Association between Blood 25-Hydroxyvitamin D Levels and Survival in Colorectal Cancer Patients: An Updated Systematic Review and Meta-Analysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection
2.3. Data Extraction
2.4. Statistical Analysis
2.4.1. Meta-Analysis
2.4.2. Dose-Response Meta-Analysis
3. Results
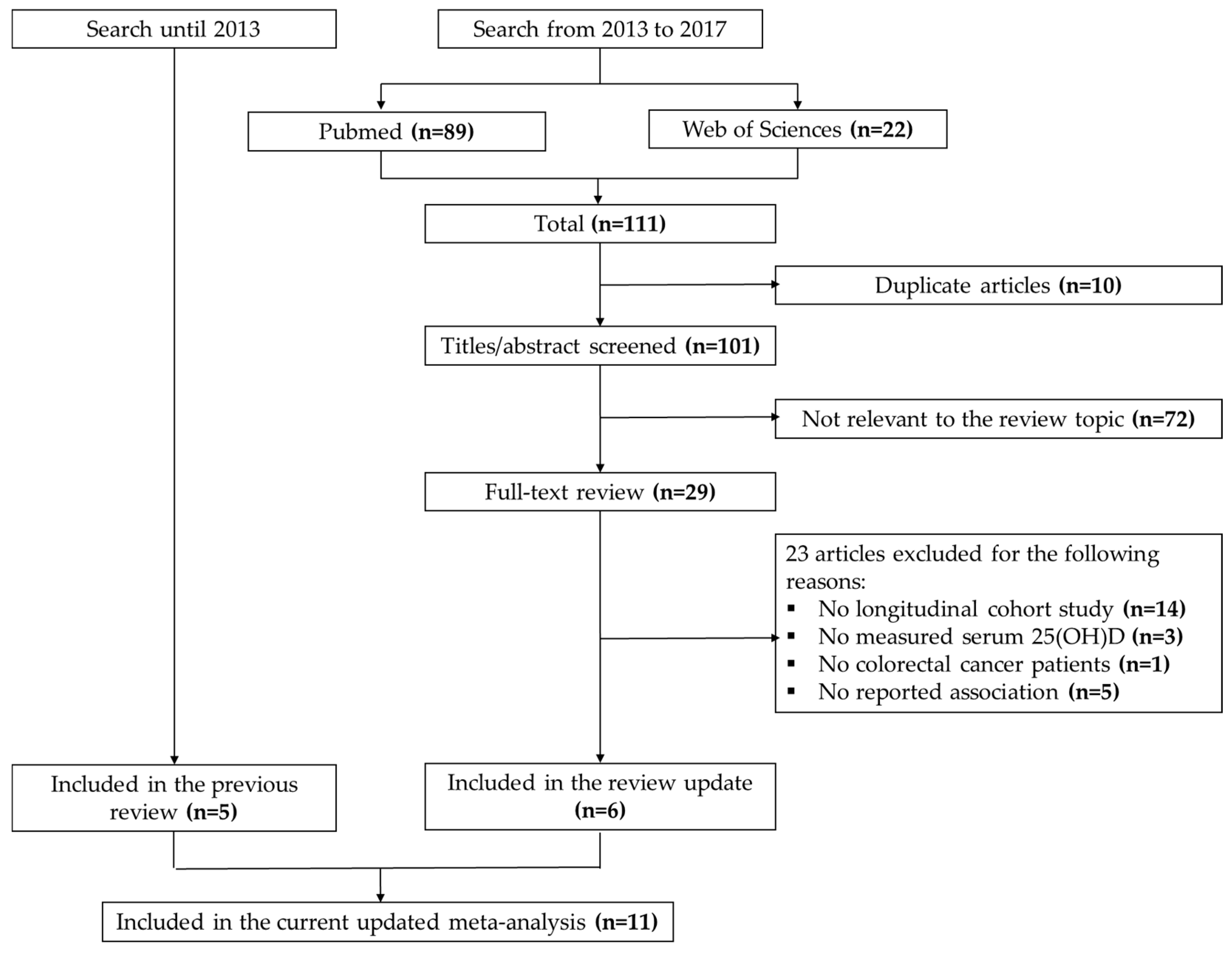
3.1. Search Results
3.2. Study Characteristics
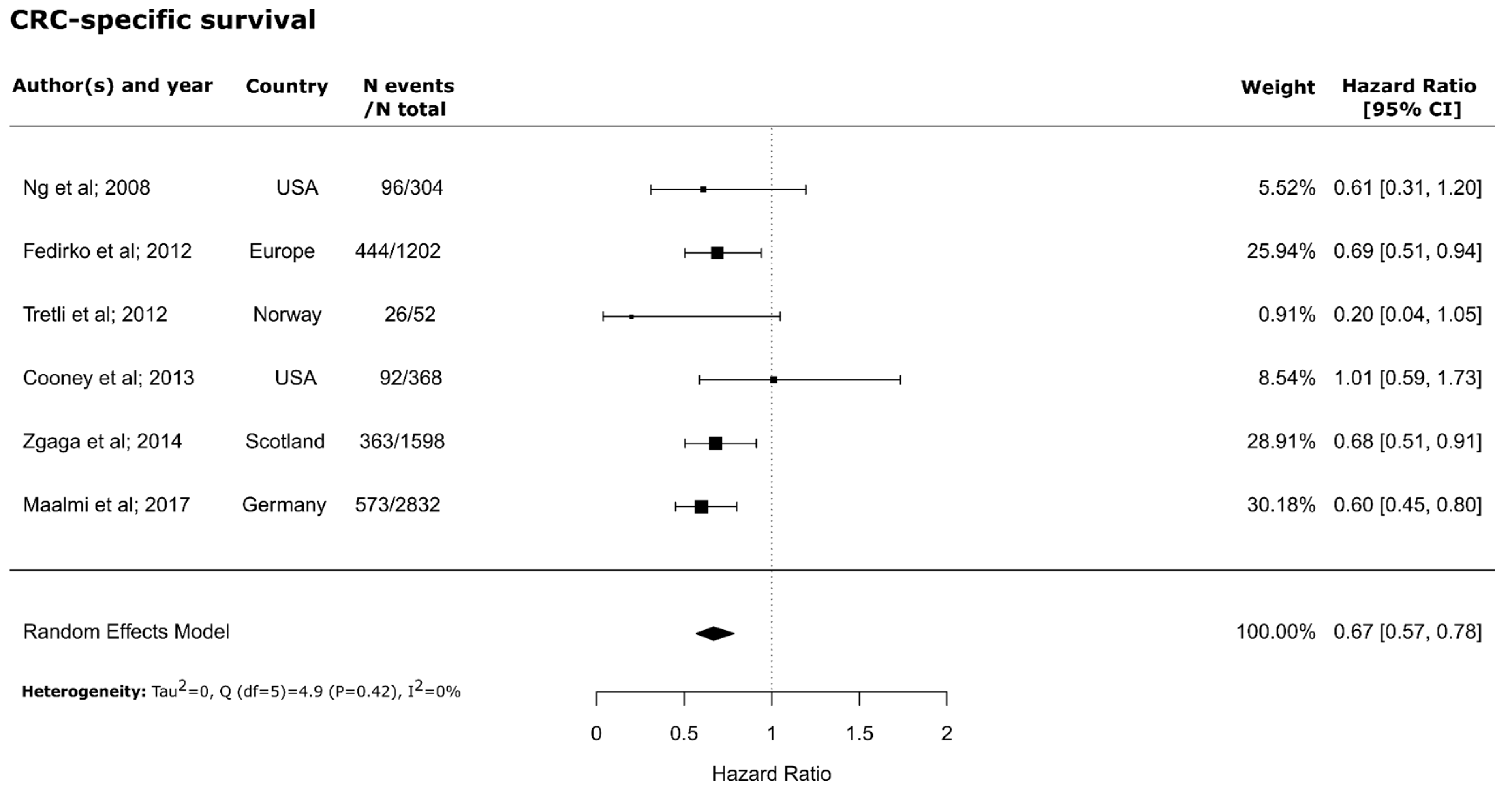
3.3. Meta-Analysis
3.4. Sensitivity Analyses
3.5. Subgroup Analyses
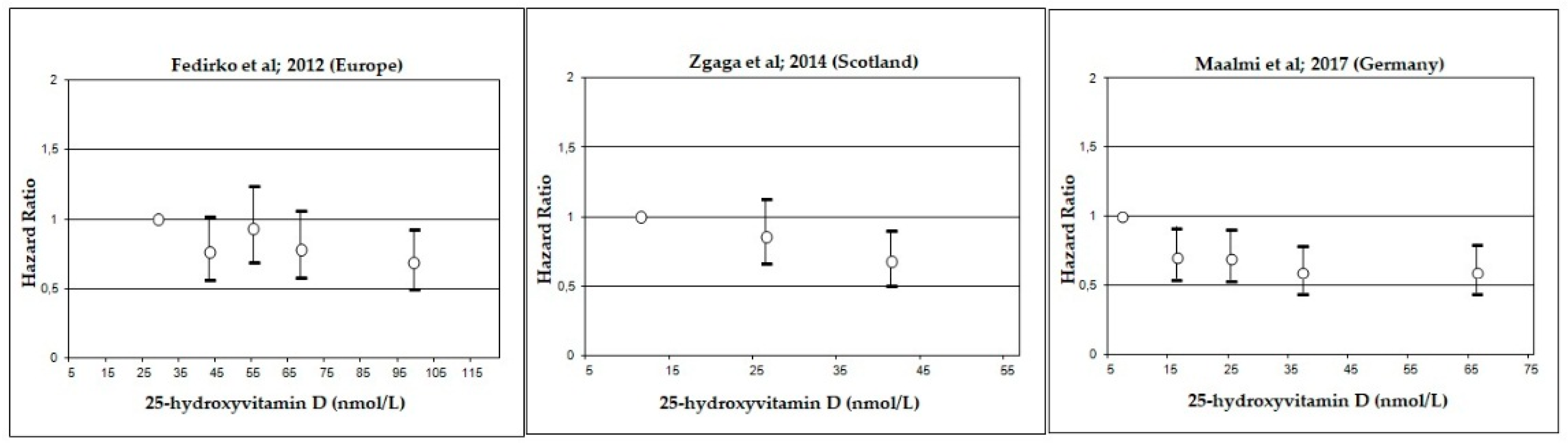
3.6. Dose-Response Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Garland, C.F.; Garland, F.C. Do sunlight and vitamin d reduce the likelihood of colon cancer? Int. J. Epidemiol. 1980, 9, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Fedirko, V.; Riboli, E.; Tjonneland, A.; Ferrari, P.; Olsen, A.; Bueno-de-Mesquita, H.B.; van Duijnhoven, F.J.; Norat, T.; Jansen, E.H.; Dahm, C.C.; et al. Prediagnostic 25-hydroxyvitamin d, vdr and casr polymorphisms, and survival in patients with colorectal cancer in western european ppulations. Cancer Epidemiol. Biomark. Prev. 2012, 21, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Mezawa, H.; Sugiura, T.; Watanabe, M.; Norizoe, C.; Takahashi, D.; Shimojima, A.; Tamez, S.; Tsutsumi, Y.; Yanaga, K.; Urashima, M. Serum vitamin d levels and survival of patients with colorectal cancer: Post-hoc analysis of a prospective cohort study. BMC Cancer 2010, 10, 347. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Meyerhardt, J.A.; Wu, K.; Feskanich, D.; Hollis, B.W.; Giovannucci, E.L.; Fuchs, C.S. Circulating 25-hydroxyvitamin d levels and survival in patients with colorectal cancer. J. Clin. Oncol. 2008, 26, 2984–2991. [Google Scholar] [CrossRef] [PubMed]
- Ng, K. Vitamin d for prevention and treatment of colorectal cancer: What is the evidence? Curr. Colorectal Cancer Rep. 2014, 10, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Toriola, A.T.; Nguyen, N.; Scheitler-Ring, K.; Colditz, G.A. Circulating 25-hydroxyvitamin d levels and prognosis among cancer patients: A systematic review. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 917–933. [Google Scholar] [CrossRef] [PubMed]
- van Harten-Gerritsen, A.S.; Balvers, M.G.; Witkamp, R.F.; Kampman, E.; van Duijnhoven, F.J. Vitamin d, inflammation, and colorectal cancer progression: A review of mechanistic studies and future directions for epidemiological studies. Cancer Epidemiol. Biomarkers Prev. 2015, 24, 1820–1828. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Chen, P.; Li, J.; Chu, R.; Xie, D.; Wang, H. Review: The impacts of circulating 25-hydroxyvitamin d levels on cancer patient outcomes: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2014, 99, 2327–2336. [Google Scholar] [CrossRef] [PubMed]
- Maalmi, H.; Ordonez-Mena, J.M.; Schottker, B.; Brenner, H. Serum 25-hydroxyvitamin d levels and survival in colorectal and breast cancer patients: Systematic review and meta-analysis of prospective cohort studies. Eur. J. Cancer 2014, 50, 1510–1521. [Google Scholar] [CrossRef] [PubMed]
- Mohr, S.B.; Gorham, E.D.; Kim, J.; Hofflich, H.; Cuomo, R.E.; Garland, C.F. Could vitamin d sufficiency improve the survival of colorectal cancer patients? J. Steroid Biochem. Mol. Biol. 2015, 148, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Ou, B.; Zhao, J.; Guan, S.; Lu, A. Plasma 25-hydroxyvitamin d levels and survival of colorectal cancer patients: A meta-analysis. Eur. J. Cancer 2015, 51, 786–788. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Jing, Z.; Li, C.; Xu, S.; Wang, Y. Blood 25-hydroxyvitamin d levels and overall mortality in patients with colorectal cancer: A dose-response meta-analysis. Eur. J. Cancer 2014, 50, 2173–2175. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of observational studies in epidemiology (moose) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Hardy, R.J.; Thompson, S.G. Detecting and describing heterogeneity in meta-analysis. Stat. Med. 1998, 17, 841–856. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, M.A.; Yuan, C.; Sato, K.; Niedzwiecki, D.; Ye, X.; Saltz, L.B.; Mayer, R.J.; Mowat, R.B.; Whittom, R.; Hantel, A.; et al. Predicted vitamin d status and colon cancer recurrence and mortality in calgb 89803 (alliance). Ann. Oncol. 2017, 28, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Wolpin, B.M.; Meyerhardt, J.A.; Wu, K.; Chan, A.T.; Hollis, B.W.; Giovannucci, E.L.; Stampfer, M.J.; Willett, W.C.; Fuchs, C.S. Prospective study of predictors of vitamin d status and survival in patients with colorectal cancer. Br. J. Cancer 2009, 101, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Cooney, R.V.; Chai, W.; Franke, A.A.; Wilkens, L.R.; Kolonel, L.N.; Le Marchand, L. C-reactive protein, lipid-soluble micronutrients, and survival in colorectal cancer patients. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 1278–1288. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Sargent, D.J.; Goldberg, R.M.; Meyerhardt, J.A.; Green, E.M.; Pitot, H.C.; Hollis, B.W.; Pollak, M.N.; Fuchs, C.S. Vitamin D status in patients with stage iv colorectal cancer: Findings from intergroup trial n9741. J. Clin. Oncol. 2011, 29, 1599–1606. [Google Scholar] [CrossRef] [PubMed]
- Wesa, K.M.; Segal, N.H.; Cronin, A.M.; Sjoberg, D.D.; Jacobs, G.N.; Coleton, M.I.; Fleisher, M.; Dnistrian, A.M.; Saltz, L.B.; Cassileth, B.R. Serum 25-hydroxy vitamin d and survival in advanced colorectal cancer: A retrospective analysis. Nutr. Cancer 2015, 67, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Zgaga, L.; Theodoratou, E.; Farrington, S.M.; Din, F.V.; Ooi, L.Y.; Glodzik, D.; Johnston, S.; Tenesa, A.; Campbell, H.; Dunlop, M.G. Plasma vitamin d concentration influences survival outcome after a diagnosis of colorectal cancer. J. Clin. Oncol. 2014, 32, 2430–2439. [Google Scholar] [CrossRef] [PubMed]
- Tretli, S.; Schwartz, G.G.; Torjesen, P.A.; Robsahm, T.E. Serum levels of 25-hydroxyvitamin d and survival in Norwegian patients with cancer of breast, colon, lung, and lymphoma: A population-based study. Cancer Causes Control 2012, 23, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Maalmi, H.; Walter, V.; Jansen, L.; Chang-Claude, J.; Owen, R.W.; Ulrich, A.; Schottker, B.; Hoffmeister, M.; Brenner, H. Relationship of very low serum 25-hydroxyvitamin d3 levels with long-term survival in a large cohort of colorectal cancer patients from germany. Eur. J. Epidemiol. 2017, 32, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Del Prete, V.; Muscatiello, N.; Crucinio, N.; Barone, M. Prognostic role of 25-hydroxyvitamin d in patients with liver metastases from colorectal cancer treated with radiofrequency ablation. J. Gastroenterol. Hepatol. 2016, 31, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Chen, H.; Zhao, M.; Peng, P. Prognostic value of circulating vitamin d binding protein, total, free and bioavailable 25-hydroxy vitamin d in patients with colorectal cancer. Oncotarget 2017, 8, 40214–40221. [Google Scholar] [CrossRef] [PubMed]
- Sambrook, P.N.; Chen, J.S.; March, L.M.; Cameron, I.D.; Cumming, R.G.; Lord, S.R.; Schwarz, J.; Seibel, M.J. Serum parathyroid hormone is associated with increased mortality independent of 25-hydroxy vitamin d status, bone mass, and renal function in the frail and very old: A cohort study. J. Clin. Endocrinol. Metab. 2004, 89, 5477–5481. [Google Scholar] [CrossRef] [PubMed]
- Fakih, M.G.; Trump, D.L.; Johnson, C.S.; Tian, L.; Muindi, J.; Sunga, A.Y. Chemotherapy is linked to severe vitamin d deficiency in patients with colorectal cancer. Int. J. Colorectal Dis. 2009, 24, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Fink, M. Vitamin d deficiency is a cofactor of chemotherapy-induced mucocutaneous toxicity and dysgeusia. J. Clin. Oncol. 2011, 29, e81–e82. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Sherman, A.; Monari-Sparks, M.J.; Schweiker, O.; Hunter, K. Correction of low vitamin d improves fatigue: Effect of correction of low vitamin d in fatigue study (evidif study). N. Am. J. Med. Sci. 2014, 6, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Kottler, M.L. Is vitamin d a key factor in muscle health? Endocrinology 2013, 154, 3963–3964. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Jansen, L.; Saum, K.U.; Holleczek, B.; Schottker, B. Vitamin d supplementation trials aimed at reducing mortality have much higher power when focusing on people with low serum 25-hydroxyvitamin d concentrations. J. Nutr. 2017, 147, 1325–1333. [Google Scholar] [CrossRef] [PubMed]
- Kimball, S.M.; Mirhosseini, N.; Holick, M.F. Evaluation of vitamin d3 intakes up to 15,000 international units/day and serum 25-hydroxyvitamin d concentrations up to 300 nmol/l on calcium metabolism in a community setting. Dermatoendocrinol 2017, 9, e1300213. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.E.; Byrne, S.N. Does sunlight protect us from cancer? Photochem. Photobiol. Sci. 2017, 16, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.D.; Ebrahim, S. ‘Mendelian randomization’: Can genetic epidemiology contribute to understanding environmental determinants of disease? Int. J. Epidemiol. 2003, 32, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Afzal, S.; Brondum-Jacobsen, P.; Bojesen, S.E.; Nordestgaard, B.G. Genetically low vitamin d concentrations and increased mortality: Mendelian randomisation analysis in three large cohorts. BMJ 2014, 349, g6330. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s) (Year) Study Acronym | Study Population | Association of 25(OH)D with Mortality | Covariates and Stratification Factors | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Overall Survival | CRC-Specific Survival | |||||||||
| Country (Recruitment Period) FU (Years) | Ntotal (Sex: F/M) (Stage) | All Deaths (CRC Deaths) | Age: Mean/Median (Range) | Time between Diagnosis and Blood Draw/Measurement Method | 25(OH)D Levels (nmol/L) Mid-Point/Interval | HR (95% CI) | 25(OH)D Levels (nmol/L) Mid-Point/Interval | HR (95% CI) | ||
| Ng et al. (2008) NHS/HPFS [5] | United States of America (USA) (1991–2002) Median: 6.5 | 304 (159/145) (stage I–IV) | 123 (96) | 68 (All) 43–70 (NHS) 40–75 (HPFS) | Pre-diagnostic (>2 years before diagnosis)/RIA | 41 59 72 100 | 1.00 0.81 (0.49–1.35) 0.81 (0.48–1.37) 0.52 (0.29–0.94) | 41 59 72 100 | 1.00 0.76 (0.41–1.42) 1.04 (0.58–1.89) 0.61 (0.31–1.19) | Age, sex, season, BMI, physical activity, race, stage, grade, tumor location, dietary vitamin D intake |
| Mezawa et al. (2010) [4] | Japan (2003–2008) Median: 2.7 | 257 (92/165)(stage I–IV) | 39 (30) | 65 (50–80) | Post-diagnostic (at operation)/RIA | 7.5–17 20–25 28–38 40–90 | 0.5 (0.16–1.54) 0.55 (0.18–1.65) 1.00 0.16 (0.04–0.63) | Per 2.5 nmol/L | 0.98 (0.89–1.08) | Age, sex, season, BMI, physical activity, stage, tumor location, type of resection, number of lymph nodes with metastasis |
| Ng et al. (2011) a N9741 [22] | USA/Canada (1998–2001) Median: 5.1 | 515 (209/306)(stage IV) | 475 (N.R) | 61 (26–85) | Post-diagnostic (after chemotherapy)/RIA | 5.7–33 33–50 50–68 68–188 | 1.00 0.78 (0.60–1.02) 1.13 (0.87–1.47) 0.94 (0.72–1.23) | N.R | N.R | Age, sex, race, geographic region, number of metastatic sites, chemotherapy |
| Fedirko et al. (2012) EPIC [3] | Europe (1992–1998) Mean: 6 | 1202 (606/596) (stage I–IV) | 541 (444) | 62 (N.R) | Pre-diagnostic/EIA | 29 43 55 68 99 | 1.000.82 (0.63–1.07) 0.91 (0.70–1.18) 0.78 (0.59–1.03) 0.67 (0.50–0.88) | 29 43 55 68 99 | 1.000.76 (0.56–1.02) 0.93 (0.69–1.24) 0.78 (0.58–1.06) 0.69 (0.50–0.93) | Age, sex, season, BMI, smoking, physical activity, stage, tumor location, grade, dietary calcium intake |
| Tretli et al. (2012) JANUS cohort [25] | Norway (1973–2007) Range: 0–24 | 52 (20/32) (stage I–IV) | 36 (26) | 59 (32–75) | 30 days (−82; +87) b /RIA | <46 46–61 62–81 >81 | 1.00 0.48 (0.18–1.29) 0.61 (0.23–1.59) 0.40 (0.10–1.60) | <44 44–56 56–76 >77 | 1.00 0.46 (0.15–1.48) 0.73 (0.25–2.15) 0.20 (0.04–1.10) | Age, sex, stage, days between sampling and measurement |
| Cooney et al. (2013) [21] | United States of America (USA) (1994–1998) Mean: 8.03 | 368 (152/216) (stage I–IV) | 175 (92) | 64.8 (<85 years) | Post-diagnostic (at least 21 days after chemotherapy)/LCMS | <38.7 38.7–52 52.2–61.7 62–77 >77 | 1.00 1.12 (0.68–1.83) 1.28 (0.78–2.10)1.45 (0.88–2.39)1.06 (0.64–1.75) | <47.5 47.5–66.5 >66.5 | 1.00 0.96 (0.57–1.63) 1.01 (0.59–1.74) | Age at diagnosis, stage, race, sex, smoking status, month of blood draw, log CRP |
| Zgaga et al. (2014) SOCCS cohort [24] | Scotland (1999–2006) Median: 8.9 | 1598 (682/916) (stage I–III) | 531 (363) | 62 (N.R) | Post-diagnostic (median of 105 days after surgery)/LCMS | <18 18–33 >33 | 1.00 0.81 (0.65–1.01) 0.70 (0.55–0.89) | <18 18–33 >33 | 1.00 0.86 (0.66–1.13) 0.68 (0.50–0.90) | Age, sex, season, stage, tumor site, surgery, time between definitive treatment and sampling, BMI, physical activity |
| Wesa et al. (2015) [23] | United States of America (USA) (2005–2006) Median: 3.4 | 241 (N.R) (stage IV) | 153 (N.R) | 63 (52–73) | Post-diagnostic (±30 days)/RIA | <75 ≥75 | 1.00 0.61 (0.38–0.98) | N.R | N.R | Albumin, ECOG performance status |
| Facciorusso et al. (2016) [27] | Italy (1999–2011) Median: 6 | 143 (41/102) (stage IV) | 95 (89) | 68 (41–85) | Post-diagnostic (after chemotherapy)/RIA | ≤50 >50 | 1.00 0.35 (0.21–0.59) | N.R | N.R | Carcinoembryonic Antigen, number of nodules, nodule size |
| Yang et al. (2017) [28] | China (2011–2012) Median: 3.75 | 206 (75/131) (stage I–III) | 87 (N.R) | 63 (30–85) | Post-diagnostic (7 days before surgery)/ELISA | <15.5 15.5–74.75 >74.75 | 1.00 1.18 (0.71–1.94) 1.79 (0.90–3.56) | N.R | N.R | Not adjusted |
| Maalmi et al. (2017) DACHS study [26] | Germany (2003–2010) Median: 4.8 | 2832 (1178/1732) (stage I–IV) | 787 (573) | 68 (30–96) | Post-diagnostic (36 days)/LCMS | <12 12–20 20–30 30–45 >45 | 1.00 0.68 (0.55–0.84) 0.59 (0.47–0.74) 0.56 (0.44–0.71) 0.56 (0.44–0.71) | 12 12–20 20–30 30–45 >45 | 1.00 0.71 (0.55–0.92) 0.70 (0.54–0.91) 0.60 (0.45–0.79) 0.60 (0.45–0.80) | Sex, age, season, stage, history of: diabetes, hypertension and cardiovascular diseases, tumor location, tumor detection mode, BMI, surgery, smoking, chemotherapy, physical activity, time between diagnosis and blood draw |
| Stratification Factor | No. of Studies/Patients | Random-Effects Model HR (95% CI) | Q (df) | Heterogeneity, I2 | Kendall’s Tau | Egger’s Test | |
|---|---|---|---|---|---|---|---|
| Overall | 11/8555 | 0.68 (0.55–0.85) | 27.9 (10) | 64% | 0.76 | 0.49 | |
| Geographic location | Europe | 5/5827 | 0.59 (0.48–0.72) | 6.9 (4) | 43% | 0.81 | 0.15 |
| USA/Asia | 6/2728 | 0.82 (0.58–1.16) | 12.4 (5) | 60% | 1.00 | 0.39 | |
| Year | <2013 | 5/2330 | 0.68 (0.50–0.92) | 7.3 (4) | 44% | 0.81 | 0.04 |
| ≥2013 | 6/6225 | 0.69 (0.50–0.95) | 19.4 (5) | 74% | 0.46 | 0.22 | |
| Sample size | <1000 | 8/2923 | 0.69 (0.47–1.00) | 23.5 (7) | 70% | 0.90 | 0.30 |
| ≥1000 | 3/5632 | 0.63 (0.55–0.73) | 1.8 (2) | 0% | 1.00 | 0.71 | |
| Median | <5 years | 4/3536 | 0.70 (0.42–1.19) | 10.7 (3) | 72% | 0.75 | 0.82 |
| Follow-time up | ≥5 years | 7/5019 | 0.67 (0.53–0.87) | 15.7 (6) | 62% | 0.23 | 0.20 |
| stage | I–IV | 6/5852 | 0.63 (0.50–0.79) | 7.0 (5) | 29% | 1.00 | 0.45 |
| I–III | 2/1804 | 1.05 (0.42–2.63) | 6.4 (1) | 84% | 1.00 | 1.00 | |
| IV | 3/899 | 0.60 (0.33–1.07) | 11.7 (2) | 83% | 0.33 | 0.01 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maalmi, H.; Walter, V.; Jansen, L.; Boakye, D.; Schöttker, B.; Hoffmeister, M.; Brenner, H. Association between Blood 25-Hydroxyvitamin D Levels and Survival in Colorectal Cancer Patients: An Updated Systematic Review and Meta-Analysis. Nutrients 2018, 10, 896. https://doi.org/10.3390/nu10070896
Maalmi H, Walter V, Jansen L, Boakye D, Schöttker B, Hoffmeister M, Brenner H. Association between Blood 25-Hydroxyvitamin D Levels and Survival in Colorectal Cancer Patients: An Updated Systematic Review and Meta-Analysis. Nutrients. 2018; 10(7):896. https://doi.org/10.3390/nu10070896
Chicago/Turabian StyleMaalmi, Haifa, Viola Walter, Lina Jansen, Daniel Boakye, Ben Schöttker, Michael Hoffmeister, and Hermann Brenner. 2018. "Association between Blood 25-Hydroxyvitamin D Levels and Survival in Colorectal Cancer Patients: An Updated Systematic Review and Meta-Analysis" Nutrients 10, no. 7: 896. https://doi.org/10.3390/nu10070896
APA StyleMaalmi, H., Walter, V., Jansen, L., Boakye, D., Schöttker, B., Hoffmeister, M., & Brenner, H. (2018). Association between Blood 25-Hydroxyvitamin D Levels and Survival in Colorectal Cancer Patients: An Updated Systematic Review and Meta-Analysis. Nutrients, 10(7), 896. https://doi.org/10.3390/nu10070896