1. Introduction
As the global population, the number of healthcare facilities, and the demand for medical services have all grown over the last decade, there has been a corresponding increase in the generation of healthcare wastes (HCWs) on a global scale. Simultaneously, trends such as the production of medical devices with multiple uses and a shift towards safer, single-use alternatives have contributed to the rise in HCW production. Consequently, managing HCW has become a challenging task for municipalities and regions, particularly in European countries that have enforced stringent regulations governing the safe handling, transport, and management of municipal and HCW waste [
1]. Given that the improper disposal of HCWs poses a serious risk of infection or injury to healthcare workers and the general public, it is now a top priority in global public health and environmental concerns. These factors have fueled a growing interest in HCW management within academic and professional circles [
2].
The intricate and complex process of HCW management involves waste collection, the careful selection of transfer routes to minimize hazards, choosing appropriate disposal plant sites, selecting suitable HCW treatment technologies to minimize pollution, and, ultimately, recovering some of the lost energy in the entire chain. Numerous socio-cultural factors associated with these processes concurrently lead local societies to erect barriers and impose bureaucratic procedures (‘red tape’) to mitigate the adverse impacts resulting from improper HCW management. The selection of the best and most efficient treatment technique for HCWs has garnered significant scientific interest due to its far-reaching ecological and economic consequences. In general, the use of the multi-criteria decision-making (MCDM) tool can be of considerable assistance in evaluating HCW treatment options, addressing this complex and significant challenge.
2. Related Work
MCDM assists various decision-makers and businesses in reaching reasonable conclusions, both in quantitative and qualitative terms. It offers suggestions for improving options in the direction of a particular objective or utility, making use of a variety of analytical techniques [
3] and instruments to assess how all pertinent data affect the decision-making process. MCDM is a goal-oriented procedure that offers the assistance required to accomplish this aim. While the traditional approach aims to find a single optimal solution, real-life problems often involve multiple options and evaluation criteria, making this goal unattainable [
4]. In practice, many problems require the consideration of numerous criteria before a final decision can be reached. Unfortunately, as the number of assessment criteria increases, the decision-making process becomes more challenging. To address this issue, decision-makers often employ ensembles of various techniques in order to achieve near optimal performance in the system. The ensemble approaches have proven advantageous in improving the effectiveness and reliability of the produced DSS. Another challenge may also refer to deciding which scenario is beneficial and/or which approach to follow amongst alternative choices [
5]. Simultaneously, when criteria evaluation is expressed through linguistic terms, fuzzy and intuitionistic fuzzy MCDM (IFMCDM) have demonstrated their effectiveness. Among various IFMCDM methodologies [
6], intuitionistic fuzzy TOPSIS (IFTOPSIS) stands out as the most popular. According to [
7], IFTOPSIS has been shown to yield results close to optimal when ordering criteria in multi-objective constrained waste management optimization problems [
8].
Studies on Medical/Hazardous Waste Management via Intuitionistic Fuzzy MCDM Methodologies
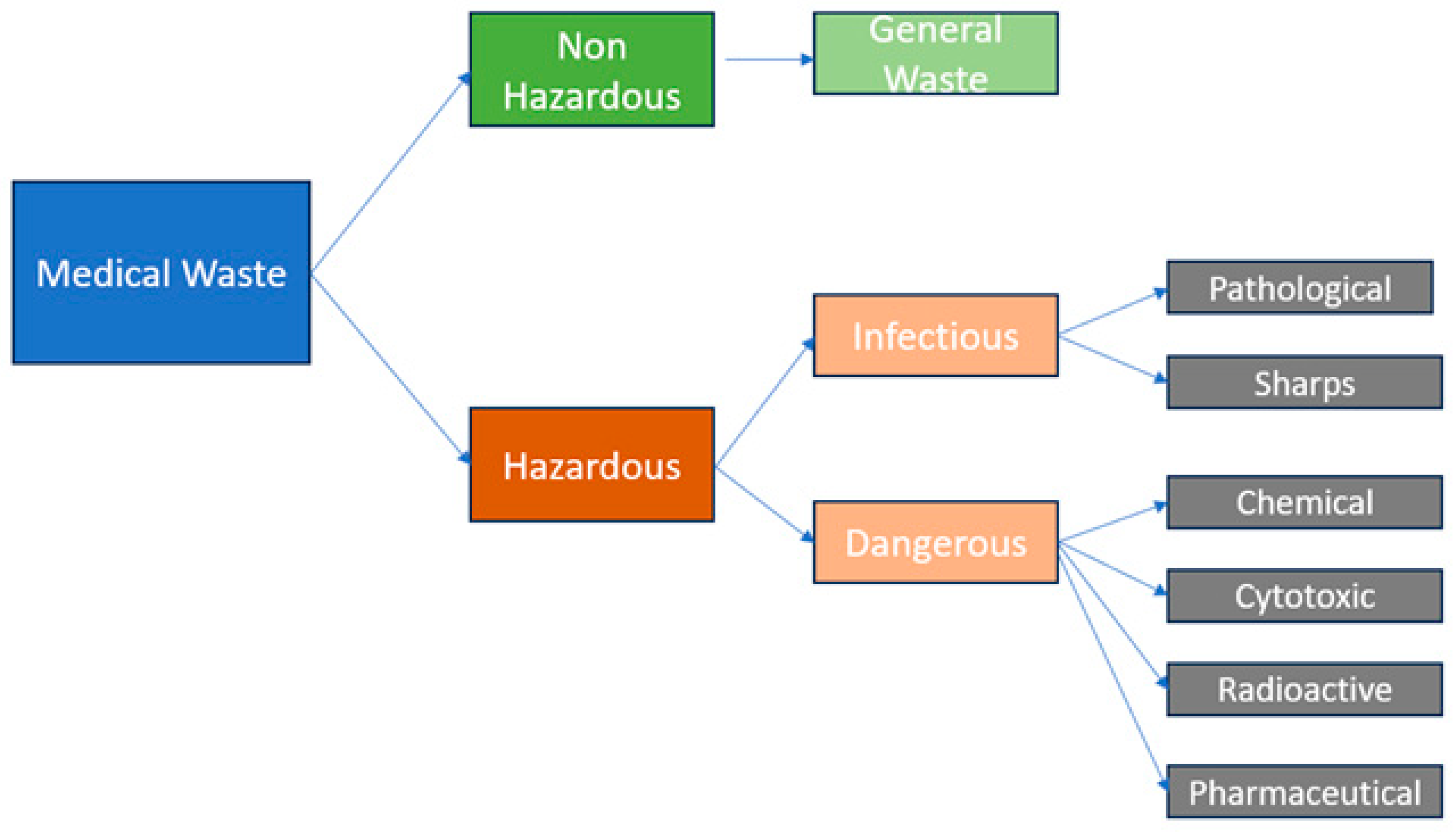
Healthcare waste (HCW) can be classified as either hazardous or non-hazardous based on specific characteristics it exhibits. Medical waste is inherently categorized as hazardous due to its potential inclusion of unwanted flammable, oxidizing, poisonous, radioactive, toxic, or explosive materials. The improper handling of such waste poses significant threats to both humans and the environment. Extensive research has been conducted on multiple-criteria decision-making (MCDM) methodologies for handling hazardous waste, including medical waste. However, there has been limited research utilizing intuitionistic fuzzy methodologies in this field until the occurrence of the COVID-19 pandemic. Due to the exponential growth in medical waste generated post-pandemic, there has been a rapid increase in research employing intuitionistic fuzzy methodologies to establish a practical hierarchy of criteria for effective waste management. The most recent and up-to-date insights on technologies for the treatment of solid medical waste have been presented by [
9]. The classification of medical waste, as outlined by [
7], is depicted in
Figure 1 and is representative of the current state in the Greek region in terms of hospital-produced waste. The authors list incineration, autoclaving, chemical disinfection, microwaving, irradiation, biological treatment, and encapsulation as the most popular methodologies for treating medical waste from a chemical-engineering perspective. The nature and categorization of medical waste, along with local laws and regulations, determine the most effective treatment procedure. To ensure the efficient and secure disposal of medical waste, some facilities may additionally employ a variety of treatment techniques.
In our original work, we explore the issue of medical waste treatment using an innovative holistic approach that encompasses social, transportation, management, and policy aspects. These include collection, storage, segregation, transportation, accident avoidance during transportation, safety practices of health workers, waste treatment, sanitation processes, disposal, capacity building of appointed companies, public awareness, monitoring processes, and overall safety. Our research on healthcare waste treatment and management is unique due to its unique approach to holistically treating the significant importance of related criteria using a repertoire of methodologies. This research is unique as it combines fuzzy methodologies with a holistic methodology, making it a unique study. Additionally, our research is the first to relate HCW holistic treatment methodologies with the region of Thessaly, Greece, making it a unique attempt in this area. Furthermore, our work successfully connects results from similar methodologies like IF-CORPAS and IF-TOPSIS with alternative objectives and scope methodologies like IF-DEMATEL, making it a unique comparative approach in the literature.
Furthermore, our focus is on advanced fuzzy logic methodologies to address the multi-criteria decision making involved in the aforementioned aspects. In this novel approach, we propose using an ensemble of such methodologies as the primary decision-making engine in a unique decision support system (DSS).
Table 1 summarizes the research on IF approaches used for this multi-objective issue.
3. Preliminaries
Since real-world HCW management issues are, by their very nature, multi-objective, we use intuitionistic fuzzy sets (IFS). The use of IFS guarantees the coverage of all participating criteria in the process and the inclusion of categorical data (linguistic expert responses) when needed. In support of that, many associated methodologies have been developed lately such as interval-valued [
26], IF-DEMATEL [
27], Pythagorean IFS [
30], etc. to address the HCW-related problems. A membership function and a non-membership function are used to represent an IFS of this type. This feature makes IFS superior compared to conventional fuzzy systems since it enables them to integrate reluctance and uncertainty at the same time. The fundamental definitions of IFS are provided in this section, while subsequent subsections provide thorough descriptions of the particular IFS approaches used in this study.
3.1. IF Sets and Relevant Terminology
Definition 1 ([
30])
. Assuming a nonempty set X, and the existence of mapping as shown in the following function definition:where the IFS of X, designated as , is activated by with be the membership function, displaying the quantity of membership of x to the IFS , be the non-membership quantity which both indicate the level of membership of x to the IFS , presuming the restriction that . Definition 2 ([
30])
. Let be the uncertainty degree with that introduces the hesitation principle so that IFSs are to be [resented as tuples of three elements ( ). Definition 3 ([
30,
31])
. For an IF number (), we now define the Score and the Accuracy functions given by the following equations. Let us note that this initial definition of Score and Accuracy has been updated (update is indicated by *) and shown in Equation (2b): Definition 4. Let be a set of IF numbers. Moreover, let be the ordered set of their weights assuming an imposed multi-objective and multi-criteria decision-making methodology. For the set , we call the IF weighted average operator which is illustrated below: 3.2. Intuitionistic Fuzzy MCDM Methodology
Many components in an MCDM process cannot be precisely evaluated due to the heterogeneity of information and the inherent fuzziness in defining criteria weights by stakeholders. As an alternative, a significant number of decision-makers and stakeholders express their evaluations and assessments using linguistic phrases.
Table 2 below presents the most commonly used rating scale, when evaluating events in fuzzy theory. This rating scale is also commonly used in evaluating and/or rating criteria in real-life questionnaire and focus group responses. Similarly, in
Table 3, we display the most frequent ratings for the expertise level of each evaluator in the criteria evaluation process.
This work addresses the challenge of selecting the optimal alternative solution for healthcare waste (HCW) treatment by introducing a decision-making technique along with an illustrative use-case solution. HCW and other healthcare professionals, as well as municipal staff members focusing on public safety and regional planning, are considered experts in the field. We are particularly interested in the treatment of HCW, as it has the potential to significantly impact municipality operators, local and regional couriers, small- and medium-sized enterprises (SMEs), and the broader society.
Any produced DSS must facilitate the IFWAA operator of Equation (3) to implement an ensemble of IF methodologies. In this research work, we utilize this operator in conjunction with the IF-TOPSIS and IF-CORPAS methods [
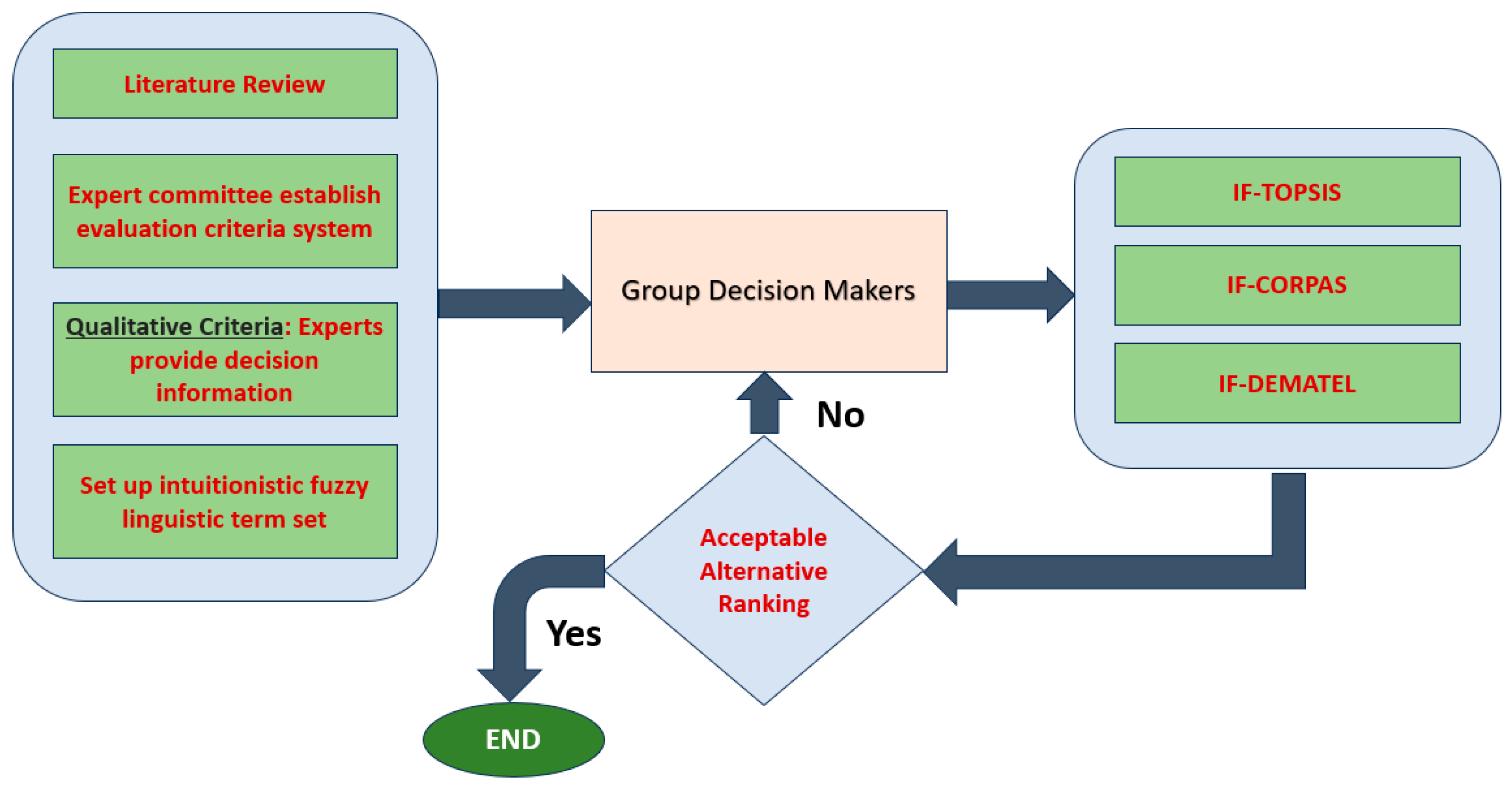
32]. The linguistic terms are converted to IF- numbers. This is predicated on the existence of plausible employment scenarios for HCW. The overall methodology begins with an extensive literature review to identify all the criteria involved in examining and evaluating the best possible solution for HCW treatment. This list of criteria, along with the metrics and performance indicators needed for evaluating the DSS under construction, is finalized through verification by field experts. Simultaneously, we establish an intuitionistic fuzzy linguistic term set for all criteria to obtain expert responses, thus organizing the process of expert evaluation.
Given a set of criteria for evaluation and a set of alternative solutions, the relative importance decision matrix for the criteria ratings is formed. It is important to note that, for each alternative solution and each overall scenario of development, different matrices must be created and computed. Moreover, the model is immune to scalability issues since the number of criteria used for the ranking process does not affect the outcome, thus model resilience is preserved. The selected methodology builds an ensemble DSS holistically using three models for criteria evaluation and ranking. Each model, when run, indicates which alternative solution scenario, out of all the candidates, has the best potential. We first give a detailed explanation of each IF methodology, and then we illustrate the logical architecture of this methodology in
Figure 2.
3.3. The IFTOPSIS Model [33]
Input:
Given a set of experts in the HCW management and treatment technology research, denoted as k, let with be the weights vector of indicating the importance of their opinion. Moreover, let be the set of criteria under the process of evaluation and ranking. For this set, let us also denote this with and
Step 1: Initially the discrete experts linguistically rate the criteria C using the rating scale of
Table 1. Immediately afterwards, we calculate the IF decision matrix
with
to be the corresponding IFN number and
.
Step 2: Based on the results of Step 1, we compute the aggregated IF decision matrix
. This is achieved by calculating the corresponding IFWAA operators. In the computation process of
, we basically compute each matrix element using the two equations below:
where
Step 3: In this step, we compute the ideal solutions denoted as
and
, respectively. Using
(beneficial) and
(non-beneficial). We compute the IF positive ideal solution (IFPIS) and the IF negative ideal solution (IFNIS). respectively (which are denoted as
and
). according to the following equations:
Step 4: Using the values
and
above, we now calculate the distances from the positive and negative ideal solution IFFPIS and IFNIS. respectively. These are calculated in the following equations, respectively, using the notion of the IF normalized Euclidean distance:
Step 5: Using the two equations above, we calculate the closeness coefficient values (CCVs). Note that, for each criterion
, the corresponding CCV, which, from now on, is denoted as
, is found by the following equation:
Step 6: Finally, we compute the criteria weights using the CCV where we presume that the total of the weights is equal to 1. In the opposite case, we repeat the normalization process to achieve the aforementioned summation.
3.4. The IF-COPRAS Model [34]
Input:
The aggregated IF decision matrix calculated in Equation (4) and in step 2 of the IF-TOPSIS model process is as follows
Step 1: We first calculate the weighted normalized values for each matrix cell of
In order to do that, we initially calculate the value
. This is computed either for the normalized case by Equation (10) or for the weighted normalized case by Equation (11) as shown below:
Step 2: Calculate the total weighted normalized value for each expertly recommended alternative in relation to the beneficial (BC) and non-beneficial (NBC) criteria. respectively. The following formulae illustrate this:
for the beneficial criteria and for the non-beneficial criteria.
Step 3: From the aforementioned
and
values, we calculate the relative importance for each expertly recommended alternative solution
. In addition, using the value of
, we then compute the utility degree
as follows:
Step 4: Either the value of or the value of can equally help determine the ranking of the expertly recommended alternative solutions.
3.5. Algorithm Intuitionistic Fuzzy DEMATEL [35]
Step 1: Construct a direct-relation matrix where the entries are based on the obtained linguistic scale data.
Ratings given by k-th experts on the interrelationship between criteria are collected and used to construct a direct-relation matrix where entries are rating scales.
Step 2: Construct a direct-relation matrix where entries are IFNs.
The IFNs defined in
Table 3 are substituted according to their linguistic terms into the direct-relation matrix.
where
is the rating for each one of the experts that participate on the criteria interrelationship evaluation process.
Step 3: Expert weight determination.
According to their level of expertise, the evaluators are assigned specific weights (levels of expertise). This is in accordance with their job experience and knowledge in the field of HCW and medical waste management. The determination of the weight for each expert is given in Equation (15) and it is based on the study of [
33]. More specifically, if
, the rating of the kth expert weight
is:
Step 4: Find the aggregated intuitionistic fuzzy decision matrix.
To construct the aggregated intuitionistic fuzzy decision matrix, the intuitionistic fuzzy weighted average (IFWA) operator is used to fuse the weights of all decision-makers into one evaluation matrix of decision-makers:
Step 5: Transform the aggregated matrix into its numeric equivalent according to [
34]. Then, the crisp values are computed for the total relationship matrix using the following equation:
using the same terminology for the membership and non-membership as in Equation (2a) and in Equation (2b).
Step 6: Construct the normalized direct-relation matrix
X using the crisp matrix
A and the constant
k,
where the equation is as follows:
Step 7: Construct the total-relation matrix T from the following equation:
with
I to be the identity matrix
Step 8: Determine the sum of rows and the sum of columns from the matrix T. The sum of the rows and the sum of the columns (denoted by D and R, respectively) can be calculated by Equations (20) and (21):
Step 9: Find the quantities and , respectively. With the calculation of , we can obtain the Cartesian co-ordinate values with respect to both axes.
Step 10: Draw the causal diagram.
Once the values of and are determined, then the two co-ordinates of each one of the criteria are determined and they can be mapped on the plane. The values of represent the Prominence Vector. Using this vector, we can visualize the importance of the criteria. On the other hand, the values of represent the Relation Vector. Depending on the values of , we can then classify the criteria either in the Cause Group or in the Effect Group if the values of the Relation Vector are positive or negative, respectively.
Step 11: The construction of the network relationship map (NRM) using the threshold is as follows: the threshold value is computed, finding the mean of all cells of the total-relation matrix.
4. Applying the IF-Models of IFTOPSIS, IFCORPAS, and IFDEMATEL for the Thessaly Case Study: Detailed Analysis and Results
Optimizing the use of effective healthcare waste (HCW) treatment methods is crucial for promoting a sustainable and environmentally friendly urban environment. Concurrently, effective HCW management has the potential to generate energy through processes like anaerobic digestion and incineration. This promotes the production of sustainable energy while also helping to reduce waste. Therefore, in order to maximize the benefits of HCW management, competent authorities and regional decision-makers are very interested in choosing the most effective treatment alternative.
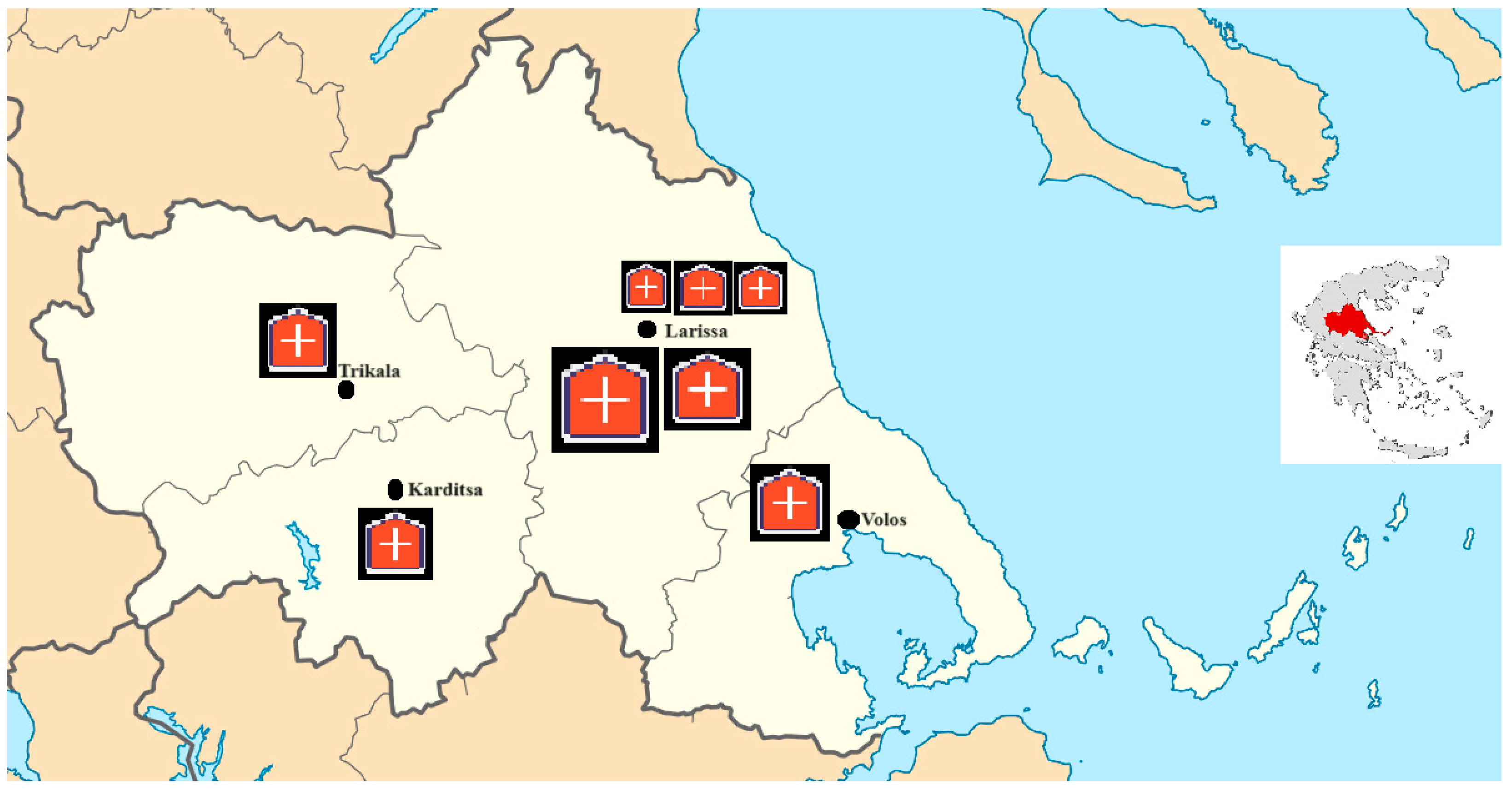
Our research focuses on identifying the best alternative methodologies for HCW treatment based on various related criteria and aspects in the Thessaly region of Greece. Thessaly, one of the thirteen regions of Greece, is located in the central part of the country and is known for its diverse landscapes, including mountains, plains, and coastal areas. Within Thessaly, several cities and towns, including Larissa (the regional capital), Volos, and Trikala, house hospitals and healthcare facilities to serve the local population. Medical or clinical waste produced from these facilities, including needles, syringes, bandages, expired medicines, and other biomedical materials, is predominantly non-hazardous, although the existence of hazardous medical waste remains significant. Proper HCW management is crucial in order to prevent the spread of diseases and protect both healthcare workers and the general public.
The volume of HCW produced is closely related to population density, the number of healthcare facilities, the types of medical services provided, and healthcare practices in the region. As depicted in the thematic map in
Figure 3, Larissa has the greatest concentration of facilities, with three other smaller cities contributing with medium-sized hospital facilities. Healthcare waste management in Thessaly adheres to national regulations and guidelines, outlining proper segregation, collection, treatment, and disposal methods for HCW. Common methods include incineration, autoclaving (sterilization), and, sometimes, landfilling for non-hazardous biomedical waste. Given the importance of environmental sustainability, efforts may also be in place to promote eco-friendly HCW treatment practices, such as waste-to-energy technologies or the recycling of certain medical materials.
The following actions are necessary to address the problem of determining the most practical and effective waste treatment for HCW in a large area with dispersed healthcare facilities, like Thessaly, Greece. The steps involved in this process include: (a) selecting the most relevant impact factors (criteria); (b) involving experts to evaluate and rank the importance of these factors/criteria; (c) selecting the most pertinent treatment alternatives based again on expert opinions and the regional priorities; and (d) compiling the responses from all decision-makers to establish a hierarchy of the criteria and compare the significance of the criteria for each proposed solution.
Various indicators, including environmental and economic costs, sensitivity to the environment, and social aspects, demonstrate that the introduction of organized infrastructures and facilities, along with integrated HCW treatment methodologies, may offer solutions to numerous challenges in hazardous material transportation, management, and treatment. To address the complex problem of choosing the best methodology or creating a comprehensive policy for HCW treatment, multiple IF methodologies can be integrated. As seen in
Table 4, we present 17 criteria grouped into six main categories: environmental, economic, social, organizational, waste-related, and legislation. The selection of the criteria is based on relevant literature, the professional judgment of hospital staff, capable authorities, and experts in the field of hazardous material treatment facilities:
In order to maximize the environmental, economic, and social sustainability of the regional societies, public safety and health, and regional development, we employ the IFTOPSIS, IFCORPAS, and IFDEMATEL IF methodologies in this research to choose the best alternative HCW treatment methodology. Four HCW treatment options are available as stated:
Incineration is a method to treat medical waste, including hazardous materials and sharps. The process involves segregation and collection, receiving and inspection, loading the incinerator, and burning the waste at high temperatures. At the same time, air pollution control devices are used to capture and neutralize harmful emissions. After incineration, the remaining ash is inspected and disposed of in designated landfills or undergoes further treatment if necessary. We denote this alternative solution as ALT1.
HCW Storage is a methodology that includes a series of steps: Initially, HCW is segregated into categories like sharps, infectious waste, pharmaceutical waste, and chemical waste, and placed in designated containers. Containers must be sturdy and leak-proof to prevent leaks. Proper labeling and documentation are essential for proper tracking and disposal. Medical waste is stored on-site in secure areas, with storage times regulated by local, state, and national regulations. Refrigeration is necessary for certain wastes, such as biological samples and certain pharmaceuticals. Healthcare staff are trained in proper protocols, and medical waste is prepared for transportation to treatment facilities. Facilities have emergency response and contingency plans in place to mitigate risks. Regulatory compliance is essential, with regular inspections and adherence to guidelines ensuring healthcare facilities maintain a safe environment for patients and staff. We denote this alternative solution as ALT2.
HCW Recycling is a complex process that converts HCW material into reusable products, reducing the environmental impact and strain on natural resources. It involves the identification and segregation of waste, decontamination to remove harmful substances, and shredded or crushed materials for transportation and processing. Specialized facilities handle processed HCW using advanced technologies. Methods include mechanical recycling, chemical recycling, and energy recovery. Quality control checks ensure materials meet required standards, especially for medical devices or sensitive applications. Regulatory compliance is essential throughout the recycling process to ensure safety and environmental standards are met. However, there are limited methodologies for treating medical waste, particularly for biohazardous materials. We denote this alternative solution as ALT3.
HCW Segregation and Landfilling is a methodology that involves identifying waste types, using color-coded containers, and training healthcare staff on proper segregation. Segregated waste is stored securely in containers, labeled with information about the type, date of generation, and facility name. On-site storage is also used to prevent environmental contamination. Packaging is carried out using double-bagged or leak-proof containers, while manifests document the type and quantity of waste being transported. Landfills are lined with protective liners and monitoring systems to prevent the leaching of hazardous materials. The waste is compacted to reduce volume and minimize environmental impact. Covering is carried out daily to minimize odor and disease transmission. Regulatory compliance ensures the safe management of medical waste and public health. We call this alternative scenario ALT4.
Under the following scenarios, experts assess the alternatives: (a) public safety; (b) environmental safety, efficiency, and pollution prevention; and (c) risk assessment for the use of HCW treatment. It is also important to note that safety cannot be quantified, meaning it cannot be assigned a weight value. Consequently, even with interactive modeling approaches, it is impossible to compare the two scenarios. The categorical phrases that the experts used to compare the 17 criteria in
Table 4 with the rating scale are listed in
Table 5:
4.1. IFTOPSIS Analysis
Expert evaluators
and
responded, evaluating the pertinent criteria. Their findings in terms of criteria importance rates are presented in
Table 3. It is important to emphasize that
are competent authorities’ officials, whilst the other two are hospital-focused personnel in different hospitals of the region. Additionally, we assume that each expert response is equally important, with an importance weight of 0.250.
Table 6 displays the linguistic responses from the expert evaluators
and
according to the criteria importance rates. We must also emphasize that
are competent authorities’ officials and the other two are hospital-focused personnel. Furthermore, we assume a 0.250 importance weight for each expert response, meaning that they are all equally important.
The stated expert criteria evaluations and objectives and the aims of the under-consideration alternatives serve as the primary guides in the selection and formulation of assessment criteria. A hierarchical criteria tree could be created, but, since the weights of the experts’ opinions have equal weight and importance for all respondents, the hierarchical tree may not provide any new information. Furthermore, unlike a multi-criteria analysis, which often uses the results or effects of the activities themselves as assessment criteria, MCDM procedures use the goals and objectives of the experts when these serve as evaluators of criteria. If all pertinent experts/stakeholders are included, these consequences will automatically show in the aims of the experts. Thus, the experts are responsible for providing non-redundant and legibility data.
Equations (4) and (5) of the IF-TOPSIS method drive the calculations.
Table 5 shows the outcomes of this process including the membership, non-membership, and the uncertainty elements. It is imperative to acknowledge that these results align with the initial scenario, which pertains to environmental safety, efficiency, and pollution prevention. Two other sets of tables similar to
Table 6 and
Table 7, respectively, have been produced and they are related to the public safety and the risk evaluation for the use of HCW treatment scenarios. However, due to space limitation reasons, they are not included but can be submitted in the supplementary material. In
Table 8, for each criterion. We indicate whether it is a beneficial or not beneficial (B/NB), the calculated values columns
,
. and
from the aggregated intuitionistic fuzzy decision matrix, and the values
and
, as well as
.
Using the findings from
Table 8, we can compute the IFPIS and IFNIS solutions. Applying the corresponding equations, we find that
and
, respectively. We then calculate the relative assessment matrix. For each matrix cell, there exists a threshold function
in order to recognize and break alternatives of equal distance from the ideal solution. As it has been proposed in [
64], this threshold is allowed to obtain values between 0.01 and 0.05. The ranking of the four alternatives is shown in
Table 9:
The above ranking indicates that the incineration alternative (ALT1) solution is the most preferable, with the ALT4 (segregation and landfill) to follow. The third preferable is ALT3, which refers to HCW recycling, with the ALT2 (HCW storage) being the least preferable.
4.2. IFCORPAS Analysis
The intuitionistic fuzzy decision matrix, which comprises all expert responses for all alternatives and is displayed in
Table 5, is the input used by the approach. We then compute the weighted decision matrix in a way that each cell is the aggregated outcome of all 17 criteria and all four alternative solutions. This is achieved by the use of Equations (10) and (11) in order to obtain the normalized value
. The IFCORPAS algorithm’s first step includes both procedures.
Table 10 displays the acquired results.
We calculate the overall weighted normalized value for Step 2 of the IFCORPAS model in relation to the non-beneficial criteria (NBC) and the beneficial criteria (BC). The last four columns of
Table 10 can be immediately utilized to obtain the results for
and
, respectively. Lastly, using Step 3, we determine each alternative’s relative importance and utility degree, providing us with a ranking of the alternatives.
Table 11 displays the acquired results. There is agreement between the IFTOPSIS rankings as seen in
Section 4.1.
4.3. IF-DEMATEL Analysis
We employed the intuitionistic fuzzy DEMATEL method for capturing the complex relationships among the 17 criteria and the four alternative options for HCW treatment. Incorporating the experts’ responses in terms of the comparative linguistic rating of the 17 criteria, as well as their rating of the criteria within each one of the alternatives
we first calculate the direct-relation matrix where the entries are IFNs. At the next step, we compute the intuitionistic fuzzy decision matrix. The transformation of this matrix into crisp values used the Equation (17) of the IF-DEMATEL methodology.
Table 12 shows the crisp values of the intuitionistic fuzzy transform. In this table, we included Step 8 of the methodology, determining the sum of the rows and the sum of the columns to compute R and D from Equation (20) and Equation (21), respectively. Finally, in
Table 13, we construct the total-relation matrix T.
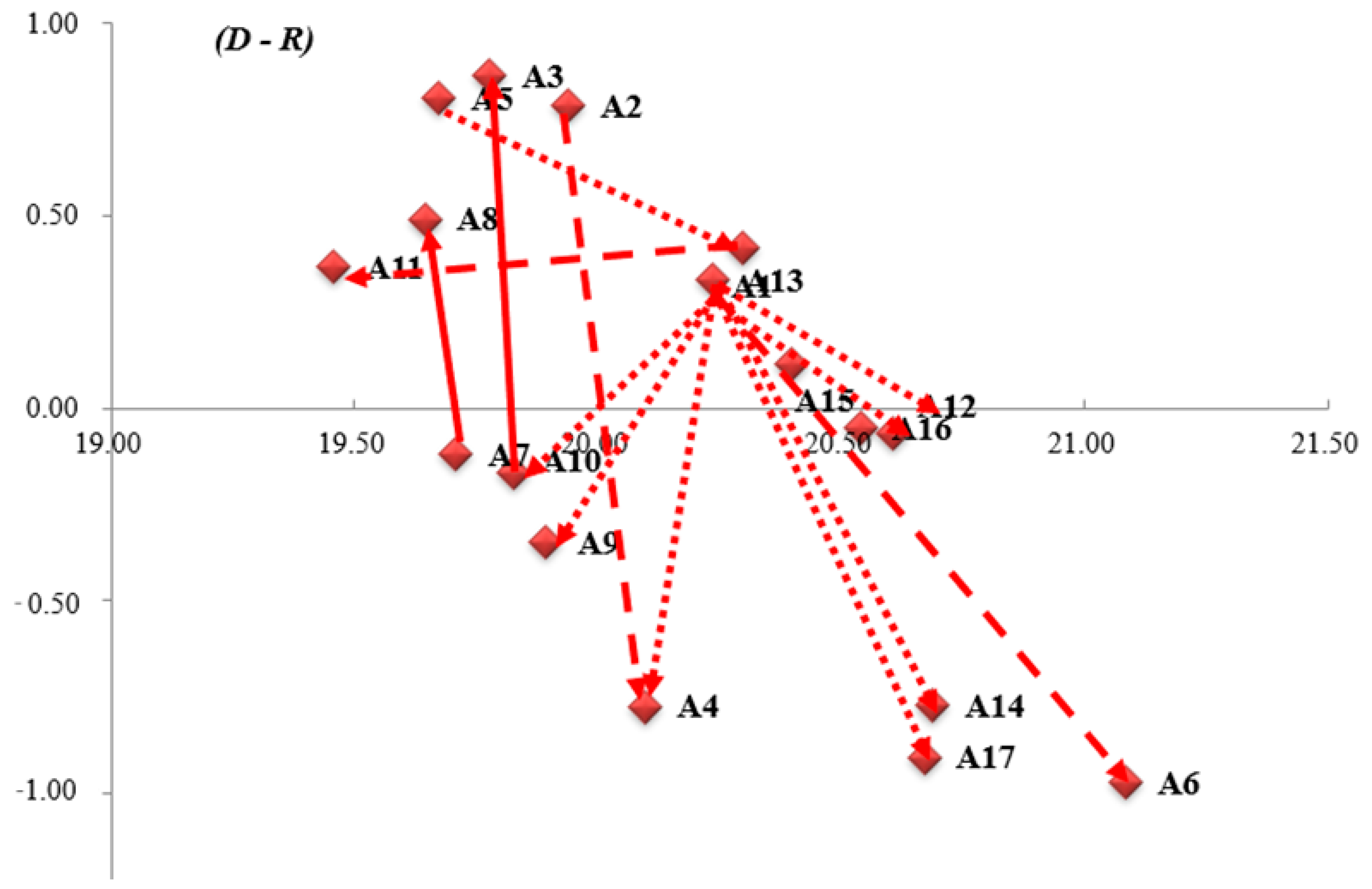
We obtained the cause-and-effect diagram (
Figure 4) by mapping a dataset of
where the horizontal axis
represents the importance of the 17 criteria and
classifies the identified challenges into each of the cause groups as shown in
Table 14.
The ranking of the four alternatives is calculated indirectly from their relative importance in terms of the scenarios. The IF-DEMATEL method is supportive of the ranking process since the ranking of alternatives can be calculated the same way as IF-TOPSIS from the intuitionistic fuzzy decision matrix of the 17 criteria. The ranking of the criteria is shown in
Table 15.
For that reason, the results of IF-DEMATEL are identical to IF-TOPSIS as shown in
Table 16:
5. Discussion of Results
Discussing the qualitative data results, as opposed to the quantitative analysis of
Section 4, we now focus on the chosen models used in the evaluation/ranking process, prioritizing the ranking of the alternatives. For frameworks utilized in the formulation of policies for sustainable urban development, this is always important [
65]. As a result, it is critical to evaluate the framework in its entirety as a tool to assist the policy-maker in supporting their decision. The results show that the three alternatives were ranked identically by all models. When the above methodologies are used on the same dataset, this demonstrates their consistency. However, if all the participating models yield the same outcome, then this fact invites the question of whether the comparative analysis is necessary for the study. To make such an argument, one must, however, further demonstrate that every issue is incorporated in this framework, which is not obviously the case. On the contrary, there are many other aspects, criteria, and parameters which have not been included in the study because they have not indicated critical significance relative to the 17 already-taken criteria. But the factor of the direct relevance of these criteria with the region of study is the one that justifies the existence of alternative methodologies working on the same aspect to produce justifiable results. We collected all data pertaining to the ranking outcomes of IF-TOPSIS, IF-CORPAS, and IF-DEMATEL, respectively, from the relative tables. More specifically, the exact relevance weights that each approach allocated to each of the different alternatives are of greater interest to us. Only IF-CORPAS gives normalized significance weights among the methodologies used. The other approaches have been normalized by us so that their performance is consistent across the board. The outcomes are displayed in
Table 17:
Incineration is ranked as the most preferable solution due to its ability to safely dispose of a wide range of medical waste types. When operated correctly, modern incinerators can efficiently burn medical waste at high temperatures, minimizing the risk of contamination and emissions. The method is considered effective for medical waste disposal because it reduces the volume of waste significantly and can destroy pathogens and harmful chemicals.
On the other hand, the storing of HCW is ranked as the least preferable alternative. This is justified by the fact that storing HCW for prolonged periods can lead to the risk of contamination, environmental pollution, and potential health hazards for workers and nearby communities. At the same time, the method does not address the disposal issue, and the waste may pose increased risks over time.
Segregation and landfill is the second most preferable alternative for the case of the Thessaly region. Experts indicated that segregating medical waste before landfilling can help reduce the volume of hazardous waste going into landfills, making it easier to manage. Properly engineered landfills can contain medical waste and prevent environmental contamination if managed effectively. On the other hand, there is still a great hazard imposed due to possible soil contamination because of the landfills.
Finally, recycling was ranked as the third important alternative HCW treatment for Thessaly. Experts indicated that recycling certain types of medical waste, such as plastics and glass, can reduce the demand for new raw materials and lower the environmental impact. However, recycling HCW is also challenging due to the risk of contamination. Not all medical waste materials are suitable for recycling, especially those contaminated with biohazardous materials. Therefore, while it is environmentally friendly, it is limited in scope due to the specific nature of medical waste. Recycling can be a part of the waste management process but cannot be the sole solution due to its limitations in handling all types of medical waste.
6. Conclusions
Rapid global urbanization and population growth have presented municipalities with a significant challenge in managing healthcare waste (HCW), attracting increased attention in recent years. Selecting the appropriate HCW treatment technology is a complex task, involving conflicting criteria and multiple social stakeholders. HCW management systems often grapple with imprecise parameters expressed through uncertain linguistic expressions. The use of fuzzy membership functions in decision making can sometimes result in the loss of valuable information.
In this study, we introduced a comprehensive decision-making framework to facilitate optimal HCW treatment technology selection, considering various stakeholders’ perspectives and employing a range of fuzzy intuitionistic methodologies, including IF-TOPSIS, IF-CORPAS, and IF-DEMATEL. We utilized an ensemble of these models to handle the linguistic assessments of experts in the field, focusing on the use case of the Thessaly region, Greece. Our approach objectively calculates decision-makers’ weights, addressing their uncertainty and divergence levels. We demonstrated our methodology through a practical case study and conducted a comparative analysis to validate its effectiveness. The study showed that our decision-making approach effectively resolves HCW disposal technology selection problems in uncertain and complex environments, thereby strengthening public health. We used the aforementioned three methods to identify the best alternative HCW treatment methods for environmental, economic, and social sustainability. Four options are identified: incineration, storage, recycling, and segregation and landfilling. We also assumed that regulatory compliance ensures the safe management of medical waste and public health. By employing distances from the ideal solution, two techniques—IF-TOPSIS and IF-CORPAS—basically distinguish criteria and alternative solutions, respectively. Distance is the basis of the IF-DEMATEL model. Every model managed to generate an identical rating amongst the alternatives, regardless of the model’s core. For the incineration alternative which was the most preferred by all IF-methodologies, IF-TOPSIS presents the highest critical significance of ~0.30, with IF-CORPAS in second place with ~0.28, and IF-DEMATEL in third place, computing ~0.26 out of the whole critical importance vector. The second-best ranking alternative is HCW segregation and landfilling. Even though, in other studies, this alternative is not popular, the Greek study showed an augmented preference. However, the most popular choice was the incineration of HCW because it can securely dispose of various kinds of medical waste. Modern incinerators can effectively burn medical waste at high temperatures while limiting the danger of contamination and pollution when used properly. The safety criterion was intended to be non-negotiable across all participants, avoiding competition with other options. We must mention that our study compares the most dominant technologies for HCW treatment in a holistic way (multiple categories of criteria have been used). Even though the results could support the medical waste hierarchy, we strongly believe that life-cycle assessment is a crucial tool in waste management practice, but little research has been performed on the evaluation of medical waste treatment from a life-cycle perspective.
Future research will focus on expanding this integrated approach to address HCW management issues involving diverse interrelationships among evaluation criteria. Moreover, methods for objectively determining criteria weights should be developed, especially in real-world situations where subjective estimation is challenging. Another avenue for future research involves creating a computer-based application system to streamline the implementation of our proposed HCW treatment technology selection algorithm and enhance human–machine interaction for presenting and analyzing selection results. This framework can be made more flexible by adding more models for more comprehensive evaluation procedures. Furthermore, further research is needed to examine the characteristics of ensemble-based systems in scenarios with inconsistent ranking outcomes. Inter-val-valued, Pythagorean, or interval type-2 fuzzy sets can also be added to a more complete framework to improve the current approach and guarantee public health.



 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}