patients with varying renal function, especially those with augmented renal clearance. Pharm. Biol. 2016, 54, 2802–2806. [Google Scholar] [CrossRef] [PubMed]
- Declercq, P.; Nijs, S.; D’Hoore, A.; Van Wijngaerden, E.; Wolthuis, A.; De Buck Van Overstraeten, A.; Wauters, J.; Spriet, I. Augmented renal clearance in non-critically ill abdominal and trauma surgery patients is an underestimated phenomenon: A point prevalence study. J. Trauma Acute Care Surg. 2016, 81, 468–477. [Google Scholar] [CrossRef] [PubMed]
- Hirai, K.; Ihara, S.; Kinae, A.; Ikegaya, K.; Suzuki, M.; Hirano, K.; Itoh, K. Augmented renal clearance in pediatric patients with febrile neutropenia associated with vancomycin clearance. Ther. Drug Monit. 2016, 38, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Kawano, Y.; Morimoto, S.; Izutani, Y.; Muranishi, K.; Kaneyama, H.; Hoshino, K.; Nishida, T.; Ishikura, H. Augmented renal clearance in Japanese intensive care unit patients: A prospective study. J. Intensive Care 2016, 4, 62. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Cotta, M.O.; Cojutti, P.; Lugano, M.; Rocca, G.D.; Pea, F. Does critical illness change levofloxacin pharmacokinetics? Antimicrob. Agents Chemother. 2016, 60, 1459–1463. [Google Scholar] [CrossRef] [PubMed]
- De Cock, P.A.J.G.; Standing, J.F.; Barker, C.I.S.; de Jaeger, A.; Dhont, E.; Carlier, M.; Verstraete, A.G.; Delanghe, J.R.; Robays, H.; De Paepe, P. Augmented renal clearance implies a need for increased amoxicillin-clavulanic acid dosing in critically ill children. Antimicrob. Agents Chemother. 2015, 59, 7027–7035. [Google Scholar] [CrossRef] [PubMed]
- De Waele, J.J.; Dumoulin, A.; Janssen, A.; Hoste, E.A. Epidemiology of augmented renal clearance in mixed icu patients. Minerva Anestesiol. 2015, 81, 1079–1085. [Google Scholar] [PubMed]
- Dias, C.; Gaio, A.R.; Monteiro, E.; Barbosa, S.; Cerejo, A.; Donnelly, J.; Felgueiras, O.; Smielewski, P.; Paiva, J.A.; Czosnyka, M. Kidney-brain link in traumatic brain injury patients? A preliminary report. Neurocrit. Care 2015, 22, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Huttner, A.; Von Dach, E.; Renzoni, A.; Huttner, B.D.; Affaticati, M.; Pagani, L.; Daali, Y.; Pugin, J.; Karmime, A.; Fathi, M.; et al. Augmented renal clearance, low beta-lactam concentrations and clinical outcomes in the critically ill: An observational prospective cohort study. Int. J. Antimicrob. Agents 2015, 45, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Morbitzer, K.A.; Jordan, J.D.; Rhoney, D.H. Vancomycin pharmacokinetic parameters in patients with acute brain injury undergoing controlled normothermia, therapeutic hypothermia, or pentobarbital infusion. Neurocrit Care 2015, 22, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, S.; Minville, V.; Asehnoune, K.; Virtos, M.; Georges, B.; Fourcade, O.; Conil, J.M. Screening of patients with augmented renal clearance in ICU: Taking into account the ckd-epi equation, the age, and the cause of admission. Ann. Intensiv. Care 2015, 5, 49. [Google Scholar] [CrossRef] [PubMed]
- Spadaro, S.; Berselli, A.; Fogagnolo, A.; Capuzzo, M.; Ragazzi, R.; Marangoni, E.; Bertacchini, S.; Volta, C.A. Evaluation of a protocol for vancomycin administration in critically patients with and without kidney dysfunction. BMC Anesthesiol. 2015, 15, 95. [Google Scholar] [CrossRef] [PubMed]
- Steinke, T.; Moritz, S.; Beck, S.; Gnewuch, C.; Kees, M.G. Estimation of creatinine clearance using plasma creatinine or cystatin C: A secondary analysis of two pharmacokinetic studies in surgical ICU patients. BMC Anesthesiol. 2015, 15, 62. [Google Scholar] [CrossRef] [PubMed]
- Adnan, S.; Ratnam, S.; Kumar, S.; Paterson, D.; Lipman, J.; Roberts, J.; Udy, A.A. Select critically ill patients at risk of augmented renal clearance: Experience in a malaysian intensive care unit. Anaesth. Intensiv. Care 2014, 42, 715–722. [Google Scholar]
- Akers, K.S.; Niece, K.L.; Chung, K.K.; Cannon, J.W.; Cota, J.M.; Murray, C.K. Modified augmented renal clearance score predicts rapid piperacillin and tazobactam clearance in critically ill surgery and trauma patients. J. Trauma Acute Care Surg. 2014, 77, 163. [Google Scholar] [CrossRef] [PubMed]
- Baptista, J.P.; Neves, M.; Rodrigues, L.; Teixeira, L.; Pinho, J.; Pimentel, J. Accuracy of the estimation of glomerular filtration rate within a population of critically ill patients. J. Nephrol. 2014, 27, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Baptista, J.P.; Roberts, J.A.; Sousa, E.; Freitas, R.; Deveza, N.; Pimentel, J. Decreasing the time to achieve therapeutic vancomycin concentrations in critically ill patients: Developing and testing of a dosing nomogram. Crit. Care (Lond. Engl.) 2014, 18, 654. [Google Scholar] [CrossRef] [PubMed]
- Campassi, M.L.; Gonzalez, M.C.; Masevicius, F.D.; Vazquez, A.R.; Moseinco, M.; Navarro, N.C.; Previgliano, L.; Rubatto, N.P.; Benites, M.H.; Estenssoro, E.; et al. Augmented renal clearance in critically ill patients: Incidence, associated factors and effects on vancomycin treatment]. Rev. Bras. Ter. Intensiv. 2014, 26, 13–20. [Google Scholar] [CrossRef]
- Hites, M.; Taccone, F.S.; Wolff, F.; Maillart, E.; Beumier, M.; Surin, R.; Cotton, F.; Jacobs, F. Broad-spectrum beta-lactams in obese non-critically ill patients. Nutr. Diabetes 2014, 4, e119. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.A.; Jarrett, P.; Stuart, J.; LassigSmith, M.; Starr, T.; Dunlop, R.; Wallis, S.C.; Roberts, J.A.; Lipman, J. Determining the mechanisms underlying augmented renal drug clearance in the critically ill: Use of exogenous marker compounds. Crit. Care 2014, 18, 657. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.A.; Baptista, J.P.; Lim, N.L.; Joynt, G.M.; Jarrett, P.; Wockner, L.; Boots, R.J.; Lipman, J. Augmented renal clearance in the ICU: Results of a multicenter observational study of renal function in critically ill patients with normal plasma creatinine concentrations. Crit. Care Med. 2014, 42, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Carlier, M.; Carrette, S.; Roberts, J.A.; Stove, V.; Verstraete, A.; Hoste, E.; Depuydt, P.; Decruyenaere, J.; Lipman, J.; Wallis, S.C.; et al. Meropenem and piperacillin/tazobactam prescribing in critically ill patients: Does augmented renal clearance affect pharmacokinetic/pharmacodynamic target attainment when extended infusions are used? Crit. Care (Lond. Engl.) 2013, 17, R84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claus, B.O.M.; Hoste, E.A.; Colpaert, K.; Robays, H.; Decruyenaere, J.; De Waele, J.J. Augmented renal clearance is a common finding with worse clinical outcome in critically ill patients receiving antimicrobial therapy. J. Crit. Care 2013, 28, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Minkute, R.; Briedis, V.; Steponaviciute, R.; Vitkauskiene, A.; Maciulaitis, R. Augmented renal clearance—An evolving risk factor to consider during the treatment with vancomycin. J. Clin. Pharm. Ther. 2013, 38, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Lipman, J. Optimal doripenem dosing simulations in critically ill nosocomial pneumonia patients with obesity, augmented renal clearance, and decreased bacterial susceptibility. Crit. Care Med. 2013, 41, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Shimamoto, Y.; Fukuda, T.; Tanaka, K.; Komori, K.; Sadamitsu, D. Systemic inflammatory response syndrome criteria and vancomycin dose requirement in patients with sepsis. Intensive Care Med. 2013, 39, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.A.; Roberts, J.A.; Shorr, A.F.; Boots, R.J.; Lipman, J. Augmented renal clearance in septic and traumatized patients with normal plasma creatinine concentrations: Identifying at-risk patients. Crit. Care (Lond. Engl.) 2013, 17, R35. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.A.; Morton, F.J.A.; NguyenPham, S.; Jarrett, P.; LassigSmith, M.; Stuart, J.; Dunlop, R.; Starr, T.; Boots, R.J.; Lipman, J. A comparison of CKD-EPI estimated glomerular filtration rate and measured creatinine clearance in recently admitted critically ill patients with normal plasma creatinine concentrations. BMC Nephrol. 2013, 14, 250. [Google Scholar] [CrossRef] [PubMed]
- Baptista, J.P.; Sousa, E.; Martins, P.J.; Pimentel, J.M. Augmented renal clearance in septic patients and implications for vancomycin optimisation. Int. J. Antimicrob. Agents 2012, 39, 420–423. [Google Scholar] [CrossRef] [PubMed]
- Grootaert, V.; Willems, L.; Debaveye, Y.; Meyfroidt, G.; Spriet, I. Augmented renal clearance in the critically ill: How to assess kidney function. Ann. Pharmacother. 2012, 46, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.A.; Varghese, J.M.; Altukroni, M.; Briscoe, S.; McWhinney, B.C.; Ungerer, J.P.; Lipman, J.; Roberts, J.A. Subtherapeutic initial β-lactam concentrations in select critically ill patients: Association between augmented renal clearance and low trough drug concentrations. Chest 2012, 142, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Baptista, J.P.; Udy, A.A.; Sousa, E.; Pimentel, J.; Wang, L.; Roberts, J.A.; Lipman, J. A comparison of estimates of glomerular filtration in critically ill patients with augmented renal clearance. Crit. Care (Lond. Engl.) 2011, 15, R139. [Google Scholar] [CrossRef] [PubMed]
- Minville, V.; Asehnoune, K.; Ruiz, S.; Breden, A.; Georges, B.; Seguin, T.; Tack, I.; Jaafar, A.; Saivin, S.; Fourcade, O.; et al. Increased creatinine clearance in polytrauma patients with normal serum creatinine: A retrospective observational study. Crit. Care (Lond. Engl.) 2011, 15, R49. [Google Scholar] [CrossRef] [PubMed]
- Spencer, D.D.; Jacobi, J.; Juenke, J.M.; Fleck, J.D.; Kays, M.B. Steady-state pharmacokinetics of intravenous levetiracetam in neurocritical care patients. Pharmacotherapy 2011, 31, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Goboova, M.; Kuzelova, M.; Kissova, V.; Bodakova, D.; Martisova, E. An adjustment of vancomycin dosing regimen for a young patient with augmented renal clearance: A case report. Acta Fac. Pharm. Univ. Comen. 2015, 62, 1–4. [Google Scholar]
- Abdul-Aziz, M.; McDonald, C.; McWhinney, B.; Ungerer, J.P.J.; Lipman, J.; Roberts, J.A. Low flucloxacillin concentrations in a patient with central nervous system infection: The need for plasma and cerebrospinal fluid drug monitoring in the ICU. Ann. Pharmacother. 2014, 48, 1380–1384. [Google Scholar] [CrossRef] [PubMed]
- Cook, A.M.; Arora, S.; Davis, J.; Pittman, T. Augmented renal clearance of vancomycin and levetiracetam in a traumatic brain injury patient. Neurocrit. Care 2013, 19, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Lonsdale, D.O.; Udy, A.A.; Roberts, J.A.; Lipman, J. Antibacterial therapeutic drug monitoring in cerebrospinal fluid: Difficulty in achieving adequate drug concentrations. J. Neurosurg. 2013, 118, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Troger, U.; Drust, A.; Martens-Lobenhoffer, J.; Tanev, I.; Braun-Dullaeus, R.; Bode-Boger, S. Decreased meropenem levels in intensive care unit patients with augmented renal clearance: Benefit of therapeutic drug monitoring. Int. J. Antimicrob. Agents 2012, 40, 370–372. [Google Scholar] [CrossRef] [PubMed]
- Caro, L.; Larson, K.; Nicolau, D.; DeWaele, J.; Kuti, J.; Gadzicki, E.; Yu, B.; Rhee, E. PK/PD and safety of 3 g ceftolozane/tazobactam in critically ill augmented renal clearance patients. In Proceedings of the 46th Critical Care Medicine Conference, Honolulu, HI, USA, 21–25 January 2017; p. 661. [Google Scholar]
- Goboova, M.; Kuzelova, M.; Fazekas, T.; Kissova, V.; Kakosova, V.; Salkovska, L. The impact of therapeutic drug monitoring (TDM) in optimizing dosage regimens of gentamicin in patients with augmented renal clearance. Int. J. Clin. Pharm. 2016, 38, 596. [Google Scholar]
- Morbitzer, K.; Jordan, D.; Sullivan, K.; Durr, E.; OlmShipman, C.; Rhoney, D. Enhanced renal clearance and impact on vancomycin trough concentration in patients with hemorrhagic stroke. In Proceedings of the Annual Meeting of the American College of Clinical Pharmacy (ACCP), Hollywood, FL, USA, 23–26 October 2016; Volume 36, p. e218. [Google Scholar]
- Morimoto, S.; Ishikura, H. An observational prospective study on the onset of augmented renal clearance: The first report. Crit. Care 2016, 20 (Suppl. 2), 182. [Google Scholar] [CrossRef]
- Dunning, J.; Roberts, J. Assessment of renal function in dosing antibiotics in septic patients: A survey of current practice within critical care units in england. Anaesthesia 2015, 70, 21. [Google Scholar]
- Baptista, J.P.; Silva, N.; Costa, E.; Fontes, F.; Marques, M.; Ribeiro, G.; Pimentel, J. Identification of the critically ill patient with augmented renal clearance: Make do with what you have! In Proceedings of the 27th Annual Congress of the European Society of Intensive Care Medicine (ESICM), Barcelona, Spain, 27 September–1 October 2014; Volume 40, p. S110. [Google Scholar]
- May, C.; Arora, S.; Parli, S.; Bastin, M.T.; Cook, A. Levetiracetam pharmacokinetics in subarachnoid hemorrhage patients with augmented renal clearance: A monte carlo simulation. In Proceedings of the 2014 Annual Meeting of the American College of Clinical Pharmacy (ACCP), Austin, TX, USA, 12–15 October 2014; Volume 34, pp. e261–e262. [Google Scholar]
- Vermis, K.; Steel, E.; Vandenbroucke, J. Prevalence of augmented renal clearance in haematological patients and the impact on vancomycin dosing. In Proceedings of the Journal of Oncology Pharmacy Practice. Conference: 14th Symposium of the International Society of Oncology Pharmacy Practitioners, Montreal, QC, Canada, 2–5 April 2014; Volume 20, p. 7. [Google Scholar]
- Weigel, J.; Egal, M.; Lima, A.; Koch, B.; Hunfeld, N.G.; Van Gelder, T.; Mouton, J.W.; Groeneveld, A.B.J. Vancomycin is underdosed in patients with high estimated glomerular filtration rate. In Proceedings of the 27th Annual Congress of the European Society of Intensive Care Medicine (ESICM), Barcelona, Spain, 27 September–1 October 2014; p. S252. [Google Scholar]
- Neves, M.; Baptista, J.P.; Rodrigues, L.; Pinho, J.; Teixeira, L.; Pimentel, J. Correlation between estimated glomerular filtration rate and measured renal creatinine clearance in critically ill patients with normal serum creatinine. Nephrol. Dial. Transplant. 2013, 28, 345. [Google Scholar]
- Grootaert, V.; Spriet, I.; Decoutere, L.; Debaveye, Y.; Meyfroidt, G.; Willems, L. Augmented renal clearance in the critically ill: Fiction or fact? Int. J. Clin. Pharm. 2012, 34, 143. [Google Scholar]
- Drust, A.; Troger, U.; MartensLobenhoffer, J.; Tanev, I.; BraunDullaeus, R.C.; BodeBoger, S.M. Therapeutic drug monitoring of meropenem is mandatory for critically ill patients with glomerular hyperfiltration. Br. J. Clin. Pharmacol. 2011, 72, 18. [Google Scholar]
- Ichai, C.; Passeron, C.; Carles, M.; Bouregba, M.; Grimaud, D. Prolonged low-dose dopamine infusion induces a transient improvement in renal function in hemodynamically stable, critically ill patients: A single-blind, prospective, controlled study. Crit. Care Med. 2000, 28, 1329–1335. [Google Scholar] [CrossRef] [PubMed]
- Ichai, C.; Soubielle, J.; Carles, M.; Giunti, C.; Grimaud, D. Comparison of the renal effects of low to high doses of dopamine and dobutamine in critically ill patients: A single-blind randomized study. Crit. Care Med. 2000, 28, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, B.; NilssonEhle, I. Advancing age and acute infection influence the kinetics of ceftazidime. Scand. J. Infect. Dis. 1989, 21, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Sime, F.B.; Udy, A.A.; Roberts, J.A. Augmented renal clearance in critically ill patients: Etiology, definition and implications for beta-lactam dose optimization. Curr. Opin. Pharmacol. 2015, 24, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Carlier, M.; Dumoulin, A.; Janssen, A.; Picavet, S.; Vanthuyne, S.; Van Eynde, R.; Vanholder, R.; Delanghe, J.; De Schoenmakere, G.; De Waele, J.J.; et al. Comparison of different equations to assess glomerular filtration in critically ill patients. Intensive Care Med. 2015, 41, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Sunder, S.; Jayaraman, R.; Mahapatra, H.S.; Sathi, S.; Ramanan, V.; Kanchi, P.; Gupta, A.; Daksh, S.K.; Ram, P. Estimation of renal function in the intensive care unit: The covert concepts brought to light. J. Intensive Care 2014, 2, 31. [Google Scholar] [CrossRef] [PubMed]
- Rybak, M.J. The pharmacokinetic and pharmacodynamic properties of vancomycin. Clin. Infect. Dis. 2006, 42 (Suppl. 1), S35–S39. [Google Scholar] [CrossRef] [PubMed]
- Mouton, J.W.; Touzw, D.J.; Horrevorts, A.M.; Vinks, A.A. Comparative pharmacokinetics of the carbapenems: Clinical implications. Clin. Pharmacokinet. 2000, 39, 185–201. [Google Scholar] [CrossRef] [PubMed]
- Binder, L.; Schworer, H.; Hoppe, S.; Streit, F.; Neumann, S.; Beckmann, A.; Wachter, R.; Oellerich, M.; Walson, P.D. Pharmacokinetics of meropenem in critically ill patients with severe infections. Ther. Drug Monit. 2013, 35, 63–70. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Year | Study Type | Age (Years) Median (IQR) | Population | N | Sex (% Male) | Measured CrCl (mL/min)—Otherwise Specified | Intervention | Main Results |
|---|---|---|---|---|---|---|---|---|
| Barletta et al. [4], 2017 | Retrospective observational | 48 ± 19 | ICU trauma patients where measured SCr available and SCr < 115 µmol/L | 133 | 76 | 168 ± 65 | ARCTIC (Augmented Renal Clearance in Trauma Intensive Care) Scoring system suggested |
|
| Naeem et al. [5], 2017 | Prospective observational | ARC: 37 ± 16 Non-ARC: 34 ± 14 | ICU patients with SCr < 115 µmol/L | 50 | ARC: 70 Non-ARC: 60 | ARC: 214 ± 46 Non-ARC: 112 ± 11 | The effects of ARC on enoxaparin determined; Patients received enoxaparin 40 mg SC daily; Anti-Xa activity measured and compared among patients with and without ARC; measured 24 h CrCl |
|
| Udy et al. [6], 2017 | Prospective observational (sub-study of BLING II RCT) | ARC: 52 (33–60) Non-ARC: 65 (55–73) | ICU patients with severe sepsis | 254 | ARC: 73 Non-ARC: 57 | ARC: 165 (144–198) Non-ARC: 56 (27–83) | Conducted to determine the effect of ARC on patient outcome; patients randomized to receive beta lactam antibiotics (piperacillin/tazobactam, ticarcillin/clavulanic acid or meropenem) by intermittent or continuous infusion; measured 8 h CrCl |
|
| Udy et al. [7], 2017 | Prospective observational | 37 (24–49) | ICU (TBI patients with SCr < 120 µmol/L) | 11 | 82 | Median (day 1): 201 (76–289) | Measured 8-h CrCl, cardiac output and ANP were determined and correlated |
|
| Barletta et al. [8], 2016 | Retrospective observational | 48 ± 18 | ICU (trauma) | 65 | 74 | 169 ± 70 | Measured 12-h CrCl compared with CG method, CKD-EPI, and MDRD-4 |
|
| Chu et al. [9], 2016 | Retrospective observational | Group A: 63 ± 15 Group B: 59 ± 14 Group C: 44 ± 16 | Patients treated with vancomycin | 148 | 66 | Estimated by CG Group A: 54 ± 17 Group B: 106 ± 15 Group C: 188 ± 50 | Vancomycin 1000 mg IV Q12H regimen given; vancomycin levels drawn pre 4th or 5th dose; levels compared across three groups: A (CrCl < 80), B (CrCl 80–129), C (CrCl ≥ 130; ARC) |
|
| Declercq et al. [10], 2016 | Prospective observational | Abdominal Surgery: 63 (51–71) Trauma Surgery: 62 (46–75) | Non-critically ill surgery patients | 232 | Abdo. Surgery: 74 Trauma Surgery: 58 | Abdominal Surgery: 109 (82–135) Trauma Surgery: 109 (85–142) | Aim to assess the prevalence of ARC in non-critically ill surgical patients; Measured 8-h CrCl |
|
| Hirai et al. [11], 2016 | Retrospective observational | 4.4 (range 1–15) | Pediatric ICU patients with normal renal function (Japan) | 109 | 59 | eGFR estimated by Schwartz formula 160 ( range 90–323) mL/min/1.73 m2 | Vancomycin 40–60 mg/kg per day given in 2–4 divided doses; vancomycin clearance estimated |
|
| Kawano et al. [12], 2016 | Prospective observational | 67 (53–77) | ICU (Japan) | 111 | 56 | Not reported | Measured 8-h CrCl |
|
| Roberts et al. [13], 2016 | Prospective PK study | 61 ± 17 | Patients treated with levofloxacin | 18 | 67 | Estimated using CG 70 ± 67 | Doses of levofloxacin 500 and 750 mg daily have been used; Monte-Carlo simulation conducted to determine PTA in ICU cohort compared to non ICU ones |
|
| De Cock et al. [14], 2015 | Prospective PK study | 2.6 (range 0.08–15) | Pediatric ICU | 50 | 60 | Not reported | Population PK of amoxicillin/clavulanate in pediatric ICU population; Conventional dosing of 25–35 mg/kg every 6 h was tested. |
|
| De Waele et al. [15], 2015 | Retrospective observational | 62 (50–72) | ICU | 1081 | 63 | ARC: 178 (140–243) Non-ARC: 54 (32–82) | Measured 24-h CrCl and ARC risk factors determined |
|
| Dias et al. [16], 2015 | Retrospective observational | Mean 42 (range 20–66) | ICU (TBI patients) | 18 | 89 | CG method 199 (Range 62–471) | Cerebrovascular pressure reactivity index (PRx) correlated with CrCl |
|
| Huttner et al. [17], 2015 | Prospective observational | ARC: 41 ± 12 Non-ARC: 51:10 | ICU with CrCl ≥ 60 mL/min | 100 | 75 | Estimated with CG ARC: 166 (145–200) Non-ARC: 103 (87–113) | They determined the influence of ARC on patient outcome; Standard dose antibiotic regimens given (imipenem/cilastatin 500 mg IV QID; meropenem 2 g IV TID; piperacillin/tazobactam 4.5 g IV TID; cefepime 2 g IV BID) |
|
| Morbitzer et al. [18], 2015 | Retrospective observational | CN: 44 (29–52) TH/PI: 48 (40–62) | ICU (TBI) | 27 | 63 | Estimated using CG CN: 119 (91–166) TH/PI: 129 (100–156) | Vancomycin pharmacokinetics compared in patients with CN (T = 36–37 C), TH (T=33–34 C) or pentobarbital infusion |
|
| Ruiz et al. [19], 2015 | Prospective observational | ARC: 39 ± 16 No ARC: 55 ± 19 | ICU (patients with normal SCr) | 360 | ARC: 75 No ARC: 65 | ARC: 173 ± 44 No ARC: 79 ± 30 | Measured 24-h CrCl compared with 4 formulas to estimate CrCl/GFR (CG, Robert, MDRD and CKD-EPI methods) |
|
| Spadaro et al. [20], 2015 | Retrospective observational | Group A: 63 ± 11 Group B: 71 ± 10 | ICU | 348 | Group A: 73 Group B: 69 | Group A: 106 ± 41 Group B: 37 ± 16 | Vancomycin administration protocol based on measured 24 h CrCl and vancomycin serum measurements; levels compared between two groups: A (CrCl > 50) and B (CrCl ≤ 50) Vancomycin serum trough target: 15–25 mg/L |
|
| Steinke et al. [21], 2015 | Prospective observational | 66 (57–74) | ICU | 100 | 61 | 73 (47–107) | Measured CrCl compared with estimated CrCl using serum cystatin C Hoek formula, CG, and CKD-EPI |
|
| Adnan et al. [22], 2014 | Prospective observational | 34 (24–47) | ICU patients with SCr < 120 µmol/L) | 49 | 76 | ARC: 173 (141–223) Non-ARC: 91 (64–112) | Measured 24-h CrCl compared with CG method |
|
| Akers et al. [23], 2014 | Prospective observational | 45 ± 19 | ICU | 13 | 62 | Not reported | They determined the ability of the ARC score to predict piperacillin/tazobactam clearance; Piperacillin/tazobactam doses given were (3.375 g IV Q6H or 4.5 g Q6H) |
|
| Baptista et al. [24], 2014 | Prospective observational | ARC: 49 ± 15 No ARC: 60 ± 18 | ICU patients with normal SCr | 54 | ARC: 64 No ARC: 36 | ARC Patients: 161 ± 28 Non-ARC Patients: 105 ± 16 | Measured 8-h CrCl compared with CG method, CKD-EPI, and MDRD |
|
| Baptista et al. [25], 2014 | Prospective observational (Group 1 data were retrospectively collected) | Group 1: 58 ± 16 Group 2: 60 ± 17 | ICU | G 1: 79 G 2: 25 | Group 1: 66 Group 2: 68 | Group 1: 125 ± 67 mL/min/1.73 m2 Group 2: 121 ± 54 mL/min/1.73 m2 | Continuous infusion Vancomycin dosing nomogram based on 8h measured CrCl was suggested Group 1: retrospective data Group 2: prospective assessment of the nomogram Target vancomycin level: 20–30 mg/L |
|
| Campassi et al. [26], 2014 | Prospective observational | ARC: 48 ± 15 Non-ARC: 65 ± 17 | ICU patients with SCr < 115 µmol/L | 363 | ARC: 48 Non-ARC: 47 | ARC: 155 ± 33 Non-ARC: 78 ± 25 | CrCl measured by 24 h urine collection; Vancomycin loading dose 15 mg/kg followed by continuous infusion 30 mg/kg/day was given Target trough 15–25 mg/L |
|
| Hites et al. [27], 2014 | Prospective observational | 61 (18–84) | Non-ICU obese (BMI ≥ 30 kg/m2) patients treated with antibiotics | 56 | 50 | 107 (6–389.0) | They assessed the adequacy of serum concentrations of antimicrobials when given to obese individuals; Standard doses of antibiotics given (Cefepime 2 g TID, Piperacillin/tazobactam 4 g QID, Meropenem 1 g TID); Measured 24-h CrCl determined |
|
| Udy et al. [28], 2014 | Prospective observational | Mean 37 (95% CI 29 –44) | ICU patients with SCr < 120 µmol/L and age ≤ 60 | 20 | 60 | Mean: 168 (95% CI 139–197) | Measured 24-h CrCl determined; various exogenous markers given to detect changes in nephron physiology |
|
| Udy et al. [29], 2014 | Prospective observational | Mean 54 (95% CI 53–56) | ICU patients with SCr < 120 µmol/L | 281 | 63.3 | Mean: 108 (95% CI 102–115) | Measured 8-h CrCl determined daily |
|
| Carlier et al. [30], 2013 | Prospective observational | 56 (48–67) | ICU | 61 | 85 | 125 (93–175) | Meropenem or piperacillin/tazobactam were given as extended IV infusions; antibiotics concentrations measured; measured 24 h CrCl determined; Meropenem dose: an IV loading of 1 g over 30 min then 1 g Q8H as extended infusion over 3 h; Piperacillin/tazobactam dose: an IV loading of 4.5 g over 30 min then 4.5 g Q6H extended infusion over 3 h. |
|
| Claus et al. [31], 2013 | Prospective observational | ARC: 54 (44–61) Non-ARC: 66 (57–77) | ICU patients receiving antimicrobial therapies | 128 | ARC: 73 Non-ARC: 61 | 98 (57–164) mL/min/1.73 m2 | Measured 8 h-CrCl determined; measuring the effect of ARC on antimicrobial therapy failure |
|
| Minkute et al. [32], 2013 | Retrospective observational | ARC: 46 (21–66) Non-ARC: 54 (22–86) | Patients treated with vancomycin | 36 | 80 | Estimated CG ARC: 151 (131–324) Non-ARC: 103 (90–127) | Vancomycin level comparison between ARC and non-ARC groups |
|
| Roberts and Lipman [33], 2013 | PK study (analysis of Phase III trial data) | 58 ± 15 | ICU patients with pneumonia | 31 | 93 | Estimated by CG 137 ± 71 | Population PK of doripenem in critically ill. |
|
| Shimamoto et al. [34], 2013 | Retrospective observational | Non-SIRS: 64 SIRS-2: 54 SIRS-3: 49 SIRS-4: 42 | ICU (Septic patients on vancomycin) | 105 | 66 | Using CG No-SIRS: 121 ± 51 SIRS-2: 160 ± 65 SIRS-3: 195 ± 70 SIRS-4: 191 ± 77 | Identified patients who had SIRS and categorized based on the number of SIRS criteria they had (non-SIRS, SIRS-2, 3 and 4); vancomycin CL and CrCL (CG) determined |
|
| Udy et al. [35], 2013 | Prospective observational | 42 ± 17 | ICU (trauma, septic, SCr < 110 µmol/L) | 71 | 63 | Mean: 135 ± 52 | They determined the prevalence and risk factors of ARC |
|
| Udy et al. [36], 2013 | Prospective observational | 51 ± 17 | ICU patients with SCr < 121 µmol/L | 110 | 64 | Mean: 125 ± 45 mL/min/1.73 m2 | Measured 8 h CrCl compared to estimated CrCl (CG and CKD-EPI) |
|
| Baptista et al. [37], 2012 | Prospective observational | Non-ARC: 70 (52–79) ARC: 41 (32–56) | ICU septic patients on vancomycin | 93 | Non-ARC: 71 ARC: 79 | Non-ARC: 70 (58–104) ARC: 159 (141–194) | The effect of ARC on vancomycin PK: ARC patients compared to non-ARC patients; measured 24 h CrCl Vancomycin dosing: A loading dose of 1000 mg if wt. < 70 kg or 1500 mg if wt. > 70 kg then 30 mg/kg/day continuous infusion |
|
| Grootaert et al. [38], 2012 | Retrospective observational | 59 (48–67) | ICU patients with measured CrCl > 120 mL/min (24-h method) | 390 | 63 | 148 (132–172) mL/min/1.73 m2 | Measured 24-h CrCl compared with CG method (CrCl) and 4-variable MDRD method (eGFR) |
|
| Udy et al. [39], 2012 | Prospective observational | 53 ± 21 | ICU | 48 | 71 | 134 ± 90 | Measured 8 h CrCl; beta lactam antibiotic concentrations measured |
|
| Baptista et al. [40], 2011 | Retrospective observational (post hoc analysis) | 35 (25–51) | ICU patients with ARC | 86 | 77 | 162 (145–190) mL/min/1.73 m2 | Measured 8-h (Australia) or 24 h (Portugal) CrCl compared with CG, modified CG, 4-variable MDRD and 6-variable MDRD |
|
| Minville et al. [41], 2011 | Retrospective observational | NPT: 58 ± 17 PT: 42 ± 18 | ICU | 284 | NPT: 63 PT: 75 | NPT: 85 ± 5 PT: 131 ± 5 mL/min/1.73 m2 | Measured 24-h CrCl; compared among patients with (NPT) and without polytrauma (PT) |
|
| Spencer et al. [42], 2011 | Prospective PK study | 54 ± 14 | Neuro ICU | 12 | 42 | 96 ± 32 (estimated, method not reported) | Patients received levetiracetam 500 mg iv every 12 h; levetiracetam levels measured |
|
| Goboova et al. [43], 2015 | Case Report | 16 | ICU (Polytrauma and sepsis) | 1 | 100 | Method not reported Day 29: 138 Days 41–51: 340 mL/min/1.73 m2 | Vancomycin initiated at doses of 1 g IV every 12 h then titrated up |
|
| Abdul-Aziz et al. [44], 2014 | Case Report | 36 | ICU (CNS infection) | 1 | 100 | 234 | Days 1–3: Flucloxacillin 2 g IV Q4H Days 4–16: Flucloxacillin 20 g/day via continuous infusion |
|
| Cook et al. [45], 2013 | Case Report | 22 | Neuro ICU (TBI) | 1 | 0 | Method not reported 153 | They described a case of ARC leading to subtherapeutic vancomycin and levetiracetam levels |
|
| Lonsdale et al. [46], 2013 | Case Report | 44 | Neuro ICU (SAH with ventriculitis) | 1 | 100 | 375 mL/min/1.73 m2 | They described a case of ARC leading to subtherapeutic vancomycin and meropenem levels |
|
| Troger et al. [47], 2012 | Case Reports | Pt 1: 37 Pt 2: 66 | ICU patients with sepsis | 2 | 100 | Estimated with CG Pt 1: Initially: 138 Day 5: 276 Pt 2: Initially: 185 Later: 219 | Described 2 cases of sepsis patients who required high doses of meropenem secondary to ARC Pt 1: meropenem 1 g IV Q8H then increased to meropenem 2 g IV Q4H Pt 2: meropenem 1 g Q8H then dose increased to1 g Q6H then to 2 g Q6H Meropenem trough target 4–10 mg/L |
|
| Udy et al. [3], 2010 | Case Series | Pt 1: 19 Pt 2: 41 Pt 3: 32 | ICU Pt 1 TBI Pt 2 Surgery Pt 3 Burn | 3 | 100 | Pt 1: 224 Pt 2: 206 Pt 3: 151 Measured 8 h CrCl | Three case reports of patients with ARC Pt. 1: meropenem Pt 2: vancomycin + meropenem Pt 3: amikacin + ciprofloxacin |
|
| Caro et al. [48], 2016 Abstract | Phase I PK study | Range 29–50 | ICU patients with ARC (CrCl ≥ 180 mL/min estimated by CG) | 5 | 40 | Estimated using CG 282 (207–417) | Determined the PK of ceftolozane/tazobactam in patients with ARC |
|
| Goboova et al. [49], 2016 Abstract | Retrospective observational | Mean 42 ± 14 | Patients treated with gentamicin | 204 | 78 | Method not reported ARC Patients: 166 ± 28 mL/min/1.73 m2 | Identification of the influence of ARC on gentamicin dosing |
|
| Morbitzer et al. [50], 2016 Abstract | Prospective observational | 63 (56–71) | Neuro ICU (Hemorrhagic stroke) | 17 | 27 | 131 (108–216) mL/min/1.73 m2 | Measured 8-h CrCl compared with CG method; vancomycin trough concentration determined |
|
| Morimoto and Ishikura [51], 2016 Abstract | Prospective observational | Not reported | ICU (Japan) | 33 | Not reported | Not reported | CrCl measured (method not reported) |
|
| Dunning and Roberts [52], 2015 Abstract | A survey | N/A | N/A | 123 | N/A | N/A | A survey of 123 ICU physicians about antibiotic prescribing and renal function assessment |
|
| Baptista et al. [53], 2014 Abstract | Retrospective observational | Not reported | ICU | 477 | Not reported | Not reported | CrCl measured by 8 h urine collection |
|
| May et al. [54], 2014 Abstract | Prospective observational | Not reported | Neuro ICU (SAH) | 20 | Not reported | 326 ± 135 mL/min/1.73 m2 | Measured 24-h CrCl determined; Monte-Carlo Simulation for levetiracetam doses to achieve trough levels ≥ 6 mg/L |
|
| Vermis et al. [55], 2014 Abstract | Retrospective observational | Not reported | Patients with hematological malignancies | 96 | Not reported | CrCl estimated using CG ARC pts: 147 Non-ARC pts: 79 | Aimed to determine the prevalence of ARC in a hematological population; Vancomycin continuous infusion: loading 15 mg/kg, maintenance 30 mg/kg given and titrated based on levels Vancomycin trough target: 20 mg/L |
|
| Weigel et al. [56], 2014 Abstract | Retrospective observational | 55 | ICU patients without renal replacement and receiving vancomycin infusion | 287 | 69 | ARC: MDRD eGFR > 130 Non ARC: MDRD eGFR < 130 | A vancomycin loading dose of 20 mg/kg was given then adjusted by Therapeutic drug monitoring to target 20–25 mg/L; Vancomycin levels compared in patients with various degrees of eGFR using MDRD |
|
| Neves et al. [57], 2013 Abstract | Prospective observational | 55 ± 13 | ICU | 54 | 72 | Mean: 138 | Measured 8-h CrCl compared with CG method |
|
| Grootaert et al. [58], 2012 Abstract | Retrospective observational | 66 (56–75) | ICU patients with measured CrCl available | 1317 | 63 | Not reported | Measured 24-h CrCl |
|
| Drust et al. [59], 2011 Abstract | Retrospective observational | Not reported | ICU patients with CrCl > 120 mL/min | 15 | Not reported | >120 | Meropenem plasma concentrations measured |
|
| ARC Scoring System [23,35] | ARCTIC Scoring System [4] | |
|---|---|---|
| Criteria | Age 50 or younger = 6 pts Trauma = 3 pts SOFA score ≤ 4 = 1 pt | SCr < 62 µmol/L = 3 pts Male sex = 2 pts Age <56 years = 4 pts Age: 56–75 years = 3 pts |
| Interpretation | 0–6 points→low ARC risk 7–10 points→high ARC risk | >6 points→high ARC risk <6 points→low ARC risk |
| Sensitivity | 100% | 84% |
| Specificity | 71% | 68% |
| Drug | Suggested Dosage | Suggestion Basis |
|---|---|---|
| Levetiracetam |
|
|
| Levofloxacin |
|
|
| Meropenem |
|
|
| Piperacillin/Tazobactam |
| |
| Vancomycin |
|
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmoud, S.H.; Shen, C. Augmented Renal Clearance in Critical Illness: An Important Consideration in Drug Dosing. Pharmaceutics 2017, 9, 36. https://doi.org/10.3390/pharmaceutics9030036
Mahmoud SH, Shen C. Augmented Renal Clearance in Critical Illness: An Important Consideration in Drug Dosing. Pharmaceutics. 2017; 9(3):36. https://doi.org/10.3390/pharmaceutics9030036
Chicago/Turabian StyleMahmoud, Sherif Hanafy, and Chen Shen. 2017. "Augmented Renal Clearance in Critical Illness: An Important Consideration in Drug Dosing" Pharmaceutics 9, no. 3: 36. https://doi.org/10.3390/pharmaceutics9030036
APA StyleMahmoud, S. H., & Shen, C. (2017). Augmented Renal Clearance in Critical Illness: An Important Consideration in Drug Dosing. Pharmaceutics, 9(3), 36. https://doi.org/10.3390/pharmaceutics9030036