Life Expectancy at Birth in Europe: An Econometric Approach Based on Random Forests Methodology




Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
3.1. Variables
3.1.1. Socio-Economic Variables
3.1.2. Ad hoc Variables
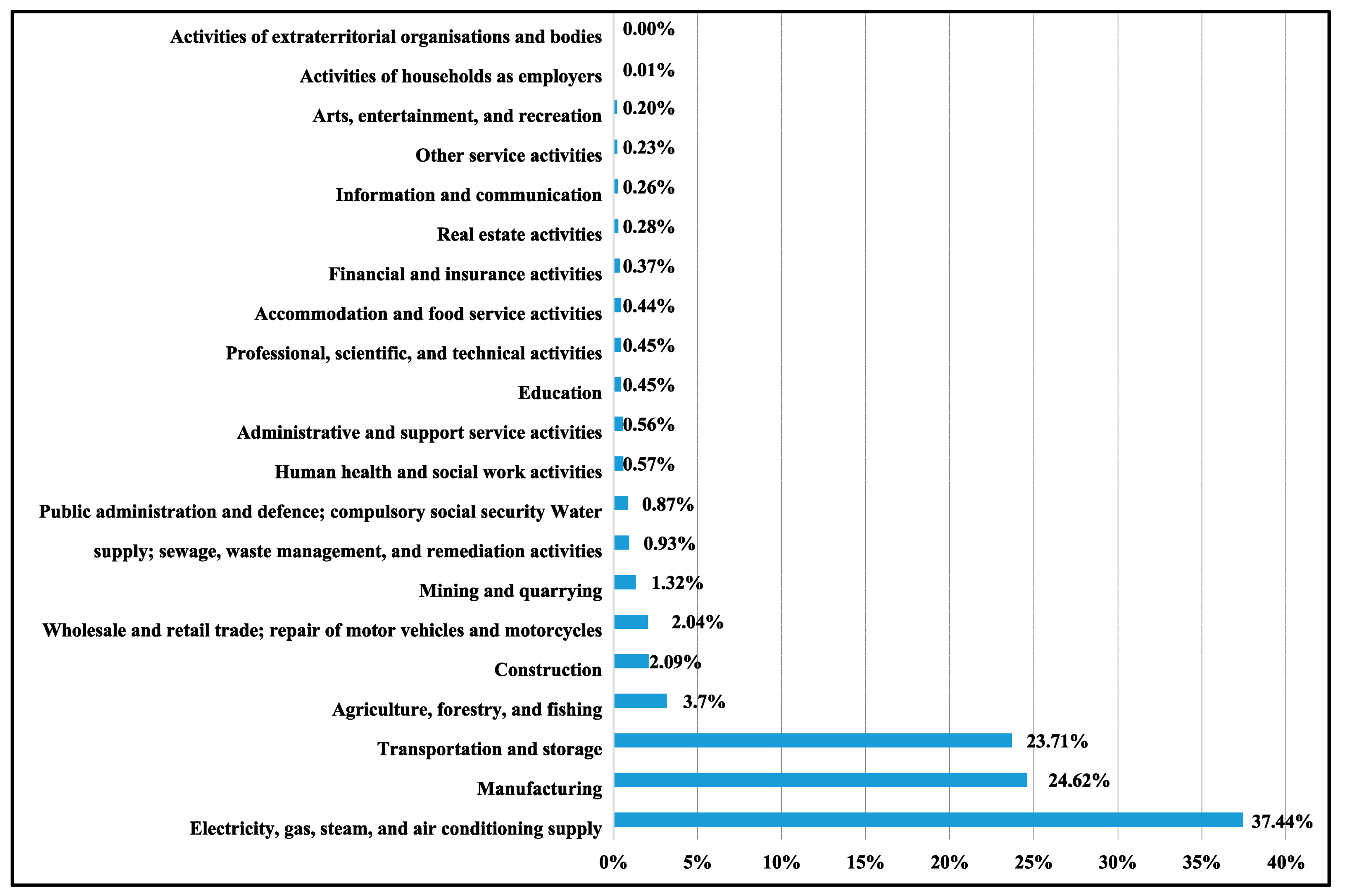
- The subscript represents the greenhouse gases included in the analysis: CO2, N2O and CH4.
- The subscript represents the economic sectors.
- denotes the annual average of the greenhouse gas i emitted by the economic sector j.
- represents the aggregate average of the 3 greenhouse gases emitted by the 21 economic sectors.
- denotes the percentage of greenhouse gas emissions attributable to sector j with respect to the average sum.
- reflects the total percentage greenhouse gas emitted by sectors whose are greater than 1%. A justification of this choice will be displayed in Section 3.2.
- Eastern EU countries (Bulgaria, Croatia, Czech Republic, Estonia, Hungary, Latvia, Lithuania, Poland, Romania, Slovakia, and Slovenia),
- Northern EU countries (Denmark, Finland, Ireland, Sweden, and United Kingdom),
- Southern EU countries (Cyprus, Greece, Italy, Malta, Portugal, and Spain), and
- Western EU countries (Austria, Belgium, France, Germany, Luxembourg, and Netherlands).
3.1.3. Other Potential Variables
3.2. Data
3.3. Random Forests Methodology
- If LE(countryi/yearj) > AVERAGE(LE/yeari = 2008,…,2017) ⇒ “LE increasing” ⇒ “Yes”.
- If LE(countryi/yearj) ≤ AVERAGE(LE/yeari = 2008,…,2017) ⇒ “LE decreasing” ⇒ “No”.
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Author (Date) [Reference Number] | Country | Period | Proxy of Health Status 1 | Methodology and Data 2 |
|---|---|---|---|---|
| Auster et al. (1969) [27] | US states | 1967 | M | CSR |
| Cochrane and St. Ledger (1978) [44] | 18 developed countries | 1970 (1969 or 1971) | MAG | CSR |
| Rodgers (1979) [45] | 56 countries (developed and developing countries) | Not specified | LEAB and IM | CSR |
| Wolfe and Gabay (1987) [30] | 22 OECD countries | 1960, 1970, 1980 | LEAB, LE 60, and IM | LSR approach for simultaneous models using CS |
| Peltzman (1987) [46] | 22 middle-income countries | 1970–1980 | M | CSR |
| McAvinchey (1988) [53] | 5 European countries | 1960–1982 | M | ADL using TS |
| Hitiris and Posnett (1992) [31] | 28 OECD countries | 1960–1987 | M | PR |
| Grubaugh and Rexford (1994) [32] | 12 OECD countries | 1960–1987 | IM | PR |
| Elola et al. (1995) [54] | 17 European countries | 1990 or 1991 | LE, PM, and IM | CSR |
| Crémieux et al. (1999) [33] | Canadian provinces | 1978–1992 | LEAB and IM | PR |
| Or (2000a) [21] | 21 OECD countries | 1970–1992 | PM | PR |
| Or (2000b) [22] | 21 OECD countries | 1970–1995 | LE 65, IM, and PM | PR |
| Garbaccio and Jorgenson (2000) [56] | China | Simulation for 1995, 2010, and 2030 | PM | A single-country CGE model |
| Robalino et al. (2001) [47] | 67 countries (OECD and less developed countries) | 1970–1995 | IM | PR |
| Berger and Messer (2002) [23] | 20 OECD countries | 1960–1992 | M | PR |
| Miller and Frech (2002) [36] | 18 OECD countries | 1998–1999 | LEAB, LE 40, LE 60, DALEB, DALE 60 and PM | CSR |
| Thornton (2002) [34] | US states | 1990 | AAM | CSR |
| Lichtenberg (2002) [35] | US | 1960–1997 | LEAB | MLE using TS |
| Self and Grabowski (2003) [48] | 191 countries (developed, middle-income, and less-developed countries) | 2000 | DALEB | CSRs |
| Laporte (2004) [37] | US | 1948–1996 | M | ECM using TS |
| Shaw et al. (2005) [39] | 19 OECD countries | 1980, 1985, 1990, and 1997 | LE 40, LE 60, and LE 65 | CSR |
| Crémieux et al. (2005) [38] | A set of Canadian provinces | 1975–1998 | LEAB, LE 65 and IM | PR |
| Nixon and Ullmann (2006) [18] | 15 European countries | 1980–1995 | LEAB and IM | PR |
| Joumard et al. (2008) [28] | 23 OECD countries | 1981–2003 | LEAB, LE 65, PMA, and IM | PR |
| Bergh and Nilsson (2010) [49] | 92 countries (with different levels of development) | 1970–2005 | LEAB | PR using PCSE |
| Mariani et al. (2010) [50] | 132 countries (with different levels of development) | 2006 | LEAB | OLG using CS |
| Halicioglu (2011) [57] | Turkey | 1965–2005 | LEAB | ARDL to cointegration method using TS |
| Bradley et al. (2011) [40] | 30 OECD countries | 1995–2005 | LEAB, IM, LBW, MM, and PYLL | Pooled cross-sectional analysis |
| Cutler and Lleras-Muney (2012) [51] | 61 countries (with different levels of development) | 2004–2009 | Others health behavior indicators 3 | CSR |
| Heijink et al. (2013) [52] | 14 developed countries | 1996–2006 | AM | PR and macro-level cost-effectiveness analysis |
| Monsef and Mehrjardi (2015) [19] | 136 countries (with different levels of development) | 2002–2010 | LEAB | PR |
| Jorgenson and Givens (2015) [60] | 69 OECD and non-OECD countries | 1990–2008 | LE | TSCS Prais–Winsten regression model with PCSE, |
| Linden and Ray (2017) [24] | 34 OECD countries | 1970–2012 | LEAB | VAR using panel TS |
| Reynolds and Avendano (2017) [41] | 20 OECD countries | 1980–2010 | LE | PR |
| Van den Heuvel and Olaroiu (2017) [55] | 31 European countries | 2013 | LEAB | CSR |
| Toader et al. (2017) [25] | European countries of OECD | 1970–2014 | LEAB | PR |
| De Keijzer et al. (2017) [58] | Spain | 2009–2013 | LEAB and M | Poisson and linear regressions |
| Ketency and Murthy (2018) [42] | US | 1960–2012 | LEAB | Unit root testing and cointegration analysis using TS |
| Jiang et al. (2018) [20] | 31 Chinese provinces | 2000 and 2010 | LE | CSR |
| Hill and Jorgenson (2018) [43] | 50 US states and the District of Columbia | 2000, 2005, and 2010 | LEAB | PR |
| Martín-Cervantes et al. (2019) [29] | 17 Spanish regions | 2006–2016 | LEAB | Granger causality test |
| Chen et al. (2019) [59] | 43 developed countries and 33 Chinese provinces | 1970–2010 | LE loss | The air pollutant emission simulation model (GAINS) |
| Mohmmed et al. (2019) [61] | The top 10 CO2-emitting countries | 1991–2014 | HLE | PR |
References
- OECD. OECD Environmental Outlook to 2030; OECD: Paris, France, 2008. [Google Scholar]
- Forouzanfar, M.H.; Alexander, L.; Anderson, H.R.; Bachman, V.F.; Biryukov, S.; Brauer, M.; Burnett, R.; Casey, D.; Coates, M.M.; Cohen, A.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2287–2323. [Google Scholar] [CrossRef] [Green Version]
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Nejat, P.; Jomehzadeh, F.; Taheri, M.M.; Gohari, M.; Majid, M.Z.A. A global review of energy consumption, CO2 emissions and policy in the residential sector (with an overview of the top ten CO2 emitting countries). Renew. Sustain. Energy Rev. 2015, 43, 843–862. [Google Scholar] [CrossRef]
- Aunan, K.; Berntsen, T.; O’Connor, D.; Persson, T.H.; Vennemo, H.; Zhai, F. Benefits and costs to China of a climate policy. Environ. Dev. Econ. 2007, 12, 471–497. [Google Scholar] [CrossRef]
- Carraro, C.; Massetti, E. Energy and climate change in China. Environ. Dev. Econ. 2012, 17, 689–713. [Google Scholar] [CrossRef] [Green Version]
- Perrings, C. Environment and development economics 20 years on. Environ. Dev. Econ. 2014, 19, 333–366. [Google Scholar] [CrossRef]
- Gao, J.; Hou, H.; Zhai, Y.; Woodward, A.; Vardoulakis, S.; Kovats, S.; Wilkinson, P.; Li, L.; Song, X.; Xu, L.; et al. Greenhouse gas emissions reduction in different economic sectors: Mitigation measures, health co-benefits, knowledge gaps, and policy implications. Environ. Pollut. 2018, 240, 683–698. [Google Scholar] [CrossRef]
- Zheng, X.S.; Streimikiene, D.; Balezentis, T.; Mardani, A.; Cavallaro, F.; Liao, H. A review of greenhouse gas emission profiles, dynamics, and climate change mitigation efforts across the key climate change players. J. Clean. Prod. 2019, 234, 1113–1133. [Google Scholar] [CrossRef]
- Hashmi, R.; Alam, K. Dynamic relationship among environmental regulation, innovation, CO2 emissions, population, and economic growth in OECD countries: A panel investigation. J. Clean. Prod. 2019, 231, 1100–1109. [Google Scholar] [CrossRef]
- Brunekreef, B.; Holgate, S.T. Air pollution and health: Review. Lancet 2002, 360, 1233–1242. [Google Scholar] [CrossRef]
- Englert, N. Fine particles and human health—A review of epidemiological studies. Toxicol. Lett. 2004, 149, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Beelen, R.; Hoek, G.; van den Brandt, P.A.; Goldbohm, R.A.; Fischer, P.; Schouten, L.J.; Jerrett, M.; Hughes, E.; Armstrong, B.; Brunekreef, B. Long-term effects of traffic-related air pollution on mortality in a Dutch cohort (NLCS-AIR study). Environ. Health Perspect. 2008, 116, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Ezzati, M.; Dockery, D.W. Fine-particulate air pollution and life expectancy in the United States. N. Engl. J. Med. 2009, 360, 376–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelucchi, C.; Negri, E.; Gallus, S.; Boffetta, P.; Tramacere, I.; La Vecchia, C. Long-term particulate matter exposure and mortality: A review of European epidemiological studies. BMC Public Health 2009, 9, 453. [Google Scholar] [CrossRef]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio-respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef] [Green Version]
- Carey, I.M.; Atkinson, R.W.; Kent, A.J.; van Staa, T.; Cook, D.G.; Anderson, H.R. Mortality associations with long-term exposure to outdoor air pollution in a national English cohort. Am. J. Respir. Crit. Care Med. 2013, 187, 1226–1233. [Google Scholar] [CrossRef] [Green Version]
- Nixon, J.; Ullmann, P. The relationship between health care expenditure and health outcomes—Evidence and caveats for a causal link. Eur. J. Health Econ. 2006, 7, 7–19. [Google Scholar] [CrossRef]
- Monsef, A.; Mehrjardi, A.S. Determinants of life expectancy: A panel data approach. Asian Econ. Financ. Rev. 2015, 5, 1251–1257. [Google Scholar] [CrossRef] [Green Version]
- Jiang, J.; Luo, L.; Xu, P.; Wang, P. How does social development influence life expectancy? A geographically weighted regression analysis in China. Public Health 2018, 163, 95–104. [Google Scholar] [CrossRef]
- Or, Z. Determinants of health outcomes in industrialised countries: A pooled, cross-country, time series analysis. OECD Econ. Stud. 2000, 30, 53–77. [Google Scholar]
- Or, Z. Exploring the effects of health care on mortality across OECD countries. In OECD Labour Market and Social Policy Occasional Papers; Occasional Paper No. 46; OECD: Paris, France, 2000. [Google Scholar]
- Berger, M.; Messer, J. Public financing of health expenditure, insurance, and health outcomes. Appl. Econ. 2002, 34, 2105–2113. [Google Scholar] [CrossRef]
- Linden, M.; Ray, D. Life expectancy effects of public and private health expenditures in OECD countries 1970–2012: Panel time series approach. Econ. Anal. Policy 2017, 56, 101–113. [Google Scholar] [CrossRef] [Green Version]
- Toader, E.; Firtescu, B.; Oprea, F. Determinants of health status and public policies implications—Lessons for Romania. Transylv. Rev. Adm. Sci. 2017, 52, 128–147. [Google Scholar] [CrossRef] [Green Version]
- Švarcova, I.; Hošková-Mayerová, S.; Navrátil, J. Crisis Management and Education in Health. In Proceedings of the 7th ICEEPSY International Conference on Education and Educational Psychology, Rhodes, Greece, 11–15 October 2016; pp. 255–261. [Google Scholar]
- Auster, R.; Levesoardln, I.; Sarachek, S. The production of health: An exploratory study. J. Hum. Resour. 1969, 4, 411–436. [Google Scholar] [CrossRef]
- Joumard, I.; André, C.; Nicq, C.; Chatal, O. Health status determinants: Lifestyle, environment, health care resources and efficiency. In OECD Economics Department Working Papers; OECD Publishing: Paris, France, 2008; Volume 626. [Google Scholar]
- Martín-Cervantes, P.; Rueda-López, N.; Cruz-Rambaud, S. A Causal Analysis of Life Expectancy at Birth. Evidence from Spain. Int. J. Environ. Res. Public Health 2019, 16, 2367. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, B.L.; Gabay, M. Health status and medical expenditures: More evidence of a link. Soc. Sci. Med. 1987, 25, 883–888. [Google Scholar] [CrossRef]
- Hitiris, T.; Posnett, J. The determinants and effects of health expenditure in developed countries. J. Health Econ. 1992, 11, 173–181. [Google Scholar] [CrossRef]
- Grubaugh, S.G.; Rexford, E.S. Comparing the performance of health-care systems: An alternative approach. South. Econ. J. 1994, 60, 1030–1042. [Google Scholar] [CrossRef]
- Crémieux, P.-Y.; Ouellette, P.; Pilon, C. Health care spending as determinants of health outcomes. Health Econ. 1999, 8, 627–639. [Google Scholar] [CrossRef]
- Thornton, J. Estimating a Health Production Function for the US: Some New Evidence. Appl. Econ. 2002, 34, 59–62. [Google Scholar] [CrossRef]
- Lichtenberg, F.R. Sources of U.S. longevity increase, 1960–1997. Q. Rev. Econ. Financ. 2004, 44, 369–389. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.D.; Frech, T. The Productivity of Health Care and Pharmaceuticals: Quality of Life, Cause. In UCSB Departmental Working Paper; No. 12-02; University of California: Santa Barbara, CA, USA, 2002. [Google Scholar]
- Laporte, A. Do economic cycles have a permanent effect on population health? Revisiting the Brener hypothesis. Health Econ. 2004, 13, 767–779. [Google Scholar] [CrossRef] [PubMed]
- Crémieux, P.Y.; Mieilleur, M.C.; Ouellette, P.; Petit, P.; Zelder, P.; Potvin, K. Public and private pharmaceutical spending as determinants of health outcomes in Canada. Health Econ. 2005, 14, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.W.; Horrace, W.C.; Vogel, R.J. The determinants of life expectancy: An analysis of the OECD health data. South. Econ. J. 2005, 71, 768–783. [Google Scholar] [CrossRef] [Green Version]
- Bradley, E.H.; Elkins, B.R.; Herrin, J.; Elbel, B. Health and social services expenditures: Associations with health outcomes. BMJ Qual. Saf. 2011, 20, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, M.M.; Avendano, M. Social policy expenditures and life expectancy in high–income countries. Am. J. Prev. Med. 2017, 54, 72–79. [Google Scholar] [CrossRef]
- Ketenci, N.; Murthy, V.N.R. Some determinants of life expectancy in the United States: Results from cointegration tests under structural breaks. J. Econ. Financ. 2018, 42, 508–525. [Google Scholar] [CrossRef]
- Hill, T.D.; Jorgenson, A. Bring out your dead! A study of income inequality and life expectancy in the United States, 2000–2010. Health Place 2018, 49, 1–6. [Google Scholar] [CrossRef]
- Cochrane, A.L.; St Ledger, A.S.; Moore, F. Health service ‘input’ and mortality ‘output’ in developed countries. J. Epidemiol. Community Health 1978, 32, 200–205. [Google Scholar]
- Rodgers, G.B. Income and inequality as determinants of mortality: An international cross–sectional analysis. Popul. Stud. 1979, 33, 343–351. [Google Scholar] [CrossRef]
- Peltzman, S. Regulation and health: The case of mandatory prescriptions and an extension. Manag. Decis. Econ. 1987, 8, 41–46. [Google Scholar] [CrossRef]
- Robalino, D.A.; Oscar, F.P.; Albertus, V. Does Fiscal Decentralization Improve Health Outcomes? Evidence from A Cross–Country Analysis; World Bank Policy Research Working Paper Series; The World Bank: Washington, DC, USA, 2001; Volume 2565, pp. 1–14. [Google Scholar]
- Self, S.; Grabowski, R. How effective is public health expenditure in improving overall health? A cross–country analysis. Appl. Econ. 2003, 35, 835–845. [Google Scholar] [CrossRef]
- Bergh, A.; Nilsson, T. Good for living? On the relationship between globalization and life expectancy. World Dev. 2010, 38, 1191–1203. [Google Scholar] [CrossRef]
- Mariani, F.; Pérez-Barahona, A.; Raffin, N. Life expectancy and the environment. J. Econ. Dyn. Control 2010, 34, 798–815. [Google Scholar] [CrossRef]
- Cutler, D.M.; Lleras-Muney, A. Education and health: Insights from international comparisons. NBER Work. Pap. 2012, 17738, 1–46. [Google Scholar]
- Heijink, R.; Koolman, X.; Westert, G.P. Spending more money, saving more lives? The relationship between avoidable mortality and healthcare spending in 14 countries. Eur. J. Health Econ. 2013, 14, 527–538. [Google Scholar] [CrossRef]
- McAvinchey, I.D. A comparison of unemployment, income and mortality interaction for five European countries. Appl. Econ. 1988, 20, 453–471. [Google Scholar] [CrossRef]
- Elola, J.; Daponte, A.; Navarro, V. Health Indicators and the Organization of Health Care Systems in Western Europe. Am. J. Public Health 1995, 85, 1397–1401. [Google Scholar] [CrossRef] [Green Version]
- Van den Heuvel, W.J.A.; Olaroiu, M. How important are health care expenditures for life expectancy? A comparative, European analysis. J. Am. Med Dir. Assoc. 2017, 18, e9–e276. [Google Scholar] [CrossRef]
- Garbaccio, R.F.; Ho, M.S.; Jorgenson, D.V. The Health Benefits of Controlling Carbon Emissions in China. In Ancillary Benefits and Costs of greenhouse Gas Mitigation; OECD Publishing: Paris, France, 2000; pp. 343–376. [Google Scholar]
- Halicioglu, F. Modeling life expectancy in Turkey. Econ. Model. 2011, 28, 2075–2082. [Google Scholar] [CrossRef] [Green Version]
- De Keijzer, C.; Agis, D.; Ambrós, A.; Arévalo, G.; Baldasano, J.M.; Bande, S.; Barrera-Gómez, J.; Benach, J.; Cirach, M.; Dadvand, P.; et al. The association of air pollution and greenness with mortality and life expectancy in Spain: A small-area study. Environ. Int. 2017, 99, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Li, M.; Li, F.; Tang, H. Response of Global Air Pollutant Emissions to Climate Change and Its Potential Effects on Human Life Expectancy Loss. Sustainability 2019, 11, 3670. [Google Scholar] [CrossRef] [Green Version]
- Jorgenson, A.K.; Givens, J. The changing effect of economic development on the consumption-based carbon intensity of well-being, 1990–2008. PLoS ONE 2015, 10, e0123920. [Google Scholar] [CrossRef] [Green Version]
- Mohmmed, A.; Lia, Z.; Arowoloa, A.O.; Su, H.; Denga, X.; Najmuddina, O.; Zhang, Y. Driving factors of CO2 emissions and nexus with economic growth, development and human health in the Top Ten emitting countries. Resour. Conserv. Recycl. 2019, 148, 157–169. [Google Scholar] [CrossRef]
- Ustaoglu, E.; Williams, B. Determinants of urban expansion and agricultural land conversion in 25 EU countries. Environ. Manag. 2017, 60, 717–746. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Communication from the Commission to the European Parliament, the European Council, the Council, the European Economic and Social Committee, the Committee of the Regions and the European Investment Bank: A Clean Planet for All a European Strategic Long-Term Vision for a Prosperous, Modern, Competitive and Climate Neutral Economy; COM (2018) 773 Final; European Commission: Brussels, Belgium, 2018. [Google Scholar]
- EEA. Manual for the EEA Greenhouse Gas Data Viewer; European Environment Agency (EEA), 2016; Available online: https://www.eea.europa.eu/data-and-maps/data/data-viewers/greenhouse-gases-viewer (accessed on 10 May 2019).
- UNO. Composition of Macro Geographical Regions, Geographical Sub-Regions, and Selected Economic and Other Groupings. 2016. Available online: http://millenniumindicators.un.org (accessed on 27 June 2019).
- Govindaraju, D.; Atzmon, G.; Barzilai, N. Genetics, lifestyle and longevity: Lessons from centenarians. Appl. Transl. Genom. 2015, 4, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindqvist, P.G.; Epstein, E.; Nielsen, K.; Landin-Olsson, M.; Ingvar, C.; Olsson, H. Avoidance of sun exposure as a risk factor for major causes of death: A competing risk analysis of the Melanoma in Southern Sweden cohort. J. Intern. Med. 2016, 280, 375–387. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Vasilopoulou, E. Mediterranean diet and longevity. Br. J. Nutr. 2001, 84 (Suppl. 2), S205–S209. [Google Scholar] [CrossRef]
- Huijts, T.; Kraaykamp, G. Religious involvement, religious context, and self-assessed health in Europe. J. Health Soc. Behav. 2011, 52, 91–106. [Google Scholar] [CrossRef] [Green Version]
- Mann, J.R.; Larimore, W. Impact of religious attendance on life expectancy. J. Am. Board Fam. Med. 2006, 19, 429–430. [Google Scholar] [CrossRef] [Green Version]
- Wallace, L.E.; Anthony, R.; End, C.M.; Way, B.M. Does religion stave off the grave? Religious affiliation in one’s obituary and longevity. Soc. Psychol. Personal. Sci. 2019, 10, 662–670. [Google Scholar] [CrossRef]
- Marmot, M.; Allen, J.J. Social determinants of health equity. Am. J. Public Health 2014, 104 (Suppl. 4), 723–731. [Google Scholar] [CrossRef] [PubMed]
- IEA. Energy and Air Pollution. In World Energy Outlook Special Report; International Energy Agency: Paris, France, 2016. [Google Scholar]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Breiman, L. Random Forests; Working Paper; Statistics Department, University of California Berkeley: Berkeley, CA, USA, 2001. [Google Scholar]
- Breiman, L. Bagging predictors. Mach. Learn. 1996, 24, 123–140. [Google Scholar] [CrossRef] [Green Version]
- Ho, T.K. Random decision forests. In Proceedings of the 3rd International Conference on Document Analysis and Recognition, Montreal, QC, Canada, 14–16 August 1995; IEEE Computer Society; pp. 278–282. [Google Scholar]
- Ho, T.K. The random subspace method for constructing decision forests. IEEE Trans. Pattern Anal. Mach. Intell. 1998, 20, 832–844. [Google Scholar]
- Cutler, A.; Cutler, D.R.; Stevens, J.R. Random Forests. In Ensemble Machine Learning: Methods and Applications; Zhang, C., Ma, Y., Eds.; Springer Science + Business Media: New York, NY, USA, 2012; pp. 157–176. [Google Scholar]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.J.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [Green Version]
- Chetty, R.; Stepner, M.; Abraham, S.; Lin, S.; Scuderi, B.; Turner, N.; Bergeron, A.; Cutler, D. The Association between Income and Life Expectancy in the United States, 2001–2014. JAMA 2016, 315, 1750–1766. [Google Scholar] [CrossRef]
- Cutler, D.M.; Lleras-Muney, A. Understanding differences in health behaviors by education. J. Health Econ. 2010, 29, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Álvarez-Gálvez, J.; Rodero-Cosano, M.L.; García-Alonso, C.R.; Salvador-Carulla, L. Changes in socioeconomic determinants of health: Comparing the effect of social and economic indicators through European welfare state regimes. J. Public Health 2014, 22, 305–311. [Google Scholar] [CrossRef]
- He, L.; Wu, M.; Wang, D.; Zhong, Z. A study of the influence of regional environmental expenditure on air quality in China: The effectiveness of environmental policy. Environ. Sci. Pollut. Res. 2018, 25, 7454–7468. [Google Scholar] [CrossRef] [PubMed]
- Stuckler, D.; Basu, S.; McKee, M. Budget crises, health, and social welfare programmes. BMJ 2010, 341, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Bradley, E.H.; Canavan, M.; Rogan, E.; Talbert-Slagle, K.; Ndumele, C.; Taylor, L.; Curry, L.A. Variation in health outcomes: The role of spending on social services, public health, and health care. 2000-09. Health Aff. 2016, 35, 760–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vavken, P.; Pagenstert, G.; Grimm, C.; Dototka, R. Does increased health care spending afford better health care outcomes? Evidence from Austrian health care expenditure since the initiations of DRGs. Swiss Med Wkly. 2012, 142, w13589. [Google Scholar]
- McCullough, J.M.; Leider, J.P. Government spending in health and nonhealth sectors associated with improvement in county health rankings. Health Aff. 2016, 35, 2037–2043. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Wang, J. Does Quality of Government Matter in Public Health? Comparing the Role of Quality and Quantity of Government at the National Level. Sustainability 2019, 11, 3229. [Google Scholar] [CrossRef] [Green Version]



| Variable Types | Abbreviated Variable Name | Variable Name |
|---|---|---|
| Dependent variable | LE | Life expectancy at birth |
| Independent variable #1 | INCO | Per capita income 1 |
| Independent variable #2 | LEDU | Educational level 2 |
| Independent variable #3 | ENVIRO | Environmental protection 3 |
| Independent variable #4 | SOPRO | Social protection 4 |
| Independent variable #5 | HEALTH | Health 5 |
| Statistic | LE | INCO | LEDU | ENVIRO | SOPRO | HEALTH |
|---|---|---|---|---|---|---|
| Mean | 79.3 | 24.6 | 72.6 | 0.8 | 16.8 | 6.3 |
| Median | 80.6 | 21.2 | 75.4 | 0.7 | 16.6 | 6.7 |
| Maximum | 83.5 | 65.7 | 88.0 | 1.9 | 25.6 | 8.9 |
| Minimum | 71.7 | 4.7 | 29.2 | −0.3 | 9.1 | 2.6 |
| Range | 11.8 | 61.0 | 58.8 | 2.2 | 16.5 | 6.3 |
| Interquartile range | 4.5 | 23.5 | 11.1 | 0.5 | 6.1 | 2.4 |
| Standard deviation | 2.9 | 14.0 | 11.8 | 0.3 | 3.8 | 1.5 |
| Skewness | −0.7 | 0.6 | −1.5 | 0.5 | 0.3 | −0.5 |
| Kurtosis | 2.2 | 2.4 | 5.0 | 3.6 | 2.3 | 2.4 |
| Summary of the Achieved Random Forests Model Results Implemented in the Variable LE | ||||
|---|---|---|---|---|
| No. of observations used to build the model: | 196 | |||
| Type of Random Forests: | Classification | |||
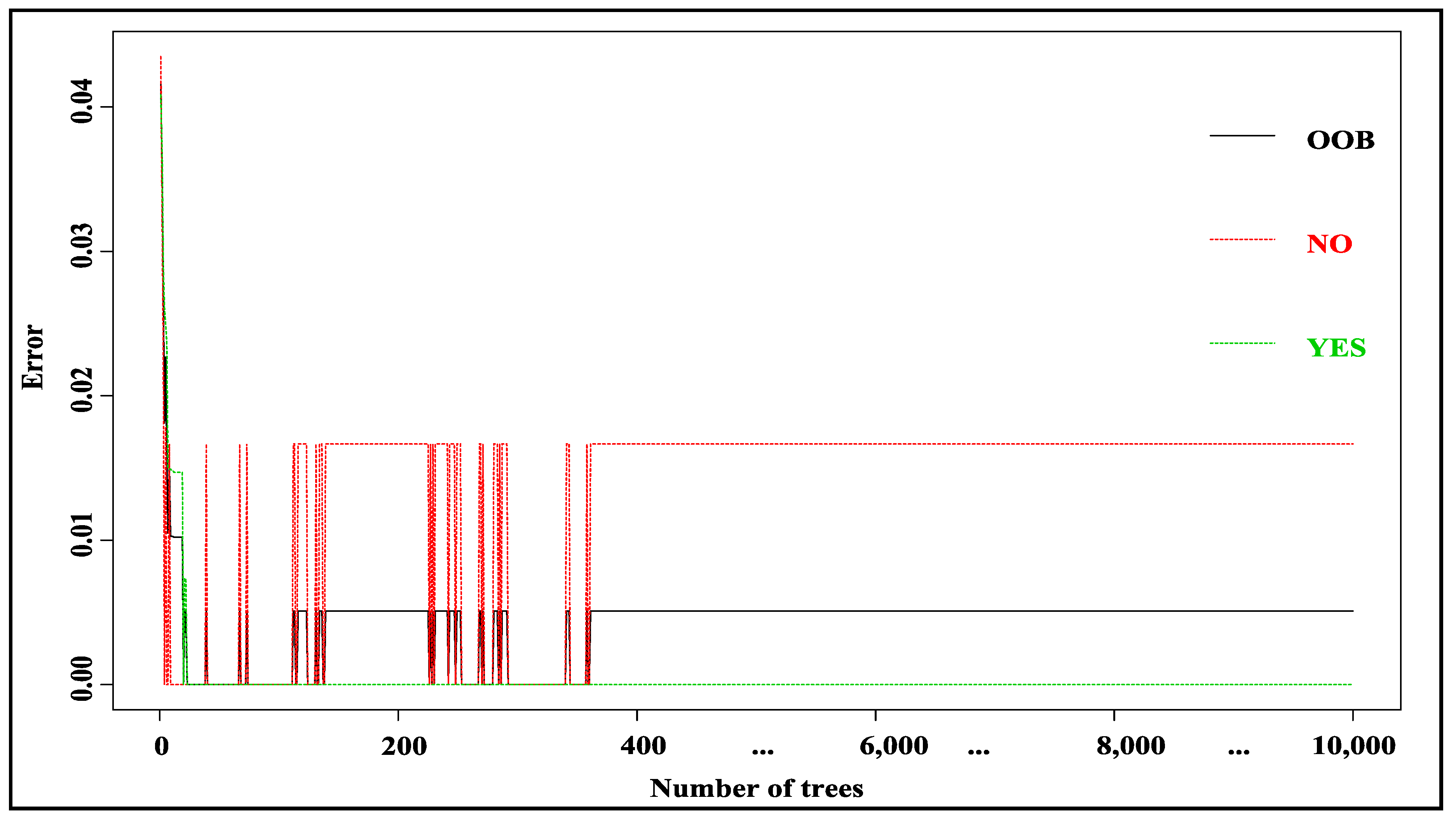
| Number of trees: | 10,000 | |||
| No. of variables tried at each split: | 6 | |||
| Out-of-bag (OOB) estimate of error rate: | 1.02% | |||
| Confusion matrix | ||||
| NO | YES | Classification error | ||
| NO | 59 | 1 | 0.016666667 (1/60) | |
| YES | 1 | 135 | 0.007352941 (1/136) | |
| Area under the curve: 95% confidence interval: 0.9701 (see [80]) | ||||
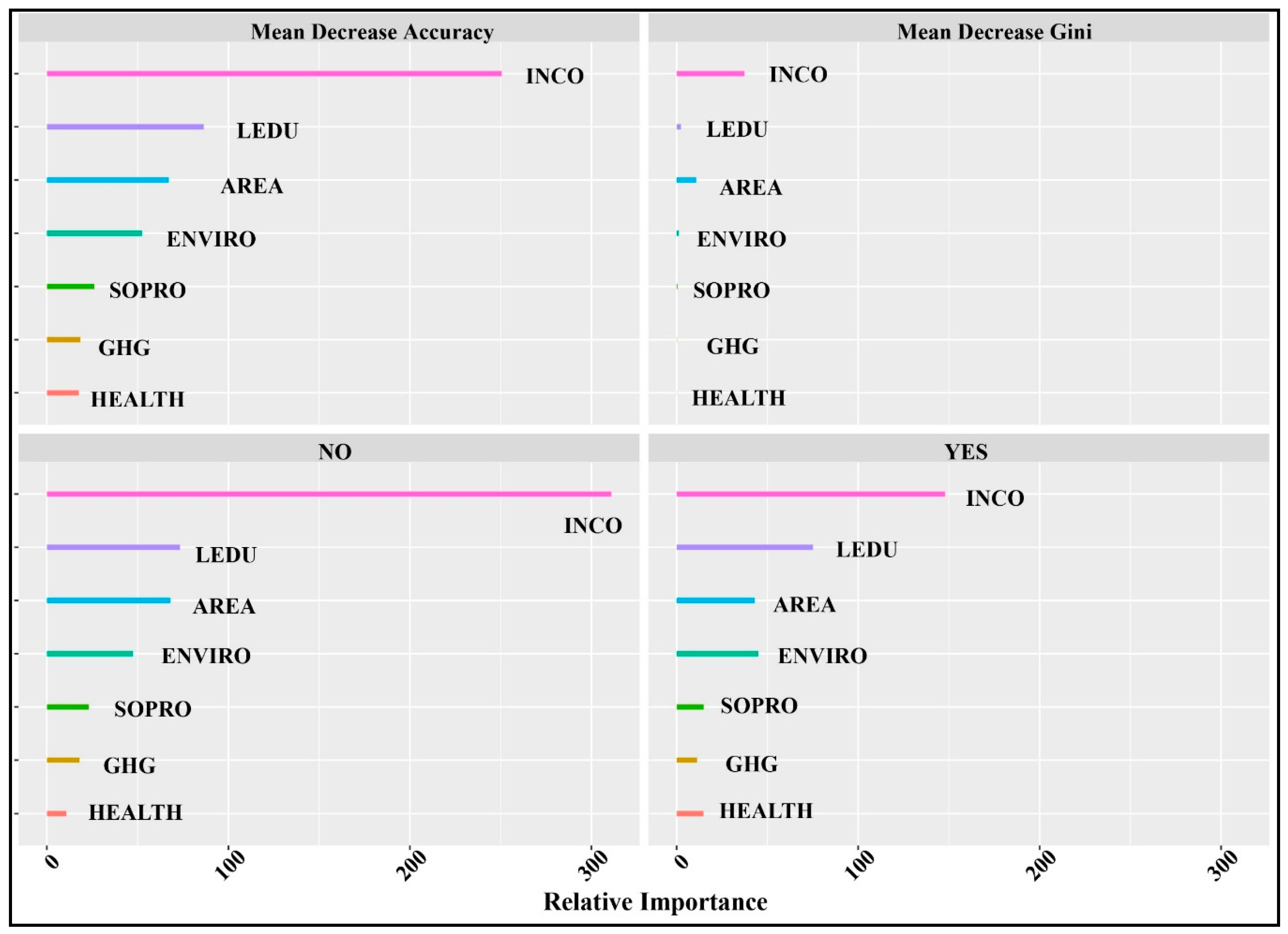
| Variable importance | ||||
| NO | YES | Mean decrease accuracy | Mean decrease Gini | |
| INCO | 311.02 | 147.93 | 250.60 | 37.40 |
| LEDU | 73.29 | 75.12 | 86.40 | 2.35 |
| AREA | 67.97 | 42.95 | 67.11 | 10.72 |
| ENVIRO | 47.40 | 44.95 | 52.43 | 1.13 |
| SOPRO | 23.07 | 14.90 | 26.15 | 0.48 |
| GHG | 18.02 | 11.20 | 18.40 | 0.25 |
| HEALTH | 10.78 | 14.83 | 17.56 | 0.15 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín Cervantes, P.A.; Rueda López, N.; Cruz Rambaud, S. Life Expectancy at Birth in Europe: An Econometric Approach Based on Random Forests Methodology. Sustainability 2020, 12, 413. https://doi.org/10.3390/su12010413
Martín Cervantes PA, Rueda López N, Cruz Rambaud S. Life Expectancy at Birth in Europe: An Econometric Approach Based on Random Forests Methodology. Sustainability. 2020; 12(1):413. https://doi.org/10.3390/su12010413
Chicago/Turabian StyleMartín Cervantes, Pedro Antonio, Nuria Rueda López, and Salvador Cruz Rambaud. 2020. "Life Expectancy at Birth in Europe: An Econometric Approach Based on Random Forests Methodology" Sustainability 12, no. 1: 413. https://doi.org/10.3390/su12010413
APA StyleMartín Cervantes, P. A., Rueda López, N., & Cruz Rambaud, S. (2020). Life Expectancy at Birth in Europe: An Econometric Approach Based on Random Forests Methodology. Sustainability, 12(1), 413. https://doi.org/10.3390/su12010413