

Exploring the Effects of Cancer as a Traumatic Event on Italian Adolescents and Young Adults: Investigating Psychological Well-Being, Identity Construction and Coping Strategies

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Participants
2.3. Ethics
2.4. Measures
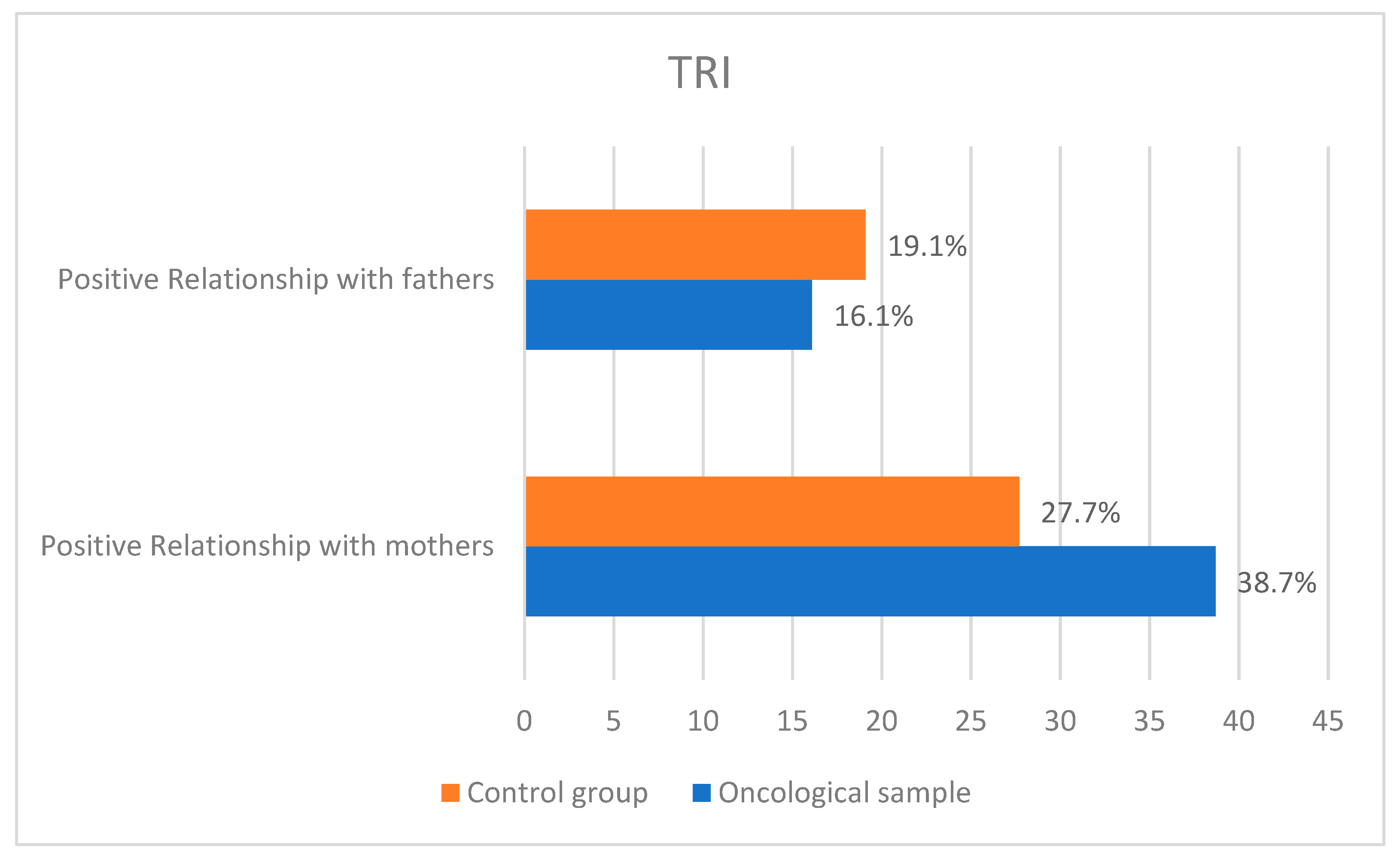
- TRI. Test of Interpersonal Relations (Bracken, 1993; Italian validation by Inaes, 1996): It was designed to assess the adequacy of children’s interpersonal relationships in the social domain, i.e., in relation to peers, in school, in relation to teachers, and in the family in relation to the relationship with parents. It consists of 35 items, each rated on a 5-point Likert scale from “strongly agree” to “strongly disagree”. In this work, we specifically used scales related to adolescents’ perceptions of the quality of their relationship with their mother and father. The questionnaire had good internal consistency (Cronbach’s alpha ranged from 0.93 to 0.96).
- KIDSCREEN-27 (Italian validation by The KIDSCREEN GROUP, 2004): Allows the assessment of well-being and health related to quality of life. It consists of 27 items and measures five Rasch-scaled dimensions: (1) Physical well-being, (2) Psychological well-being, (3) Autonomy and relationship with parents, (4) Peers and social support, (5) School environment. Each item is scored on a 5-point Likert scale ranging from 1 for “not at all” to 5 for “very much”. Higher scores indicate better quality of life and social support. Construct validity was assessed by calculating Cohen’s effect size (ES = 0.54). The questionnaire had good internal consistency (Cronbach’s alpha > 0.70).
- Centrality of Events Scale (CES; Berntsen and Rubin, 2006; Italian validation by Ionio, Mascheroni, and Di Blasio, 2018): a self-report measure designed to assess the extent to which the memory of a stressful and traumatic event was central to one’s (a) life history, (b) personal identity, and (c) attribution of meaning to other personal life events. These three factors are assessed using 20 items on a 5-point Likert scale ranging from 1 for “strongly disagree” to 5 for “strongly agree”. The questionnaire has good internal consistency (Cronbach’s alpha = 0.94).
- Trauma Symptom Checklist for Children (TSCC-A; Briere, 2011; Italian validation by Di Blasio, Piccolo, Traficante, 2011): used to assess post-traumatic stress and related psychological symptoms. This instrument is particularly suitable for assessing children and adolescents aged 11 to 16 years who have experienced traumatic events. Each item is rated on a 4-point Likert scale ranging from 0 for “never” to 3 for “almost always”. We used the 44-item version, which does not include references to sexual issues. The questionnaire consists of the following five clinical scales: (1) Anxiety, which captures general fear, overexcitement, worry, specific fears (e.g., of men, women, or both, of the dark, of being killed), episodes of free-floating fear, and a sense of impending danger. (2) Depression: feelings of sadness, unhappiness, and loneliness, episodes of weepiness, depressive cognitions such as guilt and self-denial, and self-harm and suicidality. (3) Anger, which deals with angry thoughts, feelings, and behaviors, such as feeling angry, being mean and hating others, having difficulty de-escalating anger, wanting to yell at or hurt people, arguing, or fighting. (4) Post-traumatic stress, which captures post-traumatic symptoms such as intrusive thoughts, sensations, and memories of painful past events, nightmares, anxiety, and cognitive avoidance of painful feelings; and (5) Dissociation, which examines dissociative symptoms such as derealization, thought emptiness, emotional numbing, pretending to be another person or place, daydreaming, memory problems, and dissociative avoidance. We chose to use the TSCC-A because our clinical sample was not in treatment, and this may have influenced the results of the Sexual Concerns scale. The questionnaire showed good internal consistency (Cronbach’s alpha = 0.83).
2.5. Analysis
3. Results
3.1. Psychological Well-Being and Effects of the Traumatic Event on Adolescents
3.2. Effects of the Traumatic Event on the Family System
4. Discussion
4.1. Psychological Well-Being and Effects of the Traumatic Event on Adolescents
4.2. Effects of the Traumatic Event on the Family System
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Health Observatory (GHO) data. Child Mortality and Causes of Death. Available online: http://www.who.int/gho/child_health/mortality/en/ (accessed on 17 May 2017).
- Mazzucco, W.; Cusimano, R.; Mazzola, S.; Rudisi, G.; Zarcone, M.; Marotta, C.; Graziano, G.; D’Angelo, P.; Vitale, F. Childhood and Adolescence Cancers in the Palermo Province (Southern Italy): Ten Years (2003–2012) of Epidemiological Surveillance. Int. J. Environ. Res. Public Health 2018, 15, 1344. [Google Scholar] [CrossRef] [Green Version]
- Steliarova-Foucher, E.; Stiller, C.; Kaatsch, P.; Berrino, F.; Coebergh, J.W.; Lacour, B.; Perkin, M. Geographical patterns and time trends of cancer incidence and survival among children and adolescents in Europe since the 1970s (the ACCIS project): An epidemiological study. Lancet 2004, 364, 2097–2105. [Google Scholar] [CrossRef] [PubMed]
- AIRTUM Working Group. Cancer in children and adolescents. Epidemiol. Prev. 2013, 37 (Suppl. S1), 1–296. [Google Scholar]
- Confalonieri, E.; Grazzani Gavezzi, I. Adolescenza e Compiti di Sviluppo; Edizione Unicopli: Milan, Italy, 2021. [Google Scholar]
- Righetti, P.L.; Santoro, L.; Sinatora, F.; Ricca, M. Psicologia e Pediatria. Strumenti per le Professioni Sociosanitarie; Franco Angeli: Milan, Italy, 2013; pp. 151–170. [Google Scholar]
- Ferrari, A. Non c’è un perché. Ammalarsi di Tumore in Adolescenza; Franco Angeli: Milan, Italy, 2016. [Google Scholar]
- Muzzatti, B.; Annunziata, M.A. Elementi di Psicologia Oncologica per le Professioni Sanitarie; Carocci editore S.P.A: Roma, Italy, 2020. [Google Scholar]
- Pagani Bagliacca, E.; Veneroni, L.; Ferrari, A.; Massimino, M. Curare e prendersi cura degli adolescenti ammalati di tumore: Evoluzione di un modello di assistenza centrato sul paziente. Altra Mod. 2020, 24, 39–50. [Google Scholar]
- Kutikov, A.; Weinberg, D.S.; Edelman, M.; Horwitz, E.M.; Uzzo, R.G.; Fisher, R.I. A War on Two Fronts: Cancer Care in the Time of COVID-19. Ann. Intern. Med. 2020, 172, 756–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moraliyage, H.; De Silva, D.; Ranasinghe, W.; Adikari, A.; Alahakoon, D.; Prasad, R.; Lawrentschuk, N.; Bolton, D. Cancer in Lockdown: Impact of the COVID-19 Pandemic on Patients with Cancer. Oncologist 2020, 26, 342–344. [Google Scholar] [CrossRef]
- Constantinou, C.; Kolokotroni, O.; Mosquera, M.; Heraclides, A.; Demetriou, C.; Karayiannis, P.; Quattrocchi, A.; Charalambous, A. Developing a holistic contingency plan: Challenges and dilemmas for cancer patients during the COVID-19. Cancer Med. 2020, 9, 6082–6092. [Google Scholar] [CrossRef]
- Fung, M.; Babik, J.M. COVID-19 in Immunocompromised Hosts: What We Know So Far. Clin. Infect. Dis. 2020, 72, 340–350. [Google Scholar] [CrossRef]
- Tremolada, M.; Bonichini, S.; Basso, G.; Pillon, M. Post-traumatic Stress Symptoms and Post-traumatic Growth in 223 Childhood Cancer Survivors: Predictive Risk Factors. Front. Psychol. 2016, 7, 287. [Google Scholar] [CrossRef] [Green Version]
- Compas, B.E.; Jaser, S.; Dunn, M.J.; Rodriguez, E.M. Coping with chronic illness in childhood and adolescence. Annu. Rev. Clin. Psychol. 2012, 8, 455–480. [Google Scholar] [CrossRef] [Green Version]
- Band, E.B.; Weisz, J.R. Developmental differences in primary and secondary control coping and adjustment to juvenile diabetes. J. Clin. Child Psychol. 1990, 19, 150–158. [Google Scholar] [CrossRef]
- Han, S.S.; Weisz, J.R.; Weiss, B. Specificity in relations between control-related beliefs and internalizing and externalizing psychpathology. J. Consult. Clin. Psychol. 2001, 69, 240–251. [Google Scholar] [CrossRef] [PubMed]
- Rothbaum, R.; Weisz, J.R.; Snyder, S. Changing the world and changing the self: A two process model of perceived control. J. Personal. Soc. Psychol. 1982, 42, 5–37. [Google Scholar] [CrossRef]
- Rudolph, K.D.; Dennig, M.D.; Weisz, J.R. Determinants and consequences of children’s coping in the medical setting: Conceptualization, review and critique. Psychol. Bull. 1995, 118, 328–357. [Google Scholar] [CrossRef]
- Weisz, J.R.; Rothbaum, F.M.; Blackburn, T.C. Standing out and standing in: The psychology of control in America and Japan. Am. Psychol. 1984, 39, 955–969. [Google Scholar] [CrossRef]
- Nichols, M.P.; Schwartz, R.C. Family Therapy: Concepts and Methods, 4th ed.; Allyn & Bacon: Boston, MA, USA, 1995. [Google Scholar]
- Briere, J. Trauma Sympom Checklist for Children. In Valutazione delle Conseguenze Psicologiche di Esperienze Traumatiche; Blasio, P., Piccolo, M., Traficante, D., Eds.; Edizioni Erickson: Gardolo, Italy, 2011; pp. 7–16. [Google Scholar]
- Pai, A.L.H.; Drotar, D.; Zebracki, K.; Moore, M.; Youngstrom, E. A meta-analysis of the effects of psychological interventions in pediatric oncology on outcomes of psychological distress and adjustment. J. Pediatr. Psychol. 2006, 31, 978–988. [Google Scholar] [CrossRef]
- Saevarsdottir, T.; Fridriksdottir, N.; Gunnarsdottir, S. Quality of life and symptoms of anxiety and depression of patients receiving cancer chemotherapy: Longitudinal study. Cancer Nurs. 2010, 33, E1–E10. [Google Scholar] [CrossRef]
- Patenaude, A.F.; Kupst, M.J. Psychosocial functioning in pediatric cancer. J. Pediatr. Psychol. 2005, 30, 9–27. [Google Scholar] [CrossRef] [PubMed]
- Phipps, S. Adaptive style in children with cancer: Implications for a positive psychology approach. J. Pediatr. Psychol. 2007, 32, 1055–1066. [Google Scholar] [CrossRef] [Green Version]
- Zebrack, B.; Kwak, M.; Meeseke, K.A.; Embry, L.; Aguilar, C.; Block, R.; Hayes-Lattin, B.; Li, Y.; Butler, M.; Cole, S. Trajectories of psychological distress in adolescent and young adult patients with cancer: A 1-year longitudinal study. J. Clin. Oncol. 2018, 32, 2160–2166. [Google Scholar]
- Zucchetti, G.; Bertolotti, M.; Fagioli, F. How paediatric psycho-oncology is changing during the COVID-19 epidemic in Italy: New approaches. Psychooncology 2020, 29, 1384–1386. [Google Scholar] [CrossRef] [PubMed]
- Glidden, C.; Howden, K.; Romanescu, R.G.; Hatala, A.; Scott, I.; Deleemans, J.M.; Chalifour, K.; Eaton, G.; Gupta, A.; Bolton, J.; et al. Psychological distress and experiences of Adolescents and Young Adults with cancer during the COVID-19 pandemic: A cross-sectional survey. Wiley 2021, 31, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.L.; Russel, K.; Long, A.; Phipps, S. Centrality of the childhood cancer experience and its relation to post-traumatic stress and growth. Wiley 2021, 30, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Kosir, U.; Wiedemann, M.; Wild, J.; Bowes, L. Cognitive Mechanisms in Adolescent and Young Adult Cancer Patients and Survivors: Feasibility and Preliminary Insights from the Cognitions and Affect in Cancer Resiliency Study. J. Adolesc. Young Adult Oncol. 2020, 9, 289–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| CES | Sample | Mean | Standard Deviation | T | Sign. | gl |
|---|---|---|---|---|---|---|
| Factor I | Clinical group | 53.36 | 8.98 | 2.450 | 0.017 | 64.873 |
| Control group | 47.88 | 10.11 | ||||
| Factor II | Clinical group | 55.86 | 8.11 | 4.686 | 0.000014 | 65.742 |
| Control group | 46.30 | 9.34 | ||||
| Factor III | Clinical group | 54.39 | 9.88 | 3.146 | 0.003 | 56.123 |
| Control group | 47.23 | 9.13 | ||||
| Total | Clinical group | 55.24 | 8.42 | 4.061 | 0.000134 | 65.161 |
| Control group | 46.69 | 9.55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ionio, C.; Bigoni, F.; Sacchi, M.; Zecca, M.; Bergami, E.; Landoni, M.; Ciuffo, G.; Rovati, A.; Rizzi, D. Exploring the Effects of Cancer as a Traumatic Event on Italian Adolescents and Young Adults: Investigating Psychological Well-Being, Identity Construction and Coping Strategies. Pediatr. Rep. 2023, 15, 254-262. https://doi.org/10.3390/pediatric15010021
Ionio C, Bigoni F, Sacchi M, Zecca M, Bergami E, Landoni M, Ciuffo G, Rovati A, Rizzi D. Exploring the Effects of Cancer as a Traumatic Event on Italian Adolescents and Young Adults: Investigating Psychological Well-Being, Identity Construction and Coping Strategies. Pediatric Reports. 2023; 15(1):254-262. https://doi.org/10.3390/pediatric15010021
Chicago/Turabian StyleIonio, Chiara, Francesca Bigoni, Maddalena Sacchi, Marco Zecca, Elena Bergami, Marta Landoni, Giulia Ciuffo, Anna Rovati, and Damiano Rizzi. 2023. "Exploring the Effects of Cancer as a Traumatic Event on Italian Adolescents and Young Adults: Investigating Psychological Well-Being, Identity Construction and Coping Strategies" Pediatric Reports 15, no. 1: 254-262. https://doi.org/10.3390/pediatric15010021
APA StyleIonio, C., Bigoni, F., Sacchi, M., Zecca, M., Bergami, E., Landoni, M., Ciuffo, G., Rovati, A., & Rizzi, D. (2023). Exploring the Effects of Cancer as a Traumatic Event on Italian Adolescents and Young Adults: Investigating Psychological Well-Being, Identity Construction and Coping Strategies. Pediatric Reports, 15(1), 254-262. https://doi.org/10.3390/pediatric15010021