Celiac Male’s Gluten-Free Diet Profile: Comparison to that of the Control Population and Celiac Women

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Anthropometric Measurements
2.3. Body Composition and Energy Expenditure
2.4. Dietary Assessment
2.5. Statistical Analysis
3. Results
3.1. Anthropometric Measurements
3.2. Dietary Intakes
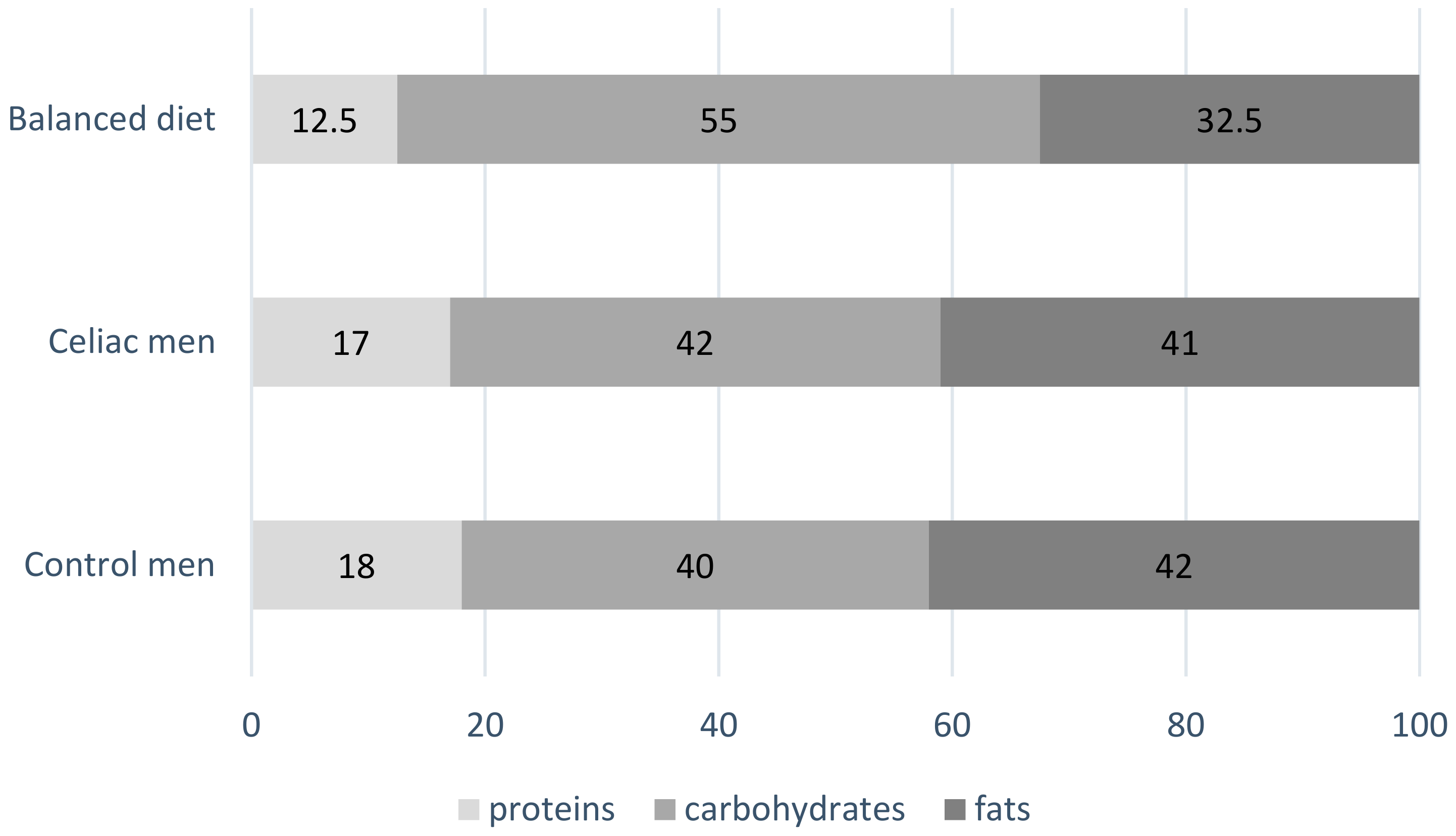
3.2.1. Energy, Macronutrients, Fiber and Cholesterol Intake in Celiac Men
3.2.2. Micronutrients Intake in Celiac Men
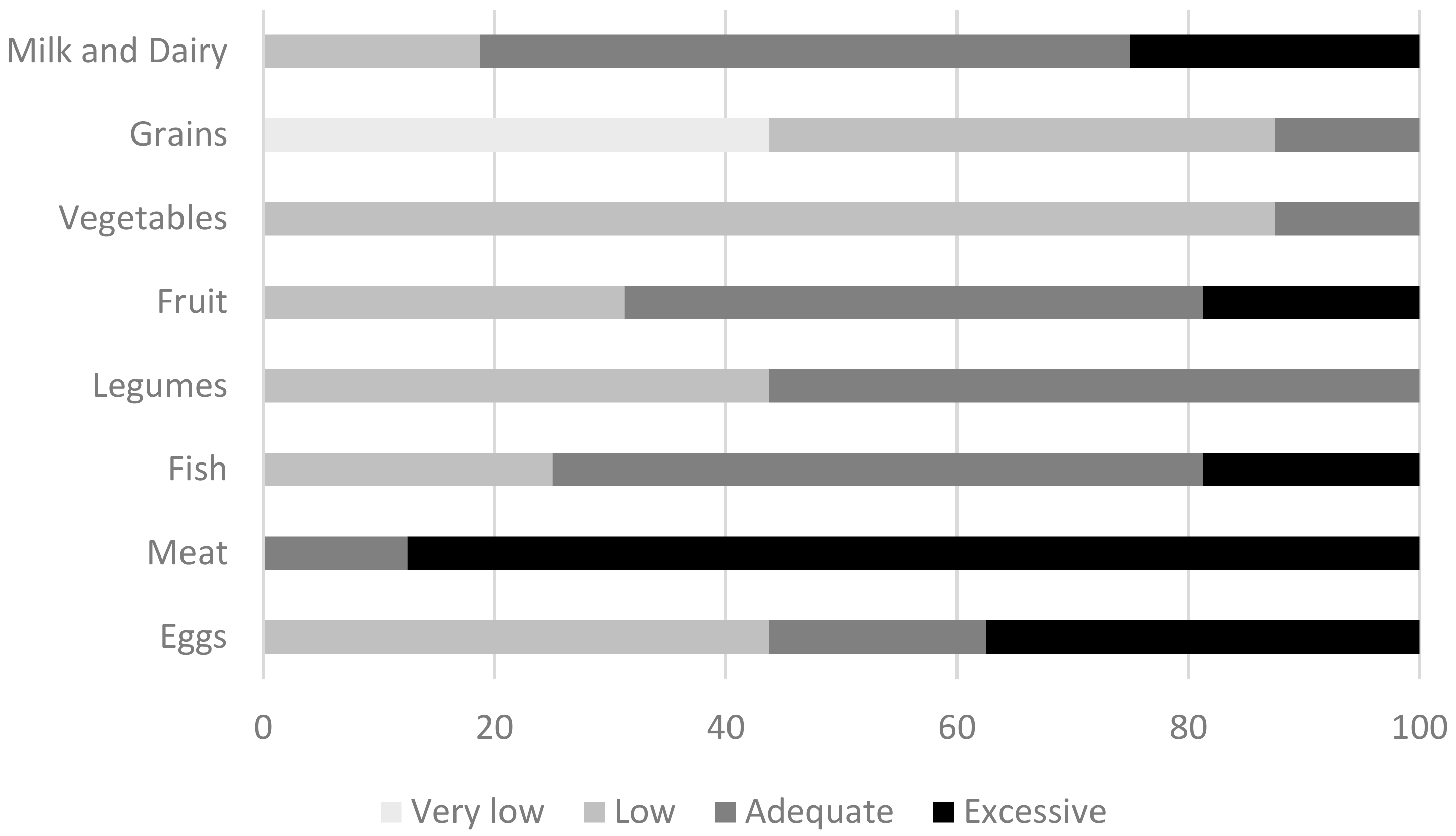
3.3. Food Consumption Frequency of Celiac Men
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Lionetti, E.; Catassi, C. New clues in celiac disease epidemiology, pathogenesis, clinical manifestations, and treatment. Int. Rev. Immunol. 2011, 30, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Peña, A.; Rodrigo, L. Epidemiology of celiac disease and non-celiac gluten-related disorders. In Advances in the Understanding of Gluten Related Pathology and the Evolution of Gluten-Free Foods; Arranz, E., Fernández-Bañares, F., Rosell, C., Rodrigo, L., Peña, A., Eds.; OmniaScience: Barcelona, Spain, 2015; pp. 27–73. [Google Scholar]
- Catassi, C.; Gatti, S.; Fasano, A. The new epidemiology of celiac disease. J. Pediatr. Gastroenterol. Nutr. 2014, 59 (Suppl. 1) (Suppl. 1), S7–S9. [Google Scholar] [CrossRef]
- Sharp, P.; Bottorff, J.L.; Hunt, K.; Oliffe, J.L.; Johnson, S.T.; Dudley, L.; Caperchione, C.M. Men’s Perspectives of a Gender-Sensitized Health Promotion Program Targeting Healthy Eating, Active Living, and Social Connectedness. Am. J. Men’s Health 2018, 2157–2166. [Google Scholar] [CrossRef] [PubMed]
- Galdas, P.M.; Cheater, F.; Marshall, P. Men and health help-seeking behaviour: Literature review. J. Adv. Nurs. 2005, 49, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Churruca, I.; Miranda, J.; Lasa, A.; Bustamante, M.; Larretxi, I.; Simon, E. Analysis of Body Composition and Food Habits of Spanish Celiac Women. Nutrients 2015, 7, 5515–5531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardella, M.T.; Fredella, C.; Prampolini, L.; Molteni, N.; Giunta, A.M.; Bianchi, P.A. Body composition and dietary intakes in adult celiac disease patients consuming a strict gluten-free diet. Am. J. Clin. Nutr. 2000, 72, 937–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, J.; Geisel, T.; Maresch, C.; Krieger, K.; Stein, J. Inadequate nutrient intake in patients with celiac disease: Results from a german dietary survey. Digestion 2013, 87, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Capristo, E.; Malandrino, N.; Farnetti, S.; Mingrone, G.; Leggio, L.; Addolorato, G.; Gasbarrini, G. Increased serum high-density lipoprotein-cholesterol concentration in celiac disease after gluten-free diet treatment correlates with body fat stores. J. Clin. Gastroenterol. 2009, 43, 946–949. [Google Scholar] [CrossRef] [PubMed]
- Vici, G.; Belli, L.; Biondi, M.; Polzonetti, V. Gluten free diet and nutrient deficiencies: A review. Clin. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Theethira, T.G.; Dennis, M. Celiac disease and the gluten-free diet: Consequences and recommendations for improvement. Dig. Dis. 2015, 33, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.M.; Kesse-Guyot, E.; McManus, R.; Hercberg, S.; Lairon, D.; Planells, R.; Roche, H.M. High dietary saturated fat intake accentuates obesity risk associated with the fat mass and obesity-associated gene in adults. J. Nutr. 2012, 142, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.L. Dietary fiber and body weight. Nutrition 2005, 21, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Capristo, E.; Mingrone, G.; Addolorato, G.; Greco, A.V.; Corazza, G.R.; Gasbarrini, G. Differences in metabolic variables between adult coeliac patients at diagnosis and patients on a gluten-free diet. Scand. J. Gastroenterol. 1997, 32, 1222–1229. [Google Scholar] [CrossRef] [PubMed]
- Capristo, E.; Addolorato, G.; Mingrone, G.; De Gaetano, A.; Greco, A.V.; Tataranni, P.A.; Gasbarrini, G. Changes in body composition, substrate oxidation, and resting metabolic rate in adult celiac disease patients after a 1-y gluten-free diet treatment. Am. J. Clin. Nutr. 2000, 72, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Russolillo, G.; Marques, I. Food Portion Sizes Album; Imagen Comunicación Multimedia: Madrid, Spain, 2008; 186p. [Google Scholar]
- FESNAD. Dietary reference intakes (DRI) for spanish population, 2010. Actividad Dietética 2010, 14, 196–197. [Google Scholar] [CrossRef]
- Aranceta, J.; Serra-Majem, L. Dietary guidelines for the Spanish population. Public Health Nutr. 2001, 4, 1403–1408. [Google Scholar] [CrossRef] [PubMed]
- AECOSAN, Agencia Española de Consumo, Seguridad Alimentaria y Nutrición. Spanish Population Dietary Intakes. National Health Survey (ENIDE). Available online: http://aesan.msssi.gob.es/AESAN/docs/docs/evaluacion_riesgos/estudios_evaluacion_nutricional/valoracion_nutricional_enide_macronutrientes.pdf (accessed on 8 June 2017).
- SENC. Nutritional objectives for the Spanish population: Consensus from the Spanish Society of Community Nutrition. Rev. Esp. Nutr. Com. 2011, 17, 178–199. [Google Scholar]
- Marshall, T.A.; Stumbo, P.J.; Warren, J.J.; Xie, X.J. Inadequate nutrient intakes are common and are associated with low diet variety in rural, community-dwelling elderly. J. Nutr. 2001, 131, 2192–2196. [Google Scholar] [CrossRef] [PubMed]
- Roman-Vinas, B.; Ribas Barba, L.; Ngo, J.; Martinez-Gonzalez, M.A.; Wijnhoven, T.M.; Serra-Majem, L. Validity of dietary patterns to assess nutrient intake adequacy. Br. J. Nutr. 2009, 101 (Suppl. 2), S12–S20. [Google Scholar] [CrossRef]
- Arganini, C.; Saba, A.; Comitato, R.; Virgili, F.; Turrini, A. Gender Differences in Food Choice and Dietary Intake in Modern Western Societies. In Public Health-Social and Behavioral Health; Maddock, J., Ed.; InTech: Hampshire, UK, 2012; ISBN 978-953-51-0620-3. Available online: http://www.intechopen.com/books/public-health-social-and-behavioral-health/gender-differences-in-foodchoice-and-dietary-intake-in-modern-western-societies (accessed on 15 October 2018).[Green Version]
- Rippin, H.L.; Hutchinson, J.; Jewell, J.; Breda, J.J.; Cade, J.E. Adult Nutrient Intakes from Current National Dietary Surveys of European Populations. Nutrients 2017, 9, 1288. [Google Scholar] [CrossRef] [PubMed]
- Valletta, E.; Fornaro, M.; Cipolli, M.; Conte, S.; Bissolo, F.; Danchielli, C. Celiac disease and obesity: Need for nutritional follow-up after diagnosis. Eur. J. Clin. Nutr. 2010, 64, 1371–1372. [Google Scholar] [CrossRef] [PubMed]
- Aranceta Bartrina, J.; Pérez Rodrigo, C. Inequality, health and nutrition in Spain: A regional view of the body mass index. Nutr. Hosp. 2018, 35, 142–149. [Google Scholar] [PubMed]
- López-Sobaler, A.M.; Aparicio, A.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Serra-Majem, L.; Varela-Moreiras, G.; Ortega, R.M. Overweight and General and Abdominal Obesity in a Representative Sample of Spanish Adults: Findings from the ANIBES Study. Biomed. Res. Int. 2016, 2016, 8341487. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Robins, G.G.; Burley, V.J.; Howdle, P.D. Evidence of high sugar intake, and low fibre and mineral intake, in the gluten-free diet. Aliment. Pharmacol. Ther. 2010, 32, 573–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shepherd, S.J.; Gibson, P.R. Nutritional inadequacies of the gluten-free diet in both recently-diagnosed and long-term patients with coeliac disease. J. Hum. Nutr. Diet. 2013, 26, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, P.; Picca, M.; Dilillo, D.; Meneghin, F.; Cravidi, C.; Tischer, M.C.; Vivaldo, T.; Bedogni, G.; Zuccotti, G.V. Changes of body mass index in celiac children on a gluten-free diet. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Larretxi, I.; Simon, E.; Benjumea, L.; Miranda, J.; Bustamante, M.A.; Lasa, A.; Eizaguirre, F.J.; Churruca, I. Gluten-free-rendered products contribute to imbalanced diets in children and adolescents with celiac disease. Eur. J. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Peralta, M.; Ramos, M.; Lipert, A.; Martins, J.; Marques, A. Prevalence and trends of overweight and obesity in older adults from 10 European countries from 2005 to 2013. Scand. J. Public Health 2018, 46, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, E.; López-Plaza, B.; López-Sobaler, A.M.; Ortega, R.M. Overweight and obesity among Spanish adults. Nutr. Hosp. 2011, 26, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Fisac, J.L.; Banegas Banegas, J.R.; Artalejo, F.R.; Regidor, E. Increasing prevalence of overweight and obesity among Spanish adults, 1987–1997. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1677–1682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, E.; Rostami, K.; Prabhakaran, S.; Al Dulaimi, D. Patients with coeliac disease are increasingly overweight or obese on presentation. J. Gastrointest. Liver Dis. 2012, 21, 11–15. [Google Scholar]
- Hallert, C.; Grant, C.; Grehn, S.; Grännö, C.; Hultén, S.; Midhagen, G.; Ström, M.; Svensson, H.; Valdimarsson, T. Evidence of poor vitamin status in coeliac patients on a gluten-free diet for 10 years. Aliment. Pharmacol. Ther. 2002, 16, 1333–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Batlle, J.; Gracia-Lavedan, E.; Romaguera, D.; Mendez, M.; Castaño-Vinyals, G.; Martín, V.; Aragonés, N.; Gómez-Acebo, I.; Olmedo-Requena, R.; Jimenez-Moleon, J.J.; et al. Meat intake, cooking methods and doneness and risk of colorectal tumours in the Spanish multicase-control study (MCC-Spain). Eur. J. Nutr. 2018, 57, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Emilsson, L.; Lebwohl, B.; Sundström, J.; Ludvigsson, J.F. Cardiovascular disease in patients with coeliac disease: A systematic review and meta-analysis. Dig. Liver Dis. 2015, 47, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Ciaccio, E.J.; Lewis, S.K.; Biviano, A.B.; Iyer, V.; Garan, H.; Green, P.H. Cardiovascular involvement in celiac disease. World J. Cardiol. 2017, 9, 652–666. [Google Scholar] [CrossRef] [PubMed]
- Lucendo, A.J.; García-Manzanares, A. Bone mineral density in adult coeliac disease: An updated review. Rev. Esp. Enferm. Dig. 2013, 105, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Nijhawan, S.; Katiyar, P.; Nagaich, N.; Saradava, V.; Nijhawan, M.; Gupta, G.; Mathur, A.; Sharma, R.; Nepalia, S. Prevalence of associated disorders in Indian patients with celiac disease. Indian J. Gastroenterol. 2013, 32, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Whitton, C.; Nicholson, S.K.; Roberts, C.; Prynne, C.J.; Pot, G.K.; Olson, A.; Fitt, E.; Cole, D.; Teucher, B.; Bates, B.; et al. National Diet and Nutrition Survey: UK food consumption and nutrient intakes from the first year of the rolling programme and comparisons with previous surveys. Br. J. Nutr. 2011, 106, 1899–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Størsrud, S.; Hulthén, L.R.; Lenner, R.A. Beneficial effects of oats in the gluten-free diet of adults with special reference to nutrient status, symptoms and subjective experiences. Br. J. Nutr. 2003, 90, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, T. Thiamin, riboflavin, and niacin contents of the gluten-free diet: Is there cause for concern? J. Am. Diet. Assoc. 1999, 99, 858–862. [Google Scholar] [CrossRef]
- Penagini, F.; Dilillo, D.; Meneghin, F.; Mameli, C.; Fabiano, V.; Zuccotti, G.V. Gluten-free diet in children: An approach to a nutritionally adequate and balanced diet. Nutrients 2013, 5, 4553–4565. [Google Scholar] [CrossRef] [PubMed]
- Cornicelli, M.; Saba, M.; Machello, N.; Silano, M.; Neuhold, S. Nutritional composition of gluten-free food versus regular food sold in the Italian market. Dig. Liver Dis. 2018. [Google Scholar] [CrossRef] [PubMed]
- Kulai, T.; Rashid, M. Assessment of Nutritional Adequacy of Packaged Gluten-free Food Products. Can. J. Diet. Pract Res. 2014, 75, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.R.; Ng, D.L.; Dave, E.; Ciaccio, E.J.; Green, P.H. The effect of substituting alternative grains in the diet on the nutritional profile of the gluten-free diet. J. Hum. Nutr. Diet. 2009, 22, 359–363. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Men |
|---|---|
| N | 42 |
| Age (year) | 31.5 ± 11.9 |
| Mean duration of GFD (year) | 20.9 ± 11.9 |
| Height (cm) | 176.2 ± 6.2 |
| Weight (kg) | 75.8 ± 13.9 |
| Fat mass (%) | 24.1 ± 8.1 |
| Body-Mass Index | |
| Mean (kg/m2) | 24.7 ± 4.1 |
| Underweight < 18.5—no. (%) | 4.8 |
| Normal 18.5–24.9—no. (%) | 57.1 |
| Overweight 25–29.9—no. (%) | 26.2 |
| Obese > 30—no. (%) | 11.9 |
| Characteristic | Celiac Men (n = 42) | Spanish Men (ENIDE Study) (n = 1589) | p Value | Sheperd 2013 (11 Men) | Martin 2013 (18 Men) | Wild 2010 (31 Men) |
|---|---|---|---|---|---|---|
| Energy (kcal) | 2355.4 ± 659.0 | 2546.8 ± 860.9 | NS | 2697 ± 445 | 2401 ± 592 | 2500 ± 717 |
| Protein (g) | 100.2 ± 30.1 | 109.4 ± 47.7 | NS | 98.8 ± 22.83 | 92.4 ± 17.5 | 92.7 ± 24.9 |
| Carbohydrate (g) | 220.7 ± 84.7 | 242.7 ± 101.8 | NS | 294 ± 72.3 | 267 ± 95 | 315.6 ± 98.5 |
| Fat (g) | 114.0 ± 32.2 | 114.9 ± 46.0 | NS | 67.9 ± 50.58 | 97.4 ± 29.7 | 93.2 ± 36.6 |
| MUFA (g) | 52.4 ± 16.1 | 48.29 ± 22.2 | NS | - | - | - |
| PUFA (g) | 13.2 ± 5.8 | 15.5 ± 8.5 | <0.05 | - | - | - |
| SFA (g) | 34.5 ± 11.2 | 32.71 ± 15.55 | NS | 34.7 ± 7.7 | - | - |
| (PUFA + MUFA)/SFA | 1.93 | 1.95 | - | - | - | - |
| PUFA/SFA | 0.38 | 0.47 | - | - | - | - |
| Cholesterol (mg) | 421.2 ± 132.8 | 423.82 ± 181.25 | NS | - | - | - |
| Fiber (g) | 20.3 ± 7.1 | 20.94 ± 11.38 | NS | 30.2 ± 7.7 | 22.3 ± 6.0 | 13.7 ± 5.3 |
| Recommended Intake * | Celiac Men | Celiac Women | p Value | |||||
|---|---|---|---|---|---|---|---|---|
| [6] | ||||||||
| Low | Adequate | Excessive | Low | Adequate | Excessive | |||
| Energy intake | ±20% of EE | 40 | 46 | 14 | 30 | 65 | 6 | <0.001 |
| Protein | 10–15% | 0 | 19 | 81 | 0 | 20 | 81 | NS |
| Carbohydrate | 50–60% | 98 | 2 | 0 | 91 | 9 | 0 | NS |
| Total Fat | 30–35% | 0 | 5 | 95 | 4 | 11 | 85 | NS |
| SFA | <10% | 0 | 17 | 83 | 0 | 33 | 67 | <0.05 |
| MUFA | 15–20% | 14 | 31 | 55 | 31 | 37 | 28 | NS |
| Celiac Men (n = 42) | Control Men (ENIDE Study) (n = 1589) | DRI: FESNAD (2010) | p | |
|---|---|---|---|---|
| Celiac Men vs. Spanish Men (ENIDE Study) | ||||
| Vitamin A (ug) | 802 ± 340 | 748 ± 338 | 700 a | NS |
| Thiamin (mg) | 2.0 ± 1.4 | 2.1 ± 6.7 | 1.2 b | NS |
| Riboflavin (mg) | 2.2 ± 1.1 | 1.5 ± 0.8 | 1.6 | <0.001 |
| Vitamin B6 (mg) | 2.7 ± 0.9 | 2.0 ± 0.9 | 1.5 c | <0.001 |
| Vitamin B12 (ug) | 8.1 ± 5.6 | 7.9 ± 6.1 | 2 | NS |
| Vitamin C (mg) | 143 ± 82 | 131 ± 81 | 60 d | NS |
| Vitamin D (ug) | 4.4 ± 4.5 | 4.3 ± 4.5 | 5 e | NS |
| Vitamin E (mg) | 10.8 ± 5.1 | 14.9 ± 8.4 | 15 | <0.001 |
| Niacin (mg) | 38.5 ± 13.6 | 45.7 ± 39.5 | 18 f | <0.01 |
| Folate (ug) | 302 ± 115 | 296 ± 121 | 300 | NS |
| Calcium (mg) | 939 ± 295 | 886 ± 345 | 900 g | NS |
| Iron (mg) | 16.5 ± 5.1 | 16.1 ± 6.5 | 9 h | NS |
| Magnesium (mg) | 323 ± 107 | 396 ± 139 | 350 | <0.001 |
| Iodine (ug) | 117 ± 88 | 100 ± 50.5 | 150 | NS |
| Phosphorus (mg) | 1580 ± 442 | 1535 ± 471 | 700 i | NS |
| Zinc (mg) | 12 ± 4.0 | 10.5 ± 3.7 | 9.5 j | <0.01 |
| Potassium (mg) | 3481 ± 980 | 3045 ± 917 | 3100 | <0.01 |
| Selenium (ug) | 93.8 ± 53.5 | 63.5 ± 35.1 | 55 | <0.001 |
| Celiac Men | Celiac Women | p Value | |
|---|---|---|---|
| [6] | |||
| % of Participants that Fulfilled at Least 67% of Recommendations | % of Participants that Fulfilled at Least 67% of Recommendations | ||
| Vitamin A (ug) | 81 | 89 | NS |
| Thiamin (mg) | 98 | 100 | NS |
| Riboflavin (mg) | 98 | 98 | NS |
| Vitamin B6 (mg) | 100 | 100 | NS |
| Vitamin B12 (ug) | 100 | 100 | NS |
| Vitamin C (mg) | 93 | 96 | NS |
| Vitamin D (ug) | 45 | 52 | NS |
| Vitamin E (mg) | 48 | 61 | NS |
| Niacin (mg) | 100 | 100 | NS |
| Folate (ug) | 76 | 82 | NS |
| Calcium (mg) | 86 | 87 | NS |
| Iron (mg) | 100 | 69 | <0.001 |
| Magnesium (mg) | 71 | 91 | <0.05 |
| Iodine (ug) | 50 | 20 | <0.01 |
| Phosphorus (mg) | 100 | 100 | NS |
| Zinc (mg) | 91 | 98 | 0.093 |
| Potassium (mg) | 98 | 85 | <0.05 |
| Selenium (ug) | 93 | 69 | <0.01 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
González, T.; Larretxi, I.; Vitoria, J.C.; Castaño, L.; Simón, E.; Churruca, I.; Navarro, V.; Lasa, A. Celiac Male’s Gluten-Free Diet Profile: Comparison to that of the Control Population and Celiac Women. Nutrients 2018, 10, 1713. https://doi.org/10.3390/nu10111713
González T, Larretxi I, Vitoria JC, Castaño L, Simón E, Churruca I, Navarro V, Lasa A. Celiac Male’s Gluten-Free Diet Profile: Comparison to that of the Control Population and Celiac Women. Nutrients. 2018; 10(11):1713. https://doi.org/10.3390/nu10111713
Chicago/Turabian StyleGonzález, Teba, Idoia Larretxi, Juan Carlos Vitoria, Luis Castaño, Edurne Simón, Itziar Churruca, Virginia Navarro, and Arrate Lasa. 2018. "Celiac Male’s Gluten-Free Diet Profile: Comparison to that of the Control Population and Celiac Women" Nutrients 10, no. 11: 1713. https://doi.org/10.3390/nu10111713
APA StyleGonzález, T., Larretxi, I., Vitoria, J. C., Castaño, L., Simón, E., Churruca, I., Navarro, V., & Lasa, A. (2018). Celiac Male’s Gluten-Free Diet Profile: Comparison to that of the Control Population and Celiac Women. Nutrients, 10(11), 1713. https://doi.org/10.3390/nu10111713