Influence of Food Neophobia Level on Fruit and Vegetable Intake and Its Association with Urban Area of Residence and Physical Activity in a Nationwide Case-Control Study of Polish Adolescents

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval Statement
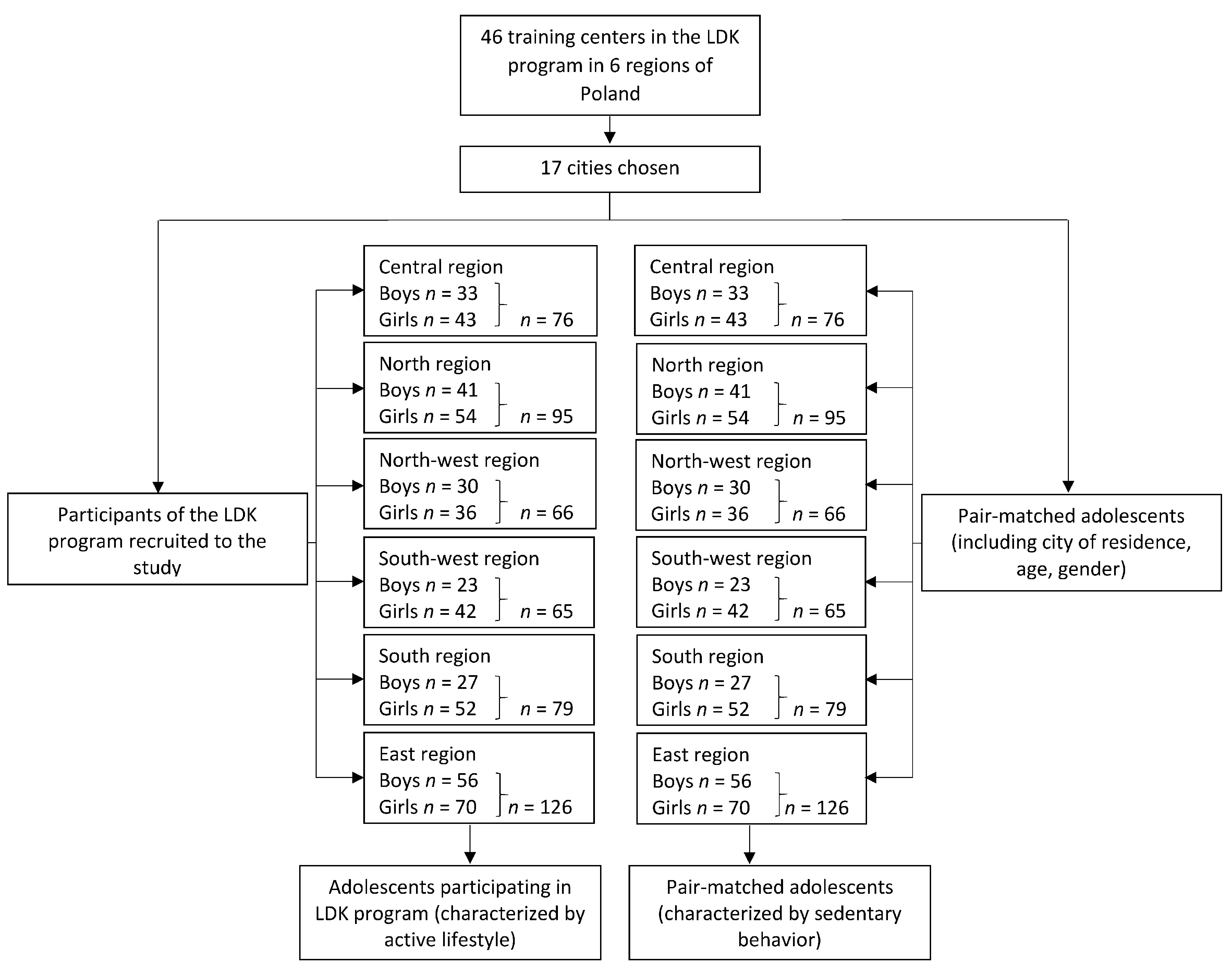
2.2. Study Participants
- -
- adolescents aged 12–13,
- -
- participating regularly in the LDK program training sessions for at least 1 year,
- -
- not participating in any other physical activity education or nutritional education program,
- -
- written consent agreement of adolescents for participation,
- -
- written consent agreement of the parent/ legal guardian for the participation of their children.
- -
- adolescents aged 12–13,
- -
- participating in the LDK program neither currently, nor in the past,
- -
- not participating in any other physical activity education or nutritional education program,
- -
- written consent agreement of adolescents for participation,
- -
- written consent agreement of the parent/ legal guardian for the participation of their children.
- -
- missing data in the completed questionnaires,
- -
- diagnosed disabilities in cognitive or motor functions,
- -
- pacemakers and other stimulators,
- -
- diagnosed epilepsy.
2.3. Study Design
2.3.1. Assessment of the Food Neophobia Level
2.3.2. Assessment of the Fruit and Vegetable Intake
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Influence of Food Neophobia Level on Fruit and Vegetable Intake
4.2. Influence of Place of Residence on Association Between Food Neophobia Level and Fruit and Vegetable Intake
4.3. Influence of Physical Activity With Peers on Association Between Food Neophobia Level and Fruit and Vegetable Intake
4.4. Summary
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dauchet, L.; Amouyel, P.; Hercberg, S.; Dallongeville, J. Fruit and vegetable consumption and risk of coronary heart disease: A meta-analysis of cohort studies. J. Nutr. 2006, 136, 2588–2593. [Google Scholar] [CrossRef] [PubMed]
- Zhan, J.; Liu, Y.J.; Cai, L.B.; Xu, F.R.; Xie, T.; He, Q.Q. Fruit and vegetable consumption and risk of cardiovascular disease: A meta-analysis of prospective cohort studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 1650–1663. [Google Scholar] [CrossRef] [PubMed]
- Dauchet, L.; Amouyel, P.; Dallongeville, J. Fruit and vegetable consumption and risk of stroke: A meta-analysis of cohort studies. Neurology 2005, 65, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Nowson, C.A.; MacGregor, G.A. Fruit and vegetable consumption and stroke: Meta-analysis of cohort studies. Lancet 2006, 367, 320–326. [Google Scholar] [CrossRef]
- Hu, D.; Huang, J.; Wang, Y.; Zhang, D.; Qu, Y. Fruits and vegetables consumption and risk of stroke: A meta-analysis of prospective cohort studies. Stroke 2014, 45, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Gan, Y.; Tong, X.; Li, L.; Cao, S.; Yin, X.; Gao, C.; Herath, C.; Li, W.; Jin, Z.; Chen, Y. Consumption of fruit and vegetable and risk of coronary heart disease: A meta-analysis of prospective cohort studies. Int. J. Cardiol. 2015, 15, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014, 349, 4490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terry, D.; Ervin, K.; Soutter, E.; Spiller, R.; Dalle Nogare, N.; Hamilton, A.J. Do Not “Let Them Eat Cake”: Correlation of Food-Consumption Patterns among Rural Primary School Children from Welfare and Non-Welfare Households. Int. J. Environ. Res. Public Health 2017, 14, 26. [Google Scholar] [CrossRef] [PubMed]
- Damsbo-Svendsen, M.; Frost, M.B.; Olsen, A. A review of instruments developed to measure food neophobia. Appetite 2017, 1, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Lafraire, J.; Rioux, C.; Giboreau, A.; Picard, D. Food rejections in children: Cognitive and social/environmental factors involved in food neophobia and picky/fussy eating behavior. Appetite 2016, 1, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Laureati, M.; Bertolia, S.; Bergamaschi, V.; Leonea, A.; Lewandowskia, L.; Giussani, B.; Battezzatia, A.; Pagliarini, E. Food neophobia and liking for fruits and vegetables are not related to Italian children’s overweight. Food Qual. Prefer. 2015, 40, 125–131. [Google Scholar] [CrossRef]
- Birch, L.L. Effects of peer models’ food choices and eating behaviors on preschoolers’ food preferences. Child Dev. 1980, 51, 489–496. [Google Scholar] [CrossRef]
- DeCosta, P.; Møller, P.; Frøst, M.B.; Olsen, A. Changing children's eating behavior–A review of experimental research. Appetite 2017, 1, 327–357. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, A.; Heary, C.; Nixon, E.; Kelly, C. Factors influencing the food choices of Irish children and adolescents: A qualitative investigation. Health Promot. Int. 2010, 25, 289–298. [Google Scholar] [CrossRef] [PubMed]
- De Andrade Previato, H.D.R.; Behrens, J.H. Taste-related factors and food neophobia: Are they associated with nutritional status and teenagers' food choices? Nutrition 2017, 42, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Prescott, J. Taste Matters: Why We Like the Foods We Do; Reaktion Books: London, UK, 2012; pp. 1–208. [Google Scholar]
- Perry, R.A.; Mallan, K.M.; Koo, J.; et al. Food neophobia and its association with diet quality and weight in children aged 24 months: a cross sectional study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 13. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Trost, S.G.; Levin, S.; Dowda, M. participation and health-related behaviors among US youth. Arch. Pediatr. Adolesc. Med. 2000, 154, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Belski, R.; Staley, K.; Keenan, S.; Skiadopoulos, A.; Randle, E.; Donaldson, A.; O’Halloran, P.; Kappelides, P.; O’Neil, S.; Nicholson, M. The impact of coaches providing healthy snacks at junior sport training. Aust. N. Z. J. Public Health 2017, 41, 561–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flight, I.; Leppard, P.; Cox, D.N. Food neophobia and associations with cultural diversity and socio-economic status amongst rural and urban Australian adolescents. Appetite 2003, 41, 51–59. [Google Scholar] [CrossRef]
- Guzek, D.; Głąbska, D.; Lange, E.; Jezewska-Zychowicz, M. A Polish Study on the Influence of Food Neophobia in Children (10–12 Years Old) on the Intake of Vegetables and Fruits. Nutrients 2017, 9, 563. [Google Scholar] [CrossRef] [PubMed]
- Pliner, P.; Hobden, K. Development of a scale to measure the trait of food neophobia in humans. Appetite 1992, 19, 105–120. [Google Scholar] [CrossRef]
- Knaapila, A.; Tuorila, H.; Silventoinen, K.; Keskitalo, K.; Kallela, M.; Wessma, M.; Peltonen, L.; Cherkas, L.C.; Spector, T.D.; Perola, M. Food neophobia shows heritable variation in humans. Physiol. Behav. 2007, 91, 573–578. [Google Scholar] [CrossRef] [PubMed]
- DeVellis, R.F. Scale Development; Sage Publications: Newbury Park, NJ, USA, 1991. [Google Scholar]
- Głąbska, D.; Malowaniec, E.; Guzek, D. Validity and Reproducibility of the Iodine Dietary Intake Questionnaire Assessment Conducted for Young Polish Women. Int. J. Environ. Res. Public Health 2017, 14, 700. [Google Scholar] [CrossRef] [PubMed]
- Dovey, T.M.; Staples, P.A.; Gibson, E.L.; Halford, J.C. Food neophobia and ‘picky/fussy’ eating in children: A review. Appetite 2018, 50, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Galinski, G.; Lonnie, M.; Kowalkowska, J.; Wadolowska, L.; Czarnocinska, J.; Jezewska-Zychowicz, M.; Babicz-Zielinska, E. Self-Reported Dietary Restrictions and Dietary Patterns in Polish Girls: A Short Research Report (GEBaHealth Study). Nutrients 2016, 8, 796. [Google Scholar] [CrossRef] [PubMed]
- Kozioł-Kozakowska, A.; Piórecka, B.; Schlegel-Zawadzka, M. Prevalence of food neophobia in pre-school children from southern Poland and its association with eating habits, dietary intake and anthropometric parameters: a cross-sectional study. Public Health Nutr. 2017, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Pelchat, M.L.; Pliner, P. “Try it. You’ll like it.”: Effects of information on willingness to try novel foods. Appetite 1995, 24, 153–165. [Google Scholar] [CrossRef]
- Pliner, P.; Loewen, E. Temperament and food neophobia in children and their mothers. Appetite 1997, 28, 239–254. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, E.; Borgers, N.; Smits, A. Presenting questionnaires for children and adolescents. In Methods for Testing and Evaluating Survey Questionnaires; Presser, S., Rothgeb, J.M., Couper, M.P., Lessler, J.T., Martin, E., Martin, J., Singer, E., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2004; pp. 409–429. ISBN 9780471654728. [Google Scholar]
- Moding, K.J.; Stifter, C.A. Stability of Food Neophobia from Infancy through Early Childhood. Appetite 2016, 97, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Nicklaus, S.; Boggio, V.; Chabanet, C.; Issanchou, S. A prospective study of food variety seeking in childhood, adolescence and early adult life. Appetite 2005, 44, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Lytle, L.A.; Seifert, S.; Greenstein, J.; McGovern, F. How do children’s eating patterns and food choices change over time? Results from a cohort study. Am. J. Health Promot. 2000, 14, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Olabi, A.; Najm, N.E.O.; Baghdadi, O.K.; Morton, J.M. Food neophobia levels of Lebanese and American college students. Food Qual. Prefer. 2009, 20, 353–362. [Google Scholar] [CrossRef]
- Bäckström, A.; Pirttilä-Backman, A.M.; Tuorila, H. Willingness to try new foods as predicted by social representation and attitude and trait scales. Appetite 2004, 43, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, R.; Abdullah, K.M.; Zahari, M.S.M.; Sharif, M.S. Revealing the Scenario of Food Neophobia among Higher Learning Institution Students from Klang Valley, Malaysia. Procedia Soc. Behav. Sci. 2015, 170, 292–299. [Google Scholar] [CrossRef]
- Tuorila, H.; Lähteenmäki, L.; Pohjalainen, L.; Lotti, L. Food neophobia among the Finns and related responses to familiar and unfamiliar foods. Food Qual. Prefer. 2001, 12, 29–37. [Google Scholar] [CrossRef]
- Ritchey, P.; Frank, R.; Hurstic, U.; Tuorila, H. Validation and cross-national comparison of the food neophobia scale (FNS) using confirmatory factor analysis. Appetite 2003, 40, 163–173. [Google Scholar] [CrossRef]
- Chung, L.; Chung, S.-J.; Kim, J.-Y.; Kim, K.-O.; O’Mahony, M.; Vickers, Z.; Cha, S.-M.; Ishii, R.; Baures, K.; Kim, H.-R. Comparing the liking for Korean style salad dressings and beverages between US and Korean consumers. Effects of sensory and non-sensory factors. Food Qual. Prefer. 2012, 26, 105–118. [Google Scholar] [CrossRef]
- Satia-About, J. Dietary Acculturation: Definition, Process, Assessment and Implications. Int. J. Hum. Ecol. 2003, 4, 71–86. [Google Scholar] [CrossRef]
- Langellotto, G.A.; Gupta, A. Gardening increases vegetable consumption in school-aged children: A meta-analytical synthesis. HortTechnology 2012, 22, 430–445. [Google Scholar]
- Paxton, S.J.; Schutz, H.K.; Wertheim, E.H.; Muir, S.L. Friendship clique and peer influences on body image concerns, dietary restraint, extreme weight-loss behaviors, and binge eating in adolescent girls. J. Abnorm. Psychol. 1999, 108, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, N.H.; Baker, J.A. The relative influence of health beliefs, parental and peer behaviors and exercise program participation on smoking, alcohol use and physical activity. Soc. Sci. Med. 1986, 22, 915–927. [Google Scholar] [CrossRef]
- Plante, T.G.; Madden, M.; Mann, S.; Muir, S.L. Effects of perceived fitness level of exercise partner on intensity of exertion. J. Soc. Sci. 2010, 6, 50–54. [Google Scholar] [CrossRef]
- Grindrod, D.; Paton, C.D.; Knez, W.L.; O’Brien, B.J. Six minute walk distance is greater when performed in a group than alone. Br. J. Sports Med. 2006, 40. [Google Scholar] [CrossRef] [PubMed]
- Salvy, S.-J.; Roemmich, J.N.; Bowker, J.C.; Romero, N.D.; Stadler, P.J.; Epstein, L.H. Effect of peers and friends on youth physical activity and motivation to be physically active. J. Pediatr. Psychol. 2009, 34, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Park, B.-K.; Cho, M.-S. Taste education reduces food neophobia and increases willingness to try novel foods in school children. Nutr. Res. Pract. 2016, 10, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Shepard, R.; Dennison, C.M. Influences on adolescent food choice. Proc. Nutr. Soc. 1996, 55, 345–357. [Google Scholar] [CrossRef] [Green Version]
- Bukowski, W.M.; Hoza, B.; Boivin, M. Measuring friendship quality during pre- and early adolescence: The development and psychometric properties of the Friendship Qualities Scale. J. Per. Soc. Psychol. 1994, 11, 471–484. [Google Scholar] [CrossRef]
- Arida, R.M.; Gomes da Silva, S.; de Almeida, A.A.; Cavalheiro, E.A.; Zavala-Tecuapetla, C.; Brand, S.; Rocha, L. Differential effects of exercise on brain opioid receptor binding and activation in rats. J. Neurochem. 2015, 132, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Berridge, K.C. “Liking” and “wanting” food rewards: Brain substrates and roles in eating disorders. Physiol. Behav. 2009, 97, 537–550. [Google Scholar] [CrossRef] [PubMed]
- Damsbo-Svendsen, M.; Frøst, M.B.; Olsen, A. Development of novel tools to measure food neophobia in children. Appetite 2017, 1, 255–263. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Food Neophobia Category | Neophilic | Neophilic Tendency | Neutral | Neophobic Tendency | Neophobic | p-Value |
|---|---|---|---|---|---|---|
| Total (n = 420) | 204.5 ± 122.4 200 * (50–600) | 209.6 ± 161.6 200 * (0–800) | 170.0 ± 128.3 100 * (0–800) | 100.1 ± 107.3 100 * (0–500) | 46.9 ± 71.3 12.5 * (0–200) | 0.0000 |
| Physical activity | ||||||
| Boys characterized by an active lifestyle (n = 210) | 212.5 ± 132.3 200 * (50–600) | 231.1 ± 172.5 200 * (0–800) | 165.8 ± 109.0 120 * (0–500) | 74.1 ± 62.9 50 * (0–200) | 108.3 ± 87.8 100 (25–200) | 0.0000 |
| Boys characterized by sedentary behavior (n = 210) | 183.3 ± 98.3 150 * (100–300) | 192.4 ± 152.0 125 * (50–800) | 173.9 ± 144.3 100 *(0–800) | 143.3 ± 148.6 100 * (0–500) | 10.0 ± 22.4 40 * (0–50) | 0.0030 |
| p-Value | 0.7681 | 0.2637 | 0.6484 | 0.2037 | 0.0737 | |
| Place of residence | ||||||
| Boys form urban area (n = 210) | 222.2 ± 83.3 200 * (100–300) | 239.5 ± 199.0 200 * (0–800) | 171.1 ± 124.0 100 * (0–600) | 132.4 ± 132.0 100 *(0–500) | 70.0 ± 83.7 50 (0–200) | 0.0072 |
| Boys form suburban area (n = 210) | 192.3 ± 145.6 150* (50–600) | 177.5 ± 99.3 175 *(50–500) | 168.8 ± 132.9 100* (0–800) | 70.8 ± 69.9 50*(0–300) | 8.3 ± 14.4 0* (0–25) | 0.0000 |
| p-Value | 0.2426 | 0.5324 | 0.7404 | 0.1399 | 0.3406 | |
| Food Neophobia Category | Neophilic | Neophilic Tendency | Neutral | Neophobic Tendency | Neophobic | p-Value |
|---|---|---|---|---|---|---|
| Total (n = 594) | 242.2 ± 151.9 200 * (50–700) | 213.4 ± 149.8 200 * (0–800) | 179.8 ± 123.8 150 * (0–700) | 112.8 ± 90.0 100 * (0–400) | 94.5 ± 90.5 75 * (0–300) | 0.0000 |
| Physical activity | ||||||
| Girls characterized by an active lifestyle (n = 297) | 263.9 ± 152.2 275 * (100–700) | 222.5 ± 163.1 200 * (0–800) | 185.4 ± 125.7 200 * (0–700) | 111.5 ± 96.9 100 * (0–400) | 108.2 ± 92.4 100 (0–300) | 0.0000 |
| Girls characterized by sedentary behavior (n = 297) | 214.3 ± 152.5 125 * (50–500) | 204.3 ± 136.1 200 * (0–600) | 174.5 ± 122.1 100 * (0–700) | 114.4 ± 85.2 100 * (0–300) | 77.8 ± 90.5 50 * (0–300) | 0.0007 |
| p-Value | 0.3141 | 0.7540 | 0.3693 | 0.7915 | 0.4250 | |
| Place of residence | ||||||
| Girls from urban area (n = 292) | 223.9 ± 164.4 150 * (50–700) | 209.9 ± 154.3 200 * (0–800) | 179.3 ± 124.3 150 * (0–700) | 137.2 ± 112.6 100 *(0–400) | 128.6 ± 122 100 (0–300) | 0.0724 |
| Girls from suburban area (n = 302) | 288.9 ± 108.3 300 (100–400) | 217.0 ± 146.3 200 * (0–600) | 180.3 ± 123.7 150 * (0–700) | 93.8 ± 65.4 100 * (0–300) | 76.2 ± 66.9 | 0.0000 |
| p-Value | 0.1368 | 0.6165 | 0.9303 | 0.2340 | 0.4054 | |
| Food Neophobia Category | Neophilic | Neophilic Tendency | Neutral | Neophobic Tendency | Neophobic | p-Value |
|---|---|---|---|---|---|---|
| Total (n = 594) | 243.2 ± 157.4 200 * (33.3–700) | 204.0 ± 142.1 200 * (0–600) | 189.1 ± 135.0 200 * (0–700) | 133.5 ± 113.6 100 * (0–500) | 45.8 ± 42.5 0 (0–100) | 0.0000 |
| Physical activity | ||||||
| Boys characterized by an active lifestyle (n = 210) | 276.0 ± 169.5 225 (100–700) | 214.5 ± 136.8 200 * (66.7–600) | 202.3 ± 137.3 200 * (0–700) | 136.0 ± 112.3 100 * (0–500) | 88.9 ± 19.2 100 * (66.7–100) | 0.0059 |
| Boys characterized by sedentary behavior (n = 210) | 155.6 ± 72.0 200 * (33.3–200) | 195.5 ± 147.2 200 * (0–600) | 176.8 ± 132.1 158.3 * (0–700) | 129.3 ± 119.7 100 * (0–400) | 20.0 ± 27.4 0 * (0–50) | 0.0068 |
| p-Value | 0.1506 | 0.4201 | 0.1162 | 0.5763 | 0.0369 | |
| Place of residence | ||||||
| Boys from urban area (n = 210) | 227.8 ± 97.2 200 (100–400) | 225.6 ± 153.3 200 * (0–600) | 183.6 ± 129.8 200 * (0–700) | 173.7 ± 135.8 150 * (0–500) | 60.0 ± 41.8 50 (0–100) | 0.0170 |
| Boys from suburban area (n = 210) | 253.8 ± 191.7 200 * (33.3–700) | 180.7 ± 126.9 175 * (0–600) | 194.6 ± 140.3 200 * (0–700) | 97.1 ± 75.3 100 * (0–600) | 22.2 ± 38.5 0 * (0–66.7) | 0.0007 |
| p-Value | 0.7894 | 0.2325 | 0.6350 | 0.0451 | 0.7894 | |
| Food Neophobia Category | Neophilic | Neophilic Tendency | Neutral | Neophobic Tendency | Neophobic | p-Value |
|---|---|---|---|---|---|---|
| Total (n = 594) | 253.1 ± 142.0 200 * (100–800) | 220.3 ± 139.3 200 * (0–700) | 213.6 ± 136.5 200 * (0–800) | 185.7 ± 126.0 200 * (0–500) | 137.5 ± 123.4 100 * (0–500) | 0.0041 |
| Physical activity | ||||||
| Girls characterized by an active lifestyle (n = 297) | 277.8 ± 148.7 275 * (100–800) | 224.7 ± 137.4 200 * (20–600) | 232.0 ± 135.8 200 * (0–700) | 179.0 ± 113.9 200 * (0–500) | 177.3 ± 150.6 100 * (0–500) | 0.0484 |
| Girls characterized by sedentary behavior (n = 297) | 221.4 ± 131.1 200 * (100–500) | 215.9 ± 142.3 200 * (0–700) | 196.3 ± 135.3 200 * (0–800) | 193.6 ± 141.0 200 * (0–500) | 88.9 ± 54.6 100 (0–200) | 0.0345 |
| p-Value | 0.1775 | 0.6296 | 0.0022 | 0.8727 | 0.2241 | |
| Place of residence | ||||||
| Girls from urban area (n = 292) | 258.7 ± 158.6 200 * (100–800) | 205.2 ± 139.6 200 * (0–700) | 200.8 ± 137.4 200 * (0–750) | 198.0 ± 145.4 200 (0–500) | 214.3 ± 165.1 200 (50–500) | 0.3521 |
| Girls from suburban area (n = 302) | 238.9 ± 92.8 200 (100–400) | 236.0 ± 138.5 200 * (30–600) | 225.6 ± 135.0 200 * (0–800) | 176.0 ± 109.9 200 * (0–500) | 96.2 ± 72.1 100 (0–300) | 0.0008 |
| p-Value | 1.0000 | 0.1566 | 0.0228 | 0.6995 | 0.0372 | |
| Analysed Group | Boys | Girls | ||
|---|---|---|---|---|
| Vegetables | Fruits | Vegetables | Fruits | |
| Physical activity | ||||
| Individuals characterized by an active lifestyle | P = 0.0000; R = −0.3390 * | P = 0.0009; R = −0.2269 * | P = 0.0000; R = −0.2679 * | P = 0.0061; R = −0.1588 * |
| Individuals characterized by sedentary behavior | P = 0.0013; R = −0.2201 * | P = 0.0031; R = −0.2032 * | P = 0.0001; R = −0.2188 * | P = 0.0348; R = −0.1225 * |
| Place of residence | ||||
| Adolescences from urban area | P = 0.0000; R = −0.2716 * | P = 0.0007; R = −0.2324 * | P = 0.0016; R = −0.1839 * | P = 0.0966; R = −0.0974 * |
| Adolescences from suburban area | P = 0.0000; R = −0.2987 * | P = 0.0029; R = −0.2040* | P = 0.0000; R = −0.2985 * | P = 0.0007; R = −0.1945 * |
| Total | P = 0.0000; R = −0.2816 * | P = 0.0000; R = −0.2168 * | P = 0.0000; R = −0.2442 * | P = 0.0006; R = −0.1404 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guzek, D.; Głąbska, D.; Mellová, B.; Zadka, K.; Żywczyk, K.; Gutkowska, K. Influence of Food Neophobia Level on Fruit and Vegetable Intake and Its Association with Urban Area of Residence and Physical Activity in a Nationwide Case-Control Study of Polish Adolescents. Nutrients 2018, 10, 897. https://doi.org/10.3390/nu10070897
Guzek D, Głąbska D, Mellová B, Zadka K, Żywczyk K, Gutkowska K. Influence of Food Neophobia Level on Fruit and Vegetable Intake and Its Association with Urban Area of Residence and Physical Activity in a Nationwide Case-Control Study of Polish Adolescents. Nutrients. 2018; 10(7):897. https://doi.org/10.3390/nu10070897
Chicago/Turabian StyleGuzek, Dominika, Dominika Głąbska, Blanka Mellová, Katarzyna Zadka, Katarzyna Żywczyk, and Krystyna Gutkowska. 2018. "Influence of Food Neophobia Level on Fruit and Vegetable Intake and Its Association with Urban Area of Residence and Physical Activity in a Nationwide Case-Control Study of Polish Adolescents" Nutrients 10, no. 7: 897. https://doi.org/10.3390/nu10070897
APA StyleGuzek, D., Głąbska, D., Mellová, B., Zadka, K., Żywczyk, K., & Gutkowska, K. (2018). Influence of Food Neophobia Level on Fruit and Vegetable Intake and Its Association with Urban Area of Residence and Physical Activity in a Nationwide Case-Control Study of Polish Adolescents. Nutrients, 10(7), 897. https://doi.org/10.3390/nu10070897