Impact of Alcohol and Coffee Intake on the Risk of Advanced Liver Fibrosis: A Longitudinal Analysis in HIV-HCV Coinfected Patients (ANRS CO-13 HEPAVIH Cohort)

 , , , , and
, , , , and
Abstract
:1. Background
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.2.1. Outcome: Advanced Liver Fibrosis (ALF)
2.2.2. Covariates
Clinical Variables
Variables in the Self-Administered Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics at the Last Available Follow-Up Visit with a Completed Self-Administered Questionnaire
3.2. Factors Associated with ALF
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pawlotsky, J.-M. Pathophysiology of hepatitis C virus infection and related liver disease. Trends Microbiol. 2004, 12, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Castello, G.; Scala, S.; Palmieri, G.; Curley, S.A.; Izzo, F. HCV-related hepatocellular carcinoma: From chronic inflammation to cancer. Clin. Immunol. 2010, 134, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Moqueet, N.; Kanagaratham, C.; Gill, M.J.; Hull, M.; Walmsley, S.; Radzioch, D.; Saeed, S.; Platt, R.W.; Klein, M.B.; Canadian Co-infection Cohort Study (CTN 222). A prognostic model for development of significant liver fibrosis in HIV-hepatitis C co-infection. PLoS ONE 2017, 12, e0174205. [Google Scholar] [CrossRef] [PubMed]
- Marcellin, P.; Asselah, T.; Boyer, N. Fibrosis and disease progression in hepatitis C. Hepatology 2002, 36, s47–s56. [Google Scholar] [PubMed]
- Poynard, T.; Ratziu, V.; Charlotte, F.; Goodman, Z.; McHutchison, J.; Albrecht, J. Rates and risk factors of liver fibrosis progression in patients with chronic hepatitis C. J. Hepatol. 2001, 34, 730–739. [Google Scholar] [CrossRef]
- Joshi, K.; Kohli, A.; Manch, R.; Gish, R. Alcoholic Liver Disease: High Risk or Low Risk for Developing Hepatocellular Carcinoma? Clin. Liver Dis. 2016, 20, 563–580. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Wang, X.; Wu, G.; Chen, L.; Hu, P.; Ren, H.; Hu, H. Coffee Consumption Decreases Risks for Hepatic Fibrosis and Cirrhosis: A Meta-Analysis. PLoS ONE 2015, 10, e0142457. [Google Scholar] [CrossRef] [PubMed]
- Alferink, L.J.M.; Fittipaldi, J.; Kiefte-de Jong, J.C.; Taimr, P.; Hansen, B.E.; Metselaar, H.J.; Schoufour, J.D.; Ikram, M.A.; Janssen, H.L.A.; Franco, O.H.; et al. Coffee and herbal tea consumption is associated with lower liver stiffness in the general population: The Rotterdam study. J. Hepatol. 2017, 67, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Heckman, M.A.; Weil, J.; De Mejia, E.G. Caffeine (1, 3, 7-trimethylxanthine) in Foods: A Comprehensive Review on Consumption, Functionality, Safety, and Regulatory Matters. J. Food Sci. 2010, 75, R77–R87. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Pluchinotta, F.R.; Marventano, S.; Buscemi, S.; Li Volti, G.; Galvano, F.; Grosso, G. Coffee components and cardiovascular risk: Beneficial and detrimental effects. Int. J. Food Sci. Nutr. 2014, 65, 925–936. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Godos, J.; Galvano, F.; Giovannucci, E.L. Coffee, Caffeine, and Health Outcomes: An Umbrella Review. Annu. Rev. Nutr. 2017, 37, 131–156. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Micek, A.; Godos, J.; Sciacca, S.; Pajak, A.; Martínez-González, M.A.; Giovannucci, E.L.; Galvano, F. Coffee consumption and risk of all-cause, cardiovascular, and cancer mortality in smokers and non-smokers: A dose-response meta-analysis. Eur. J. Epidemiol. 2016, 31, 1191–1205. [Google Scholar] [CrossRef] [PubMed]
- Alicandro, G.; Tavani, A.; La Vecchia, C. Coffee and cancer risk: A summary overview. Eur. J. Cancer Prev. 2017, 26, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Ding, M.; Bhupathiraju, S.N.; Satija, A.; van Dam, R.M.; Hu, F.B. Long-term coffee consumption and risk of cardiovascular disease: A systematic review and a dose-response meta-analysis of prospective cohort studies. Circulation 2014, 129, 643–659. [Google Scholar] [CrossRef] [PubMed]
- Carrieri, M.P.; Lions, C.; Sogni, P.; Winnock, M.; Roux, P.; Mora, M.; Bonnard, P.; Salmon, D.; Dabis, F.; Spire, B.; ANRS CO13 HEPAVIH Study Group. Association between elevated coffee consumption and daily chocolate intake with normal liver enzymes in HIV-HCV infected individuals: Results from the ANRS CO13 HEPAVIH cohort study. J. Hepatol. 2014, 60, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Oh, M.G.; Han, M.A.; Kim, M.W.; Park, C.G.; Kim, Y.D.; Lee, J. Coffee consumption is associated with lower serum aminotransferases in the general Korean population and in those at high risk for hepatic disease. Asia Pac. J. Clin. Nutr. 2016, 25, 767–775. [Google Scholar] [PubMed]
- Morisco, F.; Lembo, V.; Mazzone, G.; Camera, S.; Caporaso, N. Coffee and liver health. J. Clin. Gastroenterol. 2014, 48 (Suppl. 1), S87–S90. [Google Scholar] [CrossRef] [PubMed]
- Stroffolini, T.; Cotticelli, G.; Medda, E.; Niosi, M.; Del Vecchio-Blanco, C.; Addolorato, G.; Petrelli, E.; Salerno, M.T.; Picardi, A.; Bernardi, M.; et al. Interaction of alcohol intake and cofactors on the risk of cirrhosis. Liver Int. 2010, 30, 867–870. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Everhart, J.E.; Lindsay, K.L.; Ghany, M.G.; Curto, T.M.; Shiffman, M.L.; Lee, W.M.; Lok, A.S.; Di Bisceglie, A.M.; Bonkovsky, H.L.; et al. Coffee Intake Is Associated with Lower Rates of Liver Disease Progression in Chronic Hepatitis C. Hepatology 2009, 50, 1360–1369. [Google Scholar] [CrossRef] [PubMed]
- Carrieri, M.P.; Cohen, J.; Salmon-Ceron, D.; Winnock, M. Coffee consumption and reduced self-reported side effects in HIV-HCV co-infected patients during PEG-IFN and ribavirin treatment: Results from ANRS CO13 HEPAVIH. J. Hepatol. 2012, 56, 745–747. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.G.; Jun, D.W.; Kim, E.K.; Saeed, W.K.; Lee, K.N.; Lee, H.L.; Lee, O.Y.; Choi, H.S.; Yoon, B.C. Caffeine attenuates liver fibrosis via defective adhesion of hepatic stellate cells in cirrhotic model. J. Gastroenterol. Hepatol. 2013, 28, 1877–1884. [Google Scholar] [CrossRef] [PubMed]
- Bai, K.; Cai, Q.; Jiang, Y.; Lv, L. Coffee consumption and risk of hepatocellular carcinoma: A meta-analysis of eleven epidemiological studies. OncoTargets Ther. 2016, 9, 4369–4375. [Google Scholar]
- Loko, M.-A.; Salmon, D.; Carrieri, P.; Winnock, M.; Mora, M.; Merchadou, L.; Gillet, S.; Pambrun, E.; Delaune, J.; Valantin, M.A.; et al. The French national prospective cohort of patients co-infected with HIV and HCV (ANRS CO13 HEPAVIH): Early findings, 2006–2010. BMC Infect. Dis. 2010, 10, 303. [Google Scholar] [CrossRef] [PubMed]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Carrieri, M.P.; Protopopescu, C.; Marcellin, F.; Rosellini, S.; Wittkop, L.; Esterle, L.; Zucman, D.; Raffi, F.; Rosenthal, E.; Poizot-Martin, I.; et al. Protective effect of coffee consumption on all-cause mortality of French HIV-HCV co-infected patients. J. Hepatol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Labarga, P.; Fernandez-Montero, J.V.; de Mendoza, C.; Barreiro, P.; Pinilla, J.; Soriano, V. Liver fibrosis progression despite HCV cure with antiviral therapy in HIV-HCV-coinfected patients. Antivir. Ther. 2015, 20, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Oze, I.; Matsuo, K.; Kawakita, D.; Hosono, S.; Ito, H.; Watanabe, M.; Hatooka, S.; Hasegawa, Y.; Shinoda, M.; Tajima, K.; et al. Coffee and green tea consumption is associated with upper aerodigestive tract cancer in Japan. Int. J. Cancer 2014, 135, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Stepaniak, U.; Micek, A.; Stefler, D.; Bobak, M.; Pajak, A. Coffee consumption and mortality in three Eastern European countries: Results from the HAPIEE (Health, Alcohol and Psychosocial factors in Eastern Europe) study. Public Health Nutr. 2017, 20, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, O.J.; Roderick, P.; Buchanan, R.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Systematic review with meta-analysis: Coffee consumption and the risk of cirrhosis. Aliment. Pharmacol. Ther. 2016, 43, 562–574. [Google Scholar] [CrossRef] [PubMed]
- Setiawan, V.W.; Porcel, J.; Wei, P.; Stram, D.O.; Noureddin, N.; Lu, S.C.; Le Marchand, L.; Noureddin, M. Coffee Drinking and Alcoholic and Nonalcoholic Fatty Liver Diseases and Viral Hepatitis in the Multiethnic Cohort. Clin. Gastroenterol. Hepatol. 2017, 15, 1305–1307. [Google Scholar] [CrossRef] [PubMed]
- Jaruvongvanich, V.; Sanguankeo, A.; Klomjit, N.; Upala, S. Effects of caffeine consumption in patients with chronic hepatitis C: A systematic review and meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2017, 41, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Wolk, A. Coffee Consumption and Risk of Liver Cancer: A Meta-Analysis. Gastroenterology 2007, 132, 1740–1745. [Google Scholar] [CrossRef] [PubMed]
- Nieber, K. The Impact of Coffee on Health. Planta Med. 2017, 83, 1256–1263. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Dong, L.; Jiang, J.; Zhao, J.; Zhao, G.; Dang, X.; Lu, X.; Jia, M. Chlorogenic acid reduces liver inflammation and fibrosis through inhibition of toll-like receptor 4 signaling pathway. Toxicology 2013, 303, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.K.; Tate, J.P.; Fultz, S.L.; Goulet, J.L.; Conigliaro, J.; Bryant, K.J.; Gordon, A.J.; Gibert, C.; Rimland, D.; Goetz, M.B. Relationship between alcohol use categories and noninvasive markers of advanced hepatic fibrosis in HIV-infected, chronic hepatitis C virus-infected, and uninfected patients. Clin. Infect. Dis. 2014, 58, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Marcellin, F.; Roux, P.; Loko, M.-A.; Lions, C.; Caumont-Prim, A.; Dabis, F.; Salmon-Ceron, D.; Spire, B.; Carrieri, M.P.; et al. High levels of alcohol consumption increase the risk of advanced hepatic fibrosis in HIV/hepatitis C virus-coinfected patients: A sex-based analysis using transient elastography at enrollment in the HEPAVIH ANRS CO13 cohort. Clin. Infect. Dis. 2014, 59, 1190–1192. [Google Scholar] [PubMed]
- Balasubramanian, A.; Koziel, M.; Groopman, J.E.; Ganju, R.K. Molecular mechanism of hepatic injury in coinfection with hepatitis C virus and HIV. Clin. Infect. Dis. 2005, 41 (Suppl. 1), S32–S37. [Google Scholar] [CrossRef] [PubMed]
- Mascia, C.; Lichtner, M.; Zuccalà, P.; Vita, S.; Tieghi, T.; Marocco, R.; Savinelli, S.; Rossi, R.; Iannetta, M.; Campagna, M.; et al. Active HCV infection is associated with increased circulating levels of interferon-gamma (IFN-γ)-inducible protein-10 (IP-10), soluble CD163 and inflammatory monocytes regardless of liver fibrosis and HIV coinfection. Clin. Res. Hepatol. Gastroenterol. 2017, 41, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Negash, A.A.; Ramos, H.J.; Crochet, N.; Lau, D.T.; Doehle, B.; Papic, N.; Delker, D.A.; Jo, J.; Bertoletti, A.; Hagedorn, C.H.; et al. IL-1β Production through the NLRP3 Inflammasome by Hepatic Macrophages Links Hepatitis C Virus Infection with Liver Inflammation and Disease. PLoS Pathog. 2013, 9, e1003330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czaja, A.J. Hepatic inflammation and progressive liver fibrosis in chronic liver disease. World J. Gastroenterol. 2014, 20, 2515–2532. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Andrade, C.; Rufián-Henares, J.A.; Morales, F.J. Assessing the antioxidant activity of melanoidins from coffee brews by different antioxidant methods. J. Agric. Food Chem. 2005, 53, 7832–7836. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Grobe, Y.; Chávez-Tapia, N.; Sánchez-Valle, V.; Gavilanes-Espinar, J.G.; Ponciano-Rodríguez, G.; Uribe, M.; Méndez-Sánchez, N. High coffee intake is associated with lower grade nonalcoholic fatty liver disease: The role of peripheral antioxidant activity. Ann. Hepatol. 2012, 11, 350–355. [Google Scholar] [PubMed]
- Lundberg, G.D. A Supplement That May Block. The Toxic Effects of Alcohol. Medscape. Available online: http://www.medscape.com/viewarticle/885865 (accessed on 6 October 2017).
- Labarga, P.; Fernandez-Montero, J.V.; Barreiro, P.; Pinilla, J.; Vispo, E.; de Mendoza, C.; Plaza, Z.; Soriano, V. Changes in liver fibrosis in HIV/HCV-coinfected patients following different outcomes with peginterferon plus ribavirin therapy. J. Viral Hepat. 2014, 21, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Montero, J.V.; Barreiro, P.; Vispo, E.; Labarga, P.; Sánchez-Parra, C.; de Mendoza, C.; Treviño, A.; Soriano, V. Liver fibrosis progression in HIV-HCV-coinfected patients treated with distinct antiretroviral drugs and impact of pegylated interferon/ribavirin therapy. Antiviral Ther. 2014, 19, 287–292. [Google Scholar] [CrossRef] [PubMed]
- ANRS CO13 HEPAVIH Cohort. Regression of liver stiffness after sustained hepatitis C virus (HCV) virological responses among HIV/HCV-coinfected patients. AIDS 2015, 29, 1821–1830. [Google Scholar]
- Fontana, R.J.; Bonkovsky, H.L.; Naishadham, D.; Dienstag, J.L.; Sterling, R.K.; Lok, A.S.; Su, G.L.; Halt-C Trial Group. Serum fibrosis marker levels decrease after successful antiviral treatment in chronic hepatitis C patients with advanced fibrosis. Clin. Gastroenterol. Hepatol. 2009, 7, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Berenguer, J.; Alvarez-Pellicer, J.; Martín, P.M.; López-Aldeguer, J.; Von-Wichmann, M.A.; Quereda, C.; Mallolas, J.; Sanz, J.; Tural, C.; Bellón, J.M.; et al. Sustained virological response to interferon plus ribavirin reduces liver-related complications and mortality in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology 2009, 50, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Benhamou, Y.; Bochet, M.; Di Martino, V.; Charlotte, F.; Azria, F.; Coutellier, A.; Vidaud, M.; Bricaire, F.; Opolon, P.; Katlama, C.; et al. Liver fibrosis progression in human immunodeficiency virus and hepatitis C virus coinfected patients. The Multivirc Group. Hepatology 1999, 30, 1054–1058. [Google Scholar] [CrossRef] [PubMed]
- Graham, C.S.; Baden, L.R.; Yu, E.; Mrus, J.M.; Carnie, J.; Heeren, T.; Koziel, M.J. Influence of human immunodeficiency virus infection on the course of hepatitis C virus infection: A meta-analysis. Clin. Infect. Dis. 2001, 33, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Bräu, N.; Salvatore, M.; Ríos-Bedoya, C.F.; Fernández-Carbia, A.; Paronetto, F.; Rodríguez-Orengo, J.F.; Rodríguez-Torres, M. Slower fibrosis progression in HIV/HCV-coinfected patients with successful HIV suppression using antiretroviral therapy. J. Hepatol. 2006, 44, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Bani-Sadr, F.; Lapidus, N.; Bedossa, P.; De Boever, C.M.; Perronne, C.; Halfon, P.; Pol, S.; Carrat, F.; Cacoub, P.; French National Agency for Research on AIDS; et al. Progression of fibrosis in HIV and hepatitis C virus-coinfected patients treated with interferon plus ribavirin-based therapy: Analysis of risk factors. Clin. Infect. Dis. 2008, 46, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Zarracina, T.; Valle-Garay, E.; Collazos, J.; Montes, A.H.; Cárcaba, V.; Carton, J.A.; Asensi, V. Didanosine (ddI) associates with increased liver fibrosis in adult HIV-HCV coinfected patients. J. Viral Hepat. 2012, 19, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Dyal, H.K.; Aguilar, M.; Bhuket, T.; Liu, B.; Holt, E.W.; Torres, S.; Cheung, R.; Wong, R.J. Concurrent Obesity, Diabetes, and Steatosis Increase Risk of Advanced Fibrosis among HCV Patients: A Systematic Review. Dig. Dis. Sci. 2015, 60, 2813–2824. [Google Scholar] [CrossRef] [PubMed]
- El Ray, A.; Asselah, T.; Moucari, R.; El Ghannam, M.; Taha, A.A.; Saber, M.A.; Akl, M.; Atta, R.; Shemis, M.; Radwan, A.S.; et al. Insulin resistance: A major factor associated with significant liver fibrosis in Egyptian patients with genotype 4 chronic hepatitis C. Eur. J. Gastroenterol. Hepatol. 2013, 25, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.X.; Kyulo, N.L.; Xia, V.W.; Hillebrand, D.J.; Hu, K.Q. Factors Associated with Hepatic Fibrosis in Patients with Chronic Hepatitis C: A Retrospective Study of a Large Cohort of U.S. Patients. J. Clin. Gastroenterol. 2009, 43, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; McCullough, A.J.; Ong, J.P.; Barnes, D.S.; Post, A.; Tavill, A.; Bringman, D.; Martin, L.M.; Assmann, J.; Gramlich, T.; et al. Obesity and non-alcoholic fatty liver disease in chronic hepatitis C. J. Clin. Gastroenterol. 2004, 38, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, O.J.; Roderick, P.; Buchanan, R.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee, including caffeinated and decaffeinated coffee, and the risk of hepatocellular carcinoma: A systematic review and dose-response meta-analysis. BMJ Open 2017, 7, e013739. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Micek, A.; Marranzano, M.; Salomone, F.; Rio, D.D.; Ray, S. Coffee Consumption and Risk of Biliary Tract Cancers and Liver Cancer: A Dose-Response Meta-Analysis of Prospective Cohort Studies. Nutrients 2017, 9, 950. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N (%) | Advanced Liver Fibrosis 1 | |||
|---|---|---|---|---|
| No, 822 (84.8%) | Yes, 147 (15.2%) | p-Value (chi-2) | ||
| Age, years | 0.0856 * | |||
| Mean (±SD) | 47.8 (±6.4) | 47.4 (±6.3) | 49.3 (±7.0) | |
| Median (IQR) | 48 (44–51) | |||
| Gender | 0.2880 | |||
| Male | 710 (69.7) | 568 (69.1) | 108 (73.5) | |
| Female | 309 (30.3) | 254 (30.9) | 39 (26.5) | |
| Living in a couple | 0.8208 | |||
| No | 526 (51.9) | 418 (51.0) | 76 (52.1) | |
| Yes | 488 (48.1) | 401 (49.0) | 70 (47.9) | |
| High-school certificate | 0.1331 | |||
| No | 576 (66.4) | 449 (65.2) | 97 (71.8) | |
| Yes | 291 (33.6) | 240 (34.8) | 38 (28.2) | |
| Employment | 0.0100 | |||
| No | 525 (51.8) | 406 (49.7) | 90 (61.2) | |
| Yes | 489 (48.2) | 411 (50.3) | 57 (38.8) | |
| CDC clinical stage | 0.5139 | |||
| Stage A | 446 (45.1) | 369 (45.0) | 63 (42.9) | |
| Stage B | 260 (26.3) | 221 (26.9) | 36 (24.5) | |
| Stage C | 283 (28.6) | 230 (28.1) | 48 (32.6) | |
| CD4 count, cells/mm3 | <0.0001 * | |||
| Mean (±SD) | 564 (±309) | 594 (±311) | 394 (±355) | |
| Median (IQR) | 516 (341–733) | |||
| Body mass index 2 | 0.2155 | |||
| Underweight or Normal | 749 (78.4) | 633 (79.6) | 103 (74.6) | |
| Overweight | 162 (17.0) | 129 (16.2) | 25 (18.1) | |
| Obese | 44 (4.6) | 33 (4.2) | 10 (7.3) | |
| Diabetes | 0.1888 | |||
| No | 1008 (98.9) | 815 (99.1) | 144 (98.0) | |
| Yes | 11 (1.1) | 7 (0.9) | 3 (2.0) | |
| Receiving ART | 0.5111 | |||
| No | 50 (5.0) | 40 (4.9) | 9 (6.3) | |
| Yes | 951 (95.0) | 770 (95.1) | 135 (93.7) | |
| HCV treatment status | <0.0001 | |||
| Not yet treated | 643 (63.1) | 518 (63.0) | 98 (66.7) | |
| On treatment | 62 (6.1) | 36 (4.4) | 19 (12.9) | |
| Treated, chronic HCV | 108 (10.6) | 79 (9.6) | 25 (17.0) | |
| Treated, HCV-cured | 206 (20.2) | 189 (23.0) | 5 (3.4) | |
| Alcohol consumption 3 | 0.0018 | |||
| Low-risk | 916 (94.2) | 749 (95.3) | 125 (88.7) | |
| High-risk | 56 (5.8) | 37 (4.7) | 16 (11.3) | |
| Binge drinking 4 | 0.0699 | |||
| No | 725 (72.4) | 594 (73.5) | 96 (66.2) | |
| Yes | 276 (27.6) | 214 (26.5) | 47 (33.8) | |
| Coffee intake | 0.0002 | |||
| Low | 713 (72.6) | 561 (70.7) | 122 (85.9) | |
| High | 269 (27.4) | 232 (29.3) | 20 (14.1) | |
| Cannabis consumption | 0.5252 | |||
| No | 620 (71.8) | 497 (71.4) | 92 (74.2) | |
| Yes | 244 (28.2) | 199 (28.6) | 32 (25.8) | |
| Tobacco consumption | 0.4535 | |||
| Never | 116 (12.6) | 102 (13.3) | 13 (9.6) | |
| Past | 147 (15.9) | 123 (16.0) | 21 (15.4) | |
| Current | 659 (71.5) | 543 (70.7) | 102 (75.0) | |
| Coffee intake-alcohol consumption | <0.0001 | |||
| Low coffee intake and high-risk alcohol consumption | 39 (4.0) | 25 (3.2) | 12 (8.5) | |
| Low coffee intake and low-risk alcohol consumption | 666 (68.9) | 529 (67.8) | 109 (77.3) | |
| High coffee intake and high-risk alcohol consumption | 15 (1.6) | 10 (1.3) | 4 (2.8) | |
| High coffee intake and low-risk alcohol consumption | 246 (25.5) | 216 (27.7) | 16 (11.4) | |
| Mixed-Effects Logistic Regression Models | ||||
|---|---|---|---|---|
| Univariate Analyses | Multivariable Analysis | |||
| OR (95% CI) | p-Value | AOR (95% CI) | p-Value | |
| Age, years | 1.08 (1.05–1.1) | <0.001 | 1.18 (1.13–1.22) | <0.0001 |
| Gender | ||||
| Male | 1 | |||
| Female | 0.67 (0.41–1.09) | 0.109 | ||
| Living in a couple | ||||
| No | 1 | |||
| Yes | 0.91 (0.65–1.27) | 0.559 | ||
| High-school certificate | ||||
| No | 1 | |||
| Yes | 0.66 (0.40–1.10) | 0.114 | ||
| Employment | ||||
| No | 1 | |||
| Yes | 0.54 (0.40–0.74) | 0.0002 | ||
| CDC clinical stage | 0.463 | |||
| Stage A | 1 | |||
| Stage B | 1.25 (0.70–2.23) | 0.417 | ||
| Stage C | 1.37 (0.77–2.44) | 0.252 | ||
| CD4 count 1, cells/mm3 | 0.85 (0.82–0.88) | <0.0001 | 0.74 (0.71–0.78) | <0.0001 |
| Obesity 2 | <0.0021 | 0.0031 | ||
| No | 1 | 1 | ||
| Yes | 4.24 (1.78–10.10) | 0.0021 | 5.93 (1.95–18.07) | 0.0031 |
| Diabetes | ||||
| No | 1 | |||
| Yes | 1.55 (0.75–3.21) | 0.229 | ||
| Receiving ART | ||||
| No | 1 | |||
| Yes | 0.23 (0.13–0.39) | <0.0001 | 0.18 (0.09–0.34) | <0.0001 |
| HCV treatment status | <0.0001 | <0.0001 | ||
| Not yet treated | 1 | 1 | ||
| On treatment/Treated, chronic HCV | 2.50 (1.79–3.49) | <0.0001 | 1.96 (1.33–2.90) | 0.0008 |
| Treated, HCV-cured | 0.07 (0.04–0.13) | <0.0001 | 0.04 (0.02–0.08) | <0.0001 |
| Alcohol consumption 3 | ||||
| Low-risk | 1 | |||
| High-risk | 3.2 (1.8–5.7) | 0.0002 | ||
| Binge drinking 4 | ||||
| No | 1 | |||
| Yes | 0.85 (0.62–1.17) | 0.3065 | ||
| Coffee intake | ||||
| Low | 1 | |||
| High | 0.49 (0.35–0.69) | <0.0001 | ||
| Cannabis consumption | ||||
| No | 1 | |||
| Yes | 1.09 (0.72–1.65) | 0.687 | ||
| Tobacco consumption | 0.6354 | |||
| Never | 1 | |||
| Past | 1.28 (0.28–5.93) | 0.7402 | ||
| Current | 1.67 (0.46–6.08) | 0.4095 | ||
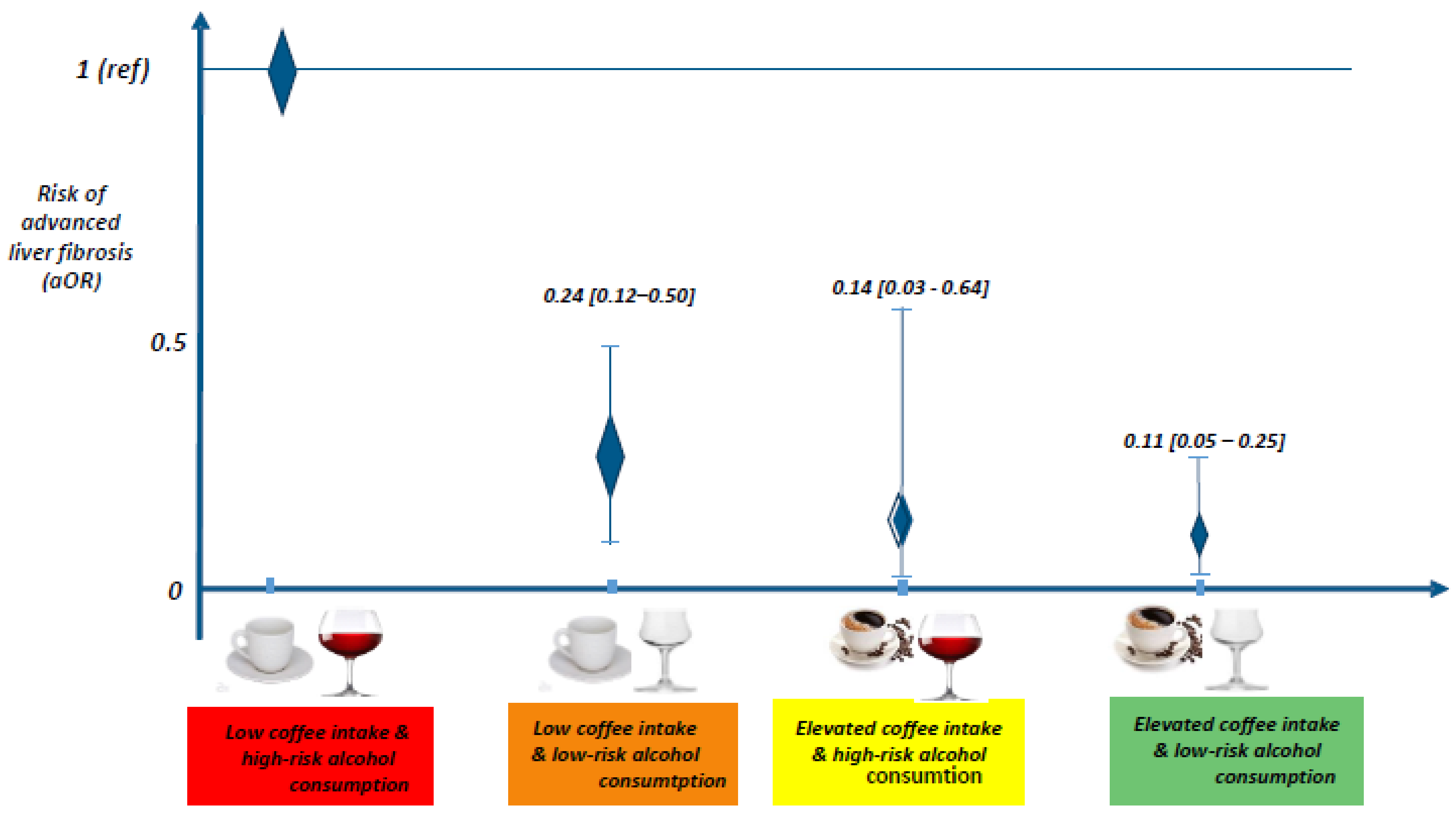
| Coffee intake-alcohol consumption | <0.0001 | <0.0001 | ||
| Low coffee intake and high-risk alcohol consumption | 1 | 1 | ||
| Low coffee intake and low-risk alcohol consumption | 0.24 (0.13–0.46) | <0.0001 | 0.24 (0.12–0.50) | 0.0002 |
| High coffee intake and high-risk alcohol consumption | 0.26 (0.09–0.74) | 0.0117 | 0.14 (0.03–0.64) | 0.0114 |
| High coffee intake and low-risk alcohol consumption | 0.14 (0.07–0.27) | <0.0001 | 0.11 (0.05–0.25) | <0.0001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yaya, I.; Marcellin, F.; Costa, M.; Morlat, P.; Protopopescu, C.; Pialoux, G.; Santos, M.E.; Wittkop, L.; Esterle, L.; Gervais, A.; et al. Impact of Alcohol and Coffee Intake on the Risk of Advanced Liver Fibrosis: A Longitudinal Analysis in HIV-HCV Coinfected Patients (ANRS CO-13 HEPAVIH Cohort). Nutrients 2018, 10, 705. https://doi.org/10.3390/nu10060705
Yaya I, Marcellin F, Costa M, Morlat P, Protopopescu C, Pialoux G, Santos ME, Wittkop L, Esterle L, Gervais A, et al. Impact of Alcohol and Coffee Intake on the Risk of Advanced Liver Fibrosis: A Longitudinal Analysis in HIV-HCV Coinfected Patients (ANRS CO-13 HEPAVIH Cohort). Nutrients. 2018; 10(6):705. https://doi.org/10.3390/nu10060705
Chicago/Turabian StyleYaya, Issifou, Fabienne Marcellin, Marie Costa, Philippe Morlat, Camelia Protopopescu, Gilles Pialoux, Melina Erica Santos, Linda Wittkop, Laure Esterle, Anne Gervais, and et al. 2018. "Impact of Alcohol and Coffee Intake on the Risk of Advanced Liver Fibrosis: A Longitudinal Analysis in HIV-HCV Coinfected Patients (ANRS CO-13 HEPAVIH Cohort)" Nutrients 10, no. 6: 705. https://doi.org/10.3390/nu10060705
APA StyleYaya, I., Marcellin, F., Costa, M., Morlat, P., Protopopescu, C., Pialoux, G., Santos, M. E., Wittkop, L., Esterle, L., Gervais, A., Sogni, P., Salmon-Ceron, D., Carrieri, M. P., & The ANRS CO13-HEPAVIH Cohort Study Group. (2018). Impact of Alcohol and Coffee Intake on the Risk of Advanced Liver Fibrosis: A Longitudinal Analysis in HIV-HCV Coinfected Patients (ANRS CO-13 HEPAVIH Cohort). Nutrients, 10(6), 705. https://doi.org/10.3390/nu10060705