Caffeine-Related Deaths: Manner of Deaths and Categories at Risk

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Criteria and Critical Appraisal
3. Results
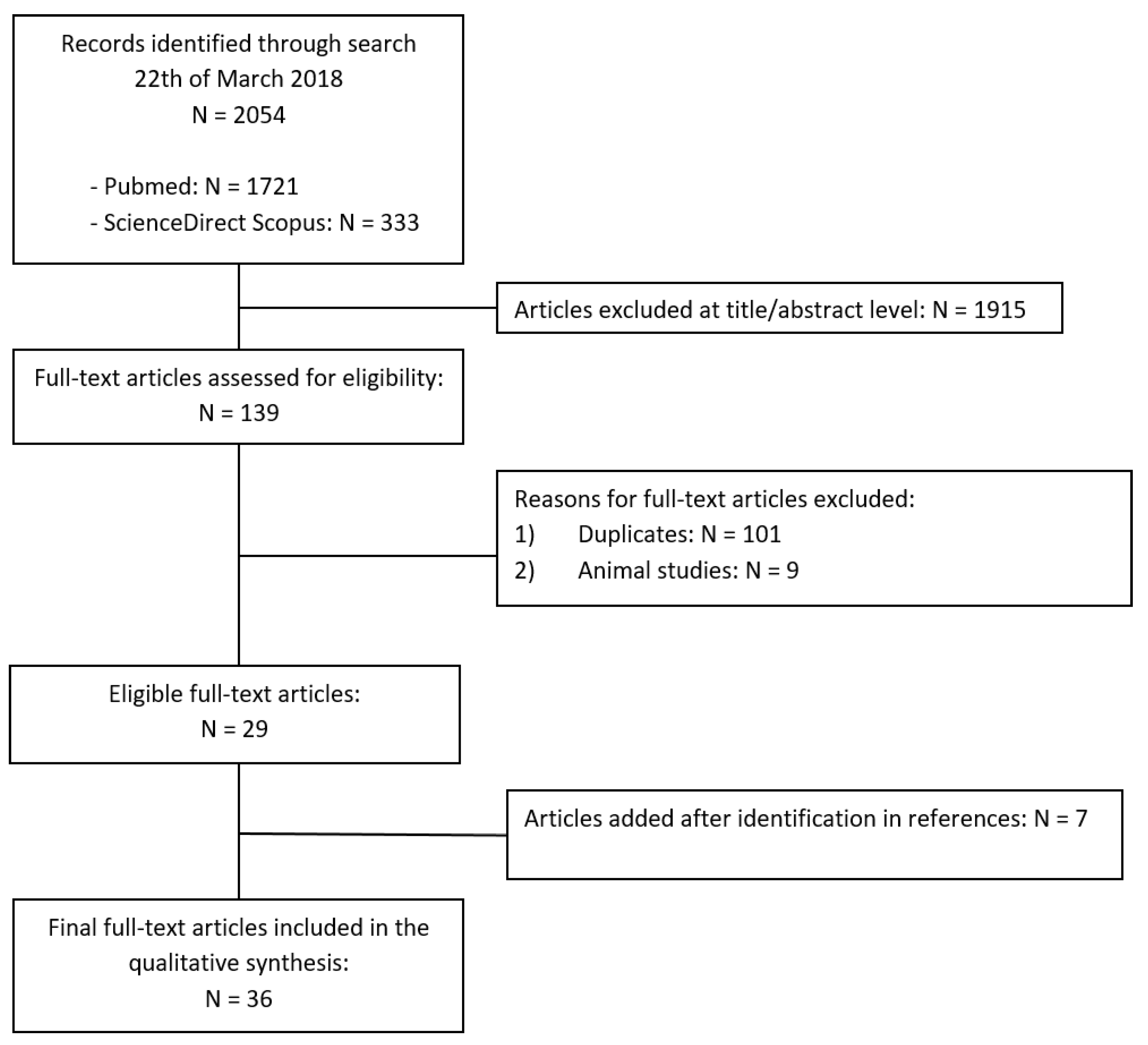
3.1. Search Results and Included Studies
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Caffeine-Related Fatalities
3.5. Athletes
3.6. Psychiatric Patients
3.7. Infants
4. Discussion
- interactions with other substances with a synergistic effect when consumed with caffeine or able to increase caffeine’s blood levels;
- individuals’ pre-existing diseases and/or conditions capable of potentiating the effects of caffeine;
- inter-individual differences, mostly genetically determined, that can affect caffeine metabolism in both directions (i.e., increase or reduction), contributing to a different individual “sensibility” to the effects of the substance.
4.1. Caffeine and Athletes
4.2. Caffeine and Psychiatric Patients
4.3. Caffeine and Infants
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Jokela, S.; Varliainen, A. Caffeine poisoning. Acta Pharmacol. Toxicol. 1959, 15, 331–334. [Google Scholar] [CrossRef]
- Cappelletti, S.; Piacentino, D.; Sani, G.; Aromatario, M. Caffeine: Cognitive and physical performance enhancer or psychoactive drug? Curr. Neuropharmacol. 2015, 13, 71–88. [Google Scholar] [CrossRef] [PubMed]
- Nawrot, P.; Jordan, S.; Eastwood, J.; Rotstein, J.; Hugenholtz, A.; Feeley, M. Effects of caffeine on human health. Food Addit. Contam. 2003, 20, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Higdon, J.V.; Frei, B. Coffee and health: A review of recent human research. Crit. Rev. Food Sci. Nutr. 2006, 46, 101–123. [Google Scholar] [CrossRef] [PubMed]
- Musgrave, I.F.; Farrington, R.L.; Hoban, C.; Byard, R.W. Caffeine toxicity in forensic practice: Possible effects and under-appreciated sources. Forensic Sci. Med. Pathol. 2016, 12, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.W. Review of caffeine-related fatalities along with postmortem blood concentrations in 51 poisoning deaths. J. Anal. Toxicol. 2017, 41, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Wikoff, D.; Welsh, B.T.; Henderson, R.; Brorby, G.P.; Britt, J.; Myers, E.; Goldberger, J.; Lieberman, H.R.; O’Brien, C.; Peck, J.; et al. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem. Toxicol. 2017, 109, 585–648. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Farago, A. Fatal accidental caffeine poisoning of a child. Bull. Int. Assoc. Forensic Toxicol. 1968, 5, 2–3. [Google Scholar]
- Alstott, R.L.; Miller, A.J.; Forney, R.B. Report of a human fatality due to caffeine. J. Forensic Sci. 1973, 18, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Grusz-Hardy, E. Lethal caffeine poisoning. Bull. Int. Assoc. Forensic Toxicol. 1973, 4, 6–7. [Google Scholar]
- Dimaio, V.J.M.; Garriott, J.C. Lethal caffeine poisoning in a child. Forensic Sci. 1974, 3, 275–278. [Google Scholar] [CrossRef]
- Turner, J.E.; Cravey, R.H. A fatal ingestion of caffeine. Clin. Toxicol. 1977, 10, 341–344. [Google Scholar] [CrossRef] [PubMed]
- McGee, M.B. Caffeine poisoning in a 19-year-old female. J. Forensic Sci. 1980, 25, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Bryant, J. Suicide by ingestion of caffeine. Arch. Pathol. Lab. Med. 1981, 105, 685–686. [Google Scholar] [PubMed]
- Chaturvedi, A.K.; Rao, N.G.; McCoy, F.E. A multi-chemical death involving caffeine, nicotine and malathion. Forensic Sci. Int. 1983, 23, 265–275. [Google Scholar] [CrossRef]
- Garriott, J.C.; Simmons, L.M.; Poklis, A.; Mackell, M.A. Five cases of fatal overdose from caffeine containing look alike drugs. J. Anal. Toxicol. 1985, 9, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Winek, C.L.; Wahba, W.; Williams, K.; Blenko, J.; Janssen, J. Caffeine fatality: A case report. Forensic Sci. Int. 1985, 29, 207–211. [Google Scholar] [CrossRef]
- Hanzlick, R.; Gowitt, G.T.; Wall, W. Deaths due to caffeine in “look-alike drugs”. J. Anal. Toxicol. 1986, 10, 126. [Google Scholar] [CrossRef] [PubMed]
- Morrow, P.L. Caffeine toxicity: A case of child abuse by drug ingestion. J. Forensic Sci. 1987, 32, 1801–1805. [Google Scholar] [CrossRef] [PubMed]
- Mrvos, R.M.; Reilly, P.E.; Dean, B.S.; Krenzelok, E.P. Massive caffeine ingestion resulting in death. Vet. Hum. Toxicol. 1989, 31, 571–572. [Google Scholar] [PubMed]
- Takayasu, T.; Nishigami, J.; Ohshima, T.; Lin, Z.; Kondo, T.; Nakaya, T.; Sawaguchi, T.; Nagano, T. A fatal case due to intoxication with seven drugs detected by GC-MS and TDx methods. Nihon Hoigaku Zasshi 1993, 47, 63–71. [Google Scholar] [PubMed]
- Rivenes, S.M.; Bakerman, P.R.; Miller, M.B. Intentional caffeine poisoning in an infant. Pediatrics 1997, 99, 736–738. [Google Scholar] [CrossRef] [PubMed]
- Shum, S.; Seale, C.; Hathaway, D.; Chucovich, V.; Beard, D. Acute caffeine ingestion fatalities: Management issues. Vet. Hum. Toxicol. 1997, 39, 228–230. [Google Scholar] [PubMed]
- Riesselmann, B.; Rosenbaum, F.; Roscher, S.; Schneider, V. Fatal caffeine intoxication. Forensic Sci. Int. 1999, 103, 49–52. [Google Scholar] [CrossRef]
- Watson, W.A.; Litovitz, T.L.; Klein-Schwartz, W.; Rodgers, G.C., Jr.; Youniss, J.; Reid, N.; Rouse, W.G.; Rembert, R.S.; Borys, D. 2003 annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am. J. Emerg. Med. 2004, 22, 335–404. [Google Scholar] [CrossRef] [PubMed]
- Holmgren, P.; Nordén-Pettersson, L.; Ahlner, J. Caffeine fatalities—Four case reports. Forensic Sci. Int. 2004, 139, 71–73. [Google Scholar] [CrossRef] [PubMed]
- Watson, W.A.; Litovitz, T.L.; Rodgers, G.C., Jr.; Klein-Schwartz, W.; Reid, N.; Youniss, J.; Flanagan, A.; Wruk, K.M. 2004 Annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am. J. Emerg. Med. 2005, 23, 589–666. [Google Scholar] [CrossRef] [PubMed]
- Kerrigan, S.; Lindsey, T. Fatal caffeine overdose: Two case reports. Forensic Sci. Int. 2005, 153, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, S.; Homma, M.; Inoue, J.; Kato, H.; Murata, K.; Ogasawara, T. Case of intractable ventricular fibrillation by a multicomponent dietary supplement containing ephedra and caffeine overdose. Jpn. J. Toxicol. 2007, 20, 269–271. [Google Scholar]
- Rudolph, T.; Knudsen, K. A case of fatal caffeine poisoning. Acta Anaesthesiol. Scand. 2010, 54, 521–523. [Google Scholar] [CrossRef] [PubMed]
- Thelander, G.; Jönsson, A.K.; Personne, M.; Forsberg, G.S.; Lundqvist, K.M.; Ahlner, J. Caffeine fatalities—Do sales restrictions prevent intentional intoxications? Clin. Toxicol. 2010, 48, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Jabbar, S.B.; Hanly, M.G. Fatal caffeine overdose: A case report and review of literature. Am. J. Forensic Med. Pathol. 2013, 34, 321–324. [Google Scholar] [CrossRef] [PubMed]
- Jantos, R.; Stein, K.M.; Flechtenmacher, C.; Skopp, G. A fatal case involving a caffeine-containing fat burner. Drug Test. Anal. 2013, 5, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Poussel, M.; Kimmoun, A.; Levy, B.; Gambier, N.; Dudek, F.; Puskarczyk, E.; Poussel, J.F.; Chenuel, B. Fatal cardiac arrhythmia following voluntary caffeine overdose in an amateur body-builder athlete. Int. J. Cardiol. 2013, 166, e41–e42. [Google Scholar] [CrossRef] [PubMed]
- Bonsignore, A.; Sblano, S.; Pozzi, F.; Ventura, F.; Dell’Erba, A.; Palmiere, C. A case of suicide by ingestion of caffeine. Forensic Sci. Med. Pathol. 2014, 10, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, P.; Ali, Z.; Levine, B.; Fowler, D.R. Fatal caffeine intoxication: A series of eight cases from 1999 to 2009. J. Forensic Sci. 2014, 59, 865–868. [Google Scholar] [CrossRef] [PubMed]
- Eichner, E.R. Fatal caffeine overdose and other risks from dietary supplements. Curr. Sports Med. Rep. 2014, 13, 353–354. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Tanifuji, T.; Abe, N.; Maeda, M.; Kato, Y.; Shibata, M.; Fukunaga, T. Characteristics of caffeine intoxication-related death in Tokyo, Japan, between 2008 and 2013. Nihon Arukoru Yakubutsu Igakkai Zasshi 2014, 49, 270–277. [Google Scholar] [PubMed]
- Ishikawa, T.; Yuasa, I.; Endoh, M. Non specific drug distribution in an autopsy case report of fatal caffeine intoxication. Leg. Med. 2015, 17, 535–538. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Yoshizawa, K.; Kubo, S.; Emoto, Y.; Hara, K.; Waters, B.; Umehara, T.; Murase, T.; Ikematsu, K. Autopsy report for a caffeine intoxication case and review of the current literature. J. Toxicol. Pathol. 2015, 28, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Aknouche, F.; Guibert, E.; Tessier, A.; Eibel, A.; Kintz, P. Suicide by ingestion of caffeine. Egypt. J. Forensic Sci. 2017, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Magdalan, J.; Zawadzki, M.; Skowronek, R.; Czuba, M.; Porębska, B.; Sozański, T.; Szpot, P. Nonfatal and fatal intoxications with pure caffeine—Report of three different cases. Forensic Sci. Med. Pathol. 2017, 13, 355–358. [Google Scholar] [CrossRef] [PubMed]
- FitzSimmons, C.R.; Kidner, N. Caffeine toxicity in a bodybuilder. J. Accid. Emerg. Med. 1998, 15, 196–197. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.C.; de Oliveira Ribeiro, N.P.; de Mello Schier, A.R.; Pereira, V.M.; Vilarim, M.M.; Pessoa, T.M.; Arias-Carrion, O.; Machado, S.; Nardi, A.E. Caffeine and suicide: A systematic review. CNS Neurol. Disord. Drug Targets 2014, 13, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Ciszowski, K.; Biedron, W.; Gomolka, E. Acute caffeine poisoning resulting in atrial fibrillation after guarana extract overdose. Prz. Lek. 2014, 71, 495–498. [Google Scholar] [PubMed]
- Bryczkowski, C.; Geib, A.J. Combined butalbital/acetaminophen/caffeine overdose: Case files of the Robert Wood Johnson Medical School Toxicology Service. J. Med. Toxicol. 2012, 8, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.J.; Alford, K. Cardiac arrest in a young man following excess consumption of caffeinated ‘‘energy drinks’’. Med. J. Aust. 2009, 190, 41–43. [Google Scholar] [PubMed]
- Rhidian, R. Running a risk? Sport supplement toxicity with ephedrine in an amateur marathon runner, with subsequent rhabdomyolysis. BMJ Case Rep. 2011. [Google Scholar] [CrossRef] [PubMed]
- World Anti-Doping Agency. The 2009 Monitoring Program. Available online: https://www.wada-ama.org/sites/default/files/resources/files/WADA_Monitoring_Program_2009_EN.pdf (accessed on 21 March 2018).
- Ogawa, N.; Ueki, H. Clinical importance of caffeine dependence and abuse. Psychiatry Clin. Neurosci. 2007, 61, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Broderick, P.; Benjamin, A.B. Caffeine and psychiatric symptoms: A review. J. Okla. State Med. Assoc. 2004, 97, 538–542. [Google Scholar] [PubMed]
- Ogawa, N.; Ueki, H. Secondary mania caused by caffeine. Gen. Hosp. Psychiatry 2003, 25, 138–139. [Google Scholar] [CrossRef]
- Childs, E.; Hohoff, C.; Deckert, J.; Xu, K.; Badner, J.; de Wit, H. Association between ADORA2A and DRD2 polymorphisms and caffeine-induced anxiety. Neuropsychopharmacology 2008, 33, 2791–2800. [Google Scholar] [CrossRef] [PubMed]
- Stock, S.L.; Goldberg, E.; Corbett, S.; Katzman, D.K. Substance use in female adolescents with eating disorders. J. Adolesc. Health 2002, 31, 176–182. [Google Scholar] [CrossRef]
- Caykoylu, A.; Ekinci, O.; Kuloglu, M. Improvement from treatment-resistant schizoaffective disorder, manic type after stopping heavy caffeine intake: A case report. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 1349–1350. [Google Scholar] [CrossRef] [PubMed]
- Hedges, D.W.; Woon, F.L.; Hoopes, S.P. Caffeine-induced psychosis. CNS Spectr. 2009, 14, 127–129. [Google Scholar] [CrossRef] [PubMed]
- Broderick, P.J.; Benjamin, A.B.; Dennis, L.W. Caffeine and psychiatric medication interactions: A review. J. Okla. State Med. Assoc. 2005, 98, 380–384. [Google Scholar] [PubMed]
- Kendler, K.S.; Prescott, C.A.; Myers, J.; Neale, M.C. The structure of genetic and environmental risk factors for common psychiatric and substance use disorders in men and women. Arch. Gen. Psychiatry 2003, 60, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Zeiner, A.R.; Stanitis, T.; Spurgeon, M.; Nichols, N. Treatment of alcoholism and concomitant drugs of abuse. Alcohol 1985, 2, 555–559. [Google Scholar] [CrossRef]
- Aubin, H.J.; Laureaux, C.; Tilikete, S.; Barrucand, D. Changes in cigarette smoking and coffee drinking after alcohol detoxification in alcoholics. Addiction 1999, 94, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Fischler, R.S. Poisoning: A syndrome of child abuse. Am. Fam. Physician 1983, 28, 103–108. [Google Scholar] [PubMed]
- Tenenbein, M. Recent advancements in pediatric toxicology. Pediatr. Clin. N. Am. 1999, 46, 1179–1188. [Google Scholar] [CrossRef]
- Meadow, R. ABC of child abuse. Poisoning. Br. Med. J. 1989, 27, 1445–1446. [Google Scholar] [CrossRef]
- Henretig, F.M.; Paschall, R.T.; Donaruma-Kwoh, M.M. Child abuse by poisoning. In Child Abuse: Medical Diagnosis and Management; Reece, R.M., Christian, C.W., Eds.; American Academy of Pediatrics: Farmington Hills, MI, USA, 2009; pp. 549–599. [Google Scholar]
- Dine, M.S.; McGovern, M.E. Intentional poisoning of children—An overlooked category of child abuse: Report of seven cases and review of the literature. Pediatrics 1982, 70, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.C.; Lin, K.L.; Lin, J.J.; Hsia, S.H.; Wu, C.T. Non-accidental chlorpyrifos poisoning-an unusual cause of profound unconsciousness. Eur. J. Pediatr. 2010, 169, 509–511. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, C.C.; Alexander, R.; Beck, D.; Bursch, B.; Feldman, K.W.; Libow, J.; Sanders, M.J.; Schreier, H.A.; Yorker, B. APSAC Taskforce on Munchausen by Proxy, Definitions Working Group. Position paper: Definitional issues in Munchausen by proxy. Child Maltreat 2002, 7, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Moldavsky, M.; Stein, D. Munchausen Syndrome by Proxy: Two case reports and an update of the literature. Int. J. Psychiatry Med. 2003, 33, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.J.; Gunn, T.R.; Holford, N.H.; Johnson, R. Caffeine overdose in a premature infant: Clinical course and pharmacokinetics. Anaesth. Intensive Care 1999, 27, 307–311. [Google Scholar] [PubMed]
- Ergenekon, E.; Dalgiç, N.; Aksoy, E.; Koç, E.; Atalay, Y. Caffeine intoxication in a premature neonate. Paediatr. Anaesth. 2001, 11, 737–739. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) | Caffeine Blood Level (mg/L) | Age | Gender | Manner of Death | Route of Administration (Source) |
|---|---|---|---|---|---|
| Jokela et al. (1959) [1] | - | 35 | F | Accidental | Intravenous |
| Farago et al. (1968) [9] | 1040 mg/L | 15 months | - | Child abuse | Intravenous |
| Alstott et al. (1973) [10] | - | 27 | M | Suicide | Oral (pills) |
| Grusz-Hardy (1973) [11] | 79 mg/L | 45 | F | Accidental | Oral (pills) |
| Dimaio et al. (1974) [12] | 158.5 mg/L | 5 | F | Accidental | Oral (pills) |
| Turner et al. (1977) [13] | 106 mg/L | 34 | F | Uncertain | Oral (pills) |
| McGee (1980) [14] | 181 mg/L | 19 | F | Accidental | Oral (pills) |
| Bryant (1981) [15] | 113.5 mg/L | 42 | F | Suicide | Oral (pills) |
| Chaturvedi et al. (1983) [16] | 62 mg/L | 21 | M | Suicide | Oral (pills) |
| Garriott et al. (1985) [17] | 129.9 mg/L | 19 | F | Suicide | Oral (pills) |
| 147 mg/L | 21 | M | Suicide | Oral (pills) | |
| 343.9 mg/L | 21 | M | Suicide | Oral (pills) | |
| 184.1 mg/L | 23 | M | Accidental | Oral (pills) | |
| 251 mg/L | 21 | F | Suicide | Oral (pills) | |
| Winek et al. (1985) [18] | 240 mg/L | 21 | F | Suicide | Oral (pills) |
| Hanzlick et al. (1986) [19] | 264 mg/L | 44 | F | suicide | Oral (pills) |
| 182 mg/L | 20 | F | accidental | Oral (pills) | |
| Morrow (1987) [20] | 117.3 mg/L | 14 months | - | Child abuse | Oral (pills) |
| Mrvos et al. (1989) [21] | 1560 mg/L | 22 | F | Accidental | Oral (pills) |
| Takayasu et al. (1993) [22] | 177.0 μg/g | 20 | F | Suicide | Oral (pills) |
| Rivenes et al. (1997) [23] | 117 mg/L | 5 weeks | M | Child abuse | Oral (pills) |
| Shum et al. (1997) [24] | 108 mcg/dL | 15 | F | Accidental | Oral (pills) |
| 30 mcg/dL | 32 | M | Accidental | Oral (pills) | |
| Riesselmann et al. (1999) [25] | 220 mg/L | 19 | F | Accidental | Oral (pills) |
| 190 mg/L | 81 | F | Suicide | Not reported | |
| Watson et al. (2004) [26] | - | 17 | - | Suicide | Oral (pills) |
| Holmgren et al. (2004) [27] | 173 mg/L | 54 | M | Uncertain | Oral (pills) |
| 210 mg/L | 21 | M | Suicide | Oral (pills) | |
| 153 mg/L | 31 | M | Suicide | Oral (pills) | |
| 200 mg/L | 47 | F | Uncertain | Oral (pills) | |
| Watson et al. (2005) [28] | - | 33 | - | Accidental | Oral (pills) |
| Kerrigan et al. (2005) [29] | 192 mg/L | 39 | F | Accidental | Intravenous |
| 567 mg/L | 29 | M | Accidental | Oral (pills) | |
| Takeuchi et al. (2007) [30] | - | - | - | Accidental | Oral (pills) |
| Rudolph et al. (2010) [31] | - | 21 | F | Suicide | Oral (pills) |
| Thelander et al. (2010) [32] | 90 mg/L | 43 | M | Uncertain | Not reported |
| 105 mg/L | 53 | M | Suicide | Not reported | |
| 170 mg/L | 47 | M | Uncertain | Not reported | |
| 86 mg/L | 26 | F | Uncertain | Not reported | |
| 210 mg/L | 25 | F | Suicide | Not reported | |
| 230 mg/L | 40 | F | Uncertain | Not reported | |
| 210 mg/L | 21 | M | Suicide | Not reported | |
| 153 mg/L | 31 | M | Suicide | Not reported | |
| 173 mg/L | 54 | M | Uncertain | Not reported | |
| 200 mg/L | 47 | F | Uncertain | Not reported | |
| 180 mg/L | 18 | F | Suicide | Not reported | |
| 166 mg/L | 20 | F | Suicide | Not reported | |
| 140 mg/L | 72 | F | Suicide | Not reported | |
| 80 mg/L | 24 | M | Suicide | Not reported | |
| 160 mg/L | 46 | F | Suicide | Not reported | |
| 113 mg/L | 73 | F | Uncertain | Not reported | |
| 138 mg/L | 66 | M | Accidental | Not reported | |
| 190 mg/L | 84 | M | Suicide | Not reported | |
| 192 mg/L | 79 | F | Suicide | Not reported | |
| 310 mg/L | 33 | F | Suicide | Not reported | |
| Jabbar et al. (2013) [33] | 350 mg/L | 39 | M | Accidental | Oral (powder) |
| Jantos et al. (2013) [34] | 141 mg/L | 25 | F | Suicide | Oral (pills) |
| Poussel et al. (2013) [35] | 190 mg/L | 44 | M | Accidental | Oral (pills) |
| Bonsignore et al. (2014) [36] | 170 mg/L | 3 | M | Suicide | Oral (pills) |
| Banerjee et al. (2014) [37] | 320 mg/L | 50 | F | Uncertain | Oral (pills) |
| 73 mg/L | 37 | F | Uncertain | Not reported | |
| 320 mg/L | 43 | F | Suicide | Oral (pills) | |
| 74 mg/L | 44 | M | Uncertain | Oral (pills) | |
| 220 mg/L | 57 | M | Suicide | Oral (pills) | |
| Eichner ER (2014) [38] | >70 mg/L | 18 | M | Accidental | Oral (powder) |
| Suzuki et al. (2014) [39] | 179 mg/L | 22 cases 20–90 years-old | - | 11 unknown 7 accidental 2 suicide 2 others | |
| Ishikawa et al. (2015) [40] | Blood 154.2 mg/L Bile 852.3 mg/L Stomach 197.5 mg/L | 20 | F | Suicide | Oral (pills) |
| Yamamoto et al. (2015) [41] | 290 mg/L | 18 | F | Suicide | Oral (pills) |
| Aknouche et al. (2017) [42] | 401 mg/L | 48 | M | Suicide | Oral (pills) |
| Magdalan et al. (2017) [43] | 140 mg/L | 27 | M | Accidental | Oral (pills) |
| 613 mg/L | 20 | F | Uncertain | Oral (powder) |
| Causes | Cases |
|---|---|
| Not reported | 10 |
| Over-the-counter caffeine products | 9 |
| Errors in hospital medication | 3 |
| Drug abuse | 2 |
| Recreational use | 2 |
| Accidental ingestion by children | 1 |
| Disease * | Number |
|---|---|
| Depression | 20 |
| Alcohol dependence | 6 |
| Sleep disorders | 6 |
| Drug dependence | 4 |
| Eating disorder | 3 |
| Panic disorder | 2 |
| Schizophrenia | 2 |
| Not specified | 2 |
| Paranoid disorder | 1 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cappelletti, S.; Piacentino, D.; Fineschi, V.; Frati, P.; Cipolloni, L.; Aromatario, M. Caffeine-Related Deaths: Manner of Deaths and Categories at Risk. Nutrients 2018, 10, 611. https://doi.org/10.3390/nu10050611
Cappelletti S, Piacentino D, Fineschi V, Frati P, Cipolloni L, Aromatario M. Caffeine-Related Deaths: Manner of Deaths and Categories at Risk. Nutrients. 2018; 10(5):611. https://doi.org/10.3390/nu10050611
Chicago/Turabian StyleCappelletti, Simone, Daria Piacentino, Vittorio Fineschi, Paola Frati, Luigi Cipolloni, and Mariarosaria Aromatario. 2018. "Caffeine-Related Deaths: Manner of Deaths and Categories at Risk" Nutrients 10, no. 5: 611. https://doi.org/10.3390/nu10050611
APA StyleCappelletti, S., Piacentino, D., Fineschi, V., Frati, P., Cipolloni, L., & Aromatario, M. (2018). Caffeine-Related Deaths: Manner of Deaths and Categories at Risk. Nutrients, 10(5), 611. https://doi.org/10.3390/nu10050611