Low Adherence to the Mediterranean Diet in Isolated Adolescents: The Mediation Effects of Stress

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Measures
2.2.1. Dietary Patterns and Adherence to the Mediterranean Diet
2.2.2. Perceived Loneliness
2.2.3. Stress Perception
2.3. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Relationship Between Loneliness and Stress with Dietary Patterns and Adherence to the MD
3.3. Differences Between Adolescents Depending on the Frequency of Perceived Loneliness in Dietary Patterns and Adherence to the MD
3.4. Prediction Ability of Loneliness and Stress on Adherence to the MD
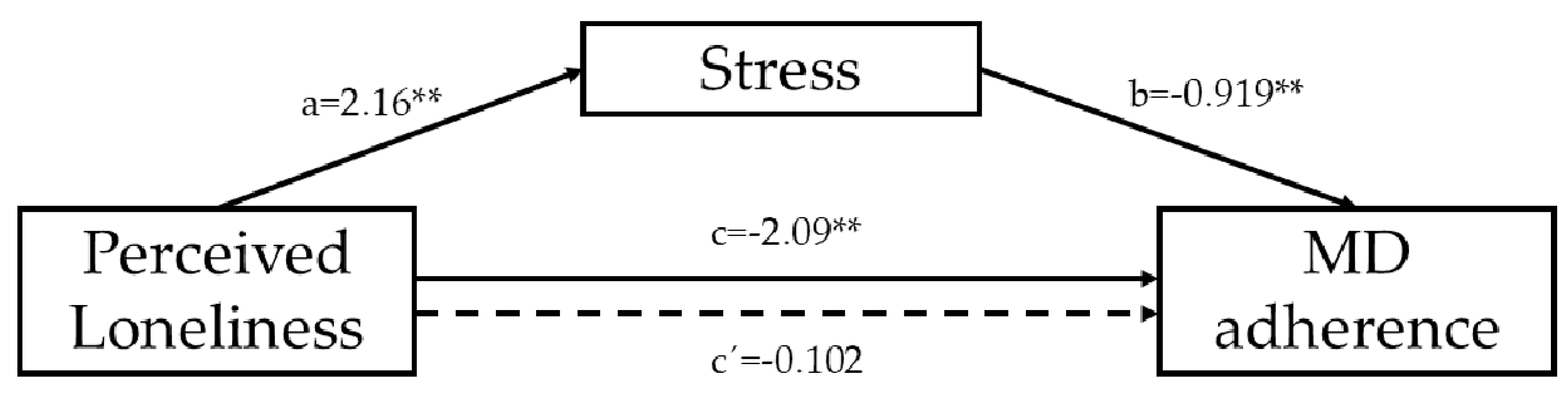
3.5. Mediation Effect of Stress on the Association Between Perceived Loneliness and Adherence to MD
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Castro-Quezada, I.; Román-Viñas, B.; Serra-Majem, L. The Mediterranean diet and nutritional adequacy: A review. Nutrients 2014, 6, 231–248. [Google Scholar] [CrossRef] [PubMed]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet foundation expert group. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed]
- Zaragoza-Martí, A.; Cabañero-Martínez, M.J.; Hurtado-Sánchez, J.A.; Laguna-Pérez, A.; Ferrer-Cascales, R. Evaluation of Mediterranean diet adherence scores: A systematic review. BMJ open 2018, 8, e019033. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N.; Stern, Y.; Tang, M.X.; Mayeux, R.; Ja, L. Mediterranean diet and risk for Alzheimer’s disease. Ann. Neurol. 2006, 59, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Costarelli, V.; Koretsi, E.; Georgitsogianni, E. Health-related quality of life of Greek adolescents: The role of the Mediterranean diet. Qual. Life Res. 2013, 22, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Adelantado-Renau, M.; Beltran-Valls, M.R.; Esteban-Cornejo, I.; Martínez-Vizcaíno, V.; Santaliestra-Pasías, A.M.; Moliner-Urdiales, D. The influence of adherence to the Mediterranean diet on academic performance is mediated by sleep quality in adolescents. Acta Paediatr. 2018. [Google Scholar] [CrossRef]
- Idelson, P.I.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in children and adolescents: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef]
- Albaladejo-Blázquez, N.; Ferrer-Cascales, R.; Ruiz-Robledillo, N.; Sánchez-Sansegundo, M.; Clement-Carbonell, V.; Zaragoza-Martí, A. Poor dietary habits in bullied adolescents: The moderating effects of diet on depression. Int. J. Environ. Res. Public. Health. 2018, 15, 1569. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Sergentanis, T.N.; Panagiotakos, D.B.; Sergentanis, I.N.; Kosti, R.; Scarmeas, N. Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann. Neurol. 2013, 74, 580–591. [Google Scholar] [CrossRef]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef]
- La Vecchia, C. Association between Mediterranean dietary patterns and cancer risk: Review. Nutr. Rev. 2009, 67, S126–S129. [Google Scholar] [CrossRef] [PubMed]
- Clement-Carbonell, V.; Ferrer-Cascales, R.; Zaragoza-Martí, A.; Ruiz-Robledillo, N.; Fernández-Alcántara, M.; Cabañero-Martínez, M.J. Effects of lifestyles and the Mediterranean diet on elderly people’s quality of life according to gender. Stud. Psychol. 2018, 1–23. [Google Scholar]
- Feart, C.; Samieri, C.; Rondeau, V.; Amieva, H.; Portet, F.; Dartigues, J.F.; Scarmeas, N.; Barberger-Gateau, P. Adherence to a Mediterranean diet, cognitive decline, and risk of dementia. JAMA 2009, 302, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Knoops, K.T.; De Groot, L.C.; Kromhout, D.; Perrin, A.E.; Moreiras-Varela, O.; Menotti, A.; Van Staveren, W.A. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA 2004, 292, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Vasilopoulou, E. Mediterranean diet and longevity. Br. J. Nutr. 2000, 84, S205–S209. [Google Scholar] [CrossRef]
- Cavaliere, A.; De Marchi, E.; Banterle, A. Exploring the adherence to the Mediterranean diet and its relationship with individual lifestyle: The role of healthy behaviors, pro-environmental behaviors, income, and education. Nutrients 2018, 10, 141. [Google Scholar] [CrossRef] [PubMed]
- Bonetti, L.; Campbell, M.A.; Gilmore, L. The relationship of loneliness and social anxiety with children’s and adolescents’ online communication. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.S.; Kozak, N.; Sullivan, K.A. An investigation of the relationship between subjective sleep quality, loneliness and mood in an Australian sample: Can daily routine explain the links? Int. J. Soc Psychiatry 2012, 58, 166–171. [Google Scholar] [CrossRef]
- Heinrich, L.M.; Gullone, E. The clinical significance of loneliness: A literature review. Clin. Psychol. Rev. 2006, 26, 695–718. [Google Scholar] [CrossRef]
- Cyr, B.A.; Berman, S.L.; Smith, M.L. The role of communication technology in adolescent relationships and identity development. Child Youth Care Forum. 2015, 44, 79–92. [Google Scholar] [CrossRef]
- Cartwright, M.; Wardle, J.; Steggles, N.; Simon, A.E.; Croker, H.; Jarvis, M.J. Stress and dietary practices in adolescents. Health Psychol. 2003, 22, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Michels, N.; Sioen, I.; Braet, C.; Eiben, G.; Hebestreit, A.; Huybrechts, I.; Vanaelst, B.; Vyncke, K.; De Henauw, S. Stress, emotional eating behavior and dietary patterns in children. Appetite 2012, 59, 762–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, T.C.; Epel, E.S. Stress, eating and the reward system. Physiol. Behav. 2007, 91, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Michels, N.; Sioen, I.; Ruige, J.; De Henauw, S. Children’s psychosocial stress and emotional eating: A role for leptin? Int. J. Eat Disord. 2017, 50, 471–480. [Google Scholar] [CrossRef]
- Coan, J.A.; Sbarra, D.A. Social baseline theory: The social regulation of risk and effort. Curr. Opin. Psychol. 2015, 1, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, R.E.; Torsheim, T.; Thuen, F. Loneliness, social integration and consumption of sugar-containing beverages: Testing the social baseline theory. PLoS ONE 2014, 8, e104421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ein-Dor, T.; Coan, J.A.; Reizer, A.; Gross, E.B.; Dahan, D.; Wegener, M.A.; Carel, R.; Cloninger, C.R.; Zohar, A.H. Sugarcoated isolation: Evidence that social avoidance is linked to higher basal glucose levels and higher consumption of glucose. Front. Psychol. 2015, 6, 492. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Hawkley, L.C.; Crawford, L.E.; Ernst, J.M.; Burleson, M.H.; Kowalewski, R.B.; Malarkey, W.B.; Van Cauter, E.; Berntson, G.G. Loneliness and Health: Potential Mechanisms. Psychosom. Med. 2002, 64, 407–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacioppo, J.T.; Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Thisted, R.A. Loneliness as a Specific Risk Factor for Depressive Symptoms: Cross-Sectional and Longitudinal Analyses. Psychol. Aging 2006, 21, 140–151. [Google Scholar] [CrossRef]
- Steptoe, A.; Owen, N.; Kunz-Ebrecht, S.R.; Brydon, L. Loneliness and Neuroendocrine, Cardiovascular, and Inflammatory Stress Responses in Middle-Aged Men and Women. Psychoneuroendocrinology 2004, 29, 593–611. [Google Scholar] [CrossRef]
- Ganley, R.M. Emotion and eating in obesity: A review of the literature. Int. J. Eat Disord. 1989, 8, 343–361. [Google Scholar] [CrossRef]
- Fox, J.R.; Power, M.J. Eating disorders and multi-level models of emotion: An integrated model. Clin. Psychol. Psychother. 2009, 16, 240–267. [Google Scholar] [CrossRef] [PubMed]
- Macht, M. How emotions affect eating: A five-way model. Appetite 2008, 50, 1–11. [Google Scholar] [CrossRef] [PubMed]
- De Vriendt, T.; Moreno, L.A.; De Henauw, S. Chronic stress and obesity in adolescents: Scientific evidence and methodological issues for epidemiological research. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Oliver, G.; Wardle, J. Perceived effects of stress on food choice. Physiol. Behav. 1999, 66, 511–515. [Google Scholar] [CrossRef]
- Mikolajczyk, R.T.; El Ansari, W.; Maxwell, A.E. Food consumption frequency and perceived stress and depressive symptoms among students in three European countries. Nutr. J. 2009, 8, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno, L.A.; Rodriguez, G.; Fleta, J.; Bueno-Lozano, M.; Lazaro, A.; Bueno, G. Trends of dietary habits in adolescents. Crit. Rev. Food Sci. Nutr. 2010, 50, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; García-Closas, R.; Ribas, L.; Pérez-Rodrigo, C.; Aranceta, J. Food patterns of Spanish schoolchildren and adolescents: The enKid Study. Public Health Nutr. 2001, 4, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Štefan, L.; Prosoli, R.; Juranko, D.; Čule, M.; Milinović, I.; Novak, D.; Sporiš, G. The reliability of the mediterranean diet quality index (KIDMED) questionnaire. Nutrients 2017, 9, 419. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Mendez, M.A.; Ribas-Barba, L.; Covas, M.I.; Serra-Majem, L. Mediterranean diet and waist circumference in a representative national sample of young Spaniards. Int. J. Pediatr. Obes. 2010, 5, 516–519. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 386–396. [Google Scholar] [CrossRef]
- Herrero, J.; Meneses, J. Short Web-based versions of the perceived stress (PSS) and Center for Epidemiological Studies-Depression (CESD) Scales: A comparison to pencil and paper responses among Internet users. Comput. Hum. Behav. 2006, 22, 830–846. [Google Scholar] [CrossRef]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Burlingame, B.; Dernini, S. Sustainable diets: The Mediterranean diet as an example. Public Health Nutr. 2011, 14, 2285–2297. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Ma, Y.; Han, Y.; Liu, Y.; Yang, K.; Zhen, S.; Wen, D. Psychosocial Correlates of Food Addiction and Its Association with Quality of Life in a Non-Clinical Adolescent Sample. Nutrients 2018, 10, 837. [Google Scholar] [CrossRef]
- Levine, M.P. Loneliness and eating disorders. J. Psychol. 2012, 146, 243–257. [Google Scholar] [CrossRef] [PubMed]
- Kalousova, L. Social isolation as a risk factor for inadequate diet of older Eastern Europeans. Int. J. Public Health 2014, 59, 707–714. [Google Scholar] [CrossRef]
- Locher, J.L.; Ritchie, C.S.; Roth, D.L.; Baker, P.S.; Bodner, E.V.; Allman, R.M. Social isolation, support, and capital and nutritional risk in an older sample: Ethnic and gender differences. Soc. Sci. Med. 2005, 60, 747–761. [Google Scholar] [CrossRef]
- Burks, C.E.; Jones, C.W.; Braz, V.A.; Swor, R.A.; Richmond, N.L.; Hwang, K.S.; Hollowell, A.G.; Weaver, M.A.; Platts-Mills, T.F. Risk factors for malnutrition among older adults in the emergency department: A multicenter study. J. Am. Geriatr. Soc. 2017, 65, 1741–1747. [Google Scholar] [CrossRef]
- Lee, C.Y.S.; Goldstein, S.E. Loneliness, stress, and social support in young adulthood: Does the source of support matter? J. Youth Adolesc. 2016, 45, 568–580. [Google Scholar] [CrossRef]
- Van Roekel, E.; Ha, T.; Verhagen, M.; Kuntsche, E.; Scholte, R.H.; Engels, R.C. Social stress in early adolescents’ daily lives: Associations with affect and loneliness. J. Adolesc. 2015, 45, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Yarcheski, A.; Mahon, N.E.; Yarcheski, T.J. Stress, hope, and loneliness in young adolescents. Psychol. Rep. 2011, 108, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Hill, D.C.; Moss, R.H.; Sykes-Muskett, B.; Conner, M.; O’Connor, D.B. Stress and eating behaviors in children and adolescents: Systematic review and meta-analysis. Appetite 2018, 123, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; Lee, C. Relationships between psychological stress, coping and disordered eating: A review. Psychol. Health 2000, 14, 1007–1035. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, C.L.; Laurent, J.; Brock, D.W. Food Addiction: A Barrier for Effective Weight Management for Obese Adolescents. Child Obes. 2017, 13, 462–469. [Google Scholar] [CrossRef]
- Arouca, A.B.; Santaliestra-Pasías, A.M.; Moreno, L.A.; Marcos, A.; Widhalm, K.; Molnár, D.; Manios, Y.; Gottrand, F.; Kafatos, A.; Kresting, M.; et al. Diet as a moderator in the association of sedentary behaviors with inflammatory biomarkers among adolescents in the HELENA study. Eur. J. Nutr. 2018. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ortiz-Andrellucchi, A. The Mediterranean diet as an example of food and nutrition sustainability: A multidisciplinary approach. Nutr. Hosp. 2018, 12, 96–101. [Google Scholar]


{kind=link}
| Variable/Characteristics (n = 527) | |||
|---|---|---|---|
| Dietary patterns | Fruit or fruit juice daily | No | 111 (21.1%) |
| Yes | 416 (78.9%) | ||
| Second serving of fruit daily | No | 260 (49.3%) | |
| Yes | 267 (50.7%) | ||
| Fresh or cooked vegetables daily | No | 173 (32.8%) | |
| Yes | 354 (67.2%) | ||
| Fresh or cooked vegetables >1/day | No | 306 (58.1%) | |
| Yes | 221 (41.9%) | ||
| Regular fish consumption (at least 2–3/week) | No | 200 (38%) | |
| Yes | 327 (62%) | ||
| Fast-food (hamburger) restaurant >1 week | No | 368 (69.8%) | |
| Yes | 159 (30.2%) | ||
| Pulse consumption >1/week | No | 181 (34.3%) | |
| Yes | 346 (65.7%) | ||
| Pasta or rice almost daily (≥5/week) | No | 216 (41%) | |
| Yes | 311 (59%) | ||
| Cereal or cereal product for breakfast | No | 210 (39.8%) | |
| Yes | 317 (60.2%) | ||
| Regular nut consumption (at least 2–3/week) | No | 252 (47.8%) | |
| Yes | 275 (52.2%) | ||
| Use of olive oil at home | No | 34 (6.5%) | |
| Yes | 493 (93.5%) | ||
| No breakfast | No | 387 (73.4%) | |
| Yes | 140 (26.6%) | ||
| Dairy product for breakfast | No | 175 (33.2%) | |
| Yes | 352 (66.8%) | ||
| Commercially baked goods or pastries for breakfast | No | 368 (69.8%) | |
| Yes | 159 (30.2%) | ||
| Two yogurts and/or 40 g cheese daily | No | 313 (59.4%) | |
| Yes | 214 (40.6%) | ||
| Sweets and candy several times a day | No | 451 (85.6%) | |
| Yes | 76 (14.4%) | ||
| Adherence to the MD | Low adherence to the MD | 103 (19.5%) | |
| Medium adherence to the MD | 197 (37.4%) | ||
| High adherence to the MD | 227 (43.1%) | ||
| Perceived Loneliness | 3.35 ± 0.89 | ||
| Stress | 8.93 ± 2.67 | ||
| Loneliness | Stress | |
|---|---|---|
| Fruit or fruit juice daily | −0.343 ** | −0.643 ** |
| Second serving of fruit daily | −0.443 ** | −0.561 ** |
| Fresh or cooked vegetables daily | −0.366 ** | −0.490 ** |
| Fresh or cooked vegetables >1/day | −0.456 ** | −0.552 ** |
| Regular fish consumption (at least 2–3/week) | −0.304 ** | −0.448 ** |
| Fast-food (hamburger) restaurant >1 week | 0.082 | 0.097 * |
| Pulse consumption >1/week | −0.287 ** | −0.314 ** |
| Pasta or rice almost daily (≥5/week) | −0.223 ** | −0.306 ** |
| Cereal or cereal product for breakfast | −0.333 ** | −0.473 ** |
| Regular nut consumption (at least 2–3/week) | −0.203 ** | −0.282 ** |
| Use of olive oil at home | −0.130 ** | −0.324 ** |
| No breakfast | 0.027 | 0.109 * |
| Dairy product for breakfast | −0.385 ** | −0.595 ** |
| Commercially baked goods or pastries for breakfast | 0.100 * | 0.051 |
| Two yogurts and/or 40 g cheese daily | −0.265 ** | −0.363 ** |
| Sweets and candy several times a day | 0.085 * | −0.084 * |
| Adherence to the MD | −0.686 ** | −0.930 ** |
| Perceived loneliness | |||||
|---|---|---|---|---|---|
| Low (n = 88) | Middle (n = 134) | High (n = 305) | |||
| Fruit or fruit juice daily | No | 1 (0.9%) | 3 (2.7%) | 107 (96.4%) | χ2 = 85.628, p = 0.0001 |
| Yes | 87 (20.9%) | 131 (31.5%) | 198 (47.6%) | ||
| Second serving of fruit daily | No | 11 (4.2%) | 34(13.1%) | 215 (82.7%) | χ2 = 133.167, p =0.0001 |
| Yes | 77 (28.8%) | 100 (37.5%) | 90 (33.7%) | ||
| Fresh or cooked vegetables daily | No | 5 (2.9%) | 17 (9.8%) | 151 (87.3%) | χ2 = 92.544, p = 0.0001 |
| Yes | 83 (23.4%) | 117 (33.1%) | 154 (43.5%) | ||
| Fresh or cooked vegetables >1/day | No | 22 (7.2%) | 39 (12.7%) | 245 (80.1%) | χ2 = 147.750, p =0.0001 |
| Yes | 66 (29.9%) | 95 (43%) | 69 (27.1%) | ||
| Regular fish consumption (at least 2–3/week) | No | 12 (6%) | 32 (16%) | 156 (78%) | χ2 = 55.915, p =0.0001 |
| Yes | 76 (23.2%) | 102 (31.2%) | 149 (45.6%) | ||
| Fast-food (hamburger) restaurant >1 week | No | 67 (18.2%) | 101 (27.4%) | 200 (54.3%) | χ2 = 6.238, p = 0.044 |
| Yes | 21 (13.2%) | 33 (20.8%) | 105 (66%) | ||
| Pulse consumption >1/week | No | 9 (5%) | 30 (16.6%) | 142 (78.5%) | χ2 = 51.369, p = 0.0001 |
| Yes | 79 (22.8%) | 104 (30.1%) | 163 (47.1%) | ||
| Pasta or rice almost daily (≥5/week) | No | 24 (11.1%) | 32 (14.8%) | 160 (74.1%) | χ2 = 39.650, p = 0.0001 |
| Yes | 64 (20.6%) | 102 (32.8%) | 145 (46.6%) | ||
| Cereal or cereal product for breakfast | No | 10 (4.8%) | 32 (15.2%) | 168 (80%) | χ2 = 73.571, p = 0.0001 |
| Yes | 78 (24.6%) | 102 (32.2%) | 137 (43.2%) | ||
| Regular nut consumption (at least 2–3/week) | No | 30 (11.9%) | 43 (17.1%) | 179 (71%) | χ2 = 34.375, p =0.0001 |
| Yes | 58 (21.1%) | 91 (33.1%) | 126 (45.8%) | ||
| Use of olive oil at home | No | 2 (5.9%) | 2 (5.9%) | 30 (88.2%) | χ2 = 13.795, p = 0.001 |
| Yes | 86 (17.4%) | 132 (26.8%) | 275 (55.8%) | ||
| No breakfast | No | 62 (16%) | 97 (25.1%) | 228 (58.9%) | χ2 = 0.748, p =0.688 |
| Yes | 26 (18.6%) | 37 (26.4%) | 77 (55%) | ||
| Dairy product for breakfast | No | 4 2.3(%) | 16 (9.1%) | 155 (88.6%) | χ2 = 102.574, p = 0.0001 |
| Yes | 84 (23.9%) | 118 (33.5%) | 150 (42.6%) | ||
| Commercially baked goods or pastries for breakfast | No | 68 (18.5%) | 102 (27.7%) | 198 (53.8%) | χ2 = 8.323, p =0.016 |
| Yes | 20 (12.6%) | 32 (20.1%) | 107 (67.3%) | ||
| Two yogurts and/or 40 g cheese daily | No | 33 (10.5%) | 63 (20.1%) | 217 (69.3%) | χ2 = 43.475, p = 0.0001 |
| Yes | 55 (25.7%) | 71 (33.2%) | 88 (41.1%) | ||
| Sweets and candy several times a day | No | 82 (18.2%) | 114 (25.3%) | 255 (56.5%) | χ2 = 5.111, p = 0.078 |
| Yes | 6 (7.9%) | 20 (26.3%) | 50 (65.8%) | ||
| Low adherence to the MD | 0 (0%) | 0 (0%) | 103 (100%) | χ2 = 418.856, p =0.0001 | |
| Medium adherence to the MD | 10 (5.1%) | 2 (1%) | 185 (93.9%) | ||
| High adherence to the MD | 78 (34.4%) | 132 (58.1%) | 17 (7.5%) | ||
| Model 1 | β | R2 | ΔR2 |
| Age | 0.012 | ||
| Sex | 0.067 | ||
| F (2,526) = 1.170, p = 0.311 | 0.004 | 0.004 | |
| Model 2 | β | R2 | ΔR2 |
| Age | 0.026 | ||
| Sex | 0.048 | ||
| Perceived Loneliness | −0.685 ** | ||
| F (3,526) = 156.509, p = 0.0001 | 0.470 | 0.469 ** | |
| Model 3 | β | R2 | ΔR2 |
| Age | −0.003 | ||
| Sex | 0.012 | ||
| Perceived Loneliness | −0.034 | ||
| Stress | −0.905 ** | ||
| F (4,526) = 837.265, p = 0.0001 | 0.864 | 0.392 ** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrer-Cascales, R.; Albaladejo-Blázquez, N.; Ruiz-Robledillo, N.; Rubio-Aparicio, M.; Laguna-Pérez, A.; Zaragoza-Martí, A. Low Adherence to the Mediterranean Diet in Isolated Adolescents: The Mediation Effects of Stress. Nutrients 2018, 10, 1894. https://doi.org/10.3390/nu10121894
Ferrer-Cascales R, Albaladejo-Blázquez N, Ruiz-Robledillo N, Rubio-Aparicio M, Laguna-Pérez A, Zaragoza-Martí A. Low Adherence to the Mediterranean Diet in Isolated Adolescents: The Mediation Effects of Stress. Nutrients. 2018; 10(12):1894. https://doi.org/10.3390/nu10121894
Chicago/Turabian StyleFerrer-Cascales, Rosario, Natalia Albaladejo-Blázquez, Nicolás Ruiz-Robledillo, María Rubio-Aparicio, Ana Laguna-Pérez, and Ana Zaragoza-Martí. 2018. "Low Adherence to the Mediterranean Diet in Isolated Adolescents: The Mediation Effects of Stress" Nutrients 10, no. 12: 1894. https://doi.org/10.3390/nu10121894
APA StyleFerrer-Cascales, R., Albaladejo-Blázquez, N., Ruiz-Robledillo, N., Rubio-Aparicio, M., Laguna-Pérez, A., & Zaragoza-Martí, A. (2018). Low Adherence to the Mediterranean Diet in Isolated Adolescents: The Mediation Effects of Stress. Nutrients, 10(12), 1894. https://doi.org/10.3390/nu10121894